Embed Size (px)
Citation preview

FOCUS: Clinical Decision Support/Business Decision Support
26 Journal of Healthcare Information Management — Vol. 21, No. 2
“There are too many cases for the specialist…so we need to teach the patient and others how to care for andmanage diabetes.”
- Dr. Elliot P. Joslin, Founder, Joslin Diabetes CenterCaring for patients with diabetes is a challenge to primary
care providers in light of the complexity of clinicallymanaging the disease: the existence of complications andco-morbidities; the introduction of new medications, medica-tion classes and delivery mechanisms, such as inhaledinsulin; and evolving clinical best practice. This high-intensity and time-consuming care, which is inadequately
served by the typical 15- to 20-minute primary care visit, isfurther challenged by a patient’s need for provider guidanceand encouragement in best-practice self-care. With theincreasing prevalence of diabetes in the U.S., the challengesthat diabetes presents to the primary care setting willcontinue to proliferate.
Disease Registries and Decision Support
Although primary care providers must be versed in bestpractices for multiple diseases, it has been proven thatchanges in best practice are slow to be disseminated into
Improving Outcomes forPatients with Diabetes Using Joslin Diabetes
Center’s Registry and Risk Stratification System
Karen Golden Russell, MA, MBA; and James Rosenzweig, MD
A B S T R A C T
Joslin Diabetes Center’s Registry and Risk Stratification System collects data on key measures
of diabetes care and provides diabetes decision support to primary care providers.
Specifically, this system identifies high-risk patients in a population, recommends patient-
specific interventions based on Joslin’s clinical guidelines, and reports a clinic’s process and
quality metrics for benchmarking and regional comparisons.This article describes Joslin’s
system and its impact on the quality of diabetes care in the primary care setting.
K E Y W O R D S
■ Diabetes ■ Decision support ■ Quality of care ■ Primary care ■ Registry ■ Risk
■ Interventions ■ Informatics

FOCUS: Clinical Decision Support/Business Decision Support
Journal of Healthcare Information Management — Vol. 21, No. 2 27
clinical practice.1 Furthermore, providers and clinics havefew resources to support their delivery of best-practice care and to assess how they are performing against quality measures.
Registries and decision support tools can fill these needs.Disease registries are Web-based systems that are used torecord data for patients with a particular diagnosis, such asdiabetes. Data elements are typically a subset of what wouldbe found in an electronic medical record, such as generalpatient data like height, weight and other information; pastdiagnoses; labs results; details of patient visits; medications;and family history.
Registries can be used in the absence of an EMR, or theirfunctionality may be incorporated as part of an EMR. Usinga clinical algorithm to analyze this data and assess patientrisk, registries support providers in making care decisionsbased on established current clinical guidelines.
Identification of high-risk patients in a provider’s panel
has many benefits, as describedin Figure 1, which is based on a patient’s level of interactionwith a provider’s office (x-axis)and the patient’s level of risk (y-axis).
Many studies and articleshave been published aboutregistries and decision supportin the primary care setting; thisarticle focuses on the specificexperience of Joslin DiabetesCenter in the creation andimplementation of a registry anddiabetes decision support basedon Joslin’s clinical guidelines.
Joslin’s Registry and RiskStratification System
Being a specialty center forthe treatment of diabetes, JoslinDiabetes Center sees some ofthe most complex, and there-fore costly, patients in theworld. To evaluate the severityof illness for its patients incapitated managed care plans,
Joslin developed a system of risk stratification in 2002, usingfive risk categories as shown in Table 1. Only one of theserisk categories, glycemic control, is directly related todiabetes; this is because diabetes is a condition that encom-passes many organ systems.
The system assigns each risk category a risk level of low,moderate, high or very high risk. For example, a patientwith a history of hypoglycemia who has not been hospital-ized or treated in an emergency department and who has anHba1c in the range of 7 percent to 7.9 percent wouldreceive a moderate risk level for the glycemic controlcategory. Joslin’s risk stratification approach allowed fortargeted interventions to improve care in subpopulations ofpeople with diabetes and was also used to select appro-priate patients for case management.
Subsequently, this approach was incorporated by Joslin’sdisease management team into a Web-based diabetesregistry, Joslin’s Registry and Risk Stratification System

FOCUS: Clinical Decision Support/Business Decision Support
28 Journal of Healthcare Information Management — Vol. 21, No. 2
(RRSS), to address the needs of patients with diabetesoutside of the Joslin Clinic in primary care settings.
This Web-based system enabled primary care providers
and other caregivers to use patient appointments moreefficiently and effectively by automatically identifying driversrisk for each patient based on the patient’s unique combina-tion of data within the system and recommending patientinterventions based on Joslin’s practical clinical guidelines.This “to-do list” is comprised of actionable, patient-specificreminders and care recommendations appropriate for use atthe point-of-care.
Practices also used the system’s reports to track clinicprocess and quality metrics for benchmarking and regionalcomparisons, which facilitates National Committee for
“There are too many cases for the
specialist…so we need to teach the
patient and others how to care for
and manage diabetes.”

FOCUS: Clinical Decision Support/Business Decision Support
Journal of Healthcare Information Management — Vol. 21, No. 2 29
Quality Assurance provider recognition, and to trackdiabetes education, which facilitates American DiabetesAssociation Education program recognition.
The system’s algorithm is based on Joslin’s clinical guide-lines.2 Joslin’s clinical oversight committee updates theguidelines annually or more frequently as new researchdictates or as new medications become available or for otherreasons. Table 2 lists Joslin’s clinical guidelines.
RRSS Reports
The System produces five major reports.The Practice Risk Stratification Summary (Figure 2)
indicates the percentages of patients that fall into each riskcategory at the four levels of severity. By clicking apercentage, the list of patients that compose that percentageappears in a new window. To drill down further, by clickingan individual patient on the list, the provider can see the
drivers of risk for that particular patient.The Risk Stratification Levels report (Figure 3) shows risk
data for a particular patient. For each of the five riskcategories shown in the first column, the patient’s risk levelis shown in column 2. Column 3 describes why the patientwas assigned to that risk level. Note that risk is cumulative,so all levels of risk up to the level for which the patientqualifies are described.
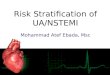
The “To Do” List for a patient (Figure 4) shows the
“Registries can be used in the
absence of an EMR, or their
functionality may be incorporated
as part of an EMR.”

FOCUS: Clinical Decision Support/Business Decision Support
30 Journal of Healthcare Information Management — Vol. 21, No. 2
patient’s last visit date and recommendations to the providerfor the patient’s care, based on Joslin’s clinical guidelines, atthis current visit.
There are many graphical trend reports available thatshow patient data in graph form; Figure 5 is one suchexample. These reports often are used during visits forpatient education purposes.
The Diabetes Performance Measure Summary (Figure 6)
enables clinics to take HEDIS3-type quality measures andcompare them with a target they have established for theirpatient population, the initial target column, as well as other clinics (“Other Sites” column) to which they areassociated.
Challenges to Using the RRSS
Primary care practices do not have time to incorporateextra processes into their workflow. Most do not have anEMR, computers in the exam room or multiple computerswith Internet access, which means that data entry for theRRSS needs to be done manually, and that it would be often difficult for busy practitioners to use the system atpoint of care.
“Primary care practices do not have
time to incorporate extra processes
into their workflow.”
Figure 4. “To Do” List.

FOCUS: Clinical Decision Support/Business Decision Support
Journal of Healthcare Information Management — Vol. 21, No. 2 31
The clinics currently using the RRSS have developedworkarounds for these challenges. For example, office staffprint the to-do list before the visit, and attach it to the frontof the patient’s chart, preparing the provider before he orshe enters the exam room to provide Joslin quality care. Inaddition, the RRSS’ data input pages are printed and used asa form by the provider to record the relevant data elementsduring the patient’s visit. After the visit, the completed formsare given to a clerical assistant to input data into the corre-sponding RRSS screens.
RRSS Outcomes
In addition to its use at Joslin’s Boston Clinic, the riskstratification system that evolved into the RRSS was used forthree years at an inner-city practice in Boston that had a
high incidence of diabetes. Joslin provided diabetes educa-tion to the provider and his patients as well as feedback tothe provider on his performance based on RRSS reports.
Outcomes included improvement in mean hemoglobinA1C (p<0.001). Because lower A1Cs indicate good diabetescontrol, a declining A1C indicates improved quality of care and patient self-care. Joslin’s Clinical Guidelines definethe target A1C for adults with diabetes of 7 percent. Anaverage reduction of 1 point in mean A1C can translate intoa 30 percent reduction of a patient’s risk of developingcomplications.
Other positive outcomes of reduction of both systolic(p<0.001) and diastolic (p<0.001) pressure, as well asincreased documented foot exams (p<0.001). Patients oftenreport that during an office visit, they did not remove shoes,

FOCUS: Clinical Decision Support/Business Decision Support
32 Journal of Healthcare Information Management — Vol. 21, No. 2
even though the foot exam is an important component of anoffice visit for patients with diabetes. If a provider actually isperforming a foot exam, it should be documented forpayment purposes. Documented foot exams are an easy butimportant improvement in quality of care.
Other positive outcomes include improved practiceoutcomes such as statistically significant improvements in thepercentage of patients with blood pressure <130/80 (p<0.01)and LDL<100 mg/dl (p<0.05). Also improved were processoutcomes, such as statistically significant improvements inthe percentage of patients on angiotensin converting enzyme
inhibitors or angiotensin receptor blockers (p<0.001). Theseinclude patients who received a microalbumin test once peryear (p<0.001); with a positive microalbumin test who wereon an ACE or ARB (p<0.001); and with hypertension whowere on medications (p<0.001).
Conclusion
Outcomes from the use of Joslin’s RRSS in the primarycare setting indicate that Joslin’s clinical guidelinesembedded into software that both risk-stratifies patientpopulations and identifies drivers of risk for individual

FOCUS: Clinical Decision Support/Business Decision Support
Journal of Healthcare Information Management — Vol. 21, No. 2 33
patients with diabetes can significantly improve quality ofcare. Furthermore, using data that reports care quality at theclinic level enables providers to assess and improve theirperformance, compared with benchmarks and subsequentlyto set care quality goals, both of which are useful in pay-for-performance programs and regional health informationorganizations. Results similar to Joslin’s have been foundwith the use of diabetes registries in several other clinicalsettings, including the Pennsylvania State Diabetes Center4
and the Mayo Clinic,5,6 with the key elements for successfulimplementation being linkage to clinical guidelines; real-timeavailability of decision support; ability to provide accurate,
usable outcomes reports; ease of use; and acceptance by providers.
About the Authors
Karen Golden Russell, MA, MBA, is responsible forbusiness development and marketing for Joslin’s StrategicInitiatives division.
James L. Rosenzweig, MD, is an Assistant Professor atHarvard Medical School and is Chairman of Joslin DiabetesCenter’s clinical oversight committee, which is responsiblefor developing and maintaining Joslin’s clinical guidelines.
References1. Kenny SJ et al. Survey Physician Practice Behaviors Related to Diabetes Mellitus in the U.S.: Physician Adherence to Consensus Recommendations.
Diabetes, 1993; 16:1507-1510.
2. To view Joslin Diabetes Center’s Clinical Guidelines, go to http://www.joslin.org/managing_your_diabetes_joslin_clinical_guidelines.asp
3. Health Plan Employer Data and Information Set (http://www.ncqa.org/programs/hedis/)
4. Gabby, R et al. Critical Features for a Successful Implementation of a Diabetes Registry. Diabetes Tech Ther 2005;7:958-967.
5. Stroebel RJ et al. A Randomized Trial of Three Diabetes Registry Implementation Strategies in a Community Internal Medicine Practice. Jt Comm JQual Improv 2002: 28:441-450.
6. Dinneen SF et al. Towards an Optimal Model for Community-based Diabetes Care: Design and Baseline Data from the Mayo Health SystemDiabetes Translation Project. J Eval Clin Pract 2000 Nov;6(4):421-9.
C E O s • C F O s • C I O s • C M I O s • C N O s • C N I O s • H E A LT H C A R E L E A D E R S • C L I N I C I A N S • S U P P L I E R S • I T C O N S U LTA N T S
SAN DIEGO MARRIOTT HOTEL AND MARINA
WWW.HIMSSSUMMIT.ORG
• Network with a who’s who of healthcare IT leaders from key organizations around the country
• Choose from four focused education tracks that present a unique opportunity to discuss essential issues: Governance Structure, Leadership Skills, Technology, EMR
• Get the solutions based education you need
• Visit vendor solution sessions provided by leading healthcare IT suppliers
REGISTER TODAY!