Embed Size (px)
Citation preview
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
1
NUKA System of Care Training Module
Improving Access
(Advanced Access Module)
1. MISSION, VISION, KEY POINTS, OPERATIONAL PRINCIPLES, CORE
CONCEPTS
2. ORGANIZATIONAL OVERVIEW
3. NUKA SYSTEM BACKGROUND
4. INTRODUCTION
5. THREE MODELS OF ACCESS
Traditional
First Generation Open Access
Second Generation Open Access
6. SIX ESSENTIAL ELEMENTS TO IMPLEMENT ADVANCED ACCESS
Match Demand and Supply
Reduce Backlog
Simplify Appointment Types and Times
Create Contingency Plans
Reduce Demand for Unnecessary Visits
Optimize the Care Team
7. LEADERSHIP INVOLVEMENT
8. IMPACT AND EFFECTIVENESS
Outcome Measures
Balancing Measures
9. SUMMARY OF ACCESS EVOLUTION AT SCF
10. MAINTAINING THE GAINS
11. OPEN ACCESS FROM CUSTOMER-OWNER PERSPECTIVE
12. OPEN ACCESS FROM EMPLOYEE PERSPECTIVE
How Employee Behavior Influences Advanced Access
13. CONCLUSION: KEY POINTS AND LESSONS LEARNED
14. RESOURCES
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
2
OBJECTIVES
This module is designed to enable you to:
Understand the three models of access
Understand the essential elements to implement advanced access
Understand the access evolution at SCF
Understand Customer-owner and employee perspectives on advanced access
Describe advanced access effectiveness
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
3
1. Mission, Vision, Key Points, Organizational Profile, Core Concepts
Vision Statement
A Native Community that enjoys physical, mental, emotional and spiritual wellness.
Mission Statement
Working together with the Native Community to achieve wellness through health and related services.
Key Points
Shared Responsibility Commitment to Quality Family Wellness
We value working together with
the individual, the family, and the
community. We strive to honor
the dignity of every individual.
We see the journey to wellness
being traveled in shared
responsibility and partnership
with those for whom we provide
services.
We strive to provide the best
services for the Native
Community. We employ fully
qualified staff in all positions and
we commit ourselves to
recruiting and training Native
staff to meet this need. We
structure our organization to
optimize the skills and
contributions of our staff.
We value the family as the heart
of the Native Community. We
work to promote wellness that
goes beyond absence of illness
and prevention of disease. We
encourage physical, mental,
social, spiritual & economic
wellness in the individual, the
family, the community and the
world in which we live.
Operational Principles
Our operational principles provide guidance from customer-owners when improving systems and/or
developing new programs or services. We believe that multi-dimensional wellness can only occur by
effectively in a relationship based system of care designed by and for the customer-owner when, where,
and how they want it.
Relationships between the customer-owner, the family, and provider must be fostered and
supported
Emphasis on wellness of the whole person, family, and community including; physical, mental,
emotional, and spiritual wellness
Locations that are convenient for the customer-owner and create minimal stops for the customer-
owner
Access is optimized and waiting times are limited
Together with the customer-owner as an active partner
Intentional whole system design to maximize coordination and minimize duplication
Outcome and process measures to continuously evaluate and improve
Not complicated but simple and easy to use
Services are financially sustainable and viable
Hub of the system is the family
Interests of the customer-owner drive the system to determine what we do and how we do it
Population-based systems and services
Services and systems build on the strengths of Alaska Native cultures
Core Concepts
Work together in relationship to learn and grow
Encourage understanding
Listen with an open mind
Laugh and enjoy humor throughout the day
Notice the dignity and value of ourselves and others
Engage others with compassion
Share our stories and our hearts
Strive to honor and respect ourselves and others
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
4
2. Organizational Overview
Southcentral Foundation (SCF) is an Alaska Native non-profit health care organization
established in 1982 by Cook Inlet Region, Inc. (CIRI), one of thirteen Alaska Native
regional corporations created by Congress in 1971 under the terms of the Alaska Native
Claims Settlement Act. CIRI established SCF to improve the health and social conditions
of Alaska Natives, enhance culture, and empower individuals and families to take charge
of their lives. SCF provides a wide range of health and human services to Alaska Natives
and American Indians living in south central Alaska. In general, services are provided
prepaid, based on legislative agreements and funding requirements, to members of 229
federally recognized tribes. Revenue sources include federal, state, and local
governments; private foundations; third-party payors.
SCF has grown dramatically in the past fifteen years—the workforce from fewer than
100 to about 1,500 employees, the operating budget from $3 million to $181 million.
While managing nearly three decades of exponential growth, SCF has distinguished itself
as one of the nation’s leading care providers for Alaska Natives and American Indians.
SCF provides a broad spectrum of health and health related services to support customer-
owners and their families on the journey to wellness including medical dental and
behavioral health care. When advanced and complex care is required, SCF provides a
seamless continuum of care by working in partnership with the Tertiary and Specialty
Medical Services Division of the Alaska Native Tribal Health Consortium (ANTHC),
with which SCF jointly owns and manages the Anchorage-based Alaska Native Medical
Center (ANMC).
Most SCF customer-owners live near Anchorage, home to the Anchorage Primary Care
Center (PCC), ANMC, and other SCF facilities and services. Care delivery mechanisms
include ambulatory office visits (individual, group, and peer), home visits, email and
telephone visits, health information and education (classes, paper, Web), inpatient
hospital services, day and residential treatment, as well as consultation with and referral
to higher levels of care. Some live in remote villages, most of which lack access to the
road system and are accessible only by air. SCF clinical teams regularly travel to these
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
5
villages to deliver family medicine, dentistry, and optometry services to these customers.
Where village clinics are in place staffed by local village health aides, SCF clinicians also
make use of electronic communication, including state-of-the art telemedicine
technology, to consult on assessment and treatment. In some cases, appropriate treatment
requires SCF to bring customers from rural villages to Anchorage.
3. NUKA SYSTEM OVERVIEW
Nearly 30 years ago, Alaska Native leadership set forth to create a health care system that
would empower Alaska Native people to take control of our health. The Southcentral
Foundation Nuka System of Care, as it is known today, has experienced many
successes—both in improved health outcomes and climbing satisfaction rates.
In an age where health care is a hot topic in nearly every household, and billions of
dollars are spent worldwide to address reform issues, these successes have been
noticed—causing health reform groups, Indian Country leaders and international
governments alike to ask, just what’s so special about Nuka?
The Southcentral Foundation Nuka System of Care is a name given to the whole health
care system created, managed and owned by Alaska Native people to achieve physical,
mental, emotional and spiritual wellness. It is a system that includes all parts of the
organization—including behavioral, dental, medical and traditional services—and all the
systems, processes and departments supporting the service delivery. Nuka is based on the
core concepts of creating effective relationships to improve health, customer and
employee satisfaction, and operational effectiveness.
“The name came from my children,” said SCF President/ CEO Katherine Gottlieb. “They
heard the name as they grew up. It is a name given to strong, giant structures and living
things, mountains and polar bears. My children gave this name to our puppy of fifteen
years. When we were looking for a name, something meaningful, Nuka came up, he was
in the room, when we were mulling it over. I have an association with this name that
relates to SCF – it is not about a puppy – it is about Love – it is an association with a
deep, long relationship with a living, breathing thing that has life.”
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
6
The Nuka System of Care has a long history. When Alaska Native and American Indian
people assumed ownership of our health care services from the federal government, the
Native health system in south central Alaska entered a period of tremendous reform.
In the Indian Self-Determination and Education Assistance Act of 1975, Congress
recognized Native people could more effectively improve our health statistics if we
managed our own health care services. As such, SCF was created in 1982 under the tribal
authority of Cook Inlet Region, Inc., with the mission of “Working together with the
Native Community to achieve wellness through health and related services.”
Leadership began by asking what we wanted in a health care system. What were our
health priorities? How did we want to experience health care services? And how was that
different from what we had been accustomed to?
“It matters to me what happens to my children and my children’s children,” said Gottlieb.
“So every day I ask myself, customer-owners and the employees of SCF, ‘If you could
design a health care system for you and your family, what standards would you set?
Would you accept only the best, or would you settle for less?’”
The feedback from these questions caused a profound shift in the focus of health care.
Leaders acknowledged health care as more than diagnosis and treatment—it’s about
people and human interactions. And at the core of human interactions are relationships.
“If I understand you more, you might in turn understand me more,” said Gottlieb. If you
build relationship with me, then I might in turn become even more successful…in health
and wellness.”
Relationships allow for a better understanding of each other. Relevant to health care,
relationships provide insight into what drives decisions outside of the doctor’s office—
whether to eat healthy, drink too much, exercise, smoke, and so on. Trusting relationships
allow providers and patients to work together to address health in the context of the
patients’ lives, values and beliefs—resulting in more effective health changes over time.
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
7
The Nuka System of Care is built on a set of core principles that prioritize the
establishment of relationships—relationships among employees and relationships
between customers-owners and providers. Shifting the focus of health care from pill and
procedure prescription to the cultivation of trusting relationships has transformed the way
health care services are structured and delivered.
A fundamental change was made putting the people who receive care into the driver’s
seat. SCF stopped using the term “patient,” and replaced it with “customer-owner,”
denoting a more active role in the health care process. As Alaska Native people, we are
customers of our health system, deserving of respect and high-quality services. We are
also the owners, which comes with a set of responsibilities to make informed choices and
to sustain what we have built.
Part of ownership is to help set health priorities. Alaska Native people experience some
of the most devastating health statistics in the country. Nuka aims to address what our
communities have identified as precedent issues: domestic violence, suicide, cancer,
diabetes, obesity, heart health, substance abuse and dental care.
Alaska Native people understand the mind, body and spirit are connected. Physical,
mental, emotional and spiritual health is intertwined—attention to all aspects is necessary
for wellness. As such, our system connects customer-owners to comprehensive services,
including behavioral health, primary care and medical, dental, traditional and
complementary services.
Nuka’s ability to do more with less has caught the attention of groups around the world.
SCF has been asked to partner with groups from New Zealand, England, China, Sweden,
Norway, Australia and Scotland, among many others. And the list continues to grow.
Organizations around the world have realized Alaska Native people are on to
something—and many of them show willingness to invest their time and resources in
learning from us.
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
8
While outside interest proves valuable, there is a much larger significance to what has
happened in the past three decades. We have turned conventional health care on its head
to establish a system designed by Alaska Native people for Alaska Native people. We
have found our voice once again. And as we continue to speak up to effect change, we
can feel confident we are moving in the right direction.
This training module is designed to provide information and guidance on one component
of a total system transformation. This is only part of our story. For more information
please visit our website at http://www.scf.cc/nuka/index.ak
4. INTRODUCTION
Customer-owners (C-O) gave SCF feedback on the health care they were receiving when
they answered a pivotal survey in 1998. One of the most frequent complaints was the
wait time to access care. It was clear that the system was broken: C-O complained about
the 4-6 week wait required for a primary care appointment; the emergency room was
stressed beyond capacity accommodating C-Os with primary care issues that could not be
postponed.
C-Os not only wanted better access; 89 percent of C-Os surveyed indicated that they
wanted a primary care provider, with whom they could establish a respectful, long-term
relationship. SCF realized it was essential to address not just access to primary care, but
access to specific providers. SCF used the C-O’s input as a guide in redesigning the
primary care system into a relationship-based system driven by C-Os, launching projects
to improve access while also establishing C-O panels and implementing panel
management.1
1 This footnote could cite or give brief description of the other relevant modules.
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
9
5. THREE MODELS OF ACCESS
SCF began access improvement by considering three different access models.
Traditional Model
In the traditional model, SCF’s approach in 1998, appointments are driven by the
provider’s schedule. A limited number of appointments are made available for each day,
and when they are filled, the appointments are gone for the day. Appointments are sorted
by urgent need and routine need. Access is poor or uneven, and appointments are
typically scheduled out for months. Overbooking is routine, with providers working long
hours in order to fit in C-Os with urgent needs. Primary care systems that use the
traditional model often refer C-Os to ER/UCC when they are over capacity. The
traditional model is the most common access model in the U.S.
First-Generation Open Access
The second model is known as first generation open access. The concept behind this
model is that there is science to the demand for urgent appointments. In this model,
appointments are either urgent or routine. Defining the demand for urgent appointments
and holding this number of appointments open each day should allow C-Os with urgent
needs to call in and be seen by their provider the same day. The flaw with this model is
that it is quite difficult to get the right number of urgent appointments held. When too
few appointments are held, overbooking results. When too many are held, resources are
wasted. Often, as more urgent appointment slots are held, routine appointments move out
farther. As routine appointments are scheduled farther and farther out, the no-show rate
increases, which further diminishes access while adding waste. Another problem of this
system is that providers are penalized for being efficient. C-Os with urgent needs are
typically booked on the schedules of efficient providers rather than those who typically
run behind, an approach that often results in a follow-up appointment later with the C-O’s
usual provider. Finally, this model promotes “black market” appointments. Many times,
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
10
urgent appointment slots are gone when the day begins because providers and nurses use
them before they become available to C-Os.
Second-Generation Open Access
The third model is called second-generation open access. In this model, appointments
are assigned in 15-minute increments according to C-O preferences, not by appointment
type. Demand and supply must be in equilibrium, and C-Os must have an identified PCP.
This model enables a C-O to call for an appointment and be seen on the same day,
regardless of the reason for the visit. (C-Os offered a same-day appointment may
schedule a future appointment if they prefer.) A study has shown that 80% of parents
would accept an appointment today for their child if offered, one and 70% of adults
would accept an appointment today if offered. All PCPs must see their C-Os if they are
present in clinic. If the PCP is not present, another provider is scheduled to cover that
PCP’s C-Os. The concept behind this model is that all of today’s work is completed
today. There are no overflow mechanisms for the second generation open access model
because there is no need for overflow. The providers are responsible for their panel of
C-Os. This type of access model will fail if C-Os do not have (assigned or chosen)
primary care providers. This system will also fail if the demand for services exceeds the
capacity of the system.
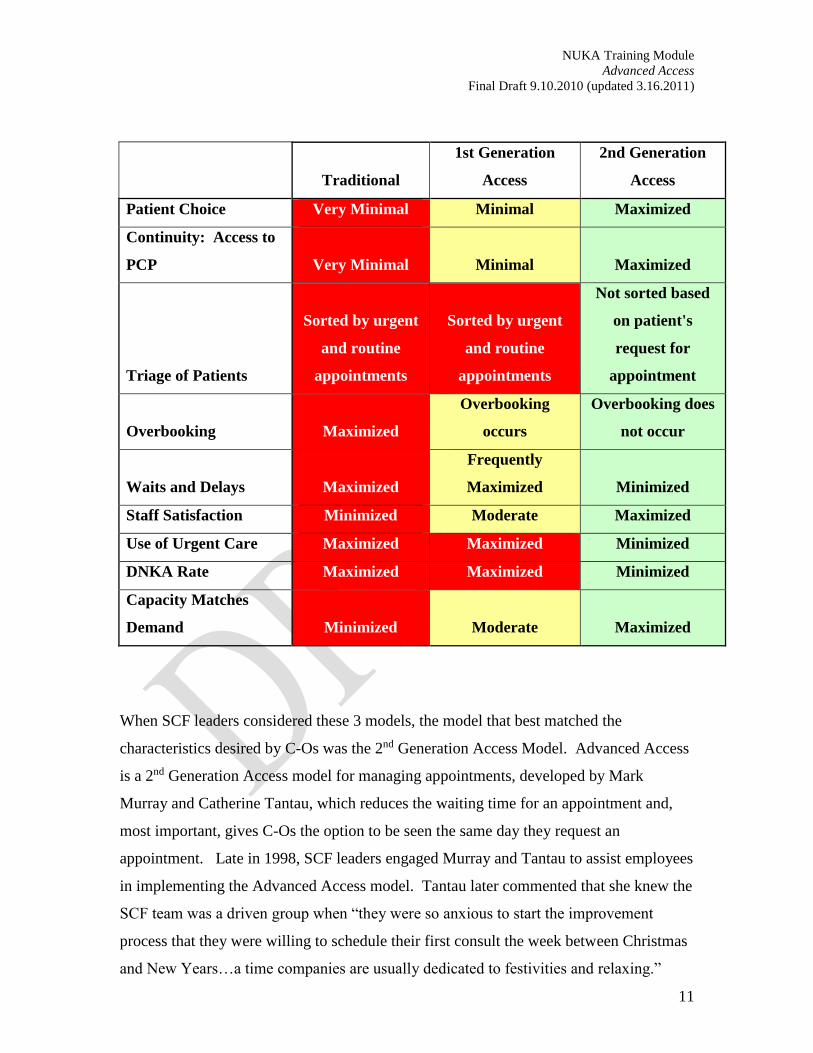
Table X. This table outlines the common features of access models and compares the
ability of these 3 models to achieve the listed features.
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
11
Traditional
1st Generation
Access
2nd Generation
Access
Patient Choice Very Minimal Minimal Maximized
Continuity: Access to
PCP Very Minimal Minimal Maximized
Triage of Patients
Sorted by urgent
and routine
appointments
Sorted by urgent
and routine
appointments
Not sorted based
on patient's
request for
appointment
Overbooking Maximized
Overbooking
occurs
Overbooking does
not occur
Waits and Delays Maximized
Frequently
Maximized Minimized
Staff Satisfaction Minimized Moderate Maximized
Use of Urgent Care Maximized Maximized Minimized
DNKA Rate Maximized Maximized Minimized
Capacity Matches
Demand Minimized Moderate Maximized
When SCF leaders considered these 3 models, the model that best matched the
characteristics desired by C-Os was the 2nd Generation Access Model. Advanced Access
is a 2nd Generation Access model for managing appointments, developed by Mark
Murray and Catherine Tantau, which reduces the waiting time for an appointment and,
most important, gives C-Os the option to be seen the same day they request an
appointment. Late in 1998, SCF leaders engaged Murray and Tantau to assist employees
in implementing the Advanced Access model. Tantau later commented that she knew the
SCF team was a driven group when “they were so anxious to start the improvement
process that they were willing to schedule their first consult the week between Christmas
and New Years…a time companies are usually dedicated to festivities and relaxing.”
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
12
SCF leaders recognized that only by improving access and offering C-os the PCP of their
choice would it be possible for C-Os to build ongoing, long-term relationships with their
PCPs. They also recognized that cooperation and commitment from PCPs and other
employees were essential to implementing the Advanced Access model. As a result,
leaders brought PCPs into the discussions with the consultants early in the process, to
encourage their input and build their buy-in. SCF leaders and physician leaders from the
Family Medicine, Pediatric, Urgent Care, and Women’s Health departments met with the
consultants to brainstorm on how to organize the clinics to offer the best flow for
customers. They determined that the best arrangement would be to make the PCP in
Family Medicine or Pediatrics the C-O’s primary access point and utilize Women’s
Health practitioners as specialists as needed. This model was then proposed to C-Os for
approval before progressing.
Once C-Os had given their approval to proceed with the redesign, SCF hired the first
project manager to coordinate the empanelling* and Advanced Access projects
simultaneously. (See Empanelling Module for more information)
6. SIX ESSENTIAL ELEMENTS TO IMPLEMENT ADVANCED ACCESS
Successfully implementing and sustaining advanced access depends on matching demand
for appointments with provider capacity to offer appointments. There are six ”high-
leverage changes” requirements advised (Murray & Tantau, 2000) for a successful
implementation of advanced access.
1. Match demand and supply
2. Reduce backlog
3. Simplify appointment types and times
4. Create contingency plans
5. Reduce demand for unnecessary visits
6. Optimize the care team
Match Demand and Supply
In order to establish the demand for the primary care clinics at SCF, the employees used a
basic tick sheet that counted any request for an appointment. All clinic employees in

NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
13
both the front and back office made a tick mark on their sheet for all appointment
requests made in person, by phone and fax. The tick sheets were collected weekly and
tallied to determine the demand patterns. This was done for one week and evaluated. If
there was a concern that the week did not represent the usual, the process was done again
for another week. This process was completed no more than 3 times over 3 one week
periods.
Once the demand for appointments was determined, the employees looked at the supply
level by calculating the amount of hours per week each provider was available. The
calculation for doing this was counting all leave time, meeting time and administrative
time and deducting this time from the hours available to manage their panel. This
number was then matched with the number of visit slots available during the open hours
of the clinic.
It was determined that the supply and demand was in equilibrium for SCF primary care
clinics. SCF also noted that they had ‘hidden capacity’ in the system when they looked at
the “DNKA rate” (Did not keep appointment). The DNKA rate before the access project
started was about 30% which revealed that there was 30% more capacity in the system if
the appointment time could be matched to the C-O’s needs. At this point, the SCF
Leadership team was confident the Advanced Access model could be successfully
implemented if the backlog could be addressed.
Reduce Backlog
Backlog refers to the length of delay until a routine appointments slot is available. The
amount of backlog at SCF was 1-1 ½ months when Advanced Access began. In order to
reduce the backlog, the clinic employees had to take care of all of the work already on
their schedules and complete the work that was being scheduled each day as overbooks.
Working down the backlog is hard work. Leadership must be present and available to
employees to provide support and encouragement. Also, it is critical that the backlog
plan has a timeline when it will begin and end.
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
14
The employees were given guidance on ‘working down the backlog’ that included adding
five “overbook” spots in the schedule, addressing customer needs by phone, max-packing
the encounter, adding ‘Saturday clinic’ capacity until the backlog was eliminated and
huddling as a team to anticipate the needs of the customers on the schedule to offer
efficient care. These guidelines for reducing the backlog eventually became best practices
for the Integrated Care Teams (See ICT Module for more information).
When SCF began the Advanced Access implementation, the “DNKA” (Did Not Keep
Appointment) rate was 30%. After 10 years of offering Advanced Access to customers,
the DNKA rate dropped to 10%. The decrease is attributed to the fact that customers are
more likely to make it to an appointment scheduled the same day versus an appointment
made more than one month in advance.
Reducing the backlog took approximately 2 months in each primary care clinic that
implemented this model. Employees were given the flexibility to work overtime to add
capacity to their day to address their newly empanelled C-Os and support the provider in
clinic. Certified Medical Assistants stayed late until the provider was finished seeing
C-Os in clinic and the case manager worked extended hours to address needs of C-Os
that didn’t present for appointments. Much of the work that the case managers addressed
were issues that previously would have landed on the provider’s desk (such as medication
refill requests, customer calls from the village or DME needs) to sort through “after
hours”. As the ICT learned skills to address work together, they started to see how
efficiently they could be as a team. (Refer to the Integrated Care Team Module for more
information).
“It’s over a decade ago and I still remember the Clinic Director and VP walking through
with an ice cream cart to reward our extra effort and thank us for our investment in being
a part of the system’s redesign. I appreciated that management noticed our hard work!”
– RN Case Manager
Reducing the Variety of Appointment types
Developing Contingency Plans for Unusual Circumstances
“
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
15
Decrease the appointment types and times
Multiple “place holders” in a schedule for varying appointment types automatically limits
when a C-O can have an appointment. Before the redesign, SCF had appointment types
such as Prenatal, Followup, New Patient, and Well Child Checks. If a C-O requested a
prenatal appointment on a day that no longer had the pre-natal slot(s) available,
employees scheduled the C-O in an appropriate slot at a later date. SCF eliminated the
variety of appointment types, creating a blank slate of 15-minute scheduling slots.
Scheduling guidelines (need reference) were established to allow for appointments
typically requiring a longer time. Schedulers received training and scripting (need
reference) and training to ensure consistent use of the guidelines.
Create Contingency Plans
Anticipating as many staffing challenges as possible puts a facility in proactive mode
versus reactive chaos. To do this, SCF looked at their staffing needs, established a
“minimum staffing” levels and made contingency plans for situations likely to arise on
occasion. Anticipating provider absences for training along with planned and unplanned
leave is a necessity for uninterrupted clinic function. SCF established a plan for absent
provider coverage and the plan have morphed over the decade to accommodate the
system’s changes and staff growth.
For example, SCF considered how best to address providing essential training in a short
time. When SCF implemented its provider-specific customer-care training, access was
maintained by using coverage employees to cover absences from clinic for the duration
of the training. Another bottleneck issue to address was how to accommodate coverage
when a PCP was out of clinic. Initially when a provider was not in clinic the other
providers shared the responsibility to see the absent providers C-Os. This presented an
extra burden on providers still getting proficient at managing their panel of C-Os and was
a challenge to schedulers who were required to evenly distribute C-Os across all the
providers on the team regardless of how full each provider was. Coverage then evolved
to SCF implementing “coverage providers,” who were responsible for a panel half the
average size and for seeing C-Os of absent PCPs. As the clinic grew, the coverage
provider position transitioned further; today, coverage providers have no panel

NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
16
responsibility making them fully available to C-Os of absent PCPs. Typically a
coverage provider is a Physician’s Assistant or a Nurse Practitioner.
Reduce demand for Unnecessary Visits
SCF was encouraged to examine their workflow and identify inefficiencies to determine
how C-O needs could be addressed in a variety of ways while maintaining
uncompromised care. It was determined that C-Os were visiting the system in excess of
10-12 visits a year on average to address needs. Upon further evaluation, there were
multiple issues that could be contributing to the high visit count for C-Os. These issues
included limited continuity of care leading C-Os to be invited back for tests and visits to
better familiarize a provider with the person’s needs, providers ‘holding drugs as hostage’
meaning chronic prescriptions would only be extended for a short duration to ensure the
C-O would return for a follow up such as a blood pressure check or a blood draw,
providers establishing a short follow up duration to ‘check on the C-O’s status’ since
there was limited case management available and multiple visits seemed to be a means to
increase C-O comfort level since this was often the only method C-Os could rely on to
validate that ‘their needs were on somebody’s radar’.
This evaluation led the SCF team to address issues of continuity, healthy panel
management strategies and learn how to offer more connections between employees and
C-Os for needs that did not require an appointment with a provider. (Refer to ICT
Module for more information)
Optimize the Care Team
Depending on the provider to address all C-O needs is a rate limiting step and is
frustrating to both the C-O and the employees. Putting a care team in place to offload
appropriate work from the provider and match it with a team member uniquely qualified
to address the need is rewarding for the employees and more efficient and timely for the
C-O. This step frees clinical empoyees to focus on clinical work and administrative
employees to concentrate on work that lends to efficient office practices.
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
17
SCF had each team member list the tasks or processes that occupied their day and assign
a percentage to each task regarding the amount of the work day that was required to
complete them. Once the lists were analyzed, work flow was redistributed to available
employees as qualified members were available to the team. For example, the provider
was able to hand follow up needs to the RN Case Manager to address with the C-O
instead of the provider automatically requesting a follow up visit just to ensure someone
was checking on the C-O’s status. As roles were redefined, training was made available
so the team members could perform to new expectations.
In the initial rollout of advanced access, the care team was made up of a PCP, 0.5-1 RN
Case Manager, 1 Certified Medical Assistant (CMA) and 0.25-0.5 Case Manger Support
(CMS). As customer needs were reevaluated and staff input was collected, staff were
added to equal the current team of 1 PCP, 1 RN Case Manager, 1 CMA, 1 CMS, 0.25
Behavioral Health Consultant, 0.15 Dietician. (See ICT Module for more information)
7. LEADERSHIP INVOLVEMENT
Communication
SCF leaders used ongoing communication and visible support to inspire and encourage
employees throughout the implementation of advanced access, particularly the backlog-
reduction phase. Leaders developed a strategy to communicate plans, give employees
predictions and assumptions about the work ahead, answer questions, and provide
updates on how the process was going. They predicted that each clinic would take three
months to reduce the backlog before reaching the maintenance phase. Leaders
intentionally extended the proposed duration of the backlog phase in case unanticipated
roadblocks became evident. As it turned out, employees were inspired because they
succeeding in moving faster than leaders anticipated. Leaders kept employees informed
by holding weekly meetings to give updates on the backlog data.
Leadership Presence and Encouragement
Since the backlog-reduction phase is the hardest to navigate in the implementation of
advanced access, SCF leaders made a special point of recognizing the hard work of the
employees. In addition to weekly updates, appropriate leaders walked through the clinic
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
18
daily to give encouragement and reward hard work. Leaders began by polling the
employees to gather their ideas about what would encourage them. Based on this
feedback, leaders responded with food and a “walking masseuse” who came through the
clinic to provide chair massages for employees. Instead of delegating the food delivery to
assistants, the VP and manager took the food items through the clinic to offer kudos and
encouragement to the employees including breakfast treats, afternoon snacks, and on a
hot day, they pushed an ice cream cart through the clinic.
8. IMPACT AND EFFECTIVENESS
To evaluate progress towards achieving same-day access and to monitor the status of
access over time, SCF selected and implemented a set of outcome and balancing
measures. This offered a balanced look at how our system was performing and how it
was affecting other clinics in the system such as specialty clinics and our emergency
room. The 3rd next available metric was reviewed at least weekly with employees during
the implementation stage. The goal of zero was made clear and each team member took
an interest in their progress on this measure. Once SCF primary care clinics achieved
same day access, the new metric followed routinely was the ‘availability at 8am’ metric.
All other metrics listed below continue to be collected routinely and made available on
the SCF Datamall for all employees to access. The clinic managers will intervene with
employees if measurement results show patterns of concern.
Outcome Measures
3rd Next Available (Delay Measure): This is the average amount of time between the
day a customer makes a request for a routine appointment and the third available
appointment. The ‘third next available’ appointment is measured versus the ‘next
available’ because is a more accurate reflection of true appointment availability. For
example, an appointment may be open at the time of a request because of a
cancelation or other unexpected event. Using the 3rd Next Available appointment
eliminates these chance occurrences from the measure of availability. The goal for
this metric is to decrease the number of days to zero (same day) for Primary Care
Clinics.
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
19
Availability at 8am: Once SCF had decreased their 3rd Next Available measure to
zero, they wanted to establish a new metric to monitor their same day access. They
currently look at each provider’s schedule at 8am and measure the percentage of
appointments available for the day in each provider’s schedule. The target for this
metric is to have greater than 50% of appointments available in each provider’s
schedule.
Balancing Measures
Match-Rate (Continuity with PCP): Because C-Os voiced the desire to have both
continuity and accessibility in their healthcare, SCF needed to balance accessibility
metrics with that of continuity with the C-O’s PCP. This is measured as the
percentage of C-Os that see their PCP during their requested appointment.
Appointments at End of Day (SCF-specific measure): Because there are unlimited
overbooks allowed at the last appointment slot of the schedule, SCF monitors this
number to determine what teams are struggling with the end of day work flow. This
number is monitored so interventions can be established before burnout can occur.
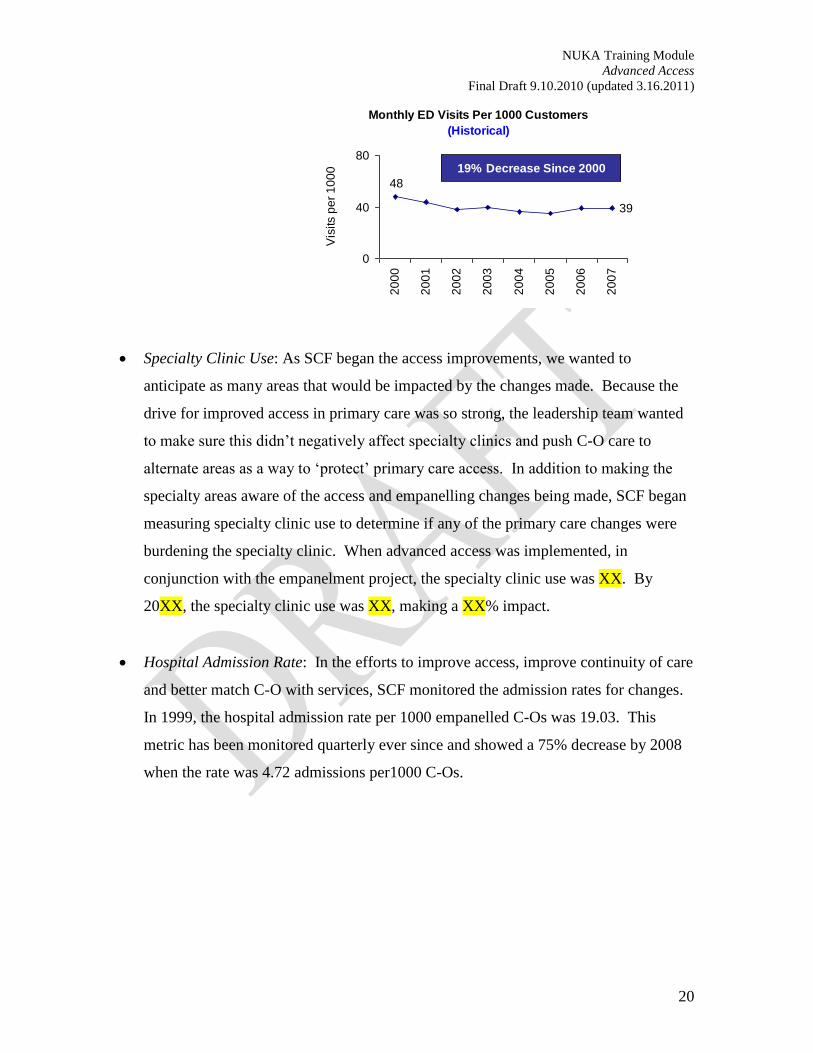
ER Use: SCF was aware that the limited access in primary care was pushing C-Os to
the ER for care. In making the efforts to improve access in primary care, SCF wanted
to measure the effect on ER use to measure what impact was being made. When the
advanced access began, in conjunction with the empanelment project, the ER use was
48 ER visits per 1000 empanelled C-Os. By 2008, the ER use has decreased to 39 ER
visits per 1000 empanelled C-Os, resulting in a 19% decrease in ER visits in that time
period.
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
20
Monthly ED Visits Per 1000 Customers
(Historical)
39
48
0
40
80
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
Vis
its p
er
10
00 19% Decrease Since 2000
Specialty Clinic Use: As SCF began the access improvements, we wanted to
anticipate as many areas that would be impacted by the changes made. Because the
drive for improved access in primary care was so strong, the leadership team wanted
to make sure this didn’t negatively affect specialty clinics and push C-O care to
alternate areas as a way to ‘protect’ primary care access. In addition to making the
specialty areas aware of the access and empanelling changes being made, SCF began
measuring specialty clinic use to determine if any of the primary care changes were
burdening the specialty clinic. When advanced access was implemented, in
conjunction with the empanelment project, the specialty clinic use was XX. By
20XX, the specialty clinic use was XX, making a XX% impact.
Hospital Admission Rate: In the efforts to improve access, improve continuity of care
and better match C-O with services, SCF monitored the admission rates for changes.
In 1999, the hospital admission rate per 1000 empanelled C-Os was 19.03. This
metric has been monitored quarterly ever since and showed a 75% decrease by 2008
when the rate was 4.72 admissions per1000 C-Os.

NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
21
Qrtly Hosp. Admissions Per 1000 Customers
(Historical)
19.03
4.72
0
10
20
1999
2000
2001
2002
2003
2004
2005
2006
2007
Adm
issi
ons
per 1
000
75% Decrease Since 1999
9. SUMMARY OF ACCESS EVOLUTION
The SCF started the journey to improve access with characteristics ripe for change.
Although the system was broken in many places, C-Os were willing to give their input
and employees were willing to offer something exceptional. Surveys, focus groups and
interviews were held to gather C-O input and employees organized the feedback into an
outline to guide a redesign of the SCF system. SCF leadership drafted a plan to redesign
the system that offered empanelment for C-Os, access to an appointment the same day
the C-O requests one and an ICT to support them in their wellness journey.
An implementation timeline was created for the redesign both to organize the
improvement project and to communicate predictions for employees. Biographies of
Primary Care Providers (PCP) were created and fifteen employees were hired and trained
to connect with C-Os and assist them in empanelling to a PCP of their choice. The 15
empanelment employees were in place for 2 years and currently the empanelment
responsibilities are maintained with 3 full time employees. Panel sizes were set, backlog
was measured and supply and demand was determined. Metrics were chosen to monitor
improvement progress. Restrictions were placed on leave requests during the backlog
reduction phase so that only emergency leave was approved in the attempt to honor a
commitment to C-Os to implement improved access in a timely manner.
Advanced access and empanelling was offered in Family Medicine first and then in
Pediatrics about 6 months later. Hospitalist positions were implemented so that PCPs are
able to focus solely on their panel of C-Os in the primary care. This step was taken
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
22
because predictions were made that it would be difficult to maintain access for C-Os if a
PCP was dividing their time between primary care and inpatient responsibilities.
ICT roles were defined as a unit and for each discipline and piloting of a case manager
support role began to shift administrative responsibilities from the clinical employees on
the team. This pilot was so successful that the ratio of CMS to teams has progressed
from 1:5 to 1:1 over the years. Training was provided for administrative employees on
the overall mission of the redesign and now in maintenance phase in the form of scripting
and shadowing to ensure new administrative employees can offer the high level of
service expected.
In an effort to meet C-O needs, SCF looked at adjustments that could be made to
accommodate workload demands. Some areas addressed were shifting work from the
afternoon to the morning, looking at overbook options and expanding clinic hours.
Routine visits in morning hours
One strategy used to relieve the bottleneck of C-Os in the afternoon, was to encourage
C-Os to schedule follow-up appointments, well-child checks and physical exams in the
morning hours. This was not a rule or a mandate, but a means to prevent predictable
needs from conflicting with the demand of acute presentations that are usually discovered
as the day progresses.
Overbooking
Since advanced access was implemented while the empanelling project was underway,
the goal of advanced access was to decrease the wait for appointments in concert with
preserving continuity of C-Os seeing their chosen PCP. The decision was made to add
overbook slots in each of the provider’s schedules at predetermined times so there was
continuity in scheduling.
Previous to the advanced access, FMC was defined with a “West” and an “East” side.
Since all the scheduling was done by one small group of administrative support staff, a
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
23
single overbook scheduling template for scheduling consistency and error-reduction.
Due to the expected backlog reduction challenges and the importance of employee buy-
in, SCF leaders chose to give both sides the liberty to define where they wanted 5
overbook slots to be located in addition to the unlimited overbooks at the end of day.
One side chose to have their overbook slots at 10:15am, 11:15am, 1:15pm, 2:15pm and
3:15pm and one side chose to have their overbook spots at 1:15pm, 2:15pm, 3:15pm,
4:00pm and 4:15pm. After acknowledging the afternoon demand was greater than the
morning, the clinic determined it would position all of it’s overbook spots in the
afternoon and currently offers overbook spots at 1:15pm, 2:15pm, 3:15, 4pm and
unlimited overbooks at 4:30pm.
Expanded hours
SCF noticed a pattern of an increased demand for appointments in the afternoon. To
address this, overbook slots were added and coverage providers were made available on a
staggered shift. Although most providers offered clinic hours of 8:00 a.m. to 4:30 p.m.,
the primary care clinic made later appointments available to C-Os by having some
providers work from 10:00 a.m. to 6:30 p.m. and then another shift from noon to 7:30
p.m. In addition to expanding the hours that appointments were available in a work
week, SCF choose to add Saturday hours to increase access for their C-Os.
Scheduling PCPs and coverage providers has evolved over the years starting with all
PCPs covering for absences of co-workers to current which has dedicated coverage
providers that do not have a panel. Monday through Friday clinic hours have changed
from 8 am to 8 pm to having more slots available 8 am to 6:30 pm Monday through
Friday. This occurred by permanently changing the coverage providers schedule to 9:30
am to 6:30 pm every week day. This change occurred to address provider dissatisfaction
over having such late evenings on their evening shift and that they were not seeing the
C-Os on their panel on this shift. There continued to be more demand for appointments
later in the day and that evening clinic was more for convenience than continuity for
C-Os and more about urgent care needs than routine health issues. PCPs are still
expected to offer an evening clinic (9:30am-6:30pm) once a week but their shift ends 1 ½
hours earlier than the previous evening template. Saturday clinic is offered from 8 am –
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
24
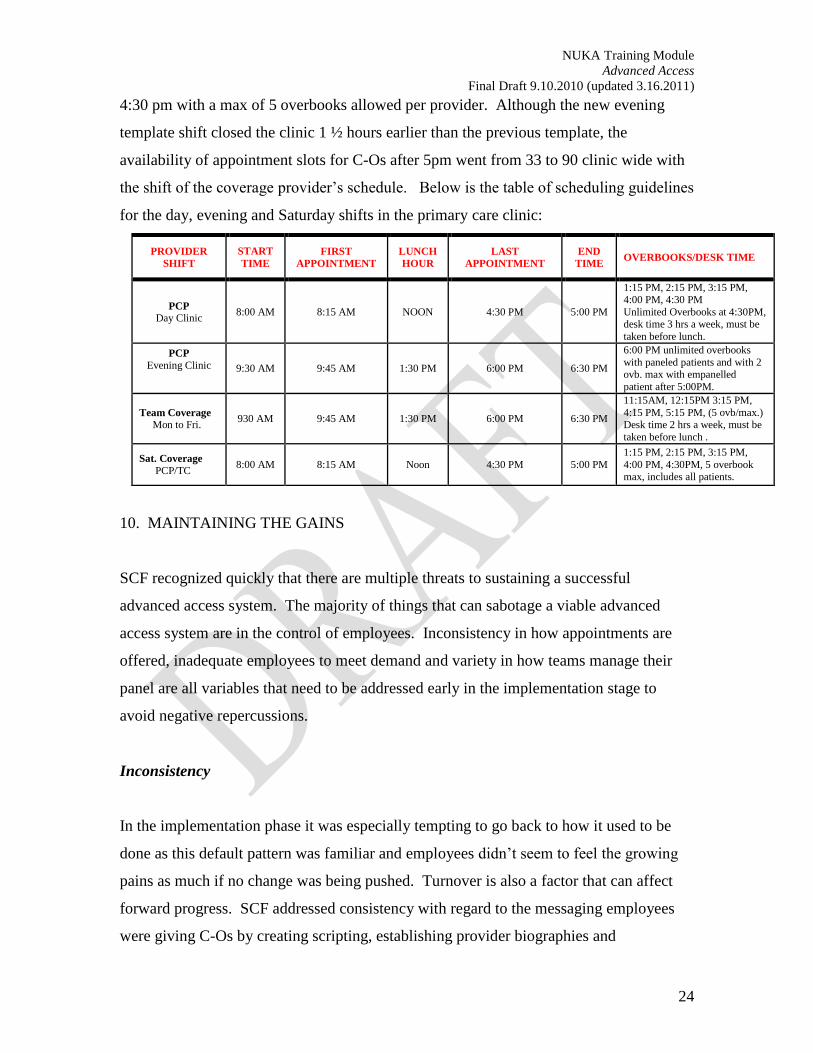
4:30 pm with a max of 5 overbooks allowed per provider. Although the new evening
template shift closed the clinic 1 ½ hours earlier than the previous template, the
availability of appointment slots for C-Os after 5pm went from 33 to 90 clinic wide with
the shift of the coverage provider’s schedule. Below is the table of scheduling guidelines
for the day, evening and Saturday shifts in the primary care clinic:
PROVIDER SHIFT
START TIME
FIRST APPOINTMENT
LUNCH HOUR
LAST APPOINTMENT
END TIME OVERBOOKS/DESK TIME
PCP Day Clinic 8:00 AM 8:15 AM NOON 4:30 PM 5:00 PM
1:15 PM, 2:15 PM, 3:15 PM, 4:00 PM, 4:30 PM Unlimited Overbooks at 4:30PM, desk time 3 hrs a week, must be
taken before lunch. PCP
Evening Clinic
9:30 AM 9:45 AM 1:30 PM 6:00 PM 6:30 PM
6:00 PM unlimited overbooks
with paneled patients and with 2 ovb. max with empanelled
patient after 5:00PM.
Team Coverage Mon to Fri. 930 AM 9:45 AM 1:30 PM 6:00 PM 6:30 PM
11:15AM, 12:15PM 3:15 PM,
4:15 PM, 5:15 PM, (5 ovb/max.) Desk time 2 hrs a week, must be
taken before lunch .
Sat. Coverage PCP/TC 8:00 AM 8:15 AM Noon 4:30 PM 5:00 PM
1:15 PM, 2:15 PM, 3:15 PM,
4:00 PM, 4:30PM, 5 overbook max, includes all patients.
10. MAINTAINING THE GAINS
SCF recognized quickly that there are multiple threats to sustaining a successful
advanced access system. The majority of things that can sabotage a viable advanced
access system are in the control of employees. Inconsistency in how appointments are
offered, inadequate employees to meet demand and variety in how teams manage their
panel are all variables that need to be addressed early in the implementation stage to
avoid negative repercussions.
Inconsistency
In the implementation phase it was especially tempting to go back to how it used to be
done as this default pattern was familiar and employees didn’t seem to feel the growing
pains as much if no change was being pushed. Turnover is also a factor that can affect
forward progress. SCF addressed consistency with regard to the messaging employees
were giving C-Os by creating scripting, establishing provider biographies and
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
25
implementing training programs for each discipline that incorporated the new way of
doing business with regards to appointment access.
Staffing
Minimum staffing levels were established for each clinic. Staffing minimums are
important so that the supply and demand of appointments for that clinic was taken into
consideration and there was a limit established on how many providers could be out of
clinic at one time. Respecting these guidelines when approving or denying leave requests
for employees prevented the system from collapsing due to inadequate supply being
available.
Panel Management Variety
The way employees manage (or mismanage) their panels can have a profound impact on
their access. An ICT that is not organized and does not work to the top of their license
limits the team’s capacity. For example, a C-O that requires blood tests to monitor their
disease status can see their PCP annually and have their labs drawn in support clinic and
communicate results and care plan updates by phone with the C-O after the PCP reviews.
If the ICT did not have good panel management efforts, a C-O might be asked to see the
PCP whenever they were due for a lab check which diminishes the PCP’s access when
this need could have been addressed elsewhere. (Refer to ICT module for further
information).
11. OPEN ACCESS FROM THE CUSTOMER-OWNER PERSPECTIVE
C-Os came into the advanced access system with decades of history of waiting on
appointment availability, seeing inconsistent providers and camping in the E.R. for
routine care needs if they couldn’t get their needs met in a timely manner elsewhere. The
news that was circulating about improvements being made to access in primary care was
met with some disbelief since there had been no comparable redesign in the C-Os
experience. When C-Os learned that the access improvements would allow for them to

NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
26
see their chosen provider the same day they requested the appointment, there was
skepticism. If the system was ever able to offer this, how long would it last?
SCF anticipated C-O skepticism as a natural reaction and was prepared for C-Os to test
the system with requests for appointments that didn’t seem particularly necessary.
Initially C-Os were not accustomed to same day access and at times did not accept
appointments initially. This would change within 6 months as C-Os tested the system
and began to trust that they can get an appointment when they wanted one. The upside to
skeptics testing the system was that C-Os began telling family members and
acquaintances about their positive experiences of getting to see their provider when they
wanted. Not only did C-Os see a difference in how quickly they could access an
appointment, but they also noticed the attentiveness of employees to returning calls the
same day, a simple action that had gone unaddressed for too long.
“I can get an appointment when I want it and that is very important to me – many other
healthcare organizations don’t have this option. I feel in control, knowing that I won’t
have to wait for weeks or months to be seen.” – Customer-Owner
SCF used various methods to communicate the availability of same-day appointments.
These included mailings, signage in both the primary care and emergency room lobby
areas, and phone greetings with a brief summary of access changes that C-Os heard when
they called primary care.
Improvements in access provided the vehicle for enhanced relationships between C-Os
and their ICT. As C-Os became more familiar with their PCP and ICT that supported
them, they relied less on clinic visits and more on interaction by phone.
Over time, both C-Os and employees developed a new sense of their roles and
accountability as partners in a relationship-based system of care. C-Os learned that as
they began to have continuity with the ICT, they were held accountable to agreements
made in previous conversations regarding their health. If a C-O proposed increasing
exercise in order to lower blood pressure, the ICT asked follow-up questions on that
progress. At the same time, employees felt a greater responsibility to be accountable for
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
27
commitments they made to C-Os. They became more conscientious about responding to
C-O needs in a timely fashion, taking the time to get better acquainted with their C-Os,
and offering a more customized plan of care.
12. OPEN ACCESS FROM THE STAFF PERSPECTIVE
Staff Reactions to Advanced Access
When employees were introduced to the concept of improving advanced access, there
was a reaction of disbelief, panic and fear. Many employees of various disciplines
thought the idea would not work. While employees agreed that access needed
improvement, they worried about what this would mean for the staff workload.
Here are some typical reactions
“If all customers are given access whenever they want it, I’ll be here all night.”
Employees were so used to gate-keeping access, they thought that there were
more C-Os than could be accommodated in a given day. As the backlog
reduction phase ended, they realized the capacity and demand was in equilibrium
as calculated and long days could be avoided if the ICT was proactive in pre-visit
planning, huddling, and resisting the temptation to schedule follow-up
appointments for issues that could be handled by phone.
“Advanced Access will leave me with no control over my schedule.”
Advanced access does put power in the C-O’s hands with regard to getting an
appointment on the day they want. However, employees learned that they could
still influence the efficiency of the schedule by prepping forms, anticipating
needed equipment and/or interventions for the visit, calling C-Os to offer earlier
appointments if there were cancellations, and increasing communication with
teammates throughout the day.
“How will I get all of the work done today”?
A system that encourages doing the work you get today by the end of the day
must have the supply to take care of each day’s demand on the day it is generated.
In clinics with this system, the only appointments that are on the books at the

NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
28
beginning of each day are the return appointments that were generated by
physician discretion or C-O preference on a previous day. There are no frozen or
held appointment slots. This provides maximum flexibility in the system to absorb
daily demand. Doing work this way requires a commitment from every member
of the care team to see C-O who want to be seen. It also requires that supply and
demand are in balance, and that the backlog is eliminated.’2–
How Staff Behavior Influences Advanced Access
The habits of an ICT can maximize or diminish the potential of advanced access.
Healthy habits include doing all work on the same day it was generated and anticipating
work by proactively managing a panel. Pushing work to another day decreases
accessibility and diminishes the team’s ability to complete work tomorrow. Here are
some healthy habits discovered among teams that manage access best:
Maximize phone follow-ups: When a C-O is seen in the E.R. and follow-up is
requested, the ICT can follow-up by phone if appropriate and acceptable to the
C-O. For example, if the E.R. requests follow-up on a child treated for otitis
media, the Case Manager would call the child’s parent or guardian to assess the
child’s status and outline anticipated progress and appropriate timing for a follow-
up clinic visit.
Another way to utilize phone follow ups is for test results. Instead of having the
C-O come into clinic to discuss results, a phone follow-up can be used to review
results and communicate recommended next steps.
Keeping customer needs on time: Efficient ICTs utilize the datamall and
reminder systems to provide preventive health maintenance and follow-up testing
on time. Timely care is not only the responsible thing, it prevents work
accumulating in the future and an increase in the need for appointments for acute
needs.
2http://www.ihi.org/IHI/Topics/OfficePractices/Access/Changes/IndividualChanges/CommittoDoi
ngTodaysWorkToday.htm
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
29
Answer phone messages in a timely manner: If employees do not return calls to
C-Os the same day, C-Os may conclude that it is quicker to get issues addressed
in an appointment than by phone. SCF found this to be true once they had
increased their access such that C-Os would make an appointment to address their
issue when it could have easily been addressed by phone.
Stick to the script: Scripting for making appointments facilitates training staff
and helps ensure a consistent customer experience. However, scripting is also
important to preserve access and promote continuity with chosen PCPs. The staff
that respected the scripting found themselves with fewer surprises and more
appointments available throughout the day.
The following are ome habits can sabotage your access plan:
Holding Drugs Hostage: Some providers fill long term prescriptions for a
limited time forcing C-Os to phone or schedule a follow-up appointment for
renewal. They use prescription renewals a way to remind themselves to check on
C-O progress. This approach fails to utilize ICT members to the fullest potential
and limits PCP access.
Unnecessary follow-ups in clinic: Requiring frequent follow up appointments as
the main way to manage a C-O is inefficient. The C-O’s time should be respected,
and the team should work to their highest potential and outreach to C-Os via
phone as a supplement to routine clinic checkups. C-Os should not be dissuaded
from being seen in clinic if that is their choice, but requiring them to come in
when there are follow-up methods more convenient and efficient for them is
unacceptable.
13. CONCLUSION: KEY POINTS AND LESSONS LEARNED
Care that is consistently safe, effective, customer-centered, timely, efficient, and
equitable depends on C-Os having access to that care.3 Success in access redesign
requires attention to customer-driven work, leadership buy-in, employee support, and
ongoing, clear communication between management and employees.
3 Institute of Medicine, Crossing the Quality Chasm (Washington, DC: National Academy Press, 2001), p.
6.
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
30
Key Points
Customer-driven work: SCF responded to C-O requests to make improvements to a
system with broken access. Even after involving consultants, leadership and
employees to frame strategy to improve access, SCF passed the proposal before C-Os
before proceeding. If you are working to make improvements, C-O should decide the
improvements that should be made. You must check in with C-Os to make sure you
are meeting their needs. SCF uses surveys, focus groups and interviews with C-Os as
ways to get input and feedback.
Leadership support and direction: Leadership, starting with the board of directors
and CEO to the clinical managers, is crucial. Leadership support and direction helps
ensure that employees receive needed support, resources, and encouragement.
Communication: There is hard work involved in implementing advanced access and
especially when employees have no experience with the concept. Without frequent
reliable communication, employees can feel abandoned and disengaged from the
improvement process. If employees are expected to foster healthy relationships with
C-O, all employees must model that behavior internally.
Staff support: Implementing any change requires support and encouragement.
Implementing advanced access requires a strategy plan and an organized deployment.
Advanced planning for what to expect, metric gathering and updating, tools such as
scripting and schedule templates and celebrating progress is critical.
Lessons Learned
Have experts on the ground: SCF had the benefit of accessing consultants at
intervals throughout the implementation of advanced access, but did not have experts
on the ground to work side by side with employees. This approach deepened the
camaraderie of employees who recognized they were all in it together. However, the
learning curve may not have been as steep if each clinic had had a resident expert
who was accessible to trouble-shoot issues in real time.
NUKA Training Module
Advanced Access
Final Draft 9.10.2010 (updated 3.16.2011)
31
Celebrate accomplishments: SCF leadership personally walked through work areas
to give encouragement and offer food, fulfilling a specific request of employees, and
employees still remember this over a decade later.
15. RESOURCES
Murray, M., & Tantau, C. (2000). Same-day appointments: Exploding the access
paradigm. Family Practice Management, 7(8), 45-50.
Tantau, C. (2008). Improving implementation strategies for clinical innovations.
Journal of the Ambulatory Care Management, 31(2), 186-187.
IHI, http://www.ihi.org/IHI/Topics/OfficePractices/Access/