Embed Size (px)
Citation preview

Implications of the International Society of UrologicalPathology Modified Gleason Grading System
Lars Egevad, MD; Roberta Mazzucchelli, MD, PhD; Rodolfo Montironi, MD, FRCPath
N Context.—Histologic grading is the clinically most usefultissue-based predictor of prognosis for prostate cancer.Over the years, there has been a gradual shift in how theGleason grading is applied in practice, with a general trendtoward upgrading. A consensus conference was organizedin 2005 by the International Society of UrologicalPathology (ISUP) for standardizing both the perception ofhistologic patterns and how the grade information iscompiled and reported.
Objective.—To review the implications of the ISUPmodified Gleason grading system.
Data Sources.—Personal experience and review of thecurrent literature.
Conclusions.—The recommendations regarding patterninterpretation and reporting are summarized. The practicalconsequences of the ISUP modification of the Gleasongrading are reported. The prognostic importance of theGleason score, its reproducibility, and its preoperativeassessment are discussed. Subsequent proposals for slightmodifications to the ISUP grading system are described.
(Arch Pathol Lab Med. 2012;136:426–434; doi: 10.5858/arpa.2011-0495-RA)
The Gleason grading system of prostatic carcinoma is thequintessential prognostic factor in predicting findings
in radical prostatectomy, biochemical failure, local recur-rences, and lymph node or distant metastasis in patientsreceiving no treatment, radiation therapy, radical prosta-tectomy, and other therapies, including cryotherapy andhigh-intensity focal ultrasound therapy. Clinicians usevarious tools, such as Partin tables or Kattan nomograms,to predict outcomes, including the pathologic stage orprognosis following radical prostatectomy or radiothera-py. All of these tools incorporate the Gleason score.1
ORIGINAL GLEASON GRADING SYSTEM
In 1966, Donald F. Gleason, MD, PhD, first published aunique grading system for prostate cancer (PCa) based solelyon the architectural pattern of the tumor, using a 5-pointscale, where patterns 1, 2, and 3 represented tumors that mostclosely resembled normal prostatic glands, and patterns 4and 5 were tumors showing increasingly abnormal glandulararchitecture (Table 1).2,3 An innovative aspect of this system,based on a study of 270 patients, was that, rather thanassigning the worst grade as the grade of the carcinoma, thegrade was defined as the sum of the 2 most common patternsand was reported as the Gleason score.
GLEASON MODIFICATIONS
By 1974, Gleason and the Veterans AdministrationCooperative Urological Research Group expanded theirstudy of the original Gleason system to 1032 men.4 Gleasonpattern 4 was described in a figure legend as ‘‘raggedly in-filtrating, fused-glandular tumor, frequently with pale cells,may resemble hypernephroma of kidney.’’4(p60) The Gleasonsystem was further refined by Mellinger5 in 1977, when thepapillary and cribriform tumor under Gleason pattern 3was described as having a ‘‘smooth and usually roundededge.’’5(p66) In describing the breakdown of Gleason patternsamong 2911 cases, Gleason pattern 1 was seen in 3.5% ofcases, pattern 2 in 24.4%, pattern 3 in 87.7%, pattern 4 in12.1%, and pattern 5 in 22.6%.5 These percentages added upto approximately 150% because 50% of the tumors showedat least 2 different patterns.
In 1977, Gleason6 provided additional comments con-cerning the application of the Gleason system: ‘‘Grading isperformed under low magnification.’’6 He also stated that‘‘an occasional small area of fused glands did not change apattern 3 tumor to pattern 4. A small focus of disorganizedcells did not change a pattern 3 or 4 tumor to pattern5.’’6(p173) The only comment relating to tertiary patternswas ‘‘occasionally, small areas of a third pattern wereobserved.’’6(p182)
CHANGES IN PROSTATE CARCINOMA SINCE THELATE 1960s
Diagnosis of PCa has changed dramatically since thelate 1960s, when the Gleason grading system wasdescribed. In the 1960s, there was no screening for PCa,other than by digital rectal examination because serumprostate-specific antigen had not yet been discovered. Inthe Gleason4 1974 study, most men had advanced diseasewith either local extension out of the prostate on digitalrectal examination or distant metastases. Only 6% of
Accepted for publication November 17, 2011.From the Department of Pathology, Karolinska University Hospital,
Stockholm, Sweden (Dr Egevad); and Section of Pathological Anatomy,Polytechnic University of the Marche Region, School of Medicine,United Hospitals, Ancona, Italy (Drs Mazzucchelli and Montironi).
The authors have no relevant financial interest in the products orcompanies described in this article.
Reprints: Rodolfo Montironi, MD, FRCPath, Section of PathologicalAnatomy, Polytechnic University of the Marche Region, School ofMedicine, United Hospitals, Via Conca 71, I-60126 Torrette, Ancona,Italy (e-mail: [email protected]).
426 Arch Pathol Lab Med—Vol 136, April 2012 Gleason Grading System—Egevad et al

patients had a nonpalpable tumor diagnosed by transure-thral resection, and 8% of patients were diagnosed with alocalized nodule on digital rectal examination.7
The method of obtaining prostate tissue was alsodifferent from today’s practice. Typically, only a coupleof thick gauge needle biopsies were directed into an areaof palpable abnormality, usually perineally. The use of18-gauge, thin biopsy needles and the concept of sextantneedle biopsies to more extensively sample the prostatewere not developed until the 1980s.7 Consequently, thegrading of prostate cancer in thin cores and in multiplecores from different sites of the prostate were not issues inthe Gleason era.
In the 1960s, radical prostatectomy was relativelyuncommon, prostates were not as often removed intact,and glands were not processed in their entirety or asextensively and systematically as currently seen. Furtherissues relating to radical prostatectomy specimens, such asthe grading of multiple nodules within the same prostate,determining variants and variations of PCa, or dealingwith tertiary patterns, were not addressed within theoriginal Gleason system.
The Gleason system also predated the use of immuno-histochemistry. It is likely that, with immunostaining forbasal cells, many of the original Gleason 1 + 1 5 2 PCawould today be regarded as adenosis (atypical adenoma-tous hyperplasia), that is, a benign lesion.8 Similarly, manyof the cases in 1966, diagnosed as cribriform Gleasonpattern 3 carcinoma, would probably now be referred to ascribriform high-grade prostatic intraepithelial neoplasia, iflabeled with basal cell markers.9
Forty Years After the Inception of the Gleason System
Nearly 40 years after its inception, the Gleason systemremains one of the most powerful prognostic factors inPCa. In part, this system has remained timely by minoradaptations to accommodate the changing practice ofmedicine.10–12 However, certain aspects of the originalGleason system are interpreted differently in today’spractice. With such changes have come variations inapplying the Gleason system among pathologists, withsome differences by region and others dependent on other
demographic factors. For example, pathologists older than50 years diagnosed Gleason scores less than 4 on needlebiopsy more often than did younger pathologists, whowere trained to do so rarely, if ever.13 The assigning of anoverall score to needle biopsy specimens with differentgrades on different cores is more often practiced in Europethan in the United States.14
2005 INTERNATIONAL SOCIETY OF UROLOGICALPATHOLOGY MODIFIED GLEASON SYSTEM
The International Society of Urological Pathology(ISUP) convened a conference in 2005 in San Antonio,Texas, in an attempt to achieve consensus in controversialareas relating to the Gleason system (Tables 2 and 3). Thatconference led to the 2005 ISUP Modified Gleason System.15
The conference was preceded by an international consen-sus meeting, the ‘‘International Consultation on Predictorsof Patient Outcome in Prostate Cancer,’’ sponsored by theWorld Health Organization, which took place in 2004in Stockholm, Sweden.10 National groups, independentof the ISUP activities, had already started a revision ofthe Gleason system with proposals that preceded thoseincluded in the 2005 ISUP Modified Gleason System.16–18
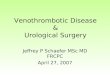
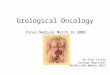
It is outside the scope of this review to describe all thefeatures included in the 2005 ISUP Modified GleasonSystem. Interested readers are referred to the confer-ence proceedings.15 The main differences between theoriginal Gleason system and the 2005 ISUP ModifiedGleason System are reported in Table 4. Below, we’veprovided a brief summary of the ISUP modifiedGleason grading system. Representative images of thevarious Gleason patterns and scores are shown in theFigure, A through F.
. The Gleason score is the sum of the primary (mostpredominant) Gleason grade and the secondary(second most predominant) Gleason grade. In needlebiopsies, this definition is modified to include anycomponent of higher grade (see below).
. A Gleason score of 1 + 1 5 2 is a grade that shouldnot be diagnosed, regardless of the type of specimen,with only rare exception.
Table 1. The 5 Architectural Patterns According to the Original Gleason Grading System
1. Very well-differentiated, small, closely packed, uniform glands in essentially circumscribed masses2. Similar to pattern 1 but with moderate variation in size and shape of glands and more atypia in the individual cells; cribriform pattern may
be present, still essentially circumscribed, but more loosely arranged3. Similar to pattern 2 but marked irregularity in size and shape of glands, with tiny glands or individual cells invading stroma away from
circumscribed masses or solid cords and masses with easily identifiable, glandular differentiation within most of them4. Large clear cells growing in a diffuse pattern resembling hypernephroma; may show gland formation5. Very poorly differentiated tumors; usually solid masses or diffuse growth with little or no differentiation into glands
Table 2. Controversial Areas of the Original Gleason Grading System Reviewed at the 2005 International Society ofUrological Pathology (ISUP) Conference
The 2005 ISUP conference attempted to achieve consensus in controversial areas relating to the Gleason grading system, including:1. General applications of the Gleason grading system2. Gleason patterns3. Grading variants and variations of acinar adenocarcinoma of the prostate4. Reporting secondary patterns of lower grade when present to a limited extent5. Reporting secondary patterns of higher grade when present to a limited extent6. Tertiary Gleason patterns7. Percentage of patterns 4 to 58. Radical prostatectomy specimens with separate tumor nodules9. Needle biopsy with different cores showing different grades
Arch Pathol Lab Med—Vol 136, April 2012 Gleason Grading System—Egevad et al 427

A, Prostate cancer Gleason score 3 + 3 5 6. Light staining glands with oval, rounded contour. This pattern would be diagnosed a decade ago bymany pathologists as Gleason pattern 2. However, the tumor shows some infiltration between the benign glands (right), and there is considerablevariation in glandular diameter and distribution, which favors a diagnosis of Gleason pattern 3. B, Prostate cancer Gleason score 3 + 3 5 6. Minimalfocus of cancer with bland features. The malignant glands infiltrate between benign glands and are irregularly distributed, which favors a grading ofGleason pattern 3. C, Prostate cancer Gleason score 4 + 4 5 8. Gleason pattern 4 of a fusion type. Glands are fused into a mazelike conglomerate.D, Prostate cancer Gleason score 4 + 3 5 7. Gleason pattern 4 of the cribriform type. These cribriform glands are too irregular for cribriform pattern 3. E,
428 Arch Pathol Lab Med—Vol 136, April 2012 Gleason Grading System—Egevad et al

. The diagnosis of Gleason scores 2 through 4 onneedle biopsies should be reported rarely, if ever(Table 5).
. Individual cells would not be allowed withinGleason pattern 3.
. Most cribriform patterns are diagnosed as Gleasonpattern 4, with only rare cribriform lesions satisfyingdiagnostic criteria for cribriform pattern 3 (see below).
. Grading variations of acinar adenocarcinoma in-clude the tumor being graded solely on theunderlying architecture (Table 6). For instance,pseudohyperplastic cancer should be assigned aGleason score of 3 + 3 5 6.
. Grading variants of adenocarcinoma include ductaladenocarcinomas, which should be graded as Glea-son score 4 + 4 5 8, whereas prostatic intraepithelialneoplasia–like adenocarcinoma should be graded asGleason pattern 3 and ductal adenocarcinoma withcomedonecrosis should be graded as Gleason pat-tern 5, retaining the diagnostic term ductal adenocar-cinoma to denote unique clinical and pathologicfindings. There is no consensus on the way mucin-ous (colloid) carcinoma should be scored. Someauthors think that all mucinous carcinomas shouldbe assigned a Gleason score of 8, whereas others saythe extracellular mucin should be ignored and thetumor should be graded on the underlying architec-tural pattern. The grading of glomeruloid glands isanother controversial area in the modified Gleasonsystem (see below). Small cell carcinoma should notbe assigned a Gleason grade. The appropriateness ofassigning a Gleason score to sarcomatoid carcinomais uncertain. In general, a Gleason grade is notassigned to the sarcomatoid component, whereas theglandular component is graded in the usual manner.
. Secondary patterns of lower-grade cancer whenpresent to a limited extent should be ignored andnot reported in the setting of a high-grade cancer andignored and not reported if they occupy less than 5%of the tumor area.
. High-grade tumor of any quantity on needle biopsyshould be included and reported within the Gleasonscore.
. For tertiary Gleason patterns, the typical situation onbiopsy includes tumors with patterns 3, 4, and 5 invarious proportions. Such tumors should be classi-fied overall as high grade (Gleason scores 8–10),
given the presence of high-grade tumor (patterns 4and 5) on needle biopsy. On needle biopsies withpatterns 3, 4, and 5, both the primary pattern and thehighest grade should be recorded. For a radicalprostatectomy specimen, the Gleason score is basedon the primary and secondary patterns, with acomment added about the tertiary pattern.
. Whether the actual percentage of a 4- or 5-patterntumor should be included in the report is not clearbased on published data to date, and if thepercentage emerges as an important parameter,meaningful, discriminatory cutoff points for thepercentage of patterns 4 or 5 will need to be defined.If one wants to include that information in additionto the routine Gleason score, doing so is acceptable.
. For needle biopsies with different cores showingdifferent grades, the pathologist should assignindividual Gleason scores to separate cores if thecores are submitted in separate containers or if thecores are in the same container but their location isspecified by the urologist (ie, by different color inks).In addition to giving separate cores individualGleason scores, an optional, overall score can begiven at the end of the case. If more than one corecontains cancer with multiple cores per container,some authors think each core should be gradedseparately, whereas other authors think an overallgrade should be given for the involved cores perspecimen container. In cases in which a containercontains multiple pieces of tissue and it is unclearwhether one is looking at an intact core, an overallscore should be given for that container.
Changes to Patterns 3 and 4
The general theme of the changes to patterns 3 and 4was to limit the definition of pattern 3 carcinoma and towiden the scope of pattern 4 carcinoma19,20 (Table 7).
As in the original Gleason description, pattern 3carcinomas are composed of discrete, circumscribed, andinfiltrative glands with well-formed glandular lumina. Inthe 2005 ISUP Modified Gleason System, very small, well-formed glands were still considered within the spectrumof Gleason pattern 3; however, a departure from theoriginal Gleason system was that ‘‘individual cells’’ arenot allowed within Gleason pattern 3.15
A further area of divergence from the original Gleasonsystem was the controversial area of cribriform Gleason
Table 3. The5ArchitecturalPatternsAccording to the2005 International SocietyofUrologicalPathologyModifiedGleasonSystem
1. Circumscribed nodule of closely packed, but separate, uniform, rounded to oval, medium-sized acini (larger glands than pattern 3)2. Like pattern 1, fairly circumscribed, but at the edge of the tumor nodule, there may be minimal infiltration; glands are more loosely
arranged and not quite as uniform as Gleason pattern 13. Discrete glandular units: typically, smaller glands than seen in Gleason patterns 1 or 2; infiltrates in and among nonneoplastic prostate
acini; marked variation in size and shape; smoothly circumscribed, small, cribriform nodules of tumor4. Fused microacinar glands: ill-defined glands with poorly formed glandular lumina; large, cribriform glands; cribriform glands with an
irregular border; hypernephromatoid5. Essentially no glandular differentiation, composed of solid sheets, cords, or single cells; comedocarcinoma with central necrosis
surrounded by papillary, cribriform, or solid masses
r
Prostate cancer Gleason score 4 + 3 5 7. Gleason pattern 4 with poorly formed glands. Many of the glands have abortive lumina or are disrupted. F,Prostate cancer Gleason score 4 + 5 5 9. There is an area with single cells and solid, infiltrating strands of epithelium, already seen with the 320 lens. Thisis sufficient for diagnosing a Gleason pattern 5 component (hematoxylin-eosin, original magnifications 310 [A through E] and 320 [F]).
Arch Pathol Lab Med—Vol 136, April 2012 Gleason Grading System—Egevad et al 429

pattern 3. Within the original Gleason illustrations ofpattern 3, large, cribriform glands are depicted withrounded and smooth contours. Gleason never conductedany studies that specifically addressed the prognosticdifferences between the rounded glands he consideredcribriform pattern 3 and the irregular glands he also calledcribriform pattern 3. At the ISUP 2005 conference,15 theconsensus was that almost all of those cribriform patternsshould be diagnosed as Gleason pattern 4. The consensuspanel required extremely stringent criteria for the diag-nosis of cribriform pattern 3, which included onlyrounded, well-circumscribed glands of the same size asnormal glands; that is, cribriform Gleason pattern 3 PCashould morphologically resemble cribriform high-gradeprostatic intraepithelial neoplasia but show diagnosticfeatures of infiltrating carcinoma such as the following:
. Glands are negative for basal cell markers,
. Glands are back to back, ruling out high-gradeprostatic intraepithelial neoplasia, or
. Glands should exhibit pathognomonic features ofcarcinoma, such as perineural invasion or extrapro-static extension.
In contrast, pattern 4, which was originally limitedto fused or irregularly contoured cribriform structures,was widened in scope. With rare exceptions, almost allcribriform morphologies were accepted as Gleason pat-tern 4. Although not included in the original Gleasondepictions, a consensus was reached that ill-definedglands with poorly formed glandular lumina, a patternthat often accompanies fused glands, warranted adiagnosis of Gleason pattern 4.
The grading of glomeruloid glands is another contro-versial area in the modified Gleason system. Glome-rulations are dilated glands containing intraluminalcribriform structures with a single point of attachment,resembling a renal glomerulus. According to some expertsat the 2005 ISUP consensus conference, the rare case of
Gleason score 3 + 3 5 6, admixed with small glomeruloidglands, should be scored as 3 + 3 5 6. Other experts inthe field felt that all glomeruloid structures should beassigned a Gleason pattern 4. Larger glomeruloid struc-tures are uniformly accepted by urologic pathologists asGleason pattern 4. Consequently, either approach wasdeemed acceptable for practicing pathologists until futuredata indicated which method was more accurate.15
EFFECT OF THE MODIFIED GLEASON GRADING SYSTEM
Upgrading
The primary result of limiting the definition of Gleasonpattern 3 and expanding the definition of pattern 4 hasbeen Gleason grade migration or upgrading. In manysettings, Gleason pattern 3 carcinoma, previously the mostcommon pattern on needle biopsy, has become lesscommon than pattern 4. In one recent study comparingthe original and modified Gleason system on needlebiopsy material, cancers with a Gleason score of 6decreased from 48% to 22% of the total, whereas cancerwith Gleason score 7 increased from 25% to 68%.12 Notsurprisingly, the magnitude of this shift depends some-what on the study population, and it is less dramatic inclinical settings with a greater proportion of early stagedisease, as seen in a study by Billis et al,11 where theproportion of needle biopsies with a Gleason score of 6was 68%, decreasing to 49% using the modified gradingscheme. Correspondingly, Gleason 7 went from 26% to39% with application of the modified grade criteria.11
Biopsy Versus Radical Prostatectomy Gleason Score
Several studies have addressed the correlation andsources for the discrepancies between Gleason scores inneedle biopsies and corresponding radical prostatectomyspecimens: sampling error, borderline cases, pathologyerror, and pathologists’ experience.
The most common type of sampling error occurs whenthere is a higher-grade component present within the
Table 5. Reasons for Not Assigning Gleason Scores 2 Through 4 on Needle Biopsy
1. Cancer with Gleason scores 2 through 4 is extraordinarily rare in needle biopsies as compared with transurethral resection specimens2. There is poor reproducibility among experts for lower-grade tumors3. The correlation with the prostatectomy score for tumors with a Gleason score of 2 through 4 is poor4. A ‘‘low’’ score of Gleason 2 through 4 may misguide clinicians and patients into believing that there is an indolent tumor
Table 4. Differences Between the Original Gleason System and the 2005 International Society of Urological Pathology(ISUP) Modified Gleason Systema
Original Gleason System 2005 ISUP Modified Gleason System
A diagnosis of GS , 4 possible on NB GS of NB specimens , 4 rarely, if ever, madeCribriform glands with rounded and smooth contours as well as with
an irregular outer border are diagnosed as Gleason pattern 3.Most cribriform patterns would be diagnosed as Gleason pattern 4,
whereas specimens with only rare cribriform lesions would satisfy thediagnostic criteria for cribriform pattern 3
The same GS is used for NB and RP specimens Different GS used for NB and RP specimensHigh-grade tumor of small quantity (,5%) on NB should be
excluded based on GS (5% threshold rule)High-grade tumor of any quantity on NB should be included within the GS
Tumors on NB should be graded by listing the primary andsecondary patterns, ie, excluding tertiary pattern
For the tertiary pattern on NB specimens, both the primary pattern andthe highest grade should be recorded
The GS of RP specimens should be assigned based on the primaryand secondary patterns
For RP specimens, the pathologist should assign the GS based on the primaryand secondary patterns; a comment should be added on the tertiary pattern
Separate or overall scoring to assess all grades of NB specimens When NB specimens show different grades in separate cores, individualGS should be assigned to these cores (separate scoring)
The grade of the largest portion should be assigned, even ifthe second largest portion is of higher grade
When RP specimens show different grades in separate tumor nodules, aseparate GS should be assigned to each of the dominant tumor nodules
a Abbreviations: GS, Gleason score; NB, needle biopsy; RP, radical prostatectomy.
430 Arch Pathol Lab Med—Vol 136, April 2012 Gleason Grading System—Egevad et al

radical prostatectomy that is not sampled on needle biopsy.This typically occurs when a needle biopsy tumor is gradedas Gleason score 3 + 3 5 6 and a Gleason pattern 4, whichwas not sampled on the biopsy, exists in the prostatectomy,resulting in a prostatectomy Gleason 3 + 4 5 7. A commonpathology error is seen when pathologists assign a Gleasonscore of less than 4 on a needle biopsy, which is, in fact, aGleason score 5 to 6 or higher. When there is a limited focusof small glands of cancer on needle biopsy, it is a Gleasonpattern 3 or higher by definition.14 Gleason pattern 3 consistsof small glands with an infiltrative pattern. Biopsying anadenocarcinoma with a Gleason score of less than 6 isunlikely to result in just a few neoplastic glands becauselow-grade adenocarcinoma grows as nodules of closelypacked glands rather than scattered, infiltrating glands.Undergrading may result from difficulty in recognizing aninfiltrative growth pattern or failing to recognize thepresence of small areas of gland fusion.14
An important effect of modifying the Gleason gradinghas been to improve the agreement between Gleason scoreson needle biopsy and radical prostatectomy. Before the2005 ISUP modification, the agreement of Gleason scoresbetween biopsy and radical prostatectomy specimensranged from 28% to 68% in most studies. This relativelylow level of agreement was predominantly due to theundergrading of low-grade carcinomas in needle biopsies,whereas the agreement was more exact in high-gradecarcinomas. Biopsies have been found to undergradecarcinomas in 24% to 60% of cases, whereas overgradingis less common, occurring in 5% to 32% of cases.
Results on the concordance of the Gleason scores betweenneedle biopsy and radical prostatectomy when the ISUPrevision was issued conflict. In a recent study by Helpap etal,12 overall exact agreement between needle biopsy andradical prostatectomy specimens increased from 58% to72% when using the modified system. As in the past, mostof the cases without perfect correlation were due toundergrading (73%). When analyzed by Gleason score,agreement using the modified system was excellent for abiopsy Gleason score of 3 + 4 5 7 (88%) and reasonable for 4+ 3 5 7 (68%) but was quite poor for 3 + 3 5 6 (28%).12 Theproportion of radical prostatectomy specimens that wereassigned a score of 6 or 7 increased from 68% to 89% with
the introduction of the ISUP 2005 modified Gleason score.21
As many as 82% of cases were assigned a Gleason score of 7.Agreement improves when cases are grouped into a fewcategories. Furthermore, Ozok et al22 showed that agree-ment between needle biopsies and radical prostatectomyspecimens in 97 men improved from 31.9% to 44.3% withthe ISUP grading system.
Other studies failed to demonstrate significantly im-proved agreement.18,23,24 In a study by Uemura et al,23 theconcordance rates for needle biopsies and radical prosta-tectomy specimens between the original Gleason systemand the ISUP modified system were 67% and 70%,respectively. Similarly, Zareba et al18 showed the biopsy–radical prostatectomy did not significantly affect theGleason score agreement (63.4% and 65.5%, respectively).
Observer Reproducibility
Exact intraobserver agreement on Gleason scores wasreported in 43% to 78% of cases, and agreement withinplus or minus one Gleason score unit was reported in72% to 87% of cases.16,17 Gleason wrote that he duplicatedexactly his previous histologic scores approximately 50%of times. Highly variable levels of interobserver agree-ment on Gleason scores have also been reported, with arange of 36% to 81% for exact agreement and 69% to 86%within plus or minus one Gleason score unit.25
An important consequence of changes to the definitionof Gleason pattern 4 has been an improvement ininterobserver reproducibility. Most studies using themodified Gleason system have shown that overallinterobserver reproducibility hovers around 80%. Again,grouping the cases into fewer categories contributes tothese results. In an early study on the reproducibility of amodified Gleason score, including primary and highestGleason pattern in radical prostatectomy specimens,Glaessgen et al26 found that weighted k was almostidentical for conventional and modified Gleason scores.That study did not, however, take into account the effect ofchanges in pattern interpretation. Although this improve-ment may be due, in part, to the decreased diagnosis ofcarcinomas with low Gleason scores (Gleason scores 2–5)on needle biopsy using the modified system,27 there hasalso been improvement in the reproducibility of Gleason
Table 6. Grading Variations and Variants of Prostate Adenocarcinoma
Pseudohyperplastic Adenocarcinoma. These cancers should be graded as Gleason score 3 + 3 5 6 with pseudohyperplastic features, in large part, based on the recognition
that they are most often accompanied by more-ordinary Gleason score 3 + 3 5 6 adenocarcinomaFoamy Gland Carcinoma. Whereas most cases of foamy gland carcinoma would be graded as Gleason score 3 + 3 5 6, higher-grade, foamy gland carcinomas
exist and should be graded accordingly based on the patternVacuoles. In the original Gleason description, vacuoles are described as signet cells under pattern 5 tumors; although vacuoles are typically
seen within Gleason pattern 4 cancer, they may be seen within Gleason pattern 5 and even Gleason pattern 3 tumors. Tumorsshould be graded as if the vacuoles were not present by evaluating only the underlying architectural pattern
Table 7. Reasons for Assigning Gleason Pattern 4 to Cribriform Glands
1. Candidate cribriform pattern 3 cancers almost always occur in association with typical Gleason pattern 4 cancer elsewhere in the case2. The rarity of candidates for cribriform Gleason pattern 33. Within these rare candidates, the lack of interobserver reproducibility by experts on assessing the diagnostic criteria proposed to
distinguish cribriform Gleason pattern 4 from Gleason pattern 34. Conceptually, the change in grade from pattern 3 to pattern 4 would be expected to be reflected in a distinct architectural paradigm shift
where cribriform as opposed to individual glands are formed, rather than merely a subjective continuum of differences in size, shape, andcontour of cribriform glands
Arch Pathol Lab Med—Vol 136, April 2012 Gleason Grading System—Egevad et al 431

pattern 4 carcinomas.28 In a recent study, which evaluatedreproducibility for each Gleason score group under themodified system, there was 68% congruence for Gleasonscore 7, compared with 27% in 1994, a finding thatunderscores the importance of the modifications toGleason pattern 4 definitions.29,30
Correlation of Gleason Score With Patient Outcomes andPathologic Stage
The true test of the validity of the new Gleason system isits correlation with patient outcomes. However, it will besome time before a sufficient follow-up period has elapsedto do those studies. Both studies by Uemura et al23 andBillis et al11 demonstrated that the Gleason scores onneedle biopsies using the modified, but not the original,Gleason system correlated with progression after radicalprostatectomy. Tsivian et al31 similarly found that themodified Gleason score, when analyzed in prognosticgrade groups (,7, 7, and .7), predicted biochemicalrecurrence after radical prostatectomy better than did theoriginal Gleason score groups. In a large study of 454transurethral resections and 347 needle biopsies, Berneyet al32 reported significant upgrading of biopsies initiallygraded in 1990–1996 and then regraded and published in2007. Whereas the initial grades did not correlate withsurvival outcome, the newly recorded grades did.32 Inthe only study favoring the original over the modifiedGleason system for progression, Delahunt et al33 reportedthat the original Gleason grading system outperformedthe modified system in predicting prostate-specificantigen nadir following external beam radiotherapyand hormone therapy. However, prostate-specific antigennadir is not currently considered the best endpoint forpredicting failure following radiotherapy.
Until more time has elapsed for follow-up studies,surrogate predictors of patient outcome have been used,such as the pathologic stage of the tumor at radicalprostatectomy. One recent study34 looking at the correla-tion among pathologic stage and the conventional andmodified Gleason systems applied to radical prostatecto-my specimens found that the only significant change instage distribution was seen for Gleason score 7, where pT2was the most common stage with modified grading (54%)and pT3 was most common with conventional grading(67%). Strikingly, 95% of Gleason score 3 + 4 5 7 tumorswere stage pT2, whereas 79% of Gleason score 4 + 3 5 7tumors were stage pT3 to pT4. That dramatic difference inclinical stage between 3 + 4 5 7 and 4 + 3 5 7 carcinomas islikely due to the inclusion of cases previously consideredGleason score 6 in the 3 + 4 5 7 category under themodified system. Whether the distinction between 3 + 4 57 and 4 + 3 5 7 under the new grading system will affectclinical decision-making remains to be seen.34
CLINICAL IMPLICATIONS OF THE MODIFIED GLEASONGRADING SYSTEM
One notable consequence of the Gleason modifications isthat it is increasingly difficult to compare data sets assessingpatient outcomes in prostate cancer over time. Today’s casesof Gleason score 6 are a homogenous group of tumorslacking cribriform and poorly formed glands, and are,therefore, associated with a better prognosis. An examplecan be seen in a study20 analyzing 38 cases that werediagnosed before the consensus conference as organ-
confined, margin negative, Gleason score 6 PCa, which weretreated with radical prostatectomy in 1983–2005 and whichhad biochemical progression. On review of these olderGleason score 6 cases, 24 (63%) would be considered to havesome Gleason pattern 4 under today’s grading scheme,including poorly formed, fused, or cribriform glands. Basedon the updated Gleason system, organ-confined, Gleasonscore 6, margin-negative cancer is virtually 100% curable.
Effect of Upgrading on Treatment Decisions
The most important clinical decision affected by theGleason score on a needle biopsy is the mode of ther-apy offered. Historically, patients with high-grade tumors(traditionally Gleason score 8–10) have been discouragedfrom undergoing radical prostatectomy because of the highlikelihood of disease not confined to the organ or evensystemic disease at presentation. However, a number ofmore recent studies from the era after the introductionof prostate-specific antigen (almost all using conventionalGleason grading) have suggested that men with high-gradetumors may do better than we previously thought aftersurgical monotherapy. Thus, the tendency toward upgrad-ing may be balanced by an increasing trend to performradical prostatectomy in the context of higher-grade disease.Additionally, the preferred mode of therapy for Gleasonscore 7 tumors (intermediate grade) has always beenambiguous. Because the most noticeable consequenceof the changing definition of Gleason pattern 4 is theregrouping of cases previously considered Gleason 6 intothe Gleason 7 category, this particular modification to theGleason system will likely have little effect on the decisionto proceed to radical prostatectomy. Occasionally, radio-therapists have distinguished between Gleason 3 + 4 and4 + 3 disease by whether the patient is a reasonablecandidate for brachytherapy. The recent suggestion thatmodified Gleason score 3 + 4 5 7 tumors behave much likeGleason 6 tumors, whereas Gleason score 4 + 3 5 7 tumorsbehave more like high-grade tumors does indicate thatrefinement of Gleason pattern 4 definitions may haveslightly shifted the traditional low-grade/high-grade cut-offs. However, those data used Gleason scoring fromradical prostatectomies rather than from needle biopsies.Because sampling is an unavoidable issue on needlebiopsy, it is unlikely that any refinement of the Gleasonsystem will make the distinction between 3 + 4 5 7 and4 + 3 5 7 into a reliable basis for determining appropriatetherapy at this time.20
There is also a need to better define the detectionthreshold for a small amount of Gleason pattern 5. Expertshave claimed that they require a cohesive focus ofepithelial structures without lumina, seen at a powerlower than 340.35 Yet, more stringent criteria is neededbecause a diagnosis of a minute component of a Gleasonpattern 5 tumor on a needle biopsy may move the Gleasonscore to 4 + 5 5 9 or 3 + 5 5 8, which is likely to affect thetreatment decision.
SUBSEQUENT PROPOSALS FOR SLIGHTMODIFICATIONS OF THE ISUP GRADING SYSTEM
The recent recommendation is that all cribriformpatterns be diagnosed as Gleason pattern 4 rather thanGleason pattern 3.19,20,36 This recommendation has beenbased on a reproducibility study by Latour et al37 and issupported by nuclear DNA studies. Latour et al37 selected30 needle biopsy cases that possibly represented cribriform
432 Arch Pathol Lab Med—Vol 136, April 2012 Gleason Grading System—Egevad et al

Gleason pattern 3 cancer. Thirty-six digital images weretaken and sent to 10 experts in prostate pathology.Consensus was defined when at least 7 of 10 experts(70%) agreed on the grade. Experts reached consensus on67% (24 of 36) of the images (pattern 4, n 5 23; pattern 3,n 5 1). Of the 12 images where consensus was not reached,7 (58%) favored pattern 4 (6 of 10 experts [60%] agreed),1 (8%) favored pattern 3 (6 of 10 experts [60%] agreed),and 4 (33%) were equivocal (,6 experts agreed). Themost common criteria used to diagnose pattern 4 in the 23pattern 4 images where consensus was reached were (infrequency from high to low): irregular contour, irregulardistribution of lumens, slitlike lumens, large glands,number of glands, and small lumens. In the only pattern3 image on which consensus was reached, the criteria usedwere regular contour, small glands, regular distribution oflumens, and uniform, round lumens. Discrepancy betweenexperts was qualified as primarily objective (differentcriteria present) in 38%, subjective (different interpretationof the same criteria) in 12%, and mixed (both objective andsubjective) in 50%. The most frequent situation withdifferent interpretations of the same criteria was regularversus irregular contours and small versus large glands,with the former being more common. Even in this highlyselected set of images thought to be the best candidates forcribriform pattern 3 from a busy consultation service, mostexperts interpreted the cribriform patterns as pattern 4.Moreover, most of the cribriform foci investigated (73%)were associated with more definitive pattern 4 elsewhereon the needle biopsy specimen.
In a recent study,38 prostate needle biopsies containingcarcinoma with glomeruloid features were examinedto establish whether there was an association betweenglomerulations and the presence of concurrent high-gradecarcinoma. Glomerulations were overwhelmingly associ-ated with high-grade cancer on the same core, werecomposed predominantly of Gleason pattern 4 (80% ofcases), and often appeared to represent a morphologictransition to larger cribriform glands. Only a fewglomerulations were surrounded exclusively by pattern3 cancer (16% of cases). Although this was an associationstudy without clinical follow-up, the weight of the currentevidence suggests that glomerulations most likely repre-sent an early stage of cribriform pattern 4 cancer andshould likely be graded as pattern 4.
GLEASON GRADING SYSTEM SUPPLEMENTED WITHNUCLEAR MORPHOLOGY
AND IMMUNOHISTOCHEMISTRY
The Gleason system and its ISUP revision are basedon the architectural patterns of PCa. The contribution ofnuclear morphology and immunohistochemistry to itsfurther refinement has been investigated only to a limitedextent.
It is worth mentioning the proposal made by the late F.K. Mostofi, MD, in 1999, in a meeting in Paris, France,sponsored by the World Health Organization, to supple-ment the Gleason system with the World Health Organi-zation nuclear grading scheme.39 The proposal was basedon his experience that patients with a Gleason score of 6 orhigher can be stratified based on the World HealthOrganization nuclear grading and that such stratificationhas a prognostic importance. This was recently confirmedin a morphometric study40 in which it was shown that
nuclear signature is important in better-defining riskgroups in patients with PCa.
There are some cases in the description of the Gleasongrading system that are right at the interface between 2different patterns, leading to interobserver and possiblyintraobserver variability.2,14 In particular, one of the majorchallenges for pathologists is the identification of smallareas of fusion in the presence of a predominantly grade 3background whose recognition will yield a Gleason scoreof 7.14 There are few immunohistochemical studies, toour knowledge, addressing this issue. Richardson et al41
investigated IGBFB2 and found the marker to be superiorto morphology in defining gland fusions and, therefore, inseparating Gleason pattern 4 from Gleason pattern 3.
CONCLUSIONS
The primary result of limiting the definition of Gleasonpattern 3 and expanding the definition of pattern 4 isGleason grade migration or upgrading, both in needlebiopsies and radical prostatectomy specimens. There areclinical consequence to upgrading the Gleason score, forinstance, in the type of therapy offered to an individualpatient with PCa.1 For example, patients with high-gradetumors from biopsies could be discouraged from under-going active surveillance. The true test of the validity ofthe 2005 ISUP Modified Gleason System is its correlationwith patient outcomes. Few studies have yet beenpublished assessing those correlations. Uemura et al23
found that the 2005 ISUP modified Gleason score of needlebiopsy specimens was significantly associated with bio-chemical recurrence-free survival after radical prostatec-tomy. They concluded that the ISUP system is clinicallyuseful for determining the most appropriate treatmentsfor patients with early stage PCa.23 However, it will besome time until studies with sufficient follow-up periodsare published.
The urologists and uropathologists have to be aware ofthe effect of the Gleason system used on patient prognosisand treatment. The pathology report and the clinicalrecords have to clearly indicate which system is adoptedfor each individual patient.
References
1. Montironi R, Cheng L, Lopez-Beltran A, et al. Original Gleason systemversus 2005 ISUP modified Gleason system: the importance of indicating whichsystem is used in the patient’s pathology and clinical reports. Eur Urol. 2010;58(3):369–373.
2. Gleason DF. Classification of prostatic carcinomas. Cancer Chemother Rep.1966;50(3):125–128.
3. Mellinger GT, Gleason D, Bailar J III. The histology and prognosis ofprostatic cancer. J Urol. 1967;97(2):331–337.
4. Gleason DF, Mellinger GT. Prediction of prognosis for prostatic adenocar-cinoma by combined histological grading and clinical staging. J Urol. 1974;111(1):58–64.
5. Mellinger GT. Prognosis of prostatic carcinoma. Recent Results Cancer Res.1977;(60):61–72.
6. Gleason DF. Histological grading and clinical staging of prostaticcarcinoma. In: Tannenbaum M, ed. Urologic Pathology: The Prostate.Philadelphia, PA: Lea and Feibiger; 1977:171–198.
7. Hodge KK, McNeal JE, Terris MK, Stamey TA. Random systematic versusdirected ultrasound guided transrectal core biopsies of the prostate. J Urol. 1989;142(1):71–74.
8. Berney DM. The case for modifying the Gleason grading system. BJU Int.2007;100(4):725–726.
9. Amin MB, Schultz DS, Zarbo RJ. Analysis of cribriform morphology inprostatic neoplasia using antibody to high molecular–weight cytokeratin. ArchPathol Lab Med. 1994;118(3):260–264.
10. Amin MB, Boccon-Gibod L, Egevad L, et al. Prognostic and predictivefactors and reporting of prostate carcinoma in prostate needle biopsy specimens.Scand J Urol Nephrol Suppl. 2005;(216):20–33.
11. Billis A, Guimaraes MS, Freitas LL, Meirelles L, Magna LA, Ferreira U. Theimpact of the 2005 international society of urological pathology consensus
Arch Pathol Lab Med—Vol 136, April 2012 Gleason Grading System—Egevad et al 433

conference on standard Gleason grading of prostatic carcinoma in needlebiopsies. J Urol. 2008;180(2):548–552.
12. Helpap B, Egevad L. The significance of modified Gleason grading ofprostatic carcinoma in biopsy and radical prostatectomy specimens. VirchowsArch. 2006;449(6):622–627.
13. Montironi R, Mazzucchelli R, Lopez-Beltran A, Scarpelli M, Cheng L. TheGleason grading system: where are we now? Diagn Histopathol. 2011;17(10):419–427.
14. Montironi R, Mazzucchelli R, Scarpelli M, Lopez-Beltran A, Fellegara G,Algaba F. Gleason grading of prostate cancer in needle biopsies or radicalprostatectomy specimens: contemporary approach, current clinical significanceand sources of pathology discrepancies. BJU Int. 2005;95(8):1146–1152.
15. Epstein JI, Allsbrook WC Jr, Amin MB, Egevad LL; ISUP GradingCommittee. The 2005 International Society of Urological Pathology (ISUP)Consensus Conference on Gleason grading of prostatic carcinoma. Am J SurgPathol. 2005;29(9):1228–1242.
16. Griffiths DF, Melia J, McWilliam LJ, et al. A study of Gleason scoreinterpretation in different groups of UK pathologists; techniques for improvingreproducibility. Histopathology. 2006;48(6):655–662.
17. Melia J, Moseley R, Ball RY, et al. A UK-based investigation of inter- andintra-observer reproducibility of Gleason grading of prostatic biopsies. Histopa-thology. 2006;48(6):644–654.
18. Zareba P, Zhang J, Yilmaz A, Trpkov K. The impact of the 2005International Society of Urological Pathology (ISUP) consensus on Gleasongrading in contemporary practice. Histopathology. 2009;55(4):384–391.
19. Epstein JI. An update of the Gleason grading system. J Urol. 2010;183(2):433–440.
20. Lotan TL, Epstein JI. Clinical implications of changing definitions withinthe Gleason grading system. Nat Rev Urol. 2010;7(3):136–142.
21. Vainer B, Toft BG, Olsen KE, Jacobsen GK, Marcussen N. Handling ofradical prostatectomy specimens: total or partial embedding? Histopathology.2011;58(2):211–216.
22. Ozok HU, Sagnak L, Tuygun C, et al. Will the modification of the Gleasongrading system affect the urology practice? Int J Surg Pathol. 2010;18(4):248–254.
23. Uemura H, Hoshino K, Sasaki T, et al. Usefulness of the 2005 InternationalSociety of Urologic Pathology Gleason grading system in prostate biopsy andradical prostatectomy specimens. BJU Int. 2009;103(9):1190–1194.
24. Veloso SG, Lima MF, Salles PG, Berenstein CK, Scalon JD, Bambirra EA.Interobserver agreement of Gleason score and modified Gleason score in needle biopsyand in surgical specimen of prostate cancer. Int Braz J Urol. 2007;33(5):639–646.
25. Lopez-Beltran A, Mikuz G, Luque RJ, Mazzucchelli R, Montironi R. CurrentpracticeofGleasongradingofprostatecarcinoma.VirchowsArch.2006;448(2):111–118.
26. Glaessgen A, Hamberg H, Pihl CG, Sundelin B, Nilsson B, Egevad L.Interobserver reproducibility of modified Gleason score in radical prostatectomyspecimens. Virchows Arch. 2004;445(1):17–21.
27. Berney DM. Low Gleason score prostatic adenocarcinomas are no longerviable entities. Histopathology. 2007;50(6):683–690.
28. Egevad L, Algaba F, Berney DM, et al. Interactive digital slides with heatmaps: a novel method to improve the reproducibility of Gleason grading.Virchows Arch. 2011;459(2):175–182.
29. Fine SW, Epstein JI. A contemporary study correlating prostate needlebiopsy and radical prostatectomy Gleason score. J Urol. 2008;179(4):1335–1338.
30. Steinberg DM, Sauvageot J, Piantadosi S, Epstein JI. Correlation of prostateneedle biopsy and radical prostatectomy Gleason grade in academic andcommunity settings. Am J Surg Pathol. 1997;21(5):566–576.
31. Tsivian M, Sun L, Mouraviev V, et al. Changes in Gleason score gradingand their effect in predicting outcome after radical prostatectomy. Urology. 2009;74(5):1090–1093.
32. Berney DM, Fisher G, Kattan MW, et al; Trans-Atlantic Prostate Group.Major shifts in the treatment and prognosis of prostate cancer due to changes inpathological diagnosis and grading. BJU Int. 2007;100(6):1240–1244.
33. Delahunt B, Lamb DS, Srigley JR, et al. Gleason scoring: a comparison ofclassical and modified (international society of urological pathology) criteriausing nadir PSA as a clinical end point. Pathology. 2010;42(4):339–343.
34. Helpap B, Egevad L. Correlation of modified Gleason grading of prostatecarcinoma with age, serum prostate specific antigen and tumor extent in needlebiopsy specimens. Anal Quant Cytol Histol. 2008;30(3):133–138.
35. Egevad L, Allsbrook WC Jr, Epstein JI. Current practice of Gleason gradingamong genitourinary pathologists. Hum Pathol. 2005;36(1):5–9.
36. Egevad L, Engstrom K, Mattson S, Wester K, Busch C. Heterogeneity ofDNA ploidy in prostate cancer. J Urol Pathol. 1999;10:23–37.
37. Latour M, Amin MB, Billis A, et al. Grading of invasive cribriformcarcinoma on prostate needle biopsy: an interobserver study among experts ingenitourinary pathology. Am J Surg Pathol. 2008;32(10):1532–1539.
38. Lotan TL, Epstein JI. Gleason grading of prostatic adenocarcinoma withglomeruloid features on needle biopsy. Hum Pathol. 2009;40(4):471–477.
39. Bostwick DG, Foster CS, Algaba F, et al. Prostate tissues factor. In: MurphyG, Khoury S, Partin A, Denis L, eds. Prostate Cancer: 2nd InternationalConsultation on Prostate Cancer—1999 Paris. Plymouth, Devon, UK: PlymbridgeDistributors Ltd; 2000:162–201.
40. Venkataraman G, Rycyna K, Rabanser A, et al. Morphometric signaturedifferences in nuclei of Gleason pattern 4 areas in Gleason 7 prostate cancer withdiffering primary grades on needle biopsy. J Urol. 2009;181(1):88–93.
41. Richardsen E, Ukkonen T, Bjornsen T, Mortensen E, Egevad L, Busch C.Overexpression of IGBFB2 is a marker for malignant transformation in prostateepithelium. Virchows Arch. 2003;442(4):329–335.
434 Arch Pathol Lab Med—Vol 136, April 2012 Gleason Grading System—Egevad et al