Embed Size (px)
Citation preview
Paroxysmal nocturnal hemoglobinuria
Literature reviewOctober 2012
B DEVALET
Plan
Paroxysmal nocturnal hemoglobinuria
history
definition
diagnosis
clinical aspects
pathophysiology of disease
thrombotic events
pathophysiology of thrombosis
risk factors for thrombosis
treatment
treatment of subclinical PNH and AAPNH
treatment of classic PNH
prophylaxis of thrombosis
treatment of thrombosis
treatment during pregnancy
Literature
PNH History
First description by a german physicianPaul Struumlbing in 1889
More detailed description by Dr Ettore Marchiafava and Dr Alessio Nazari in 1911 then Dr Ferdinando Micheli in 1931 (Marchiafava-Micheli syndrome)
Identification of the molecular basis of PNH helped to define the physiology of the complement system in humans (47)
PNH Definition
Rare acquired disorder of hematopoietic stem cells
Incidence not really known but estimated 1-21000000 inhabyear
Somatic mutation in X-linked gene the phosphatidylinositol glycan class A (PIG-A)
PIG-A si required for synthesis of glycosyl phosphatidylinositol (GPI) anchor
Deficiency in GPI anchored proteins (many)
Lack of CD59 laquo MIRL raquo and CD55 laquo DAF raquo (complement regulatory proteins) leads to complement mediated intravascular hemolysis (47)
PNH Definition
Non malignant clonal expansion 2 steps hypothesis (53)
step 1 PIG-A mutation
no clonal expansion asymptomatic
step 2 injury to the normal bone marrow
T cells and NK cells attack
normal hematopoietic cells destroyedbut PNH cells escape (absence of GPI anchored targeted peptides or accessory molecules required for T cells attack)
bone marrow failure clonal expansion
PNH Diagnosis
(Ham and sucrose tests)
Flow cytometry with monoclonal antibodies that bind to specific GPI-anchored proteins (precentage of PNH cells measured)(38)
clone size
use at least 2 different monoclonal antibodies directed against 2 different GPI-anchored proteins(rare congenital deficiencies of CD59 or CD55)
on at least 2 different cells lineages(risk of falsely negative tests if only red cells are screened ndash recent hemolytic crisis or recent transfusion)
phenotypic mosaicism
PNH III cells completely deficient in GPI anchored-proteins
PNH II cells partly deficient
laquo PNH raquo I cells express GPI-anchored proteins at normal density
PNH Diagnosis
FLAER (fluorescein-labeled proaerolysin)(34)
Aerolysin = the principal virulence factor of the bacterium Aeromonas hydrophila
binds selectively and with high affinity to the GPI anchor
more accurate assessment of the GPI anchor deficit in PNH (PNH clones lt1 can be detected)
complete blood count reticulocytes LDH bilirubin haptoglobin iron stores BM aspirate and biopsy cytogenetics
PNH Clinical aspects
3 different forms (clinical polymorphism)(3 4 34)
Classic PNH
young adults
intravascular hemolytic anemia (with crisis)
Hb lt12 gdL
hemoglobinuria (in the morning)
jaundice
general symptoms (asthenia malaise)
worsening of hemolysis during infection (complement activation above basal level)
no evidence of bone marrow failure (neutro gt1500microL platelets gt120 000microL)
dysphagia abdominal pain erectile dysfunction (35)
thrombosis
reccurent infectious diseases (ORL lungs) 40 2d cause of death
risk of MDSAML 5 25 at 10y (x100)
PNH Clinical aspects
PNH associated with aplastic anemia
small PNH clone (majority of patients lt10)
clinicalbiochemical evidence of hemolysis
2 or 3 cytopenias (Hb lt10 gdL neutro lt1000microL platelets lt80 000microL)
BM failure dominates the clinical picture
PNH Clinical aspects
Subclinical PNH
clone size lt1
no hemolysis
We find PNH clone in 60 of AA and in 20 of low risk MDS(47)
associated to AA high probability of response to immunosuppressive therapy
associated to low risk MDS (refractory anemia)
less pronounced morphological abnormalities of the blood cells
more severe thrombocytopenia
lower rate of karyotypic abnormalities
higher incidence of HLA-DR15
lower rate of progression to AML
higher probability of reponse to cyclosporine
Hypothesis that aplastic anemia and a subgroup of low risk MDS are immune-mediated diseases
immunity provides the selection pressure that favors the outgrowth of PNH clone
PNH Clinical aspects (3-4)
Classic PNH Aplastic anemia-PNH
Age 40y 30y
Abdominal pain 35 20
Median clone size 916 168
Median survival 18y gt22y
Thrombotic events (at 10y) 379 278
Medullar aplasia 20 at 10y 100
PNH Pathophysiology of disease (1)
Intravascular hemolysis
free Hb in the plasma
NO fixation to Hb
NO depletion
smooth muscle dystonias
dysphagia
abdominal pain
erectile dysfunction
arterial constriction
reduced blood flow to the kidneys
arterial hypertension
pulmonary hypertension (+undiagnosed thrombosis)
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
Plan
Paroxysmal nocturnal hemoglobinuria
history
definition
diagnosis
clinical aspects
pathophysiology of disease
thrombotic events
pathophysiology of thrombosis
risk factors for thrombosis
treatment
treatment of subclinical PNH and AAPNH
treatment of classic PNH
prophylaxis of thrombosis
treatment of thrombosis
treatment during pregnancy
Literature
PNH History
First description by a german physicianPaul Struumlbing in 1889
More detailed description by Dr Ettore Marchiafava and Dr Alessio Nazari in 1911 then Dr Ferdinando Micheli in 1931 (Marchiafava-Micheli syndrome)
Identification of the molecular basis of PNH helped to define the physiology of the complement system in humans (47)
PNH Definition
Rare acquired disorder of hematopoietic stem cells
Incidence not really known but estimated 1-21000000 inhabyear
Somatic mutation in X-linked gene the phosphatidylinositol glycan class A (PIG-A)
PIG-A si required for synthesis of glycosyl phosphatidylinositol (GPI) anchor
Deficiency in GPI anchored proteins (many)
Lack of CD59 laquo MIRL raquo and CD55 laquo DAF raquo (complement regulatory proteins) leads to complement mediated intravascular hemolysis (47)
PNH Definition
Non malignant clonal expansion 2 steps hypothesis (53)
step 1 PIG-A mutation
no clonal expansion asymptomatic
step 2 injury to the normal bone marrow
T cells and NK cells attack
normal hematopoietic cells destroyedbut PNH cells escape (absence of GPI anchored targeted peptides or accessory molecules required for T cells attack)
bone marrow failure clonal expansion
PNH Diagnosis
(Ham and sucrose tests)
Flow cytometry with monoclonal antibodies that bind to specific GPI-anchored proteins (precentage of PNH cells measured)(38)
clone size
use at least 2 different monoclonal antibodies directed against 2 different GPI-anchored proteins(rare congenital deficiencies of CD59 or CD55)
on at least 2 different cells lineages(risk of falsely negative tests if only red cells are screened ndash recent hemolytic crisis or recent transfusion)
phenotypic mosaicism
PNH III cells completely deficient in GPI anchored-proteins
PNH II cells partly deficient
laquo PNH raquo I cells express GPI-anchored proteins at normal density
PNH Diagnosis
FLAER (fluorescein-labeled proaerolysin)(34)
Aerolysin = the principal virulence factor of the bacterium Aeromonas hydrophila
binds selectively and with high affinity to the GPI anchor
more accurate assessment of the GPI anchor deficit in PNH (PNH clones lt1 can be detected)
complete blood count reticulocytes LDH bilirubin haptoglobin iron stores BM aspirate and biopsy cytogenetics
PNH Clinical aspects
3 different forms (clinical polymorphism)(3 4 34)
Classic PNH
young adults
intravascular hemolytic anemia (with crisis)
Hb lt12 gdL
hemoglobinuria (in the morning)
jaundice
general symptoms (asthenia malaise)
worsening of hemolysis during infection (complement activation above basal level)
no evidence of bone marrow failure (neutro gt1500microL platelets gt120 000microL)
dysphagia abdominal pain erectile dysfunction (35)
thrombosis
reccurent infectious diseases (ORL lungs) 40 2d cause of death
risk of MDSAML 5 25 at 10y (x100)
PNH Clinical aspects
PNH associated with aplastic anemia
small PNH clone (majority of patients lt10)
clinicalbiochemical evidence of hemolysis
2 or 3 cytopenias (Hb lt10 gdL neutro lt1000microL platelets lt80 000microL)
BM failure dominates the clinical picture
PNH Clinical aspects
Subclinical PNH
clone size lt1
no hemolysis
We find PNH clone in 60 of AA and in 20 of low risk MDS(47)
associated to AA high probability of response to immunosuppressive therapy
associated to low risk MDS (refractory anemia)
less pronounced morphological abnormalities of the blood cells
more severe thrombocytopenia
lower rate of karyotypic abnormalities
higher incidence of HLA-DR15
lower rate of progression to AML
higher probability of reponse to cyclosporine
Hypothesis that aplastic anemia and a subgroup of low risk MDS are immune-mediated diseases
immunity provides the selection pressure that favors the outgrowth of PNH clone
PNH Clinical aspects (3-4)
Classic PNH Aplastic anemia-PNH
Age 40y 30y
Abdominal pain 35 20
Median clone size 916 168
Median survival 18y gt22y
Thrombotic events (at 10y) 379 278
Medullar aplasia 20 at 10y 100
PNH Pathophysiology of disease (1)
Intravascular hemolysis
free Hb in the plasma
NO fixation to Hb
NO depletion
smooth muscle dystonias
dysphagia
abdominal pain
erectile dysfunction
arterial constriction
reduced blood flow to the kidneys
arterial hypertension
pulmonary hypertension (+undiagnosed thrombosis)
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH History
First description by a german physicianPaul Struumlbing in 1889
More detailed description by Dr Ettore Marchiafava and Dr Alessio Nazari in 1911 then Dr Ferdinando Micheli in 1931 (Marchiafava-Micheli syndrome)
Identification of the molecular basis of PNH helped to define the physiology of the complement system in humans (47)
PNH Definition
Rare acquired disorder of hematopoietic stem cells
Incidence not really known but estimated 1-21000000 inhabyear
Somatic mutation in X-linked gene the phosphatidylinositol glycan class A (PIG-A)
PIG-A si required for synthesis of glycosyl phosphatidylinositol (GPI) anchor
Deficiency in GPI anchored proteins (many)
Lack of CD59 laquo MIRL raquo and CD55 laquo DAF raquo (complement regulatory proteins) leads to complement mediated intravascular hemolysis (47)
PNH Definition
Non malignant clonal expansion 2 steps hypothesis (53)
step 1 PIG-A mutation
no clonal expansion asymptomatic
step 2 injury to the normal bone marrow
T cells and NK cells attack
normal hematopoietic cells destroyedbut PNH cells escape (absence of GPI anchored targeted peptides or accessory molecules required for T cells attack)
bone marrow failure clonal expansion
PNH Diagnosis
(Ham and sucrose tests)
Flow cytometry with monoclonal antibodies that bind to specific GPI-anchored proteins (precentage of PNH cells measured)(38)
clone size
use at least 2 different monoclonal antibodies directed against 2 different GPI-anchored proteins(rare congenital deficiencies of CD59 or CD55)
on at least 2 different cells lineages(risk of falsely negative tests if only red cells are screened ndash recent hemolytic crisis or recent transfusion)
phenotypic mosaicism
PNH III cells completely deficient in GPI anchored-proteins
PNH II cells partly deficient
laquo PNH raquo I cells express GPI-anchored proteins at normal density
PNH Diagnosis
FLAER (fluorescein-labeled proaerolysin)(34)
Aerolysin = the principal virulence factor of the bacterium Aeromonas hydrophila
binds selectively and with high affinity to the GPI anchor
more accurate assessment of the GPI anchor deficit in PNH (PNH clones lt1 can be detected)
complete blood count reticulocytes LDH bilirubin haptoglobin iron stores BM aspirate and biopsy cytogenetics
PNH Clinical aspects
3 different forms (clinical polymorphism)(3 4 34)
Classic PNH
young adults
intravascular hemolytic anemia (with crisis)
Hb lt12 gdL
hemoglobinuria (in the morning)
jaundice
general symptoms (asthenia malaise)
worsening of hemolysis during infection (complement activation above basal level)
no evidence of bone marrow failure (neutro gt1500microL platelets gt120 000microL)
dysphagia abdominal pain erectile dysfunction (35)
thrombosis
reccurent infectious diseases (ORL lungs) 40 2d cause of death
risk of MDSAML 5 25 at 10y (x100)
PNH Clinical aspects
PNH associated with aplastic anemia
small PNH clone (majority of patients lt10)
clinicalbiochemical evidence of hemolysis
2 or 3 cytopenias (Hb lt10 gdL neutro lt1000microL platelets lt80 000microL)
BM failure dominates the clinical picture
PNH Clinical aspects
Subclinical PNH
clone size lt1
no hemolysis
We find PNH clone in 60 of AA and in 20 of low risk MDS(47)
associated to AA high probability of response to immunosuppressive therapy
associated to low risk MDS (refractory anemia)
less pronounced morphological abnormalities of the blood cells
more severe thrombocytopenia
lower rate of karyotypic abnormalities
higher incidence of HLA-DR15
lower rate of progression to AML
higher probability of reponse to cyclosporine
Hypothesis that aplastic anemia and a subgroup of low risk MDS are immune-mediated diseases
immunity provides the selection pressure that favors the outgrowth of PNH clone
PNH Clinical aspects (3-4)
Classic PNH Aplastic anemia-PNH
Age 40y 30y
Abdominal pain 35 20
Median clone size 916 168
Median survival 18y gt22y
Thrombotic events (at 10y) 379 278
Medullar aplasia 20 at 10y 100
PNH Pathophysiology of disease (1)
Intravascular hemolysis
free Hb in the plasma
NO fixation to Hb
NO depletion
smooth muscle dystonias
dysphagia
abdominal pain
erectile dysfunction
arterial constriction
reduced blood flow to the kidneys
arterial hypertension
pulmonary hypertension (+undiagnosed thrombosis)
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Definition
Rare acquired disorder of hematopoietic stem cells
Incidence not really known but estimated 1-21000000 inhabyear
Somatic mutation in X-linked gene the phosphatidylinositol glycan class A (PIG-A)
PIG-A si required for synthesis of glycosyl phosphatidylinositol (GPI) anchor
Deficiency in GPI anchored proteins (many)
Lack of CD59 laquo MIRL raquo and CD55 laquo DAF raquo (complement regulatory proteins) leads to complement mediated intravascular hemolysis (47)
PNH Definition
Non malignant clonal expansion 2 steps hypothesis (53)
step 1 PIG-A mutation
no clonal expansion asymptomatic
step 2 injury to the normal bone marrow
T cells and NK cells attack
normal hematopoietic cells destroyedbut PNH cells escape (absence of GPI anchored targeted peptides or accessory molecules required for T cells attack)
bone marrow failure clonal expansion
PNH Diagnosis
(Ham and sucrose tests)
Flow cytometry with monoclonal antibodies that bind to specific GPI-anchored proteins (precentage of PNH cells measured)(38)
clone size
use at least 2 different monoclonal antibodies directed against 2 different GPI-anchored proteins(rare congenital deficiencies of CD59 or CD55)
on at least 2 different cells lineages(risk of falsely negative tests if only red cells are screened ndash recent hemolytic crisis or recent transfusion)
phenotypic mosaicism
PNH III cells completely deficient in GPI anchored-proteins
PNH II cells partly deficient
laquo PNH raquo I cells express GPI-anchored proteins at normal density
PNH Diagnosis
FLAER (fluorescein-labeled proaerolysin)(34)
Aerolysin = the principal virulence factor of the bacterium Aeromonas hydrophila
binds selectively and with high affinity to the GPI anchor
more accurate assessment of the GPI anchor deficit in PNH (PNH clones lt1 can be detected)
complete blood count reticulocytes LDH bilirubin haptoglobin iron stores BM aspirate and biopsy cytogenetics
PNH Clinical aspects
3 different forms (clinical polymorphism)(3 4 34)
Classic PNH
young adults
intravascular hemolytic anemia (with crisis)
Hb lt12 gdL
hemoglobinuria (in the morning)
jaundice
general symptoms (asthenia malaise)
worsening of hemolysis during infection (complement activation above basal level)
no evidence of bone marrow failure (neutro gt1500microL platelets gt120 000microL)
dysphagia abdominal pain erectile dysfunction (35)
thrombosis
reccurent infectious diseases (ORL lungs) 40 2d cause of death
risk of MDSAML 5 25 at 10y (x100)
PNH Clinical aspects
PNH associated with aplastic anemia
small PNH clone (majority of patients lt10)
clinicalbiochemical evidence of hemolysis
2 or 3 cytopenias (Hb lt10 gdL neutro lt1000microL platelets lt80 000microL)
BM failure dominates the clinical picture
PNH Clinical aspects
Subclinical PNH
clone size lt1
no hemolysis
We find PNH clone in 60 of AA and in 20 of low risk MDS(47)
associated to AA high probability of response to immunosuppressive therapy
associated to low risk MDS (refractory anemia)
less pronounced morphological abnormalities of the blood cells
more severe thrombocytopenia
lower rate of karyotypic abnormalities
higher incidence of HLA-DR15
lower rate of progression to AML
higher probability of reponse to cyclosporine
Hypothesis that aplastic anemia and a subgroup of low risk MDS are immune-mediated diseases
immunity provides the selection pressure that favors the outgrowth of PNH clone
PNH Clinical aspects (3-4)
Classic PNH Aplastic anemia-PNH
Age 40y 30y
Abdominal pain 35 20
Median clone size 916 168
Median survival 18y gt22y
Thrombotic events (at 10y) 379 278
Medullar aplasia 20 at 10y 100
PNH Pathophysiology of disease (1)
Intravascular hemolysis
free Hb in the plasma
NO fixation to Hb
NO depletion
smooth muscle dystonias
dysphagia
abdominal pain
erectile dysfunction
arterial constriction
reduced blood flow to the kidneys
arterial hypertension
pulmonary hypertension (+undiagnosed thrombosis)
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
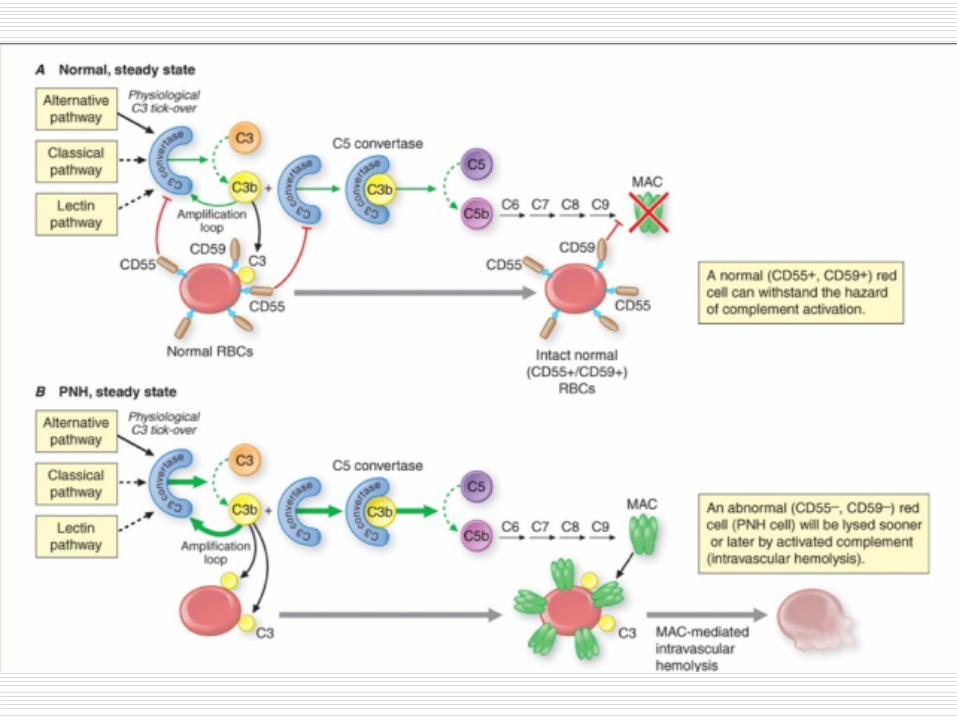
PNH Definition
Non malignant clonal expansion 2 steps hypothesis (53)
step 1 PIG-A mutation
no clonal expansion asymptomatic
step 2 injury to the normal bone marrow
T cells and NK cells attack
normal hematopoietic cells destroyedbut PNH cells escape (absence of GPI anchored targeted peptides or accessory molecules required for T cells attack)
bone marrow failure clonal expansion
PNH Diagnosis
(Ham and sucrose tests)
Flow cytometry with monoclonal antibodies that bind to specific GPI-anchored proteins (precentage of PNH cells measured)(38)
clone size
use at least 2 different monoclonal antibodies directed against 2 different GPI-anchored proteins(rare congenital deficiencies of CD59 or CD55)
on at least 2 different cells lineages(risk of falsely negative tests if only red cells are screened ndash recent hemolytic crisis or recent transfusion)
phenotypic mosaicism
PNH III cells completely deficient in GPI anchored-proteins
PNH II cells partly deficient
laquo PNH raquo I cells express GPI-anchored proteins at normal density
PNH Diagnosis
FLAER (fluorescein-labeled proaerolysin)(34)
Aerolysin = the principal virulence factor of the bacterium Aeromonas hydrophila
binds selectively and with high affinity to the GPI anchor
more accurate assessment of the GPI anchor deficit in PNH (PNH clones lt1 can be detected)
complete blood count reticulocytes LDH bilirubin haptoglobin iron stores BM aspirate and biopsy cytogenetics
PNH Clinical aspects
3 different forms (clinical polymorphism)(3 4 34)
Classic PNH
young adults
intravascular hemolytic anemia (with crisis)
Hb lt12 gdL
hemoglobinuria (in the morning)
jaundice
general symptoms (asthenia malaise)
worsening of hemolysis during infection (complement activation above basal level)
no evidence of bone marrow failure (neutro gt1500microL platelets gt120 000microL)
dysphagia abdominal pain erectile dysfunction (35)
thrombosis
reccurent infectious diseases (ORL lungs) 40 2d cause of death
risk of MDSAML 5 25 at 10y (x100)
PNH Clinical aspects
PNH associated with aplastic anemia
small PNH clone (majority of patients lt10)
clinicalbiochemical evidence of hemolysis
2 or 3 cytopenias (Hb lt10 gdL neutro lt1000microL platelets lt80 000microL)
BM failure dominates the clinical picture
PNH Clinical aspects
Subclinical PNH
clone size lt1
no hemolysis
We find PNH clone in 60 of AA and in 20 of low risk MDS(47)
associated to AA high probability of response to immunosuppressive therapy
associated to low risk MDS (refractory anemia)
less pronounced morphological abnormalities of the blood cells
more severe thrombocytopenia
lower rate of karyotypic abnormalities
higher incidence of HLA-DR15
lower rate of progression to AML
higher probability of reponse to cyclosporine
Hypothesis that aplastic anemia and a subgroup of low risk MDS are immune-mediated diseases
immunity provides the selection pressure that favors the outgrowth of PNH clone
PNH Clinical aspects (3-4)
Classic PNH Aplastic anemia-PNH
Age 40y 30y
Abdominal pain 35 20
Median clone size 916 168
Median survival 18y gt22y
Thrombotic events (at 10y) 379 278
Medullar aplasia 20 at 10y 100
PNH Pathophysiology of disease (1)
Intravascular hemolysis
free Hb in the plasma
NO fixation to Hb
NO depletion
smooth muscle dystonias
dysphagia
abdominal pain
erectile dysfunction
arterial constriction
reduced blood flow to the kidneys
arterial hypertension
pulmonary hypertension (+undiagnosed thrombosis)
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Diagnosis
(Ham and sucrose tests)
Flow cytometry with monoclonal antibodies that bind to specific GPI-anchored proteins (precentage of PNH cells measured)(38)
clone size
use at least 2 different monoclonal antibodies directed against 2 different GPI-anchored proteins(rare congenital deficiencies of CD59 or CD55)
on at least 2 different cells lineages(risk of falsely negative tests if only red cells are screened ndash recent hemolytic crisis or recent transfusion)
phenotypic mosaicism
PNH III cells completely deficient in GPI anchored-proteins
PNH II cells partly deficient
laquo PNH raquo I cells express GPI-anchored proteins at normal density
PNH Diagnosis
FLAER (fluorescein-labeled proaerolysin)(34)
Aerolysin = the principal virulence factor of the bacterium Aeromonas hydrophila
binds selectively and with high affinity to the GPI anchor
more accurate assessment of the GPI anchor deficit in PNH (PNH clones lt1 can be detected)
complete blood count reticulocytes LDH bilirubin haptoglobin iron stores BM aspirate and biopsy cytogenetics
PNH Clinical aspects
3 different forms (clinical polymorphism)(3 4 34)
Classic PNH
young adults
intravascular hemolytic anemia (with crisis)
Hb lt12 gdL
hemoglobinuria (in the morning)
jaundice
general symptoms (asthenia malaise)
worsening of hemolysis during infection (complement activation above basal level)
no evidence of bone marrow failure (neutro gt1500microL platelets gt120 000microL)
dysphagia abdominal pain erectile dysfunction (35)
thrombosis
reccurent infectious diseases (ORL lungs) 40 2d cause of death
risk of MDSAML 5 25 at 10y (x100)
PNH Clinical aspects
PNH associated with aplastic anemia
small PNH clone (majority of patients lt10)
clinicalbiochemical evidence of hemolysis
2 or 3 cytopenias (Hb lt10 gdL neutro lt1000microL platelets lt80 000microL)
BM failure dominates the clinical picture
PNH Clinical aspects
Subclinical PNH
clone size lt1
no hemolysis
We find PNH clone in 60 of AA and in 20 of low risk MDS(47)
associated to AA high probability of response to immunosuppressive therapy
associated to low risk MDS (refractory anemia)
less pronounced morphological abnormalities of the blood cells
more severe thrombocytopenia
lower rate of karyotypic abnormalities
higher incidence of HLA-DR15
lower rate of progression to AML
higher probability of reponse to cyclosporine
Hypothesis that aplastic anemia and a subgroup of low risk MDS are immune-mediated diseases
immunity provides the selection pressure that favors the outgrowth of PNH clone
PNH Clinical aspects (3-4)
Classic PNH Aplastic anemia-PNH
Age 40y 30y
Abdominal pain 35 20
Median clone size 916 168
Median survival 18y gt22y
Thrombotic events (at 10y) 379 278
Medullar aplasia 20 at 10y 100
PNH Pathophysiology of disease (1)
Intravascular hemolysis
free Hb in the plasma
NO fixation to Hb
NO depletion
smooth muscle dystonias
dysphagia
abdominal pain
erectile dysfunction
arterial constriction
reduced blood flow to the kidneys
arterial hypertension
pulmonary hypertension (+undiagnosed thrombosis)
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Diagnosis
FLAER (fluorescein-labeled proaerolysin)(34)
Aerolysin = the principal virulence factor of the bacterium Aeromonas hydrophila
binds selectively and with high affinity to the GPI anchor
more accurate assessment of the GPI anchor deficit in PNH (PNH clones lt1 can be detected)
complete blood count reticulocytes LDH bilirubin haptoglobin iron stores BM aspirate and biopsy cytogenetics
PNH Clinical aspects
3 different forms (clinical polymorphism)(3 4 34)
Classic PNH
young adults
intravascular hemolytic anemia (with crisis)
Hb lt12 gdL
hemoglobinuria (in the morning)
jaundice
general symptoms (asthenia malaise)
worsening of hemolysis during infection (complement activation above basal level)
no evidence of bone marrow failure (neutro gt1500microL platelets gt120 000microL)
dysphagia abdominal pain erectile dysfunction (35)
thrombosis
reccurent infectious diseases (ORL lungs) 40 2d cause of death
risk of MDSAML 5 25 at 10y (x100)
PNH Clinical aspects
PNH associated with aplastic anemia
small PNH clone (majority of patients lt10)
clinicalbiochemical evidence of hemolysis
2 or 3 cytopenias (Hb lt10 gdL neutro lt1000microL platelets lt80 000microL)
BM failure dominates the clinical picture
PNH Clinical aspects
Subclinical PNH
clone size lt1
no hemolysis
We find PNH clone in 60 of AA and in 20 of low risk MDS(47)
associated to AA high probability of response to immunosuppressive therapy
associated to low risk MDS (refractory anemia)
less pronounced morphological abnormalities of the blood cells
more severe thrombocytopenia
lower rate of karyotypic abnormalities
higher incidence of HLA-DR15
lower rate of progression to AML
higher probability of reponse to cyclosporine
Hypothesis that aplastic anemia and a subgroup of low risk MDS are immune-mediated diseases
immunity provides the selection pressure that favors the outgrowth of PNH clone
PNH Clinical aspects (3-4)
Classic PNH Aplastic anemia-PNH
Age 40y 30y
Abdominal pain 35 20
Median clone size 916 168
Median survival 18y gt22y
Thrombotic events (at 10y) 379 278
Medullar aplasia 20 at 10y 100
PNH Pathophysiology of disease (1)
Intravascular hemolysis
free Hb in the plasma
NO fixation to Hb
NO depletion
smooth muscle dystonias
dysphagia
abdominal pain
erectile dysfunction
arterial constriction
reduced blood flow to the kidneys
arterial hypertension
pulmonary hypertension (+undiagnosed thrombosis)
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Clinical aspects
3 different forms (clinical polymorphism)(3 4 34)
Classic PNH
young adults
intravascular hemolytic anemia (with crisis)
Hb lt12 gdL
hemoglobinuria (in the morning)
jaundice
general symptoms (asthenia malaise)
worsening of hemolysis during infection (complement activation above basal level)
no evidence of bone marrow failure (neutro gt1500microL platelets gt120 000microL)
dysphagia abdominal pain erectile dysfunction (35)
thrombosis
reccurent infectious diseases (ORL lungs) 40 2d cause of death
risk of MDSAML 5 25 at 10y (x100)
PNH Clinical aspects
PNH associated with aplastic anemia
small PNH clone (majority of patients lt10)
clinicalbiochemical evidence of hemolysis
2 or 3 cytopenias (Hb lt10 gdL neutro lt1000microL platelets lt80 000microL)
BM failure dominates the clinical picture
PNH Clinical aspects
Subclinical PNH
clone size lt1
no hemolysis
We find PNH clone in 60 of AA and in 20 of low risk MDS(47)
associated to AA high probability of response to immunosuppressive therapy
associated to low risk MDS (refractory anemia)
less pronounced morphological abnormalities of the blood cells
more severe thrombocytopenia
lower rate of karyotypic abnormalities
higher incidence of HLA-DR15
lower rate of progression to AML
higher probability of reponse to cyclosporine
Hypothesis that aplastic anemia and a subgroup of low risk MDS are immune-mediated diseases
immunity provides the selection pressure that favors the outgrowth of PNH clone
PNH Clinical aspects (3-4)
Classic PNH Aplastic anemia-PNH
Age 40y 30y
Abdominal pain 35 20
Median clone size 916 168
Median survival 18y gt22y
Thrombotic events (at 10y) 379 278
Medullar aplasia 20 at 10y 100
PNH Pathophysiology of disease (1)
Intravascular hemolysis
free Hb in the plasma
NO fixation to Hb
NO depletion
smooth muscle dystonias
dysphagia
abdominal pain
erectile dysfunction
arterial constriction
reduced blood flow to the kidneys
arterial hypertension
pulmonary hypertension (+undiagnosed thrombosis)
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Clinical aspects
PNH associated with aplastic anemia
small PNH clone (majority of patients lt10)
clinicalbiochemical evidence of hemolysis
2 or 3 cytopenias (Hb lt10 gdL neutro lt1000microL platelets lt80 000microL)
BM failure dominates the clinical picture
PNH Clinical aspects
Subclinical PNH
clone size lt1
no hemolysis
We find PNH clone in 60 of AA and in 20 of low risk MDS(47)
associated to AA high probability of response to immunosuppressive therapy
associated to low risk MDS (refractory anemia)
less pronounced morphological abnormalities of the blood cells
more severe thrombocytopenia
lower rate of karyotypic abnormalities
higher incidence of HLA-DR15
lower rate of progression to AML
higher probability of reponse to cyclosporine
Hypothesis that aplastic anemia and a subgroup of low risk MDS are immune-mediated diseases
immunity provides the selection pressure that favors the outgrowth of PNH clone
PNH Clinical aspects (3-4)
Classic PNH Aplastic anemia-PNH
Age 40y 30y
Abdominal pain 35 20
Median clone size 916 168
Median survival 18y gt22y
Thrombotic events (at 10y) 379 278
Medullar aplasia 20 at 10y 100
PNH Pathophysiology of disease (1)
Intravascular hemolysis
free Hb in the plasma
NO fixation to Hb
NO depletion
smooth muscle dystonias
dysphagia
abdominal pain
erectile dysfunction
arterial constriction
reduced blood flow to the kidneys
arterial hypertension
pulmonary hypertension (+undiagnosed thrombosis)
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Clinical aspects
Subclinical PNH
clone size lt1
no hemolysis
We find PNH clone in 60 of AA and in 20 of low risk MDS(47)
associated to AA high probability of response to immunosuppressive therapy
associated to low risk MDS (refractory anemia)
less pronounced morphological abnormalities of the blood cells
more severe thrombocytopenia
lower rate of karyotypic abnormalities
higher incidence of HLA-DR15
lower rate of progression to AML
higher probability of reponse to cyclosporine
Hypothesis that aplastic anemia and a subgroup of low risk MDS are immune-mediated diseases
immunity provides the selection pressure that favors the outgrowth of PNH clone
PNH Clinical aspects (3-4)
Classic PNH Aplastic anemia-PNH
Age 40y 30y
Abdominal pain 35 20
Median clone size 916 168
Median survival 18y gt22y
Thrombotic events (at 10y) 379 278
Medullar aplasia 20 at 10y 100
PNH Pathophysiology of disease (1)
Intravascular hemolysis
free Hb in the plasma
NO fixation to Hb
NO depletion
smooth muscle dystonias
dysphagia
abdominal pain
erectile dysfunction
arterial constriction
reduced blood flow to the kidneys
arterial hypertension
pulmonary hypertension (+undiagnosed thrombosis)
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Clinical aspects (3-4)
Classic PNH Aplastic anemia-PNH
Age 40y 30y
Abdominal pain 35 20
Median clone size 916 168
Median survival 18y gt22y
Thrombotic events (at 10y) 379 278
Medullar aplasia 20 at 10y 100
PNH Pathophysiology of disease (1)
Intravascular hemolysis
free Hb in the plasma
NO fixation to Hb
NO depletion
smooth muscle dystonias
dysphagia
abdominal pain
erectile dysfunction
arterial constriction
reduced blood flow to the kidneys
arterial hypertension
pulmonary hypertension (+undiagnosed thrombosis)
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
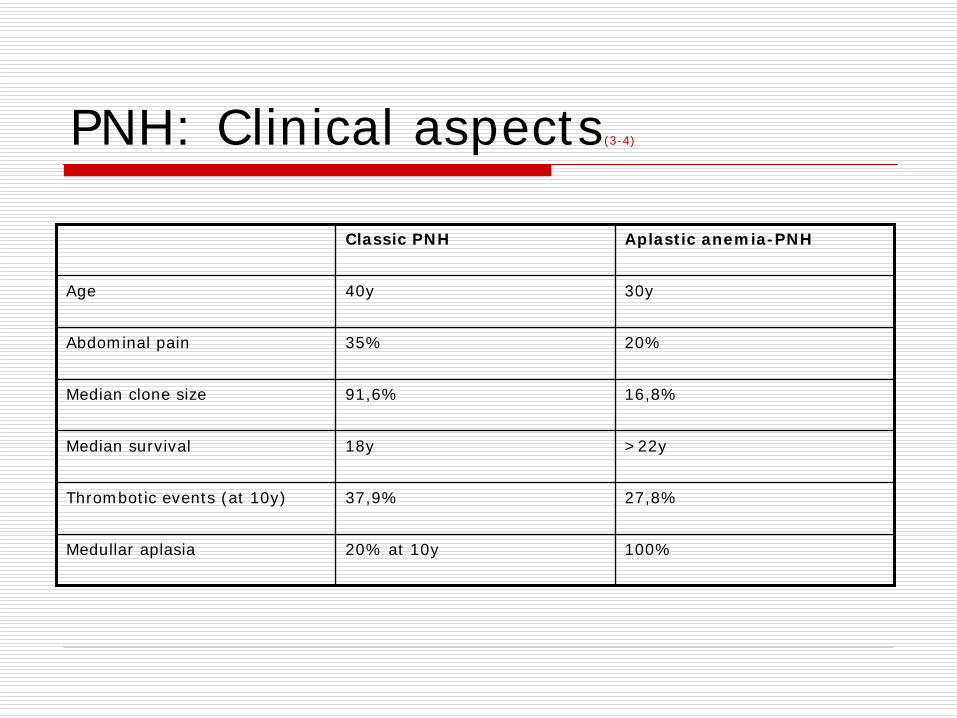
PNH Pathophysiology of disease (1)
Intravascular hemolysis
free Hb in the plasma
NO fixation to Hb
NO depletion
smooth muscle dystonias
dysphagia
abdominal pain
erectile dysfunction
arterial constriction
reduced blood flow to the kidneys
arterial hypertension
pulmonary hypertension (+undiagnosed thrombosis)
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Thrombotic events (1-2)
Occurs in 40 of PNH
Cause of death in 40-67 of patients (major cause of death)
Arterial (15) and venous (85) thrombosis
Involve more than one site (205)
Usual sites
deep veins thrombosis
pulmonary embolism
myocardial infarction
CNS arteries
and unusual sites
hepatic veins (Budd-Chiari syndrome the most frequent thrombotic complication of PNH 407)
cavernous sinus
CNS veins
mesenteric veins
dermal veins
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Thrombotic events
Age of onset lower than in general population (46y vs 73y)
Recurrences despite anticoagulant therapy described(3)
Thrombosis during pregnancy and post-partum
increased risk of thrombosis
maternal mortality 20
perinatal mortality 10
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Pathophysiology of thrombosis (1)
Unknown - multifactorialhellip
Role of hemolysis controversialhellip
no link between
severity of hemolysis and thrombosis
severity of anemia and thrombosis
NO depletion(40)
causes arterial constriction
increases platelets activation and aggregation
enhances TF expression
ADP release induce platelets activation(5)
human RBC stroma activate the alternate complement pathway(7)
interraction of activated complement components with platelets
release of PF-3
activation of coagulation
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria
Journal of Thrombosis and Haemostasis Volume 10 Issue 1 pages 1-10 4 JAN 2012 DOI 101111j1538-7836201104562x httponlinelibrarywileycomdoi101111j1538-7836201104562xfullf1
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
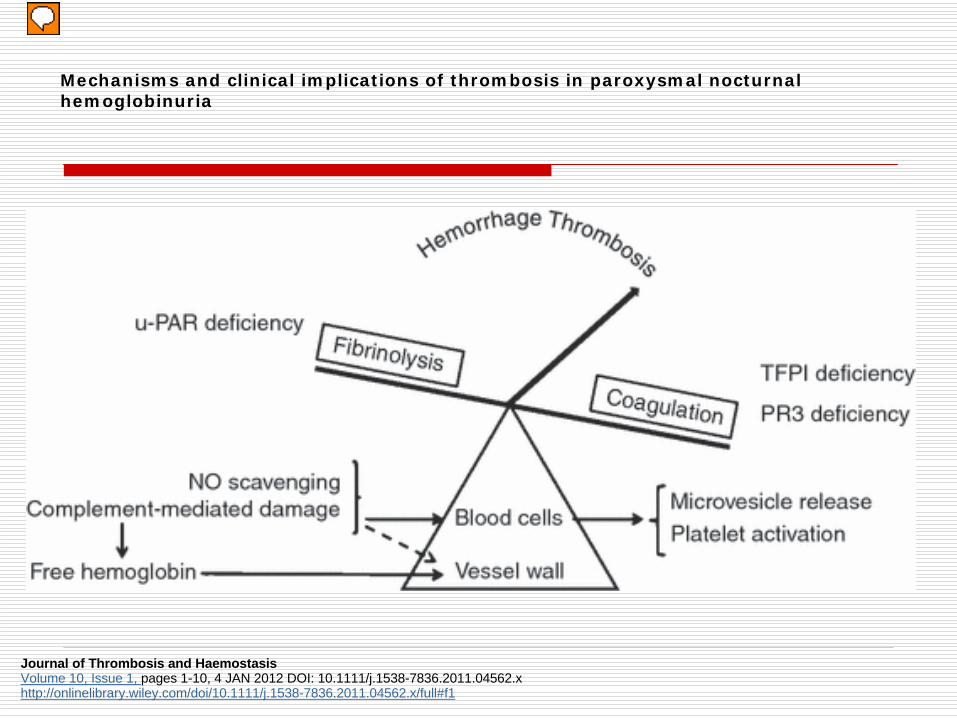
PNH Pathophysiology of thrombosis
CD59 and CD55-deficient platelets
complement can induce platelet activation
one study showed increased adherence of patelets to the abdominal vessels(1)
PNH platelets after MAC (membrane attack complex) stimulation expose more FVa-binding sites and increase thrombin generation more than normal platelets(40)
BUT other studies showed impaired function of PNH platelets (reactive downregulation in response to chronic hyperstimulation)
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Pathophysiology of thrombosis
Endothelial cells(40)
direct toxicity of free hemoglobin released
endothelial precursor cells seem to be bone marrow-derived cells
probable same GPI-anchored proteins deficiency
more susceptible to complement injury
thrombosis in unusual sites
damage resulting from the uptake of monocyte-derived MVs (released from GPI-deficient monocytes upon complement damage)
These MVs contain tissue factor thus increasing TF expression on endothelial cells
increased number of EMVs with a prothrombotic and proinflammatory phenotype in PNH
increased levels of endothelial cells activation markers (VWF sVCAM-1)
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Pathophysiology of thrombosis
Possible role of C5a protein
binds to a receptor on granulocytes
recruitement and activation of granulocytes and monocytes (enhanced in GPI-deficient white blood cells)
release of inflammatory molecules
damage the endothelium
TF expression
release of monocyte-derived MVs containing TF
= link between inflammation and thrombosis
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Pathophysiology of thrombosis
Tissue factor pathway inhibitor (TFPI)
TFPI limits coagulation initiation by inhibiting TF formation
mainly produced by the endothelium of the microvasculature
bound to GPI-anchored protein (definciency in PNH)
loss of TFPI expression has been associated with increased risk of thrombosis
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Pathophysiology of thrombosis
Neutrophil proteinase-3 (PR-3)(19)
membrane bound protein co-localized with GPI- anchored neutrophil antigen 2a
absence of neutrophil antigen 2a in PNH leads to loss of expression of neutrophil proteinase-3
PAR-1 (the predominant human platelet thrombin receptor) is a substrate for PR-3
impared down regulation of PAR-1
increased
propensity for platelet activation
PR-3 also modulates coagulation in various other ways
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Pathophysiology of thrombosis
Urokinase-type plasminogen activator receptor (u-PAR)(10131517)
central role in the regulation of haemostatic processes on cell surface
binding of u-PA (urokinase plasminogen activator) to u-PAR converts plasminogen into plasmin
involved in fibrinolysis make it localized pericellularly
GPI-anchored protein
underexpressed on cellular surface in PNH (granulocytes and monocytes)
increased concentrations of soluble uPAR (released from PNH hematopoietic cells)
impaired and displaced fibrinolytic system
Other fibrinolysis parameters
conflicting results
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Pathophysiology of thrombosis
Increased circulating MVs in PNH patients(18)
procoagulant properties of MVs (exposing PS containing TF) have been demonstrated in vitro
complement activation may stimulate the release of procoagulant MVs
no link between clone size and number of MVs
majority of them come from platelets(8)
EMVs levels are also increased in PNH patients with prothrombotic and proinflammatory phenotypes(9)
similar level of erythrocyte MVs in vivo but PNH erythrocytes release higher amounts of procoagulant MVs upon complement stimulation in vitro (may suggest rapid clearance from the circulation)(40)
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Pathophysiology of thrombosis
Increase of procoagulant activity (fact V fibrinogen fact VIII fact IX fact X and vWF)(10)
positive correlation with clone size
Frequency of congenital thrombophila factors is not increased in PNH(40)
testing for such factors may identify PNH patients at additional risk
its value for treatment decision in PNH is unknown
authors do not recommend routine testing
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Risk factors for thrombosis (1-2)
Large WBC clone(4)
clone gt50 10y cumulative incidence of thrombosis = 345
clone lt50 10y cumulative incidence of thrombosis = 53
Previous history of thrombosis
Old age (gt55y)
Use of transfusions(3)
Other Elevation of D-dimers
Indications of prophylactic anticoagulation
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Treatment of subclinical PNH and AAPNH (47)
Subclinical PNH
no symtoms no treatment
close monitoring (every 6-12 months) because expansion of the clone may occur
PNH associated with aplastic anemia
treatment of the underlying bone marrow failure syndrome (allogenic transplantation immunosuppressive therapy)
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Treatment of classic PNH
Eculizumab (Solirisreg Alexion Pharmaceuticals)(6 18 31)
humanized monoclonal antibody
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
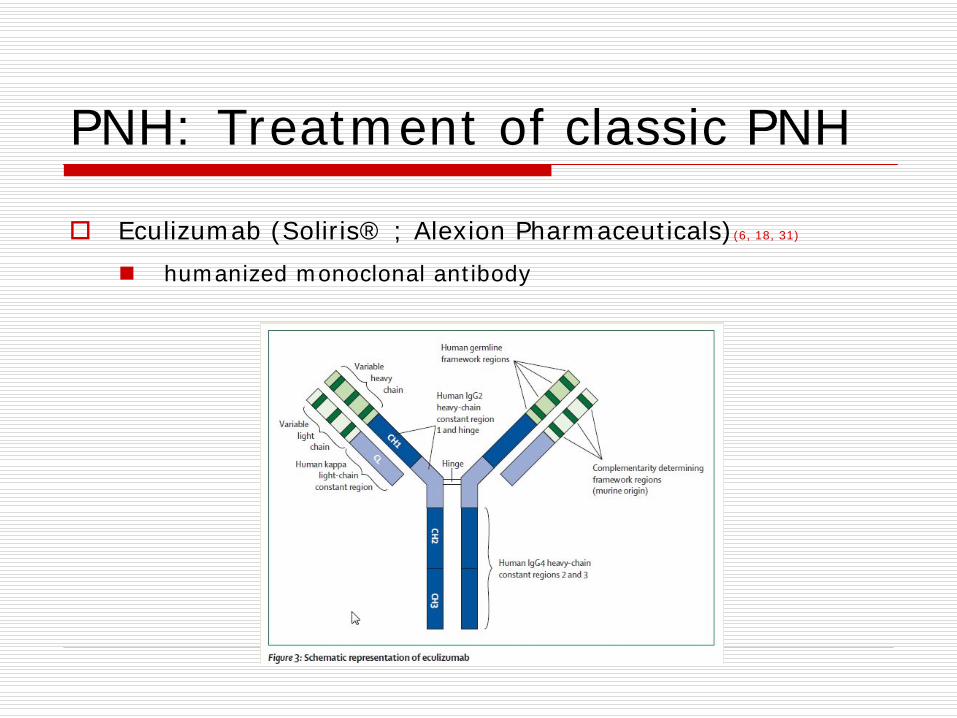
PNH Treatment of classic PNH eculizumab
blocks the activation of terminal complement C5 and prevents the formation of C5a and C5b-9
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
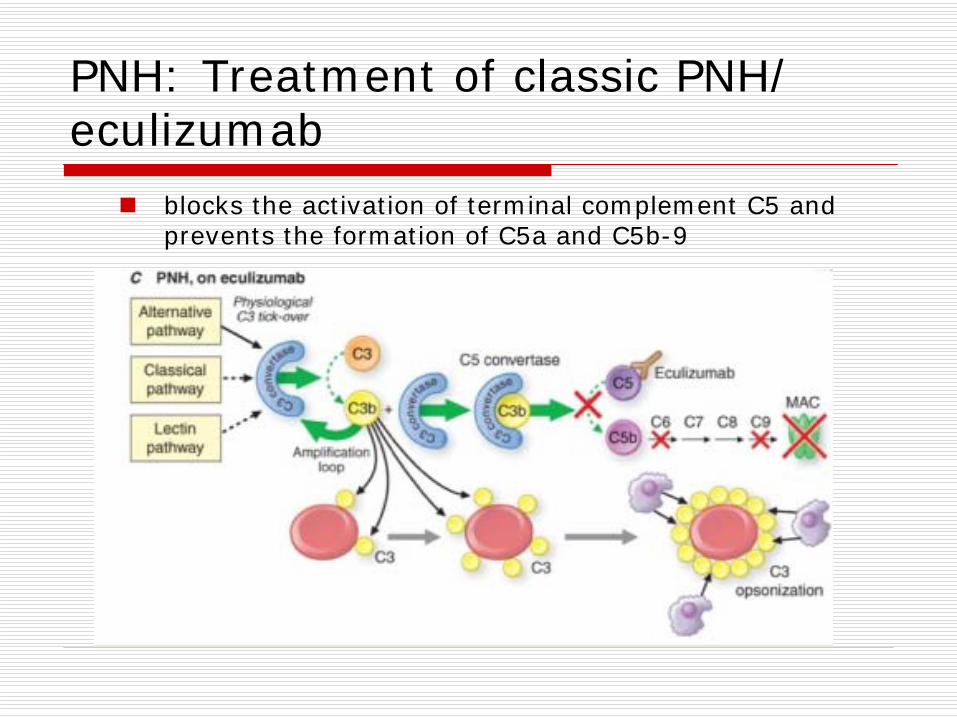
PNH Treatment of classic PNH eculizumab
administration schedule
25-45 min IV infusion
induction dose of 600 mg every 7 days for 4 doses
then 900 mg 7 days later
followed by a maintenance dose of 900 mg every 14 days
vaccination against Neisseria meningitidis at least 14 days prior to receiving eculizumab
05y risk of neisserial sepis (even after vaccination)(34)
revaccinate every 3 to 5 years
medical attention if patient develops signs of neisserial infection
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Treatment of classic PNH eculizumab
TRIUMPH (randomized placebo-controlled phase 3 study)
in transfusion-dependant PNH patients with good bone marrow reserve
reduces hemolysis transfusion requirements
improves anemia fatigue and measures of quality of life
SHEPHERD (open-label phase 3 study)(6)
to investigate the long-term safety and efficacy of eculizumab
97 patients enrolled median age 41 y follow up 52 weeks
8997 pat got a fast response and maintained complete inhibition of hemolysis
efficient
most common adverse events headache nasopharyngitis upper respiratory tract infection
83 of infections possibly related to treatment
44 SAEs (none was considered probably or definely related to treatment)
well tolerated
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Treatment of classic PNH eculizumab
Impact on overall survival
Survival for patients on eculizumab appears to be similar to that of the normal population(50)
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Treatment of classic PNH eculizumab
Reasons for suboptimal response(47-48)
breakthrough intravascular hemolysis near the end of a treatment cycle
cycles of 13 or 12 days
increase dose of eculizumab
extravascular hemolysis
Frequently persistant elevation of reticulocytes bilirubin and LDH levels presistant reduction of haptoglobin
A small group of eculizumab-treated patients little or no improvement in either anemia or constitutional symptoms
inhibition of intravascular lysis by eculizumab
increase of PNH red blood cells loaded with early components of the complement system (C3 opsonins)
eculizumab does not block the C3 convertase (not down regulated by CD55)
recognized by reticuloendothelal cells
hemolysis in the spleen (and the liver)
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Treatment of classic PNH eculizumab
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
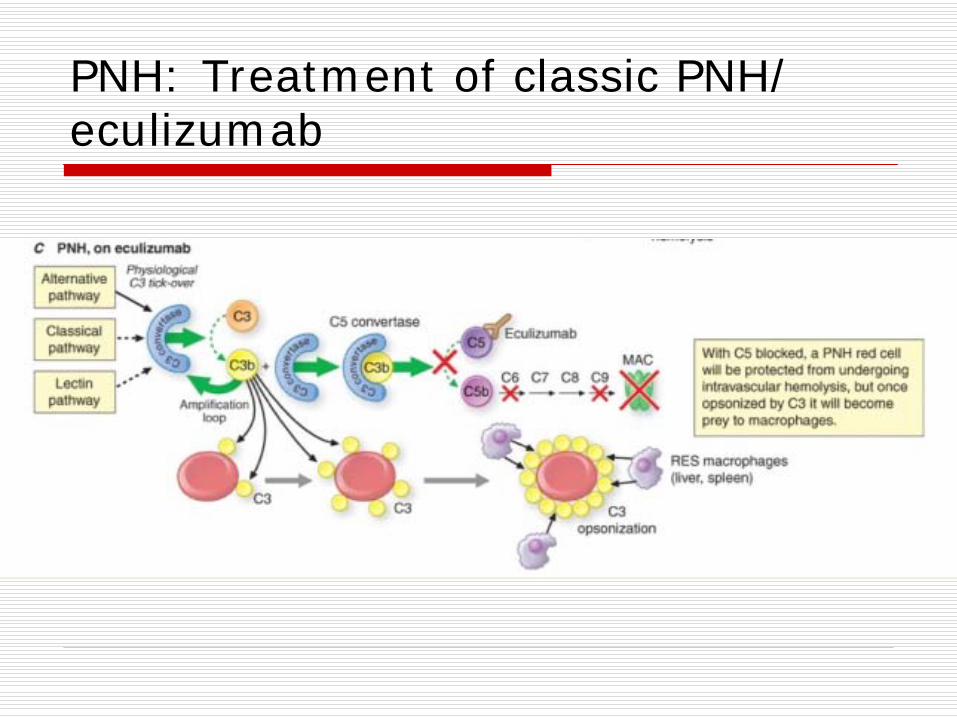
PNH Treatment of classic PNH eculizumab
What to do
No treatment if no constitutional or anemia symptoms or transfusion dependance
Corticosteroids or splenectomy
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Treatment of classic PNH eculizumab
Reduction of thombosis with eculizumab
Number of TE events and incidence rates determined in patients from 3 clinical studies with eculizumab(31)
87-94 reduction of the thrombotic events rate during eculizumab treatment
Decrease in plasma D-dimers levels with eculizumab(44)
suppression of thrombin generation
Study of markers of thrombin generation and fibrinolysis in 23 PNH patients(18)
before and after 5 and 11 w of eculizumab treatment
eculizumab reduces the activation of the plasma hemostatic system and the vascular endothelium
role of the endothelial cell activation in the pathogenesis of thrombosis in PNH
no effect of eculizumab on the number of EMVs on MVs procoagulant activity or on the number of ICAM-1 expressing EMVs
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Treatment of classic PNH eculizumab
Rapid and sustained decrease in the markers of thrombin generation and inflammation during eculizumab therapy(44)
significant reduction in D-dimers thrombin- antithrombin complex IL-6 soluble P-selectin (expressed by activated platelets and endothelial cells) TFMP (tissue factor bearing microparticles)
no link between hemolysis (LDH) and markers of thrombin generation and inflammation
the decrease of TFMP didnrsquot correlate with changes in markers of thrombin generation and inflammation
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Treatment of classic PNH eculizumab
What happens if we stop eculizumab
risk of hemolytic crisis
increased number of PNH red blood cells during eculizumab treatment
risk of thrombosis
one case described of a first thrombotic event 3 weeks after the last eculizumab dose (women died)
during anticoagulant prophylaxy (therapeutically dosed phenprocoumonMarcoumarreg)
no hemolysis
mechanism
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Treatment of classic PNH (2)
Bone marrow transplantation
the only curative option
important graft-versus-PNH effect
lack of suitable donnors
high rates of treatment-related morbiditymortality
2-year survival probability 56(34)
acute and chronic graft versus host disease 15 and 20
only for patients with life threatning cytopenias or disabling hemolysis or thrombosis that is not controlled with eculizumab
Supportive care
transfusions if needed (efficient may lessen hemolysis by suppressing erythropoiesis)
folate supplements
iron supplements if needed (hemoglobinuria hemosiderinuria) rare during eculizumab therapy (sometimes iron depletion therapy needed)
EPO increases hemolysis symptoms may be used when patients remain anemic with eculizumab and have low EPO level
corticosteroids long term toxicity use for acute hemolysis crises
androgens (Danazol) no data
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Prophylaxis of thrombosis (1-2)
Primary prophylactic anticoagulation
no randomized trials
some data suggest that warfarin effectively reduces thrombotic risk
anticoagulation in PNH patients is difficult
thrombocytopenia (aplasia liver failure)
risk of bleeding
difficult to maintain a therapeutic INR with warfarin
oesophagal spasm
mesenteric insufficiency
irregular feeding
recommendation of the international PNH interest group
consider vitamin K antagonist prophylaxis in patients with PNH granulocyte clone gt50 and no contraindications for prophylaxis
other authors say
No proven benefit for primary prophylactic anticoagulation (except pregnancy)
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Prophylaxis of thrombosis (1-2)
aspirin glycoprotein IIb-IIIa receptor antagonists
platelets may have a role in the pathophysiology of thrombosis in PNH
most thrombotic events occur in the venous system
LMWH
New oral anticoagulants (rivaroxaban dabigatran hellip)
Immunosuppressive therapy
need to define subgroups of PNH patients who could benefit from anticoagulation (risk factors)
Eculizumab is the best preventive treatment for thrombosis
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Treatment of thrombosis (1-2)
If life-threatening thrombosis
thrombolytic therapy
Anticoagulation therapy
foundation of treatement
warfarin LMWH NOAC
for how long lifelong
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
PNH Treatment during pregnancy (34)
greater need for folate and iron supplementation
prophylactic full anticoagulation with LMWH if no contraindication
example enoxaparin 1mgkg12h SC
starting when pregnancy is confirmed
monitor anti-factor Xa levels
sometimes need to switch to unfractionated heparin if a cesarean section is planned
anticoagulation has to be continued during the post-partum period
eculizumab
listed as category C pharmaceuticals (drug with little or no information available)
important potential benefit of eculizumab in reducing thrombosis
IgG2 isotypes do not cross the placenta probably little impact on the fetus
single case report eculizumab was administered to a pregnant PNH patient in week 30 of her pregnancy (twins) No complications were reported
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
Literature
1) Weitz IC Thrombosis in patients with paroxysmal nocturnal hemoglobinuria Seminars in Thrombosis and Hemostasis 2011 37(3) 315-321
2) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075(3)642-5
3) Peffault de Latour R Mary JY Salanoubat C Terriou L Etienne G Mohty M et al Paroxysmal nocturnal hemoglobinuria natural history of disease subcategories Blood 2008112(8)3099-106
4) Moyo VM Mukhina GL Garrett ES Brodsky RA Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays Br J Haematol 2004126(1)133-8
5) Hall C Richards S Hillmen P Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH) Blood 2003102(10)3587-91
6) Brodsky RA Young NS Antonioli E Risitano AM Schrezenmeier H Schubert J et al Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria Blood 2008111(4) 1840-7
7) Poskitt TR Fortwengler HP Jr Lunskis BJ Activation of the alternate complement pathway by autologous red cell stroma J Exp Med 1973138(3)715-22
8) Hugel B Socie G Vu T Toti F Gluckman E Freyssinet JM et al Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia Blood 199993(10)3451-6
9) Simak J Holada K Risitano AM Zivny JH Young NS Vostal JG Elevated circulating endothelial membrane microparticles in paroxysmal nocturnal haemoglobinuria Br J Haematol 2004125(6)804-13
10) Grunewald M Siegemund A Grunewald A Schmid A Koksch M Schopflin C et al Plasmatic coagulation and fibrinolytic system alterations in PNH relation to clone size Blood Coagul Fibrinolysis 200314(7)685-95
11) Wiedmer T Hall SE Ortel TL Kane WH Rosse WF Sims PJ Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria Blood 199382(4)1192-6
12) Gralnick HR Vail M McKeown LP Merryman P Wilson O Chu I et al Activated platelets in paroxysmal nocturnal haemoglobinuria Br J Haematol 199591(3)697-702
13) Ploug M Eriksen J Plesner T Hansen NE Dano K A soluble form of the glycolipid-anchored receptor for urokinase-type plasminogen activator is secreted from peripheral blood leukocytes from patients with paroxysmal nocturnal hemoglobinuria Eur J Biochem 1992208(2)397-404
14) Ronne E Pappot H Grondahl-Hansen J Hoyer-Hansen G Plesner T Hansen NE et al The receptor for urokinase plasminogen activator is present in plasma from healthy donors and elevated in patients with paroxysmal nocturnal haemoglobinuria Br J Haematol 199589(3)576-81
15) Plesner T Behrendt N Ploug M Structure function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor uPAR Stem Cells 199715(6)398-408
16) Ninomiya H Hasegawa Y Nagasawa T Abe T Excess soluble urokinase-type plasminogen activator receptor in the plasma of patients with paroxysmal nocturnal hemoglobinuria inhibits cellassociated fibrinolytic activity Int J Hematol 199765(3)285-91
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
Literature
17) Sloand EM Pfannes L Scheinberg P More K Wu CO Horne M et al Increased soluble urokinase plasminogen activator receptor (suPAR) is associated with thrombosis and inhibition of plasmin generation in paroxysmal nocturnal hemoglobinuria (PNH) patients Exp Hematol 200836(12)1616-24
18) Helley D Peffault de Latour R Porcher R Rodrigues CA Galy-Fauroux I Matheron J Duval A Schved J-F Fischer A-M and Socieacute G on behalf of the French Society of Hematology Evaluation of hemostasis and endothelial function in patients with paroxysmal nocturnal hemoglobinuria receiving eculizumab Haematologica 201095574-581
19) Jankowska AM Szpurka H Calabro M Mohan S Schade AE Clemente M Silverstein RL Maciejewski JP Loss of expression of neutrophil proteinase-3 a contributory factor in thrombotic risk in paroxysmal nocturnal hemoglobinuria Haematologica 2011 Jul96(7)954-62
20) Burnier L Fontana P Kwak BR Angelillo-Scherrer A Cell-derived microparticles in haemostasis and vascular medicine Thromb Haemost 2009 Mar101(3)439-51
21) Williams JC Mackman N MPs or ICs Blood 2011 Jan 27117(4)1101-2
22) Beyer C Pisetsky DS The role of microparticles in the pathogenesis of rheumatic diseases Nat Rev Rheumatol 2010 Jan6(1)21-9 Epub 2009 Dec 1
23) Owens AP 3rd Mackman N Microparticles in hemostasis and thrombosis Circ Res 2011 May 13108(10)1284-97
24) van der Pol E Hoekstra AG Sturk A Otto C van Leeuwen TG Nieuwland R Optical and non-optical methods for detection and characterization of microparticles and exosomes J Thromb Haemost 2010 Dec8(12)2596-607
25) Lacroix R Robert S Poncelet P Dignat-George F Overcoming limitations of microparticle measurement by flow cytometry Semin Thromb Hemost 2010 Nov36(8)807-18 Epub 2010 Nov 3 Review
26) Yuana Y Oosterkamp TH Bahatyrova S Ashcroft B Garcia Rodriguez P Bertina RM Osanto S Atomic force microscopy a novel approach to the detection of nanosized blood microparticles J Thromb Haemost 2010 Feb8(2)315-23 Epub 2009 Oct 19
27) Freyssinet JM Toti F Membrane microparticle determination at least seeing whats being sized J Thromb Haemost 2010 Feb8(2)311-4 Epub 2009 Oct 30
28) Lacroix R Robert S Poncelet P Kasthuri RS Key NS Dignat-George F ISTH SSC Workshop Standardization of platelet- derived microparticle enumeration by flow cytometry with calibrated beads results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop J Thromb Haemost 2010 Nov8(11)2571-4
29) Mullier F Bailly N Chatelain C Dogneacute JM Chatelain B Needs interests and limitations of calibrated polystyrene beads for flow cytometry-based quantification of biological microparticles J Thromb Haemost 2011 Jun 4
30) Jy W Ricci M Shariatmadar S Gomez-Marin O Horstman LH Ahn YS Microparticles in stored red blood cells as potential mediators of transfusion complications Transfusion 2011 Apr51(4)886-93
31) Hillmen P Muus P Duhrsen U Risitano AM Schubert J Luzzatto L et al Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria Blood 2007110(12)4123-8
32) Ziakas PD Poulou LS Rokas GI Bartzoudis D Voulgarelis M Thrombosis in paroxysmal nocturnal hemoglobinuria sites risks outcome An overview J Thromb Haemost 20075 642ndash5
33) Borowitz MJ Craig FE Digiuseppe JA Illingworth AJ Rosse W Sutherland DR Wittwer CT Richards SJ Clinical Cytometry Society Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry Cytometry B Clin Cytom 2010 Jul78(4)211-30
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
Literature
34) Brodsky RA How I treat paroxysmal nocturnal hemoglobinuria Blood 20091136522-6527
35) Hardij J Mejia J Gheldof D Varin E Michiels C Chatelain B Lucas S Mullier F Dogneacute JM The CPS disc centrifuge a new original method to detect microparticles (MPs) International Society of Thrombosis and Hemostasis July 2011 Abstract 01827
36) Kozuma Y Sawahata Y Takei Y Chiba S Ninomiva H Procoagulant properties of micrparticles released from red blood cells in paroxysmal nocturnal haemoglobinuria Br J Haematol 2011 Mar152(5)631-9 Epub 2011 Jan 17
37) Piccin A Murphy WG Smith OP Circulating microparticles pathophysiology and clinical implications Blood Rev 2007 May21(3)157-71
38) Peffault de Latour R Amoura Z Socieacute G Lrsquoheacutemoglobinurie paroxystique nocturne La revue de meacutedecine interne 31(2010) 200-7
39) Weitz IC Thrombosis in paroxysmal nocturnal hemoglobinuria- insights into the role of complement in thrombosis Thromb Res 2010 Apr125 Suppl2S106-7
40) Van Bijnen ST Van Heerde WL Muus P Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria J Thromb Haemost 2012101-10
41) Raghupathy R Derman O Response of paroxysmal nocturnal hemoglobinuria clone with aplastic anemia to rituximab Case Report Hematol 20122012106182 Epub 2012 May 7
42) Bellido M van der Velden VH Leebeek FW Te Boekhorst PA Thrombotic complications without evidence of hemolysis in paroxysmal nocturnal hemoglobinuria is eculizumab indicatedAnn Hematol 2012 Jul 4
43) Peffault de Latour R Schrezenmeier H Bacigalupo A Blaise D de Souza CA Vigouroux S Willemze R Terriou L Tichelli A Mohty M de Guibert S Marsh J Passweg J Mary JY Socie GAllogeneic stem cell transplantation in paroxysmal nocturnalhemoglobinuria Haematologica 2012 Jun 11
44) Weitz IC Razavi P Rochanda L Zwicker J Furie B Manly D Mackman N Green R Liebman HAEculizumab therapy results in rapid and sustained decreases in markers of thrombin generation and inflammation in patients with PNH independent of its effects on hemolysis and microparticle formation Thromb Res 2012 Sep130(3)361-8 Epub 2012 Apr 28
45) Liebman HA Feinstein DI Thrombosis in patients with paroxysmal noctural hemoglobinuria is associated with markedly elevated plasma levels of leukocyte-derived tissue factor Thromb Res 2003111(4-5)235-8
46) van Bijnen ST van Rijn RS Koljenovic S te Boekhorst P de Witte T Muus PPossible high risk of thrombotic events in patients with paroxysmal nocturnal haemoglobinuria after discontinuation of eculizumab Br J Haematol 2012 Jun157(6)762- 3 Epub 2012 Feb 29
47) Parker CJ Management of paroxysmal nocturnal hemoglobinuria in the era of complement inhibitory therapy Hematology Am Soc Hematol Educ Program 2011201121-9 Review
48) Roumlth A Hock C Konik A Christoph S Duumlhrsen U Chronic treatment of paroxysmal nocturnal hemoglobinuria patients with eculizumab safety efficacy and unexpected laboratory phenomena Int J Hematol 2011 Jun93(6)704-14 Epub 2011 May 25
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24
Literature
50) Kelly RJ Hill A Arnold LM Brooksbank GL Richards SJ Cullen M Mitchell LD Cohen DR Gregory WM Hillmen PLong- term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria sustained efficacy and improved survival Blood 2011 Jun 23117(25)6786-92 Epub 2011 Apr 1
51) Pu JJ Brodsky RA Paroxysmal nocturnal hemoglobinuria from bench to bedside Clin Transl Sci 2011 Jun4(3)219-24