Embed Size (px)
Citation preview

Pergamon
Int. J. Radiation Oncology Biol. Phys.. Vol. 33, No. 5, pp. 979-983, IYY5 Copyright 0 1995 Elsevier Science Inc.
Printed in the USA. All rights reserved 0360-3016/95 $9.50 + 00
0360-3016(95)02060-O
IMPLEMENTATION OF THREE DIMENSIONAL CONFORMAL RADIATION THERAPY: PROSPECTS, OPPORTUNITIES, AND CHALLENGES
SRINIVASAN VIJAYAKUMAR, M.B.B.S, DMRT AND GEORGE T. Y. CHEN, PH.D. Michael Reese/University of Chicago Center for Radiation and Cellular Oncology,
University of Chicago, 5841 So. Maryland Ave., Chicago, IL 60637
Purpose: To briefly review scientific rationale of 3D conformal radiation therapy (3DCRT) and discuss the prospects, opportunities, and challenges in the implementation of 3DCRT. Some of these ideas were discussed during a workshop on “Implementation of Three-Dimensional Conformal Radiation Therapy” in April 1994 at Bethesda, MD, and others have been discussed elsewhere in the literature. Methods and Materials: Local-regional control of cancer is an important component in the overall treatment strategy in any patient with cancer. It has been shown that failure to achieve local-regional control can lead to (a) an increase in chances of distant metastases, and (b) a decrease in the survival. In many disease sites, the doses delivered currently are inadequate to achieve satisfactory local tumor control rates; this is because in many sites, only limited doses of radiotherapy can be delivered due to the proximity of cancer to radiosensitive normal tissues. By conforming the radiotherapy beams to the tumor, doses to the tumors can be enhanced and doses to the normal tissues can be reduced. With the advances in 3DCRT, such conformation is possible now and is the rationale for using 3DCRT. However, a number of questions do remain that are not limited to the following: (a) What are the implications in terms of target volume definitions when implementing 3DCRT? (b) Are there some sites where research efforts can be focused to document the efficacy and cost effectiveness of 3DCRT? (c) How do we implement day-to-day 3DCRT treatment efficiently? (d) How do we transfer the technology from the university centers to the community without compromising quality? (e) What are all the quality assurance/quality improvement questions that need to be addressed and how do we ascertain quality assurance of 3DCRT? (f) Have we looked at cost-benefit ratios and quality of life (QOL) issues closely? Results: There is a need for defining multiple target volumes: gross tumor volume, clinical target volume(s), and planning target volume(s). Such definitions should make implementation of JDCRT more complex, yet will make high-dose delivery a possibility. There are many sites in which single and multiinstitutional studies are ongoing that include prostate, lung, head and neck, and brain. In other areas, cooperative group trials are required because of the inabiity of single institutions to accrue enough patients to answer clinically relevant questions with statistical validity. Although implementation of 3DCRT will require multiple steps, these multiple steps can be brought into clh&zal practice gradually and one does not have to wait until all steps required for implementation of 3DCRT are available. In this respect, “3DCRT” should be used in a very broad sense, from beam’s eye view blocking, use of multibeam dose distribution, use of dose-volume histograms in choosing alternative plans, noncoplanar beam arrangements, intensity modulation, inverse planning, to totally automated implementation of 3DCRT. To transfer the 3DCRT capabiities to the community from the University Centers, there is a necessity to develop quality assurance programs. RTOG and the Three-Dimensional Oncology Group are spearheading these efforts. Three-dimensional conformal radiation therapy has potential not only to improve local control and decrease toxicity, but also to improve the cost benefit ratio in the use of radiotherapy as well as in improving quality of life in patients with cancer. Conclusions: Achieving many potential benefits of 3DCRT (improvement in local control, decreasing toxicity, organs-function preservation, improvement in cost effectiveness) will require further physics-related and clinical research in carefully conceived and success~y completed future clinical trials.
Three-dimensional radiation therapy, Radiotherapy, Conformal radiotherapy.
INTRODUCTION ma1 Radiation Therapy” on April 21 and 22, 1994, at The National Cancer Institute (NCI) sponsored a work- Bethesda, MD (22). Oncologists and physicists reviewed shop on “Implementation of Three-Dimensional Confor- current status of three-dimensional conformal radiation
Reprint requests to: S. Vijayakumar, M.D., Michael Reese Hospital & Medical Center, Department of Radiation Oncology, 2929 So. Ellis Ave., Room 149 MR, Chicago, IL 60616. Acknowledgements-We thank Dr. Samuel Hellman, M.D., for
reviewing the manuscript and Ms. Evelyn Davison for secre- tarial assistance.
Accepted for publication 21 July 1995.
979
980 I. J. Radiation Oncology 0 Biology 0 Physics Volume 33, Number 5, 1995
therapy (3DCRT) and discussed plans for future research to realize the full potential of 3DCRT. Three-dimensional conformal radiation therapy is a recent advance in a series of continued improvements in radiotherapy (RT) technol- ogy since World War II. The history of RT shows that as technology has advanced, outcomes have improved (17) for many malignancies, and complication rates have declined. It is reasonable to expect similar success with 3DCRT. However, in today’s climate of health care cost containment, it is important to critically analyze the po- tential cost to benefits ratio before widely accepting a new technology. The purpose of this commentary is to briefly review (a) the scientific rationale for using 3DCRT, (b) to summarize some of the issues raised in the workshop and (c) suggest potential areas for future research. This is not meant to be a comprehensive review of the proceedings of the “workshop,” nor is it a formal report of the meeting. Only issues that are relevant to the objectives of this article discussed in the workshop are reviewed in addition to other sources.
METHODS AND MATERIALS
ScientiJic rationale for 3DCRT Radiotherapy is a local-regional modality like surgery.
Improvements in RT techniques and dose delivery result in improvements in local-regional control of disease (3, 4, S- 10). A critical question is, “How important is local- regional control?” Local-regional control is important be- cause failure to achieve local-regional control appears to (a) increase chances of distant metastases, and (b) de- crease the survival, at least in some sites (3, 4, 9, 11, 13- 15). For instance, Fuks et al. (4) and Leibel et al. (9) showed that in prostate cancer and head and neck squa- mous cell carcinoma, respectively, patients in whom local control was achieved had fewer distant metastases and improved overall survival. One significant advantage of using RT, at least in some sites, in combination or instead of surgery, is organ preservation (11). However, in many sites only limited doses of RT can be delivered due to the proximity of cancer to radiosensitive normal tissues (1). If radiotherapy beams can be made to more closely conform to the tumor, then the doses to the normal tissues can be reduced (6) and doses to the tumors can be en- hanced (5-7,19). With the advances in computer technol- ogy, such conformation is possible and is the rationale for using 3DCRT (2, 10). Many single institutional pro- spective and retrospective studies show that (a) safe dose escalation is possible in some sites (5, 7, 16), and (b) radiotherapy toxicity is lower when 3DCRT techniques are used compared to conventional techniques (16, 18- 21). To summarize, 3DCRT has the potential to improve local control and, in turn, possibly the survival, decrease toxicity, and improve quality of life. As systemic thera- pies improve, the argument for improving local-regional disease control is even more important, because recur- rence tends to occur at sites of greatest tumor bulk (12).
However, a number of questions do remain and have to be answered regarding 3DCRT (22): (a) What are the implications in terms of target volume definitions when implementing 3DCRT? (b) Are there some sites where research efforts can be focused to document the efficacy and cost effectiveness of 3DCRT? (c) How do we imple- ment day-to-day 3DCRT treatment efficiently? (d) How do we transfer the technology from the university centers to the community without compromising quality? (e) What are all the quality assurance/quality improvement questions that need to be addressed and how do we ascer- tain quality assurance of 3DCRT? (f) Have we looked at cost-benefit ratios and quality of life (QOL) issues closely?
RESULTS AND DISCUSSION
Target delineation Recent ICRU definitions need to be publicized, and indi-
vidual institutions and research groups should use these definitions consistently. There is a need for defining multiple target volumes in individual patients. Gross tumor volume (GTV) can be defined reasonably accurately for a majority of sites, although it is still problematic for some sites, e.g., brain tumors. There is a need to document the influence of physiological organ motion on GTV for different sites. Defining clinical target volumes (CTV) is more difficult than defining GTV. Clinical tumor volume should be subdi- vided to include CTV 1 and CTV 2. Clinical tumor volume 1 is potential subclinical disease extensions derived from the known natural history of site-specific neoplasms. For instance, clinically negative neck nodes in the treatment of tonsillar or nasopharyngeal carcinoma or computerized tomography (CT) negative pelvic lymph nodes in the treat- ment of squamous cell carcinoma of the uterine cervix will be considered CTV 1. Although, intuitively, radiation oncol- ogists have been defining such subclinical target volumes on the simulation films, defining them in individual CT slices is a new concept to most radiation oncologists and often need some thought and practice; this also may be time consuming in the beginning; however, defining such CTV 1 in individual disease site can lead to novel treatment tech- niques using 3DCRT, thus decreasing morbidity. One such potential example is decreasing the dose to the salivary glands in the irradiation of head and neck squamous cell carcinoma. Such CTV 1 volumes can be standardized by developing “standard anatomical catalogs” from previous and new studies delineating normal anatomical structures at risk in three dimensions. A second clinical target volume (CTV 2) is the microscopic disease extension adjacent to GTV. However, current imaging modalities do not visualize microscopic disease and currently, arbitrary margins (usu- ally l-3 cm) around GTV are used to define CTV 2. By being forced to define such CTV volumes, new thoughts and research regarding CTV 2 are likely to emerge; for instance, in the future, developments such as monoclonal antibody imaging may help define CTV 2 better. In addition,

Aspects of 3D conformal radiation therapy l S. VIJAYAKUMAR AND G. T. Y. COHEN 981
new techniques including use of noncoplanar beams and intensity modulation will emerge replacing the current prac- tice of “one-size-fit-all” use of techniques; for instance, the use of two upper lateral and a lower anterior field in the treatment of most head and neck squamous cell carcinomas. Planning target volume (PTV) is an anatomical concept that will vary from site to site; this is the margin around GTV, CTV 1, and CTV 2, depending upon physiological motion and day-to-day setup variations. Again, significant research needs to be done to document the necessary dimensions of PTV for individual organ sites.
In implementing these new concepts in target delinea- tion the following need to be considered: the nominal static treatment plan usually presented for signature ap- proval as currently implemented does not reflect absolute accuracy. Uncertainties in patient setup, internal organ movement in some parts of the body, and errors in the implementation of an image based plan result in a possi- bility of not fully delivering the prescribed dose to target volume. Recognition of the uncertainties in dose delivery have resulted in the development of new technologies to better control them, or to analyze and collect data to understand their magnitudes. Electronic portal imaging devices (EPIDS) may eventually guide daily targetry, es- pecially if radio-opaque markers are used to localize the target in the presence of internal organ motion. Choosing patient position and appropriate immobilization will re- duce setup errors. Gated treatments may evolve to reduce uncertainties associated with respiration. Recent publica- tions and presentations have described the magnitude and direction of internal organ and tumor motion by analysis of serial volumetric imaging methods. Additional studies are needed to improve the understanding and reducing the uncertainties associated with implementing 3D conformal therapy. Folding these reductions of uncertainty into the composite dose distribution will provide the radiation on- cologist with a more accurate dose map and redefine CTVs and PTVs in the future.
Potential areas of clinical research In Table 1, an attempt is made to identify potential
disease sites where prospective clinical studies may be appropriate. Two criteria-not necessarily exclusive-
need to be fulfilled to attempt dose escalation or nondose escalation 3DCRT multiinstitutional group-wide studies: (a) a documented high local failure with current radiother- apy doses and/or (b) a significant incidence of distressing toxicity/potential toxicity with or without dose escalation. In addition, a sufficient number of accessible cases are needed to design statistically viable studies. In the table, a tick mark indicates feasibility and/or ongoing clinical studies. A question mark indicates a doubt of ability to accrue a statistically sufficient number of cases in single institutions; the usefulness of 3DCRT for these sites needs to be studied by cooperative groups such as the Radiation Therapy Oncology Group (RTOG).
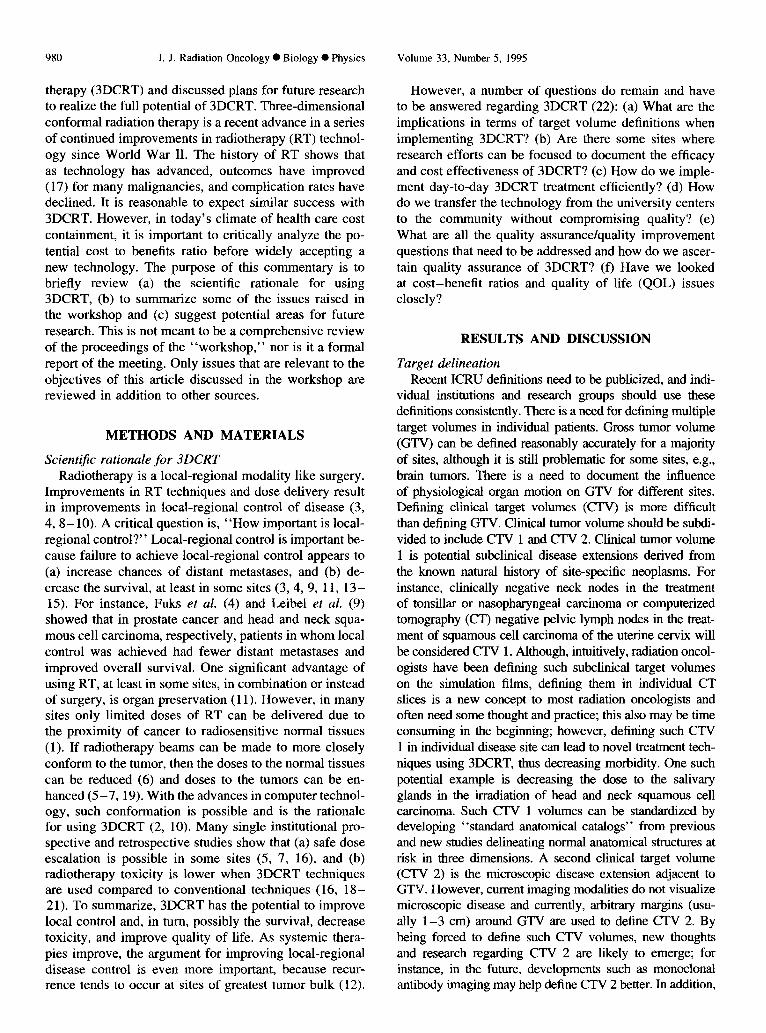
Day-to-day implementation of 3DCRT In Fig. 1, a futuristic flow chart of 3DCRT implementation
for individual patients is shown. After a patient is set up with satisfactory immobilization, a “dry run” of treatment to be implemented is performed. Such dry runs are practiced in many institutions currently and are deemed necessary to avoid accidents; most dry runs require less than 1 or 2 min of the radiotherapists’ time. A diagnostic x-ray head attached to the treatment machine can be extremely helpful because diagnos- tic quality orthogonal x-rays can be taken during the dry run However, technology has to be developed to automatically compare such daily films with simulation films, and if unsatis- factory, to make corrections automatically. The areas of future research are indicated in dotted lines in Fig. 1. The aim is to automatically carry out satisfactory, multifield treatment with instantaneous dose documentation for each portal; if, a “dis- crepancy” is found in the dose delivered, the treatment needs to be suspended immediately and corrective actions taken; significant research effort needs to be focused to achieve this, including the use of artificial intelligence. In addition, it is not yet known whether multileaf collimator (MLC) treatment is satisfactory for all sites, as well as what may be the ideal width of leaves in MLCs.
Does one have to wait until all of the above steps are achievable before implementing 3DCRT in a department? Not necessarily. Implementing some of the feasible steps at any given time is possible and may even be desirable; as data emerges from further research and new tools to imple- ment other features made available, those steps can be gradu-
Table 1.
Site
Brain Head and neck Lung- NSCLC Esophagus Pancreas Rectum Prostate Skull base Sarcomas
High local failure (type/stage)
Glioblastoma Multiforme Tz,. Tz,r N3 T,, I-z,, Nf
Yes Yes B,, C Tjr T4 Different histopathologies
-
Distressing toxicity/sensitive organ
- Xerostomia Lung, heart
Lung, Heart Small bowel Small bowel Rectum Brainstem, spinal cord Yes, in some; e.g., lymphedema
Clinical trials
J J r/
? ? ? J ? ?
982 1. J. Radiation Oncology 0 Biology 0 Physics
:.........“.............~ : ARCHIVED i
, . . . . . . . . . . . . . . . . . . . . . . . , i ANATOMICAL i .--.-.-.* TREATMENT
3D ; PLANNING ; LIBRARY i
PLANS i
: i . . ..-..................... ; : ARTIFICIAL i . . . . .
I :INTELLIGENCE i : . . . . . . . . . . . . . . . . . . . . . . . . . i
DIAGNOSTIC
(ORTHOGONAL)
MECHANICAL
1 SATIS:O*TCTORY 1
i I.. . . . . . . . . . . . . . . . . . . . . . . ., AUTO
i CORRECTION i 4 TREATMENT 1 I ;
Fig. 1. One conceptual design of the implementation of 3DCRT. The solid boxes indicate our current ability to implement 3DCRT in patients. The dotted blocks indicate the areas that require research and implementation in the future. For instance, archived anatomical 3D library and archival of alternative plans need to be developed that can automatically interact with the 3D treatment-planning process with or without the help of artificial intelligence in choosing the “right” plan from many choices. Choosing a specific plan should also take into consideration normal tissue complication probabilities (NTCP) as well as tu- mor control probabilities (TCP). Tumor control probabilities and NTCP information are not yet available for most of the tumors and normal tissues. Once a plan is chosen and simula- tion/virtual simulation has been completed, the patient will be ready to be treated. On the first day of treatment as well as subsequently, a “dry run” may be necessary to avoid accidental mechanical obstacles. If a noncoplanar, unusual portals, are to be used, orthogonal x-rays are required to ascertain accurate delivery of treatment. Currently, human interaction to ascertain such accuracy is required; however, in the future, automatic checking and automatic correction should be feasible. Another desirable feature not indicated in the figure is documentation of the actual dose delivered from each port and summation of the dose to the target from recording of such individual portal dose delivery, which will require significant future research.
ally brought in. In this respect, “3DCRT” should be used in a very broad sense, which includes beam’s eye view blocking, use of multiplane dose distribution, use of dose-volume his- tograms in choosing alternative plans, noncoplanar beam ar- rangements, intensity modulation, inverse planning, to totally automated implementation of simple or complex treatment plans based on 3D anatomy/tumor extent with methods to document actual execution of a treatment plan. In other words, any steps which help “conform” the dose delivery in radio- therapy to a target volume and implement such dose delivery should be considered “conformal therapy.”
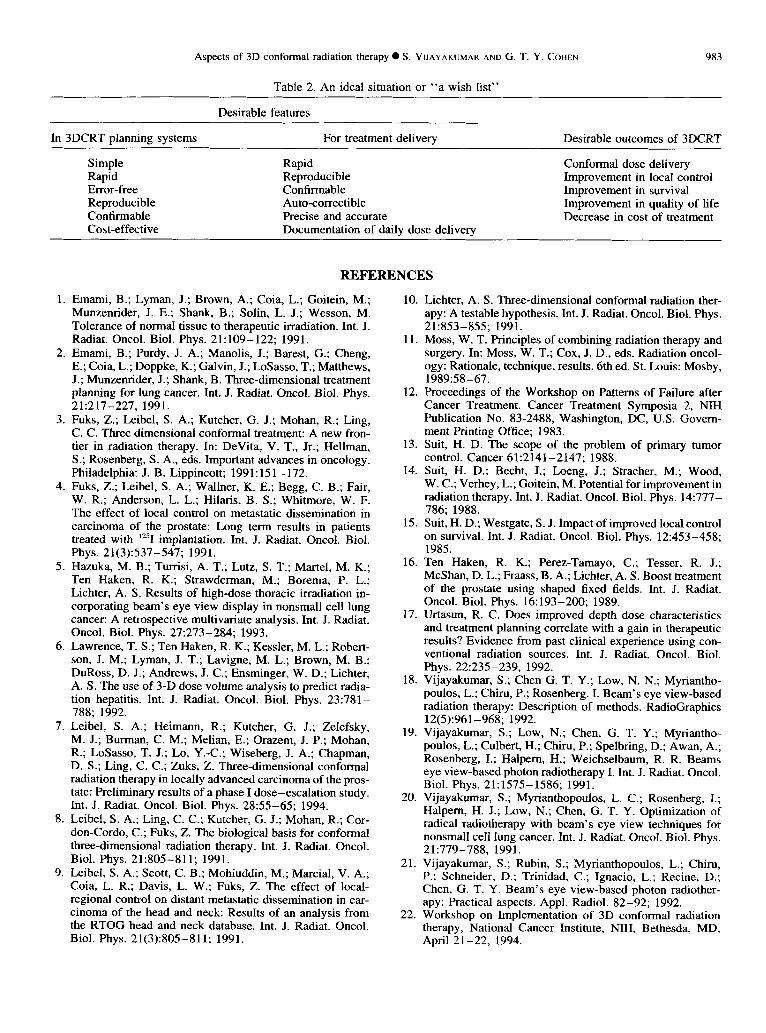
Transfer of technology to the community Some of the desirable features of 3DCRT, especially if
one wishes to transfer 3DCRT to the community, are shown
Volume 33, Number 5. 1995
in Table 2. The treatment-planning process has to be made simple and the treatment delivery rapid. If multiple fields and noncoplanar beams are to be used, more rapid treatment delivery has to be implemented. Fortunately, the multileaf collimator (MLC) has made such a requirement feasible. However, to be error free, reproducible, and confirmable, many more developments and quality assurance require- ments have to be met. On-line portal imaging is one method that can ascertain reproducibility. However, many feel that there is a need for documentation of the actual doses deliv- ered vis-a-vis just documenting the port treated. If pretreat- ment imaging demands adjustment of patient positioning, who decides the type and extent of such adjustment? It is not practical to expect a physician to be monitoring pretreatment images every day for every patient. We have to further train our radiotherapists to make such decisions and/or develop methods that will automatically implement such adjust- ments. There is also a need to recognize the differences between precision and accuracy-a precise treatment deliv- ery may not be accurate, and more research is needed in this area.
Quality assurance, cost-benefit, and quality of life issues
Currently, no mechanisms to assure quality assurance in the implementation of 3DCRT exist. However, the 3DCRT committee in RTOG as well as the quality assurance com- mittee of the Three Dimensional Oncology Group have de- veloped/are developing a number of criteria in terms of quality assurance. As we gain experience in carrying out multiinstitutional, cooperative group trials, new questions and answers to quality assurance issues are likely to emerge. Similarly, most of the studies, either from individual institu- tions or ongoing multiinstitutional studies, have mainly ad- dressed feasibility and/or outcome issues in specific disease sites with the use of 3DCRT. It will become more and more important to carefully subselect not only patients who may be benefited from 3DCRT but also may not require all steps indicated in Fig. 1, thus saving cost and time. As 3DCRT becomes more widely available and implemented, it is very important to systematically study these issues; radiation on- cologists and radiotherapy physicists who pioneered patterns of care study can use some of the knowledge and experience gained from such studies to conduct nationwide patterns of care studies in 3DCRT to ascertain their usefulness and utility, as well as influence on improving quality of life.
CONCLUSIONS
In summary, 3DCRT has the potential to not only im- prove the local control and decrease the toxicity, but devel- opments related to 3DCRT may also help deliver day-to-day radiotherapy more efficiently and cost effectively. However, achieving such goals requires further physics-related and clinical research in individual institutions and cooperative groups, as well as significant focus in addressing quality assurance, cost benefit, and quality of life issues.
Aspects of 3D conformal radiation therapy 0 S. VIJAYAKUMAR AND G. T. Y. COHEN
Table 2. An ideal situation or “a wish list”
983
Desirable features
In 3DCRT planning systems For treatment delivery Desirable outcomes of 3DCRT
Simple Rapid Rapid Reproducible Error-free Confirmable Reproducible Auto-cotrectible Confirmable Precise and accurate Cost-effective Documentation of daily dose delivery
Conformal dose delivery Improvement in local control Improvement in survival Improvement in quality of life Decrease in cost of treatment
1
2
3.
4.
5.
6.
7.
8.
9.
REFERENCES
Emami, B.; Lyman, J.; Brown, A.; Coia, L.; Goitein, M.; Munzenrider, J. E.; Shank, B.; Solin, L. J.; Wesson, M. Tolerance of normal tissue to therapeutic irradiation. Int. J. Radiat. Oncol. Biol. Phys. 21:109-122; 1991. Emami, B.; Purdy, J. A.; Manolis, J.; Barest, G.; Cheng, E.; Coia, L.; Doppke, K. ; Galvin, J.; LoSasso, T.; Matthews, J.; Munzemider, J.; Shank, B. Three-dimensional treatment planning for lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 21:217-227, 1991. Fuks, Z.; Leibel, S. A.; Kutcher, G. J.; Mohan, R.; Ling, C. C. Three dimensional conformal treatment: A new fron- tier in radiation therapy. In: DeVita, V. T., Jr.; Hellman, S.; Rosenberg, S. A., eds. Important advances in oncology. Philadelphia: J. B. Lippincott; 1991: 151- 172. Fuks, Z.; Leibel, S. A.; Wallner, K. E.; Begg, C. B.; Fair, W. R.; Anderson, L. L.; Hilaris, B. S.; Whitmore, W. F. The effect of local control on metastatic dissemination in carcinoma of the prostate: Long term results in patients treated with “‘1 implantation. Int. J. Radiat. Oncol. Biol. Phys. 21(3):537-547; 1991. Hazuka, M. B.; Turrisi, A. T.; Lutz, S. T.; Mattel, M. K.; Ten Haken, R. K.; Strawderman, M.; Borema, P. L.; Lichter, A, S. Results of high-dose thoracic irradiation in- corporating beam’s eye view display in nonsmall cell lung cancer: A retrospective multivariate analysis. Int. J. Radiat. Oncol. Biol. Phys. 27:273-284; 1993. Lawrence, T. S.; Ten Haken, R. K.; Kessler, M. L.; Robert- son, J. M.; Lyman, J. T.; Lavigne, M. L.; Brown, M. B.; DuRoss, D. J.; Andrews, J. C.; Ensminger, W. D.; Lichter, A. S. The use of 3-D dose volume analysis to predict radia- tion hepatitis. Int. J. Radiat. Oncol. Biol. Phys. 23:781- 788; 1992. Leibel, S. A.; Heimann, R.; Kutcher, G. J.; Zelefsky, M. J.; Burman, C. M.; Melian, E.; Orazem, J. P.; Mohan, R.; LoSasso, T. J.; Lo, Y.-C.; Wiseberg, J. A.; Chapman, D. S.; Ling, C. C.; Zuks, Z. Three-dimensional conformal radiation therapy in locally advanced carcinoma of the pros- tate: Preliminary results of a phase I dose-escalation study. Int. J. Radiat. Oncol. Biol. Phys. 28:55-65; 1994. Leibel, S. A.; Ling, C. C.; Kutcher, G. J.; Mohan, R.; Cor- don-Cordo, C.; Fuks, Z. The biological basis for conformal three-dimensional radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 21:805-811; 1991. Leibel, S. A.; Scott, C. B.; Mohiuddin, M.; Martial, V. A.; Coia, L. R.; Davis, L. W.; Fuks, Z. The effect of local- regional control on distant metastatic dissemination in car- cinoma of the head and neck: Results of an analysis from the RTOG head and neck database. Int. J. Radiat. Oncol. Biol. Phys. 21(3):805-811; 1991.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
Lichter, A. S. Three-dimensional conformal radiation ther- apy: A testable hypothesis. Int. J. Radiat. Oncol. Biol. Phys. 21:853-855; 1991. Moss, W. T. Principles of combining radiation therapy and surgery. In: Moss, W. T.; Cox, J. D., eds. Radiation oncol- ogy: Rationale, technique, results. 6th ed. St. Louis: Mosby, 1989:58-67. Proceedings of the Workshop on Patterns of Failure after Cancer Treatment. Cancer Treatment Symposia 2, NIH Publication No. 83-2488, Washington, DC, U.S. Govem- ment Printing Office; 1983. Suit, H. D. The scope of the problem of primary tumor control. Cancer 61:2141-2147; 1988. Suit, H. D.; Becht, J.; Loeng, J.; Stracher, M.; Wood, W. C.; Verhey, L.; Goitein, M. Potential for improvement in radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 14:777- 786; 1988. Suit, H. D.; Westgate, S. J. Impact of improved local control on survival. Int. J. Radiat. Oncol. Biol. Phys. 12:453-458; 1985. Ten Haken, R. K.; Perez-Tamayo, C.; Tesser, R. J.; McShan, D. L.; Fraass, B. A.; Lichter, A. S. Boost treatment of the prostate using shaped fixed fields. Int. J. Radiat. Oncol. Biol. Phys. 16:193-200; 1989. Urtasun, R. C. Does improved depth dose characteristics and treatment planning correlate with a gain in therapeutic results? Evidence from past clinical experience using con- ventional radiation sources. Int. J. Radiat. Oncol. Biol. Phys. 22:235-239, 1992. Vijayakumar, S.; Chen G. T. Y.; Low, N. N.; Myriantho- poulos, L.; Chiru, P.; Rosenberg. I. Beam’s eye view-based radiation therapy: Description of methods. RadioGraphics 12(5):961-968; 1992. Vijayakumar, S.; Low, N.; Chen, G. T. Y.; Myriantho- poulos, L.; Culbert, H.; Chiru, P.; Spelbring, D.; Awan, A.; Rosenberg, I.; Halpem, H.; Weichselbaum, R. R. Beams eye view-based photon radiotherapy I. Int. J. Radiat. Oncol. Biol. Phys. 21:1575-1586; 1991. Vijayakumar, S.; Myrianthopoulos, L. C.; Rosenberg, I.; Halpem, H. J.; Low, N.; Chen, G. T. Y. Optimization of radical radiotherapy with beam’s eye view techniques for nonsmall cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 21:779-788, 1991. Vijayakumar, S.; Rubin, S.; Myrianthopoulos, L.; Chiru, P.; Schneider, D.; Trinidad, C.; Ignacio, L.; Recine, D.; Chen, G. T. Y. Beam’s eye view-based photon radiother- apy: Practical aspects. Appl. Radiol. 82-92; 1992.
22. Workshop on Implementation of 3D conformal radiation therapy, National Cancer Institute, NIH, Bethesda, MD, April 21-22, 1994.