Embed Size (px)
Citation preview

Implementation of a Simple Process for Preoperative Skin Antisepsis in the Cardiovascular Population Leads to Sustained SSI Reduction in CABG Procedures
Lisa Caffery MS, BSN, RN, BC, CIC
Surgical site infections (SSIs) are associated with increased morbidity, mortality, and excess costs.1-3 A recent analysis of National Healthcare Safety Network (NHSN) data revealed the incidence of SSIs are declining slower than other hospital-acquired infections.4 This analysis included 6,263 coronary artery bypass grafts (CABGs), and revealed standard antimicrobial prophylaxis in three-quarters of CABGs was inadequate against >50% of resistant pathogens.4 Alternative strategies for SSI prevention were recommended.4
The use of 2% chlorhexidine gluconate (CHG) cloths, coupled with antibiotic prophylaxis 30 minutes prior to skin incision has been shown to reduce SSIs,5 and higher concentrations of CHG on the skin have been reported with the use of 2% CHG cloths compared with 4% rinse-away CHG solution.6
An evidence-based quality improve-ment (QI) initiative was designed to provide additional skin antisepsis for the prevention of SSIs in CABG pro-cedures. The long-standing QI initia-tive has been sustainable over the course of 4 years, with many lessons learned, improved patient outcomes, and cost savings.
CLInICAL PoPuLAtIon: Cardiovascular patients undergoing CABG procedures
QI tImeLIne: • Baselinedata:Jan-Dec2009• 1styearIntervention:Jan-Dec2010• 3yearsPost-intervention:Jan-Dec2011throughJan-Dec2012
QI teAm: A multidisciplinary team was developed to design the QI initiative. Team members consisted of cardiovascular surgeons, nurse practitioners, cardiovascular operating room staff, infectionpreventionstaff,andcardiovascularservicelineleadership.ThePlan,Do,Check,Act(PDCA)methodologywasutilizedtoguideQIefforts.
Root CAuSe AnALySIS: A root cause analysis was conducted by the QI team to identify areas for improvement. It was determined there was inconsistent preoperative patient education regarding bathing and the need for skin antisepsis. Furthermore, patients were receiving basin baths preoperatively in the outpatient surgery center if nurses perceived they were “dirty” on admission, which could wash away the protection of preoperative antimicrobial protection.
LIteRAtuRe RevIew: The QI team reviewed the literature to determine best practices and alternativesforskinantisepsis.Basedonthesefindings,thedecisionwasmadetoimplementnon-rinse 2% CHG cloths* for chin-to-toe application the night before surgery at the patient’s home and the morning of surgery in the hospital.
InteRventIonS: • TheQIteamdevelopedstandardizedpreoperativeeducationforpatientsregardingthe preoperative bathing and skin antisepsis regimen. The focus was on providing patients withasimplifiedandstandardizedprocess.• TheQIteamdevelopedstandardizedteachingpointsforthehealthcareteamregarding standardizedpreoperativebathingandskinantisepsisandtheneedforSSIprevention. Thefocuswasonprovidingstaffwithasimplifiedandstandardizedprocess.• Patientswereprovidedthe2%CHGclothspreoperativelyduringtheCardiac Rehabilitationvisitandreceivedstandardizededucationonappropriateusebyhospital staff. • Surgerystaffwereprovidedeasyaccessto2%CHGclothsforstandardizedapplication to the skin the morning of surgery and to ensure compliance with skin antisepsis.
eduCAtIon:StandardizededucationwasdisseminatedinNovemberof2009andadditionaleducation is provided on an ongoing and annual basis.
1.CDC.DatafromtheNationalHospitalDischargeSurvey.2010[cited2014]. Availablefrom:http://www.cdc.gov/nchs/data/nhds/4procedures/2010pro_ numberpercentage.pdf2.EdmistonCEJr,SeabrookGR,JohnsonCP,PaulsonDS,BeausoleilCM. Comparative of a new and innovative 2% chlorhexidine gluconate-impregnated cloth with 4% chlorhexidine gluconate as topical antiseptic for preparation of the skinpriortosurgery.AmJInfectControl.2007;35(2):89-96.3.ScottDR.thedirectmedicalcostsofhealthcare-associatedinfectionsinU.S. hospitalsandthebenefitsofprevention.Availableat:http://www.cdc.gov/hai/pdfs/ hai/scott_costpaper.pdf4.Berríos-TorresSI,YiSH,BratzlerDW,MaA,MuY,ZhuL,JerniganJA.Activity of commonly used antimicrobial prophylaxis regimens against pathogens causing coronaryarterybypassgraftandarthroplastysurgicalsiteinfectionsintheUnited States,2006-2009.InfectControlHospEpidemiol.2014Mar;35(3):231-9.5.RileyMM,SudaD,TabshK,FloodA,PeguesDA.Reductionofsurgicalsite infectionsinlowtransversecesareansectionatauniversityhospital.AmJInfect Control.2012;40(9):820-5.6.EdmistonCEJr,KrepelCJ,SeabrookGR,LewisBD,BrownKR,TowneJB. Preoperativeshowerrevisited:canhightopicalantisepticlevelsbeachievedon theskinsurfacebeforesurgicaladmission?JAmCollSurg.2008;207(2):233-9.
• Involvingcareprovidersinallsettingsintheteamhelpedtoidentifygaps leading to improved communication between patients and staff. • ThePDCAQImethodologyassistedtheQIteaminthedevelopmentofa sustainable initiative. •Developingstandardizedandsimplifiededucationaltoolshelpedensure compliance with preoperative skin antisepsis. •Continuouseducationandcommunicationisnecessarytoensure appropriate team feedback and input. • Theuseof2%non-rinseCHGclothshelpspreventSSIsaspartofa rigorous preoperative antimicrobial prophylaxis regimen.
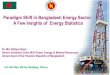
Implementationofastandardizedprocessforensuringpreoperativeskinantisepsisledtoa76.9%SSIratereductionbyend-2013frombaseline(Figure1),andacumulativeROIasaresult of cost avoidance associated with SSI prevention (Figure 2).
onGoInG QI CommunICAtIonS: • TheORManagerandDirectorarenotifiedimmediatelywhenSSIisidentified.• Theteamisassembledtorevieweachcasetodetermineiftherewereanydeviationsincare.• SSIinformationissharedattheCardiacServiceLineCommittee,SurgicalServices,and InfectionPreventionandControlCommitteemeetings.• SSIinformationissharedwithstaffattheirdailysafetyhuddles.• QISSIreportsareprovidedonmonthlyQualityScoreCardsandQuarterlyInfectionControl meetings. • ResearcharticlesaredisseminatedregardingbestpracticesassociatedwithSSIprevention as it becomes available.
ComPLIAnCe monItoRInG: TheoperatingroomnurseeducatorandCVORobservenursesduring preoperative skin antisepsis application in orientation and as part of their annual skills lab.
The author would like to acknowledge the evidence-based efforts of the entire staff in the success of this long-term QI initiative.
Sage®2%ChlorhexidineGluconateCloths(SageProductsLLC,Cary,IL)
BACkGRoundAnd RAtIonALe
metHodS
ReSuLtS
metHodS continued LeSSonS LeARned
ACknowLedGmentS
RefeRenCeS
PReSented At tHe APIC 41St AnnuAL ConfeRenCe June 7-9, 2014; AnAHeIm, CA
Disclosure:Theauthorhasnothingtodisclose.