Embed Size (px)
Citation preview

Implanting Devices –
A Practical Guide Dr Stuart Harris
Consultant Cardiologist & Electrophysiologist

Overview
• Patient preparation
• Equipment
• Incision
• Pocket formation
• Central venous access techniques
• Lead selection
• Pacing/Defibrillator parameters
• Post procedure care

Patient preparation
• Generally use left side
– More natural for operating (for right
handed operators)
– Easier to position leads (especially
atrial lead)
– 90% of patients are right handed
• Sedation (operator preference)
• Procedure field
Implantable Defibrillators
•“Oh come on, it’s just a big pacemaker”
Before you start...
• Operator
• Needs to be experienced Bradycardia Implanter
• Needs to know how the ICD works
• Needs to know about DFT testing, specifically what can go wrong and how to fix it, quickly







Implant basics
• Monitoring
• ECG, pulse oximetry
• BP- non invasive will do
• External defibrillator and pads (ICD’s)
• Spare defibrillator nearby (ICD’s)
• Aseptic technique and antibiotics
• General Anaesthetic or Sedation

GA or Local with Sedation?
• GA
• Total control
• Easier for patient
• Small risk of adverse
event due to the GA itself
• May not be readily
available
GA or Local with Sedation?
• Local with Sedation
• Less control (can still be safe)
• Potential for airway problems
• Some patients find it uncomfortable
or distressing
• No anaesthetist or anaesthetic
needed
• Readily available

Equipment

Draping

Incision
Deltopectoral incision
Oblique incision
Horizontal incision

Incision
• Operator preference
– access to both cephalic and subclavian/axillary veins
– cosmetic result
• Landmarks
– Lateral third of clavicle
– Delto-pectoral groove (indentation between clavicular
head of pectoralis major medially and deltoid laterally)
• Length of incision
– big enough for device
– longer if more subcutaneous tissue
• Local anaesthetic

Pocket formation
• Start or end of procedure?
• Subcutaneous or subpectoral?
Subpectoral implants
• The normal site for most patients is prepectoral
• Easier surgery and box change, less painful
• Fine for most patients
• You need to be able to perform a subpectoral implant if
needed
• Young patients
• Thin patients
• Mastectomy or surgery
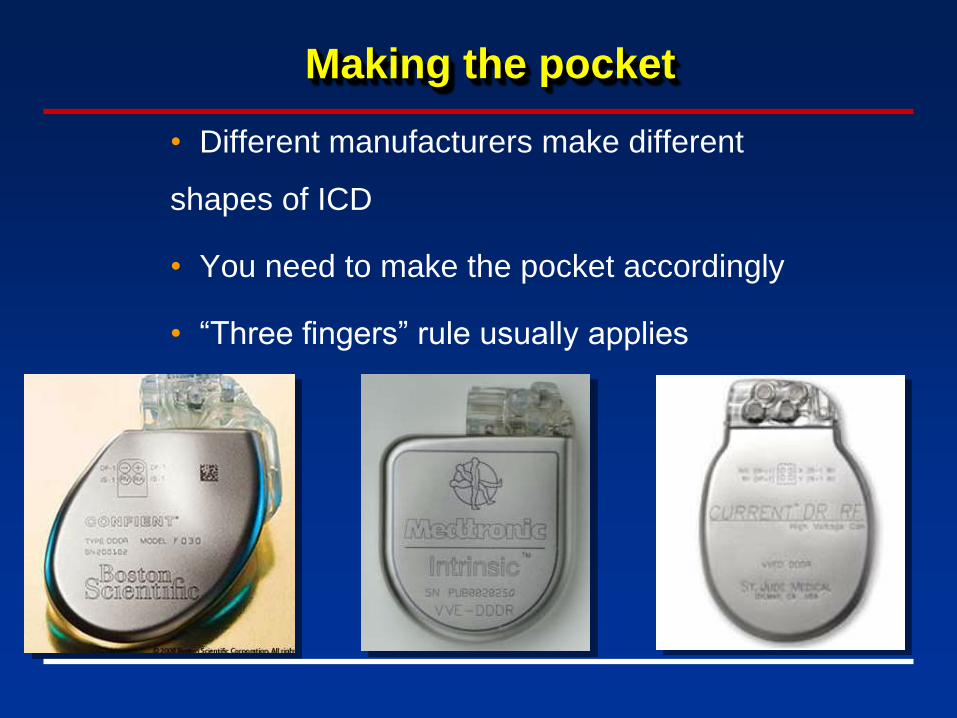
Making the pocket
• Different manufacturers make different
shapes of ICD
• You need to make the pocket accordingly
• “Three fingers” rule usually applies

Pocket formation
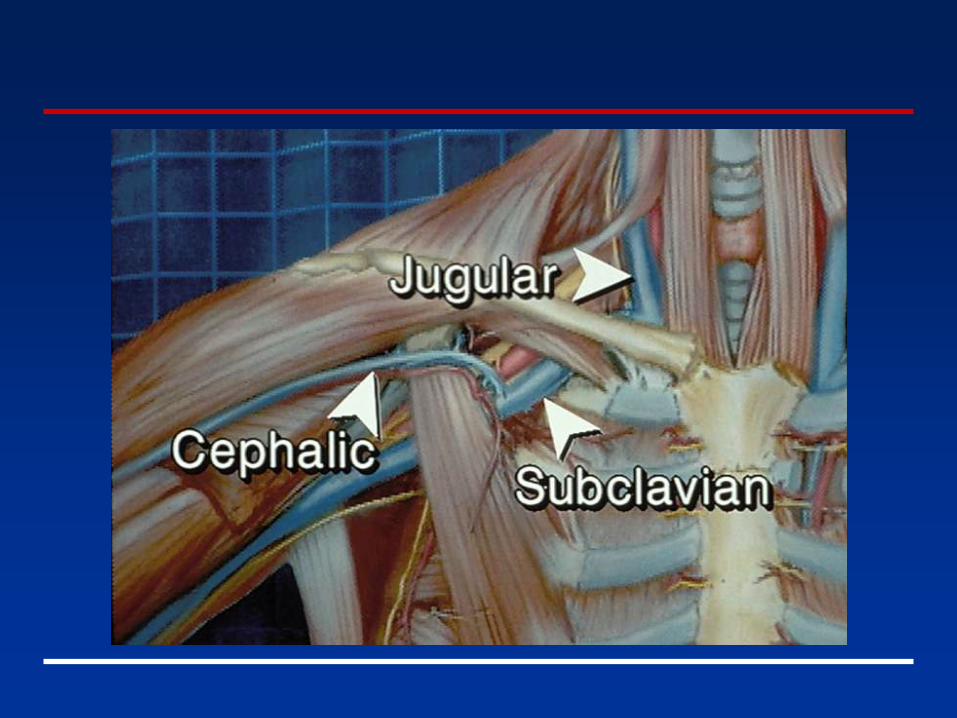
Central venous access techniques
• Cephalic vein cut down
• Subclavian vein puncture
– intrathoracic – used to it
– extrathoracic – safer
• Axillary vein puncture
• Internal jugular puncture

Cephalic vein cut down
• Advantages
– exposed during dissection and directly punctured
so no risk of pneumothorax
– may be essential (e.g. pneumonectomy/severe
COPD)
• Disadvantages
– not always present
– may not be big enough for > 1 lead
– fiddly and may increase procedure time
– technique more skilled and requires practice

Cephalic Access
Cephalic vein
Pectoral muscle


Subclavian vein puncture
• Advantages
– almost always present
– always big enough for as many leads as you need
– usually quick
– technique widely practised
• Disadvantages
– pneumothorax/haemothorax (~2% of punctures)
– risk of arterial puncture

Subclavian vein puncture
Extrathoracic
Traditional

Anaesthetise under clavicle

Subclavian puncture

Lead through sheath

Tined lead

Active (screw-in) lead

Single Coil
• 1 high voltage coil per lead:
- RV (Right Ventricle)
- Other extra HV Coils/Patches
• 1 or 2 Connector Pins - (HV only or P/S + HV)
Dual Coil
• 2 High Voltage coils per lead: - RV + SVC
• 3 Connector Pins (P/S + 2 HV)

Active or passive leads?
• More flexibility over position with active leads
• Better stability but increased risk of perforation
• Easier to extract
• Remember in young patients life expectancy of
patient often much longer than that of lead

Dual coil or single coil
• Single coil leads have slightly higher DFT than
dual coil leads
• With dual coil leads in large hearts the SVC coil
can end up in the right atrium
― Increases DFT
• Single coil leads are much easier to extract
― SVC coil can tear the SVC as it is extracted

Dual coil or single coil
• Dual coil leads
• For older patients with not too dilated hearts
• Not expected to outlive their lead
• Single coil leads
• Younger patients
• Older patients with large hearts
• Can add a standalone SVC coil if DFT is high
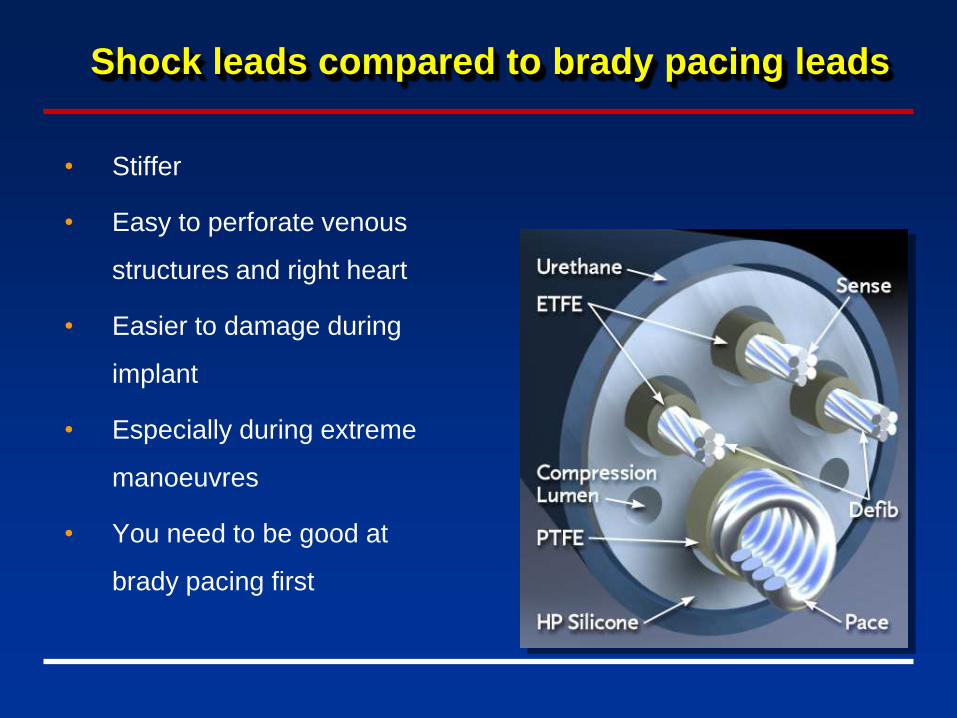
Shock leads compared to brady pacing leads
• Stiffer
• Easy to perforate venous
structures and right heart
• Easier to damage during
implant
• Especially during extreme
manoeuvres
• You need to be good at
brady pacing first

RV apex vs septum
• RV Apex
• Usually good stability and R wave
• Lowest DFTs
• Pacing from here worsens heart failure
• RV Septum
• R wave smaller, poorer stability
• Higher DFTs
• Pacing from here neutral for heart failure
• Better in combination with LV lead

Shock lead electrical parameters
• In brady pacing, the threshold is usually the most
important factor
• For ICDs, the R wave is the most important factor
• Small R waves may lead to undersensing of VF and
failure to deliver therapy
• High sensitivities to allow for small R waves lead to
oversensing of noise and inappropriate shocks

Check leads with testing cables
Suturing the leads to the muscle
• Failure to do this properly is the commonest cause
of lead displacement
• Can be difficult
― Subpectorally
― CRT-D systems
• At least two sutures per lead
― Tug each one after you have sutured to make
sure


Connecting leads and device
• Pace/ sense part of the lead has an IS-1 connector
• Same as a brady pacing lead
• Defib part of the lead has a DF-1 connector
• Shorter
• Use the diagram on the defib to tell you where to place
each lead
• If you have a single coil shock lead you need to plug
the SVC port of the device

Connecting leads and device
• Common Cock ups
• Mixing up RV, RA, LV IS-1 leads
• DF1 in IS-1 or vice versa
• RV coil connected to SVC port or vice versa
• Multiple set screws in device- not all tightened up
• SVC port not plugged
• Beware confusing labelling on some leads/ devices
• RV coil labelled as “-”, SVC coil as “+”
• Remember Proximal coil is Positive


Wound closure

Chest x-rays
• Subclavian puncture needs PA on day of
procedure
• If exclusively cephalic then does not
need x-ray
• Careful inspection for pneumothorax
• No need for lateral x-ray routinely
Chest x-rays

Chest x-rays
Questions?