Embed Size (px)
Citation preview

Cranio-maxillofacial
Implant Directions®
Vol. 12 N° 1 January 2017 English Edition
CASE REPORT: COMPLETE ORAL REHABILITATION IN ATROPHIC JAWS
WITH IMMEDIATE LOAD IMPLANTS
CASE REPORT: ORAL REHABILITATION WITH FIXED PROTESES ON IMPLANTS IN VERY ATROPHIC
MAXILARS USING BASAL IMPLANTS AND MONOPHASIC IMPLANTS
Published by IF Publishing, Germany
ISS
N 1
86
4-1
19
9 /
e-I
SS
N 1
86
4-1
23
7


Implant Directions®
1
Editorial board
Managing editor
Dr. Łukas Pałka [email protected]
Dr. Vivek Gaur [email protected]
Coordinating editor
N. N.
Editorial board (in alphabetic order) Dr. Yassen Dimitrov, Bulgaria Za. Stephan Haas, Germany Prof. Dr. Vitomir S. Konstantinovic, Serbia Dr. Valeri Lysenko, Ukraine Katarina Markova, Prague Jura Mitruschenkow, Moskow Dr. Gerald Schillig, Germany Dr. Narender Singh, India Dr. Katrin Tost, Greece
Evidence reports and Critical Appraisals
IF Research & Evidence Dept.
Single Issue Price
Euro 30 Annual Subscription
Euro 120
Copyright
Copyright ©2006 - 2015 by International Implant Foundation DE- 80802 Munich / Germany www.implantfoundation.org
Contact
CMF.Impl.dir.
ISSN 1864-1199 e-ISSN 1864-1237
Disclaimer
Hazards
Great care has been taken to maintain the accuracy of the informa- tion contained in this publication. However, the publisher and/or the distributer and/or the editors and/or the authors cannot be held responsible for errors or any consequences arising from the use of the information contained in this publication. The statements or opinions contained in editorials and articles in this publication are solely those of the authors thereof and not of the publisher, and/or the distributer, and/or the IIF. The products, procedures and therapies described in this work are hazardous and are therefore only to be applied by certified and trained medical professionals in environment specially designed for such procedures. No suggested test or procedure should be car- ried out unless, in the user‘s professional judgment, its risk is justi- fied. Whoever applies products, procedures and therapies shown or described in this publication will do this at their own risk. Because of rapid advances in the medical sience, IF recommends that in- dependent verification of diagnosis, therapies, drugs, dosages and operation methods should be made before any action is taken. Although all advertising material which may be inserted into the work is expected to conform to ethical (medical) standards, inclusi- on in this publication does not constitute a guarantee or endorse- ment by the publisher regarding quality or value of such product or of the claims made of it by its manufacturer.
Legal restrictions
This work was produced by IF Publishing, Munich, Germany. All rights reserved by IF Publishing. This publication including all parts thereof, is legally protected by copyright. Any use, exploitation or commercialization outside the narrow limits set forth by copyright legislation and the restrictions on use laid out below, without the publisher‘s consent, is illegal and liable to prosecution. This applies in particular to photostat reproduction, copying, scanning or dupli- cation of any kind, translation, preparation of microfilms, electronic data processing, and storage such as making this publication availa- ble on Intranet or Internet. Some of the products, names, instruments, treatments, logos, designs, etc. reffered to in this publication are also protected by patents and trademarks or by other intellectual property protection laws« (eg. «IF«, «IIF« and the IF-Logo) are registered trademarks even though specific reference to this fact is not always made in the text. Therefore, the appearance of a name, instrument, etc. without de- signation as proprietary is not to be construed as a representation by publisher that it is in the public domain. Institutions‘ subscriptions allow to reproduce tables of content or prepare lists of Articles including abstracts for internal circulation within the institutions concerned. Permission of the publisher is required for all other derivative works, including compilations and translations. Permission of the publisher is required to store or use electronically any material contained in this journal, including any article or part of an article. For inquiries contact the publisher at the adress indicated.

®
The Foundation of Knowledge
2017 2 CMF. Impl. Dir. Vol. 12 No. 1
COMPLETE ORAL REHABILITATION IN ATROPHIC JAWS WITH
IMMEDIATE LOAD IMPLANT*
* English translation of the Spanish original.
Authors
Dr. Manuel Espadas García
Dr. Miguel Alvarado Pastor
Dra. Miriam Espadas Domínguez
Dr. Manuel Espadas García &
Dra. Miriam Espadas Domínguez
Paseo Cordellas Nº9.1-2
08290 Cerdanyola del Vallés
Barcelona (Spain)
Tel.: (0034) 666569658
Mail: [email protected]
Dr. Miguel Alvarado Pastor
Hernan Cortes 13, bajo
46004 Valencia (Spain)
Tel.: (0034) 963034838
Mail: [email protected]
The clinical case of a 58 years old male, partially edentulous patient with pro- nounced atrophy of his jaw bones is pre- sented.
The patient did not tolerate a removable prosthesis at all.
Applying the criteria of Strategic Implan- tology, extraction of all teeth was planned and done. Then BCS® strategic implants and an immediately produced fixed and definitive prosthesis was delivered in less than one week.
Keywords
• Strategic implant®1
• Basal Implantology • BCS® implants2
• KOS® implants • Implants and immediate load • Avoid bone grafting • Avoid sinus lift • Bone atrophy and immediate loading
1 Strategic Implant® is a registered trade-mark
2 KOS® & BCS® are registered trade-marks

Implant Directions®
3
Introduction
Placement of implants in atrophic jaws is a major surgical challenge because of the limited amount of available bone structure and the lack of available surface for os- seo-integration.
The procedures of maxillary sinus lift and mental nerve displacement are frequently applied to overcome the unfavorable ana- tomical problems and to adapt their fu- ture biomechanical conditions.
Despite acceptable success rates, these approaches imply unpredictable degrees of surgical morbidity at donor and/or re- reption sites.
Patients often refuse to undergo multiple procedures which delay their oral reha- bilitation and add surgical and financial risks. The typical patient however usually accepts with greater enthusiasm the pos- sibility of an immediate surgical and pros- thetic treatment with implants, especially if the extraction and the implant place- ment is done during the same appoint- ment. They also appreciate, if the future teeth have been planned prior to insertion of the implant, because they can see the aethetic outcome in advance. If possible the insertion of fixations without flap or sinus lifting lifting should be planned. Im- plans are today not undergoing the pro- cedure of “biologic osseointegration” as it was done in the past. Instead “osseofixa-
tion” is acchieved in the 2nd and 3rd cor- tical, which barely ever resorb over the time. The implant abutments are then bent parallel to achieve greater functional and esthetic success. This also makes the lab work easier.
In this article, we are going to show the advantages of applying this surgical and prosthodontic approach with the devices which have been named Strategic Im- plant® .
“Strategic Implantology” requires know- ledge and skills necessary to enable the practitioner to carry out treatments where surgery and prosthetics are adding up to a unique and stable result. It is advisable to strictly follow the proto- cols as described in the textbooks which are provided by the International Implant Foundation, Munich since 2012 (see list of references) . The anchoring of the im- plants in the second and sometimes third cortical, as well as the polygonal distri- bution of the same are essential for the technique and durability of the result. Like- wise the periodic control of the occlusal and masticatory situation, according to the principles of Strategic Implantology.

®
The Foundation of Knowledge
2017 4 CMF. Impl. Dir. Vol. 12 No. 1
Case Report
A 58 years old Caucasian male patient re- quested rehabilitation of the masticatory system, preferably with fixed teeth due to nausea, and under psychological and functional aspects.
The patient had no hereditary or personal history pointing towards unability for re- ceiving dental imlants or medical treat- ment, nor surgery in general. He did not report drug abuse nor allergies.
Toxic habits: Patient is a smoker of admit- ted 20 cigarettes a day and a moderate drinker. He does not visit regularly den- tist and prefers a short intervention and shortest possible treatment.
Fig. 1 Partial edentulous patient, remnant teeth with poor peri-
odontal prognosis.
We consider the indication of planning a complete oral rehabilitation under the cri- teria of strategic implantology very suit- able, and the patient accepts the treat- ment. In the clinical examination, partial bimaxillary edentulism is observed (Fig. 1), with presence of 25 and 27 in upper max- illary; 32, 33, 34 and 42, 43, 44 and 45 in the lower jaw. All remaining teeth had a poor prognosis, from the point of view periodontal and not suitable for rehabilita- tion with immediate fixed prosthesis with the criteria of Strategic Implant®.
We performed the complementary explo- ration Rx panoramic orthopantomography and CBCT (cone beam CT Carestream®), observing a bone atrophy of the upper jaws (Fig. 2) and inferior (Fig. 3) Division C (compromised bone) (Classification of Misch and Judy 1985 Fig. 4).
Fig. 2 Panoramic view of TAC scan in upper maxillary , atrophy
Misch type C.
Fig. 3 Panoramic view of TAC scan in lower jaw.

Implant Directions®
5
Bone division C
Width (bone C-w): 0 to 25 mm
Height (bone C-h): < 12 mm
Angulation of occlusal loading (bone C-a) > 30 degrees
Space crown height (ECA) > 15 mm
Fig. 4 Characteristics of the atrophy, type C of Misch and Judy.
Proceed to take the study pictures, im- pressions and assembly of models in ar- ticulator. We performed a pre-operative determination of the acceptable vertical dimension (Fig. 5) and determined the po- sition of the lips in relationship to the fu- ture teeth (Fig. 6). Teeth were tried in in this position. (Fig. 7a and 7b).
Fig. 5 Record bases and oclusion rims in impression compound
for determination of the vertical dimension, lip support and in-
ter maxillary relationship.
Fig. 6 Clinical determination of lip competence.
Fig. 7a Elaboration of a try of teeth.
Fig. 7b Assessment of try teeth, clinical control of incisal expo-
sure, lip support and intermaxillary relationship.

®
The Foundation of Knowledge
2017 6 CMF. Impl. Dir. Vol. 12 No. 1
We establish the intermaxillary relation- ship (Fig. 8a, 8b and 8c) and prepare a surgical guide (Fig. 9) that guide us in the bending of the implants to place the pillars in the most appropriate prosthetic position since the placement of the pillars will be determined by the bone structure of the patient.
Fig. 8a Transfer of the upper jaw with silicone.
Fig. 8b Transfer of the lower jaw with silicone.
Fig. 8c Interrelation of jaws.
Fig. 9 Surgical guide reproducing exactly the shape of the im-
mediate provisional prosthesis.

Implant Directions®
7
We had prepared a complete combined implants and soft-tissue borne denture for upper and lower jaw preoperatively for relining on the implants immediately after surgery (Fig. 10a, 10b and 10c). The pa- tient can leave the office the same day with his immediate provisional prosthesis and start oral functionality with the advantag- es that it allows, in the sense “aesthetic- social” and in the sense of rehabilitation of the immediate masticatory function.
Fig. 10a Provisional prosthesis of the upper jaw immediately af-
ter surgery. Later, it will be relined with resin.
Fig. 10b Provisional prosthesis of the lower jaw.
Fig. 10c Provisional immediate intraoperative.
The palate of the upper denture can also be removed after the position of the up- per tooth arch has been determined.
The placement of 10 implants for imme- diate loading in the maxilla and 9 BCS®
implants in the lower jaw was planned. During surgery in the upper jaw, especially in the intercanine zone, we chose to place three KOS® implants instead of the BCS®, utilizing the opportunities & possibilities which the bone offered. (Fig. 11a, 11b and 11c).
Fig. 11a Thickening marked at the basal level secondary or in- ternal at the tuberosity level and the septum by Underwood.

®
The Foundation of Knowledge
2017 8 CMF. Impl. Dir. Vol. 12 No. 1
Fig. 11b Hourglass shape of the Mental Symphysis zone.
Fig. 11c It is observed high densification of the internal cortical at level of the mylohyoid line.
Before the surgical procedure we per- form a thorough disinfection with Beta- dine in the oral cavity incl. all teeth and the tongue. According to our experience (and logically) this step gives more savety against infection than preoperative antibi- otic therapy, which we administer only to anxious patients and more for psychologi- cal reasons than for anything else. During the surgical procedure, we observed and utilized a very compact 2nd cortical, both in the maxillary tuberositary and behind
this bone (Fig. 11a) as well as in the lingual and mylohyoid area of the mandible (Fig. 11c). This favors the stabilization of the implants enormously.
We proceeded with implants in the first quadrant, beginning distally in the tube- ro-pterygoid region, where the pterygoid wings are very low because of the atro- phy of the tuberosity zone. We reached excellent fixation in the tuberosity & the pterygoid plate of the sphenoid bone (i.e. the 2nd and 3rd cortical). We placed three BCS® implants with Ø 3.5 and 17mm, 14mm and 10mm of length.
For the instrumentation, we used initially the pilot drill BCD1, then we applied the Twist drill Ø 2.0 in 21mml or 30 mml and later placed the implant with the help of the handgrip and the AHB-adapter. Subsequently in the second quadrant we performed the extraction of 25 and 27 and placed an implant BCS® Ø 3.5 and lenght 14mm in the tuberosity zone taking advantage of the alveolus of the distal root of the molar extracted an an- other one of 10 mm for mesial. The pre- ferred method of treatment would have been however the engagement of another implant in the tubero-pterygoid plate.

Implant Directions®
9
All implant placements in the upper jaw are performed with the handgrip and with manual torque, applying percussion with a surgical hammer when reaching to the second cotical especially in the tuberosity regions, to obtain good primary anchor- age.
Between the anterior wall of the left maxillary sinus and the socket of tooth 25 we placed one implant BCS®
Ø 3.5 of 10 mml and another one ante- rior to it, thereby also until obtaining good primary stability. In such reduced bone areas with low quality of the bone, place- ment of the implant is done very carefully. as an alternative the placement of an im- plant with 5.5 mm diameter would have been a good option in this area.
In the premaxilla, due to having only 1.5 mm bone height (Fig. 12a and 12b), we initiated BCS® insertion through the pala- tal aspect of the maxilla, but dehiscence occured in the palatine wall (Fig. 12a and 12b). We changed the treatment plan and inserted three implants in the anterior re- gion (KOS® B Ø 3.2 of 12 mm in 11 and 22 and KOS® Ø 3.7 of 10 in area of 13- 14).
Fig. 12a and b Cuts of the TAC scan in premaxilla, with severe
atrophy of the same in different sections.
For this we open a flap and were able visu- alize the real anatomy. There these KOS®
implants by their conic geometry and compression design allowed comfortable insertion without fracture of the cortical bone in a flapless approach (Fig. 13).
In the lower jaw we inserted into the molar zones (posterior to the first and second molars) two implants on each side with a pilot drill BCD 1 and spiral drill Ø 2.0, us- ing a straight handpice and approximately 15.0 RpM. Insertion of the implants was done with the handgrip in lingual and

®
The Foundation of Knowledge
2017 10 CMF. Impl. Dir. Vol. 12 No. 1
Fig. 13 Making changes in the position of the cut in the TAC
scan. In the mesiodistal sense we find some areas more propi-
tious for implant placement.
Fig. 14 Angulation of the implant in its insertion in the direction
of the mylohyoid line.
distal direction right down to the the my- lohyoid line BCS®. Implants in the diameter 3.5 mmd and of 10mm length are placed (Fig. 15). For this technique the 2nd corti- cal is fully penetrated towards the floor of the mouth. In the distal mandible no endangered structures (like dangerous the sublingual arterial anastomosis) in the inter-foraminal region are to be expected.
In anterior mandibular region, which is very dense, due to the hourglass-type morphology of the mental symphysis (Fig. 14), there is no necessity to place long implants although a lot of vertical bone is visible on the radiograph. BCS® implants are placed until they reach the isthmus of the two corticals (buccal and lingual), resulting in bicortical engagement. On the panoramic picture these implants appear short, but in the clinical reality they are an- choured rigidly with almost 80 Ncm. We placed four BCS® implants of Ø 3.5mm 14mm and one of 10mm.
Fig. 15 Anterior region of the mandibular symphysis in form of
“hourglass”.
At the end of implant surgery, we adapt and reline the immediate provisional pros- thesis. For taking impressions we use impression caps for the abutment head (small or large), do an inter-maxillary registration at the correct vertical dimen- sion, and cement the temporary with a temporary cement (Fig. 10c).

Implant Directions®
11
Fig. 10c Provisional immediate intraoperative.
Subsequently, on the second day, the metal try-in was done, we determined the color of the teeth, removed some of the the stitches and performed a thorough in- tra-oral disinfection with Batadine® again.
On the third postoperative day we cemented the definitive prosthesis (Fig. 17), after the adjustment of occlusion following the parameters established by Ihde & Ihde (Libro de Recetas de la Masti- cación 4.): • AFMP (Functional Masticatory Angle
of Planas) & chewing table are sym- metrical
• the occlusal plane is parallel to the plane of Kamper
• anterior teeth are without contact both in occlusion and in mastication
• Harmonic arches of similar length and with teeth only until the anterior half of the first molars.
Fig. 16a Prosthetic wotkpiece with inclined planes vestibule lin-
gually.
Fig. 16b Basal areas of the prosthetic workpiece in contact with
the mucosa polished to highest gloss.
Fig. 17 Prosthesis cemented at 72 hours.

®
The Foundation of Knowledge
2017 12 CMF. Impl. Dir. Vol. 12 No. 1
It is important to design the prosthetic workpiece in a way that self-cleaning in possible (Fig. 16). The basal areas of the bridge (in contact with the mucosa must be polished to highest gloss) (Fig. 16a and 16b).
We then perform periodic monthly checks by adjusting the occlusion per the para- meters discussed above during the first six months. And presented radiographic control at two years (Fig. 18), in which the perfect integration of the rehabilitated system is observed, without any bone loss, no peri-implant craters (as often seen in conventional dental implantology) nor signs of perimplantitis.
Fig. 18 Radiographic control of the patient at two years of evolution. Asymptomatic patient who continues his periodic occlusion and
hygiene checks.

Implant Directions®
13
Discussion
The difficulty to rehabilitate patients with moderate or severe maxillary atrophy is evident. Following the conventional crite- ria in implantology, these rehabilitations require the alteration of the bone struc- ture prior to the placement of implants. Without this step treatment is impossible to perform or at least the chances for success are low. Hence a vast amount of patients even today and world wide remains without treatment if the conven- tional approach is used. In medical statis- tics regarding dental implant treatment all these untreated cases should be counted as failure of the conventional method, be- cause the “Intend to Treat Principle” (ITT) in medical statistics does not allow to dis- regard such patients (www.medicalforum. ch/docs/smf/archiv/de/2009/2009- 25/2009-25-011.pdf ). When we use the Strategic Implant® we are almost unlimited by lack of bone. With “Strate- gic Implantology” we can insert implants into the cortical bone structures or pil- lars such as tubero-pterygoid region, zy- gomatic region, naso-palatine buttress, nasal spine, the base of the vomer in the maxilla and below the mylohyoid line, as well as in the symphyseal and inter-foram- inal region (with or without engagement in the basal/2nd cortical) in the anterior lower jaw.
Today we have for the Strategic Implant®, the diagnostic, surgical and prosthetic
protocol available, which is necessary to perform rehabilitations with fixed pros- thesis implant supported even in atrophic jaws.
When we can bend the necks of the im- plants, at the end of the surgical stage, and this way we make the work both for the laboratory and the prosthetic dentist quite easy. In very atrophic jaws, and to obtain an acceptable aesthetic, we chose hybrid cemented metal-resin or metal-com- posite prostheses. The great challenge for the professional is to obtain very satisfactory aesthetic results, with metal- ceramic structures. This is usually more feasible when we work on non-atrophic jaws, in cases where only the clinical crowns have to be replaced without too much soft and hard tissue.
The possibility of responding to patients expectations (with or without atrophic jaws), in relation to:
• the speed of the execution of the treat- ment
• with less aggressive surgery (using technique without flapless flap) thus creating less or no postoperative pain
• the immediate rehabilitation of the full masticatory function (immediate func- tional loading)
• the obtaining of very acceptable aesthetic results. All this generates the resolution of the expectations generated by our patients.

®
The Foundation of Knowledge
2017 14 CMF. Impl. Dir. Vol. 12 No. 1
In the case of this article, the patient’s ex- pectations were satisfactorily fulfilled. Our patient had phobias to dental treatments, he is a smoker (hence he was never a can- didate for any kind of augmentation) and he desired and received in shortest time a fixed restoration. For conventional den- tal implant concepts such patients are dif- ficult to treat and in fact most treatment providers using conventional implantologi- cal approaches would reject this a case as “untreatable”.
Summary
The protocol established for the Strategic Implant® increases the success and satis- faction of our patients. The philosophy and systematics for the work with the Strate- gic Implant® (as layed out in the textbooks of Ihde S. & Ihde A. , published by the International Implant Foundation IF, Mu- nich/Germany), with unnumerable cases and research work, include large clinical experience and scientific knowledge, has offered a simple and effective technique for dental implantology.
Rehabilitation with fixed prosthe- ses even in patients with atrophic jaws are now finally possible in the regular dental office. There is no need for waiting times (healing times), nor for all kinds of regeneration surgeries and grafts.

Implant Directions®
15
Bibliography
Ihde S., Ihde A.. Introducción al Trabajo con Strategic Implant 1. International Foundation Publishing. 2015. ISBN 978-3-945889-01-5
Ihde S., Ihde A. Libro de Recetas de la Masticación. International Foundation Publishing. 2015. ISBN 987-3-9851468-8-0
Ihde S., Ihde A. Trabajo de Laboratorio en Implantes Estratégicos 6. International Foundation Publishing. 2016. ISBN 978-3-945889-13-8
Ihde S., Ihde A., Lysenko V., Konstantino- vic V.S.K, Palka L. Nueva Terminologia Si- stematica de las Areas de Hueso Cortical para Implantes Oseofijados en Implantolo- gia. Jacobs Journal de Anatomia. Jacobs Publishers. 2016.
Misch C. Implantología contemporánea. 3ª edición. Mosby-Year Book, Inc. St. Lou- is, MO 63146, USA
Dr.Marco Mozzati La carga inmediata en implantología. 2008

®
The Foundation of Knowledge
2017 16 CMF. Impl. Dir. Vol. 12 No. 1
ORAL REHABILITATION WITH FIXED PROTESIS ON IMPLANTS
IN VERY ATROPHIC MAXILARS WITH BASAL IMPLANTS AND
MONOPHASIC IMPLANTS
A Clinical Case solved with the Strategic Implant®
Authors
Dr. Miguel Alvarado Pastor
Dr. Manuel Espadas García
Dr. Miguel Alvarado Pastor
Hernan Cortes 13,
bajo 46004
Valencia (Spain)
Tel.: (0034) 963034838
Dr. Manuel Espadas García &
Paseo Cordellas Nº9.1-2
08290 Cerdanyola del Vallés
Barcelona (Spain)
Tel.: (0034) 666569658
Mail: [email protected]
Abstract
This article shows how to solve the case of a patient with a very advanced alveolar atrophy in both jaws, applying the rules of “Strategic Implantology” developed by Dr. Stefan Ihde and associated colleagues from the International Implant Founda- tion (IF), Munich/Germany. Because this system/procedure was the only prom- issing approach, the patient decided to have “Strategic Implant®” placed in the upper jaw (BCS® brand model of Ø 3.5 and lengths of 20 mm, 17mm, 14mm and 10 mm, as well as ZSI® Zygomatic screw implants Ø 4.6 in the length of 50 mm. In the lower jaw, the clinical situation allowed to place single phase/piece

Implant Directions®
17
implants KOS® and KOS B® of Ø 3,0 - 3,2 - 3,7 and 4,1 of lengths of 12, 15, 10 and 6 mm.
All implants are made of Ti6AI4V Titanium alloy (Manufacturer: Dr Ihde Dental AG, 8737 Gommiswald, Switzerland). The use of these types of implants allows the re- habilitation of patients who present very atrophic jaws, and in immediate loading.
Following the rules applied “Strategic Im- plantology” the patient can (and must) be rehabilitated in an immediate load pro- tocol, without having to undergo sinus lifts, bone grafts or lateralizations of the dental nerve. In addition the patient may use the new teeth immediately, thus re- establishing normal and adequate masti- catory function, acceptable phonetics and good aesthetics on the same day with provisionals made from resin. Later we place the definitive zirconium prosthesis within 4 days. Today there is no need to wait for “biologic osseointegration” for 6-9 months or more, as in the traditional ap- proach which also we had been performed earlier.
For cases of extreme atrophy, we even prefer to splint the implants with a metal- lic bar on the same day and to restore for a number of months with a removable denture, to allow gradual loading and peri- ods of non-loading every day (by taking the denture out).
The high speed or therapy and the pre- dictability of the treatment is greatly ap- preciated both by the patient and the treatment provider.
Keywords
• Strategic Implant®1
• Basal Implantology • BCS® Implants2
• ZSI® Implants • KOS® Implants • Immediate load Implants • Avoiding Bone Grafts • Avoiding Maxillary Sinus lift • Bone Atrophy
1 Strategic Implant® is a registered trade-mark
2 KOS® & BCS® are registered trade-marks

®
The Foundation of Knowledge
2017 18 CMF. Impl. Dir. Vol. 12 No. 1
Introduction
The traditional rehabilitation of patients with highly atrophic jaw bones involves treatments with a high degree of difficulty, because augmentations become part of the treatment plan. Such plans are usu- ally set up for the old type of „biphasic“ implants which are still used frequently. A large number of patients is however excluded from dental implant treatment. They are being told that implants cannot be implanted because of lack of bone, or that they must undergo long and painful additional interventions, such as block bone grafts, sinus elevations or lateraliza- tion of the nerve, become treatable in one step with the treatment concept explained here. Typically patiets refuse such treat- ments.
On the other hand patients nowadays de- mand more and more immediately effec- tive solutions, as well painless treatment and treatments which do not cause colla- teral damages. Also the cost-effectiveness of a treatment is an increasing concern of patients.
In this article, we demonstrate only some of the uncountable advantages of following the philosophy of work with the Strategic implant®. This system/technology really and finally breaks the rules and dogmata that were established powerful in the (from our todays perspective) historical field of oral implantology. The technolo-
gy improves our treatment options, it is very bone based and yet innovative. The concept of the Strategic Implant® is a true
game changer in the world of oral implanto- logy, its the easy to pass-through door to a new life both for patients and for treat- ment providers. In summary, these are the concepts of Strategic Implant®:
Discipline and protocol in the preparation of
the prosthesis
The prosthesis must follow very easy but strict parameters, such as; The splinting of the implants in the framework of a rigid structure, the shape of the rounded parts without sharp edges and of course, a very stable occlusion, leaving the posterior are- as (behind the 1st molar) free from teeth and contacts. And all can be done in a time record.
Precise surgery is the basis of the treatment Any surgery, whatever it may be, should always be well planned. But with Strate- gic Implant®, especially when we work in atrohpied cases, we need good knowledge of the anatomy and we should be prepar- ted to take advantage of the clinical ana- tomy as we find it, actually feel it durign surgery and implant-bed preparation. We have to be aware that we are working with atrophied maxillae and with rests of ba- sal bone, where clever implant choice and favourable positioning of the implants are fundamental to the success of the treat- ment. In addition, we must have an ex- cellent anatomical knowledge of the two

Implant Directions®
19
jaws and the surrounding hard and soft tissues; To search bone for anchoring in the 2nd or 3rd cortical and to reach these corticals safely, requires experience and somtime patience.
Clinical Case
A 43-year-old female patient (healthy, non- smoker), without systemic diseases asked us for a rehabilitation with implants. Duri- ng the examination, the patient presents the 1st and 3rd quadrant edentulous, fixed prosthesis from 12 to 28 and another fixed prosthesis bridge from 34 to 45 and finally old 3 biphasic implants with cemen- ted crowns in the lower right mandible (Fig. 1).
Fig. 1 Preoperative orthopantomography.
On the panoramic overview we find severe atrophy in the edentulous areas, rests of roots, and we assume that there are even residual infections. The patient states that she is very unhappy with the aesthetics of her prosthesis, in addition to the dis- comfort caused by the leakage of this and the bad odors stemming from it. She also confesses that she is unable to wear the two removable dentures because they cause nausea and they are too unstable in function. All this has led to her request the treatment with implants.

®
The Foundation of Knowledge
2017 20 CMF. Impl. Dir. Vol. 12 No. 1
The patient had previously consulted with a number of other treatment providers and he had been told that she was not a candidate for a rehabilitation with im- plants or that she had to undergo pre-im- plantological interventions (bilateral sinus lift, bone-block grafts and possible latera- lization of the lower alveolar nerve in the 3rd quadrant), Another solution that was given was to place 6 implants in the upper jaw and 4 in the lower jaw, rehabilitating with two hybrid prostheses, which the pa- tient rejected however immediately becau- se of their characteristics.
We offered the following treatments to her: extraction of all teeth and root rests, (since almost all the teeth were very dete- riorated by caries, utilization of the alrea- dy existing three biphasic implants which were well integrated, and to add a number of Strategic Implants as per the rules of Strategic Implantology in the upper jaw (BCS® and zygomatic ZSI® - Manufacturer: Dr. Ihde Dental AG, 8737 Gommiswald, Switzerland) and in the lower jaw insertion of single-phase implants (KOS® and KOS B®). An immediate provisional prosthe- sis of resin and later a definite zirconium prostheses were also part of the treat- ment plan.
Fig. 2 Postoperative orthopantomography, shows the strategic implants placed; (Basal BCS® and zygomatic ZSI®) in the upper jaw and KOS® single phase implants in the lower jaw as well as the three biphasic implants previously carried by the patient.

Implant Directions®
21
Method and Materials
The patient is given an upper and lower TAC scan, and study models and bite re- gistrations were taken for the preparation of the provisional prostheses, so that they would be available on the day of surgery.
On the day of surgery, the bridges were removed and the teeth and roots were extracted and 7 BCS® strategic implants are placed in the anterior zone of the up- per jaw, 5 of them looking for anchoring in the floor of the nose and 2 of them in the naso-maxillary buttress.
ZSI® strategic zygomatic implants (2 on the right side and 2 on the left side) are also placed, and in the 2nd quadrant at the level of the tuberosity a strategic BCS® im- plant with anchorage in the cortical of the sinus floor and the tuberosity, whereas in the first quadrant at the level of the tube- rosity a single - phase KOS® implant was placed, looking for the anchorage in the plate of the pterygoid process of the sphe- noid bone.
Fig. 3 Radiographic appearance showing the BCS® Strategic Implants in the anterior group and the naso-maxillary buttress.
Fig. 4 and 5 Radiographic sections of the scanner where the strategic zygomatic ZSI implants are observed on both sides.
ZSI® strategic zygomatic implants fea- ture a fully polished surface, Ø 4.6 and lengths ranging from 35mm to 55mm. These characteristics allow the placement of implants for anchorage in the body of the zygomatic bone, right through the si- nus without causing large destructions or opening of the same, causing maximum a

®
The Foundation of Knowledge
2017 22 CMF. Impl. Dir. Vol. 12 No. 1
Fig. 6 and 7 Radiographic sections of the scanner showing the most distal implants, one with anchorage in the cortical of the sinus floor and the other in the cortical of the pterygoid.
slight, passager inflammation, facilitating a quick recovery and obtain with these im- plants a very strong and secure ancho- rage to fully rehabilitate the patient with his fixed prosthesis.
In the lower jaw, we proceeded to per- form the extractions of the teeth and
took advantage of the 3 biphasic implants already carried by the patient. First, 6 KOS® implants were placed in the ante- rior zone and then 2 more KOS implants in the 3rd quadrant. Another implant was then placed in the 4th quadrant. Once all the implants were placed, the abutments were bent and grinded for better paralle- lity and hence easier prosthetic handling. We proceeded to take the impressions and bite and vertical registration for the preparation of the fixed prosthesis in the dental laboratory.
Immediately the provisional prostheses were inserted and ground, the occlusion was adjusted. In the rest of the remai- ning 4 days various try-ins were made, and adjustments of occlusion and masti- catory function was done. The finishing and cementing of the definitive zirconium prosthesis was done on day 4. The occlu- sal and masticatory concept followed the rules given by Ihde & Ihde in the „Cook- book Mastication“. These rules are today the world-wide accepted standard for this technology. Subsequently the appropriate radiographic controls are performed, as well as possible occlusal and masticatory adjustments.
Implant Directions®
23
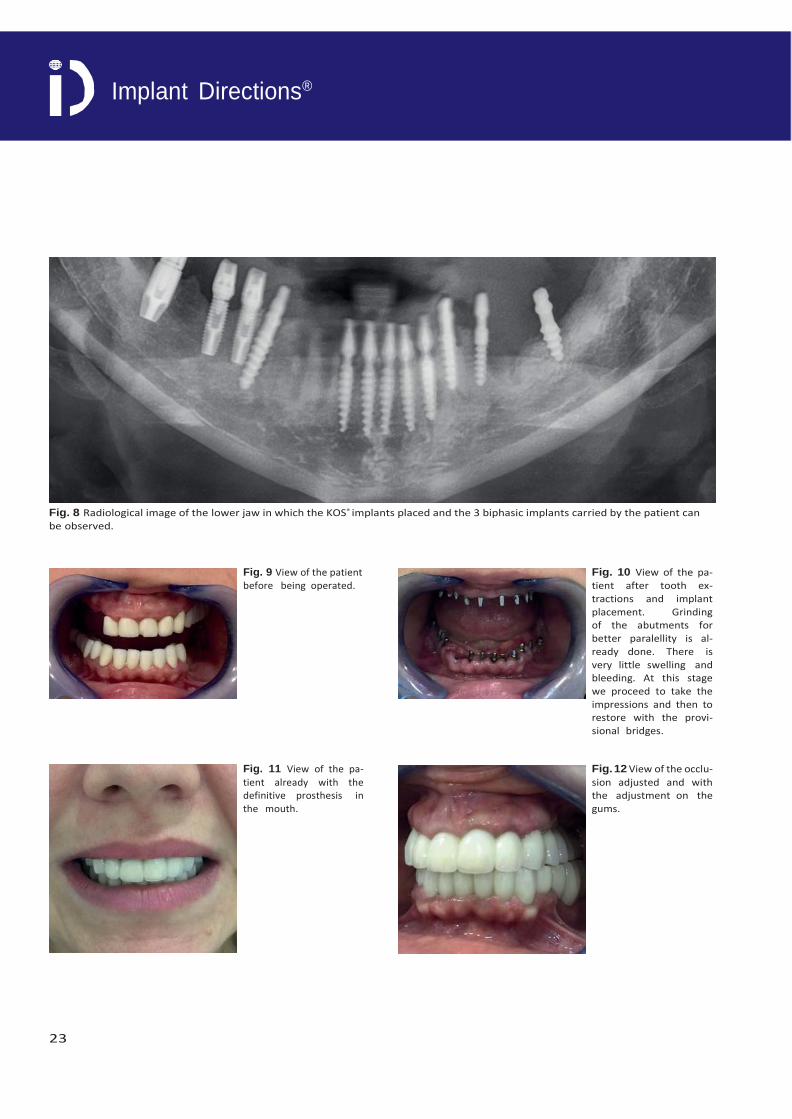
Fig. 8 Radiological image of the lower jaw in which the KOS® implants placed and the 3 biphasic implants carried by the patient can be observed.
Fig. 9 View of the patient before being operated.
Fig. 10 View of the pa- tient after tooth ex- tractions and implant placement. Grinding of the abutments for better paralellity is al- ready done. There is very little swelling and bleeding. At this stage we proceed to take the impressions and then to restore with the provi- sional bridges.
Fig. 11 View of the pa-
tient already with the definitive prosthesis in the mouth.
Fig. 12 View of the occlu-
sion adjusted and with the adjustment on the gums.
®
The Foundation of Knowledge
2017 24 CMF. Impl. Dir. Vol. 12 No. 1
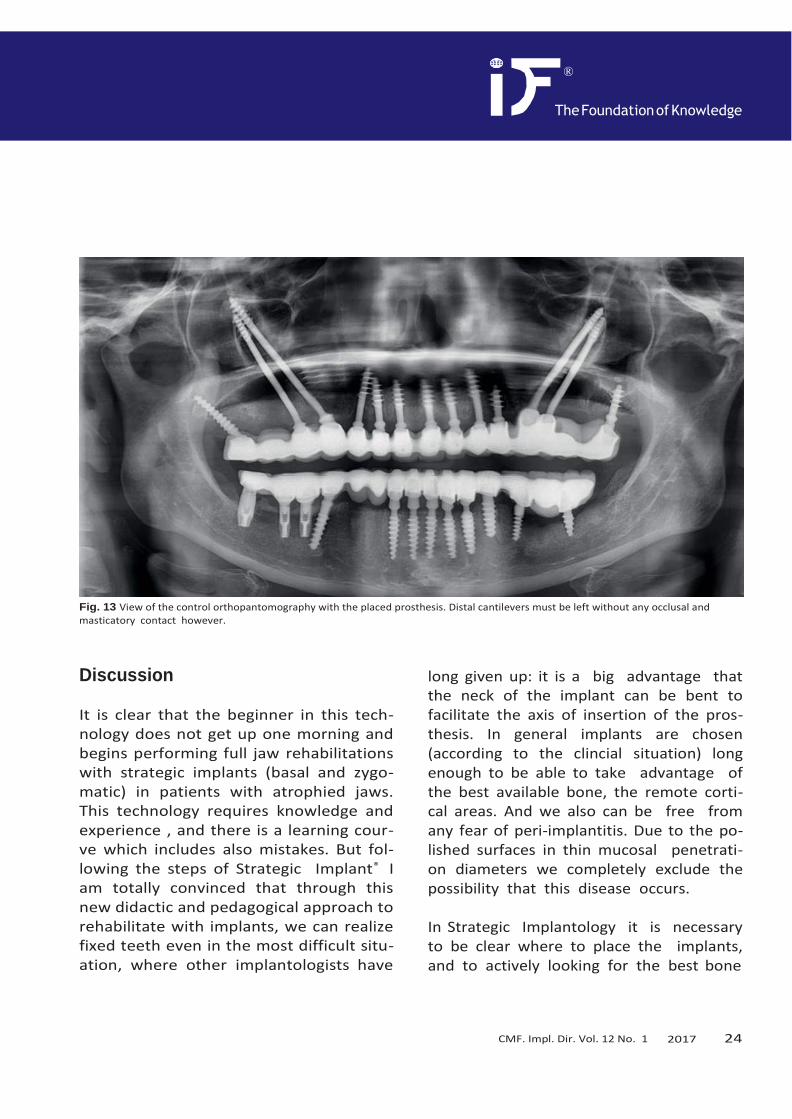
Fig. 13 View of the control orthopantomography with the placed prosthesis. Distal cantilevers must be left without any occlusal and masticatory contact however.
Discussion
It is clear that the beginner in this tech- nology does not get up one morning and begins performing full jaw rehabilitations with strategic implants (basal and zygo- matic) in patients with atrophied jaws. This technology requires knowledge and experience , and there is a learning cour- ve which includes also mistakes. But fol- lowing the steps of Strategic Implant® I am totally convinced that through this new didactic and pedagogical approach to rehabilitate with implants, we can realize fixed teeth even in the most difficult situ- ation, where other implantologists have
long given up: it is a big advantage that the neck of the implant can be bent to facilitate the axis of insertion of the pros- thesis. In general implants are chosen (according to the clincial situation) long enough to be able to take advantage of the best available bone, the remote corti- cal areas. And we also can be free from any fear of peri-implantitis. Due to the po- lished surfaces in thin mucosal penetrati- on diameters we completely exclude the possibility that this disease occurs.
In Strategic Implantology it is necessary to be clear where to place the implants, and to actively looking for the best bone

Implant Directions®
25
available, the best and most stable areas of anchorage of the 2nd and/or 3rd corti- cal. We utilize areas which are not prone to resorption, and allow the transmission of large masticatory loads. We set up a supporting polygon in which the mastica- tory slopes and occlusal contact-points should be located. The occlusal faces of the prostheses form part of the transmis- sion of the load together with the implants and their position in the bone, all closely together form strategic positions (hence the meaning of the name of the concept „Strategic Implantology“) that makes the success of the treatment.
The combination of all these fragments are thought to conform to a living form which constitutes a whole, as it is; bone, chewing forces and how these are trans- mitted by the implants and in turn the ske- letal architecture of the jaws.
When I sit down with the patient to plan the treatment, knowing well about all the possibilities which the native bone provi- des, and listening to their wishes and ex- pectations, I can today explain to them that we are going to perform a rehabilita- tion that meets their demands fully. Also I am satisfied when I can tell them that this result will be reached in a very simple manner and almost right away.
We have been using the technology of the Strategic Implant® (BCS brand: Manufac- turer: Dr. Ihde Dental AG/ Switzerland)
for 5 years in our clinic, and we consider this method to be by far superior to the traditional technique which we have used for many years before.
We do not have the intention to return to the previous (historic) technology of 2-stage implantology, nor are we (or the patients) interested to go risky and ex- pensive bone augmentations or even bone transplants.
Some of the big advantages of the new technology are described here. In our view very advantageous is the fact that we have full control over the process of surgical „osseo-fixation“, and we do not depend on „biologic osseo-integration” for the success of the treatment. When using the old technique we never knew why implants failed. Today, with the new technology we do have a defined treat- ment protocol and we can know why our implants fail if they do. This technology of the Strategic Implant® is a real game changer in dental implantology. It opens a new world of treatment possibilities.

®
The Foundation of Knowledge
2017 26 CMF. Impl. Dir. Vol. 12 No. 1
Summary
The evolutionary step to save “Immediate Loading” is to carry out the rehabilitations of our patients with the guidelines of Stra- tegic Implant®, that guarantee and mini- mize the risks, increasing the success and satisfaction of our patients in a safe and calm way. It is evident that these rules dif- fer from conventional (historical) concepts in dental implantology and new rules and guidelines must be learned. This is hard but not impossible, and in any case is ea- sier than placing grafts.
The philosophy and methodology for the work with the Strategic Implant® is based on the scientific evidence of Immediate Load implants at was layed out in text- books and articles by Dr. Stefan Ihde and Cols. in the International Implant Founda- tion (IF, Munich/Germany), with a long biography and large amount of case se- ries. A tremendous amount of research work was carried out all over the world, providing a high level of clinical experience and scientific knowledge, which has grea- tly simplified the technique and has layed ground for teaching to transmit it to the scientific world of health.
The most important change has to be made in our heads: as treatment provi- ders we have to understand that all our patients can now carry implants and fixed teeth all their life, and that it is not ne- cessary to perform bone grafts or to deli-
ver removable dentures. We only have to follow a new clinical approach and forget what we did in earlier years (although it often worked). The new approach was in- vented and described by the team around the german dentist Dr. Stefan Ihde (www. ihde.com).
Strategic Implant® provides for us the ne- cessary tools to be the number one in our area to be able to provide the best ser- vice to our patients and to differentiate us from the rest of the professionals.
The beginner should work under supervisi- on for some time. In any case it is neces- sary to correct all mistakes immediately . The Strategic Implant® revolutionized my way of rehabilitating my patients, they are eternally thankful, just as I am thankful to my teachers. The work with the Strategic Implant has taken my clinic to a new level. Without Strategic Implant® guidelines, I would never have rehabilitated my pati- ents in any way so satisfactory for them, realizing for them rehabilitations that allo- wed immediate and almost care-free life with fixed teeth.

Implant Directions®
27
Bibliography
Ihde S., Ihde A.. Introducción al Trabajo con Strategic Implant 1. International Foundation Publishing. 2015. ISBN 978-3-945889-01-5
Ihde S., Ihde A. Libro de Recetas de la Masticación 4. International Foundation Publishing. 2015. ISBN 987-3-9851468-8-0
Ihde S., Ihde A. Trabajo de Laboratorio en Implantes Estratégicos 6. International Foundation Publishing. 2016. ISBN 978-3-945889-13-8
Ihde S., Ihde A., Lysenko V., Konstantino- vic V.S.K, Palka L. Nueva Terminologia Si- stematica de las Areas de Hueso Cortical para Implantes Oseofijados en Implantolo- gia. Jacobs Journal de Anatomia. Jacobs Publishers. 2016.

®
The Foundation of Knowledge
2017 28 CMF. Impl. Dir. Vol. 12 No. 1
Case 1
Fig. 14 A 68-year-old male patient with peridontal problems and with superior implants fenestrated (with vestibular exposure).
Fig. 15 Patient rehabilitated with Strategic Implant; 2 pterygoid, 2 in naso-maxillary buttress and other 3 in the floor of the nose.

Implant Directions®
29
Fig. 16 CT scan showing the anchoring of the BCS® implant in
the second cortical, in the floor of the nose.
Fig. 18 CT scan with panoramic image showing pterygoid on
the left side.
Fig. 17 CT scan showing the anchoring of the BCS® implant in
the second cortical, in the floor of the sinus and in the cortical
vestibular to it.
Fig. 19 CT-Slides showing in the anterior part the anchorage of
the implants BCS® in the second cortical.
Fig. 20 CT scan with panoramic image showing the pterygoid
plate on the right side.

®
The Foundation of Knowledge
2017 30 CMF. Impl. Dir. Vol. 12 No. 1
Case 2
Fig. 21 A 52-year-old male patient, with absence of teeth in the first quadrant and leaky crowns.
Fig. 22 Patient rehabilitated with 2 pterygoid implants and 2 zygomatic implants on the right side and the rest of the rehabilitation
with KOS® implants.

Implant Directions®
31
ou will be able to
plan for good
and receive the patientˇs
time-plan
Founda5ion Publishing
will be able to
technologytechnology
or good
receive the patientˇs
-plan
nda5ion Publishing
Educational Book Series
1 Introduction into the Work with Strategic Implant®
Avaiable in
English ISBN 978-3-945889-01-5
Russian ISBN 978-3-945889-04-6
Ukrainian ISBN 978-3-945889-01-5
Order Nr. 11-0024-05
2 Cookbook Mastication
Avaiable in
English ISBN 987-3-9851468-8-0
Bulgarian ISBN 978-3-945889-03-9
Spanish ISBN 987-3-945889-05-3
Hungarian ISBN 978-3-945889-02-2
Russian ISBN 987-3-9851468-8-0
Serbian ISBN 987-3-9851468-8-0
Order Nr. 4447
Please send your order via e-mail to
www.implantfoundation.org
or via regular postage mail to
International Implant Foundation
Leopoldstr. 116, DE-80802 München
Guide for Authors
ID publishes articles, which contain information, that will impro- ve the quality of life, the treatment outcome, and the afforda- bility of treatments. The following types of papers are published in the journal:
Full length articles (maximum length abstract 250 words, total 2000 words, references 25, no limit on tables and figures). Short communications including all case reports (maximum length abstract 150 words, total 600 words, references 10, figures or tables 3) Technical notes (no abstract, no introduc- tion or discussion, 500 words, references 5, figures or tables 3). Interesting cases/lessons learned (2 figures or tables, le- gend 100 words, maximum 2 references).
Literature Research and Review articles are usually commis- sioned. Critical appraisals on existing literature are welcome.
Direct submissions to: [email protected]. The text body (headline, abstract, keywords, article, conclusion), tables and figures should be submitted as separate documents. Each submission has to be accompanied by a cover letter. The cover letter must mention the names, addresses, e-mails of all authors and explain, why and how the content of the article will contribute to the improvement of the quality of life of patients.
4 Ihde & Ihde
Cookbook Mastication 2nd Edition
How to make patients chew successfully
(not only) on a Strategic Implant®
β γ
After reading and understanding this book you will be able to
• establish an equal, bilateral masticatory function in every patient
• safely determine the correct bite and rest position of the mandible
• incorporate safely prosthetic work-pieces on immediately loaded jaw implants
• correct the masticatory situation in case that a mobility of the bridges on
immediately loaded implants occurs
• maintain the implant`s stability and maintain a lateral pattern of mastication
over years
Ihde & Ihde 1
Introduction into the Work with the Strategic Implant
®
Definitions, General Explanations and Treatment Planning
2
After reading and understanding this book you
● understand how to work with the Strategic Implant®
● evaluate the case and set up a safe treatment n f
long-term results
● inform patients about the treatment possibilities d
informed consent
● calculate the costs of the treatment and set up a ime
In5erna5ional Implan55
In5erna5ional Implan5 Founda5ion Publishing