Embed Size (px)
Citation preview

ated with novelty seeking or impulsiveness in healthysubjects15,22–24 or in patients with Parkinson’s disease.4 Thepresent results support the idea that the novelty seeking traitrelates to specific insular dopaminergic function, not to thelevel of the dopaminergic activity per se. Further multi-tracer analyses for the same individuals are needed to de-termine the possible contribution of different insular dopa-mine receptor subtypes or different neurotransmittersystems on novelty seeking modulation.
Acknowledgments: The assistance of the staff of the TurkuPET Centre is gratefully acknowledged. This study was finan-cially supported by Turku University Hospital (clinical grants;EVO). This study utilized analysis methodology validated inthe Drug 2000 project, funded by the National Agency ofTechnology, Finland.
REFERENCES
1. Cloninger CR. A systematic method for clinical description andclassification of personality variants. Arch Gen Psychiatry 1987;44:573–588.
2. Suhara T, Yasuno F, Sudo Y, et al. Dopamine D2 receptors in theinsular cortex and the personality trait of novelty seeking. Neuro-image 2001;13:891–895.
3. Menza MA, Golbe LI, Cody RA, Forman NE. Dopamine-relatedpersonality traits in Parkinson’s disease. Neurology 1993;43:505–508.
4. Kaasinen V, Nurmi E, Bergman J, et al. Personality traits and braindopaminergic function in Parkinson’s disease. Proc Natl Acad SciU S A 2001;98:13272–13277.
5. Cloninger CR, Svrakic DM, Przybeck TR. A psychobiologicalmodel of temperament and character. Arch Gen Psychiatry 1993;50:975–990.
6. Kaasinen V, Någren K, Hietala J, et al. Extrastriatal dopamine D2
and D3 receptors in early and advanced Parkinson’s disease. Neu-rology 2000;54:1482–1487.
7. Gunn RN, Lammertsma AA, Hume SP, Cunningham VJ. Paramet-ric imaging of ligand-receptor binding using a simplified referenceregion model. Neuroimage 1997;6:279–287.
8. Sudo Y, Suhara T, Inoue M, et al. Reproducibility of [11C]FLB 457binding in extrastriatal regions. Nucl Med Commun 2001;22:1215–1221.
9. Friston KJ, Holmes AP, Worsley KJ, Poline J-B, Frith CD, Frack-owiak RS. Statistical parametric maps in functional imaging: ageneral linear approach. Hum Brain Map 1995;2:189–210.
10. Kaasinen V, Vilkman H, Hietala J, et al. Age-related dopamineD2/D3 loss in extrastriatal regions of the human brain. NeurobiolAging 2000;21:683–688.
11. Kaasinen V, Någren K, Hietala J, Farde L, Rinne JO. Sex differ-ences in extrastriatal dopamine D2-like receptors in the humanbrain. Am J Psychiatry 2001;158:308–311.
12. Brooks DJ, Ibanez V, Sawle GV, et al. Striatal D2 receptor statusin patients with Parkinson’s disease, striatonigral degeneration,and progressive supranuclear palsy, measured with 11C-racloprideand positron emission tomography. Ann Neurol 1992;31:184–192.
13. Brandstrom S, Richter J, Przybeck T. Distributions by age and sexof the dimensions of temperament and character inventory in across-cultural perspective among Sweden, Germany, and the USA.Psychol Rep 2001;89:747–758.
14. Gunn RN, Lammertsma AA, Grasby PM. Quantitative analysis of[carbonyl-11C]WAY-100635 PET studies. Nucl Med Biol 2000;27:477–482.
15. Kaasinen V, Nurmi E, Bergman J, Solin O, Kurki T, Rinne JO.Personality traits and striatal 6-[18F]fluoro-L-dopa uptake inhealthy elderly subjects. Neurosci Lett 2002;332:61–64.
16. Krolak-Salmon P, Henaff MA, Isnard J, et al. An attention mod-ulated response to disgust in human ventral anterior insula. AnnNeurol 2003;53:446–453.
17. Surguladze SA, Brammer MJ, Young AW, et al. A preferentialincrease in the extrastriate response to signals of danger. Neuro-image 2003;19:1317–1328.
18. Wicker B, Keysers C, Plailly J, Royet JP, Gallese V, Rizzolatti G.Both of us disgusted in My insula: the common neural basis ofseeing and feeling disgust. Neuron 2003;40:655–664.
19. Gordon CM, Dougherty DD, Rauch SL, et al. Neuroanatomy ofhuman appetitive function: a positron emission tomography inves-tigation. Int J Eat Disord 2000;27:163–171.
20. Calder AJ, Lawrence AD, Young AW. Neuropsychology of fearand loathing. Nat Rev Neurosci 2001;2:352–363.
21. Noble EP, Ozkaragoz TZ, Ritchie TL, Zhang X, Belin TR, SparkesRS. D2 and D4 dopamine receptor polymorphisms and personality.Am J Med Genet 1998;81:257–267.
22. Breier A, Kestler L, Adler C, et al. Dopamine D2 receptor densityand personal detachment in healthy subjects. Am J Psychiatry1998;155:1440–1442.
23. Farde L, Gustavsson JP, Jonsson E. D2 dopamine receptors andpersonality traits. Nature 1997;385:590.
24. Laakso A, Vilkman H, Kajander J, et al. Prediction of detachedpersonality in healthy subjects by low dopamine transporter bind-ing. Am J Psychiatry 2000;157:290–292.
Impairment of Individual FingerMovements in Patients With
Hand Dystonia
Antonio Curra, MD, PhD,1
Rocco Agostino, MD, PhD,2 Loredana Dinapoli, PhD,1
Sergio Bagnato, MD,2 Mario Manfredi, MD,1,2
and Alfredo Berardelli, MD1,2*1Dipartimento di Scienze Neurologiche, Universita degli
Studi di Roma “La Sapienza,” Rome, Italy;2Istituto Neurologico Mediterraneo Neuromed IRCCS,
Pozzilli, IS, Italy
Abstract: We investigated finger movements in patients withhand dystonia to compare the kinematics of repetitive in-dividual and non-individual finger oppositions. We used anoptoelectronic motion analysis system to record movementsin 3-D space, and recorded three 5-second trials for eachtask, counting how many finger oppositions subjects car-ried out during each trial, and measured the duration andamplitude of flexions, extensions, and pauses. During tasks,
*Correspondence to: Prof. Alfredo Berardelli, Dipartimento di Sci-enze Neurologiche, Universita degli Studi di Roma “La Sapienza,”Viale dell’Universita 30, 00185 Rome, Italy.E-mail: [email protected]
Received 25 October 2003; Revised 10 March 2004; Accepted 22March 2004
Published online 10 June 2004 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/mds.20190
INDIVIDUAL FINGER MOVEMENTS IN DYSTONIA 1351
Movement Disorders, Vol. 19, No. 11, 2004

normal subjects and patients carried out finger flexionsfaster than extensions, and invariably they paused longerbefore extension than before flexion. Patients were slowerand paused longer than controls during both individual andnon-individual oppositions. During individual finger move-ments, patients were disproportionately slow during exten-sion and pause before extension. Patients with hand dysto-nia perform finger movements abnormally; they areaffected predominantly during individual oppositions. Thisfinding reflects the finer cortical control needed to promoteand sustain this highly fractionated type of motor output,and points toward underactivity of the primary motor cor-tex in dystonia. © 2004 Movement Disorder Society
Key words: individual finger movements; dystonia; kine-matic analysis
Neurophysiological investigation of patients with dys-tonia shows abnormal execution of voluntary move-ments.1 Patients with segmental or generalized dystoniaaffecting the upper limb perform simple or complexmovements involving the elbow or more proximal jointswith reduced speed (bradykinesia), prolonged concomi-tant activation of agonist and antagonist muscles (co-contraction), and the presence of unusually evident elec-tromyographic (EMG) activity in remote muscles notinvolved in the motor task (overflow).2–5
Besides these well-known neurophysiological abnor-malities, clinical observation suggests that patients withdystonia, even those with focal, task-specific dystonia,may have more subtle disorders of motor control. Afeature that patients with task-specific dystonia sharewith those affected by segmental or generalized dystonia,is that their disorder of motor control affects skilledfinger movements that have to be carried out rapidly,selectively, and independently.6,7 Physiological investi-gation in patients with hand cramps showed that duringisolated finger movements, EMG activity spreads tomuscle groups of nonmoving fingers, an abnormalityinterpreted as a lack of selectivity during individualfinger movements.8
Cortical control of finger movements is a field ofactive investigation. Schieber9 proposed a physiologicalmodel on how the motor cortex individuates fingermovements, whereby more cortical neurons in the pri-mary motor cortex are needed for generating more inde-pendent finger movements. The model also predicts thatthe set of cortical neurons controlling isolated movementof a single finger includes a subset of neurons involved ina more rudimentary, related movement (hand openingand closing).
Evidence from studies investigating movement-relatedcortical potentials,10–12 cerebral blood flow activationpatterns,13–15 and the silent period induced by transcra-
nial magnetic stimulation (TMS)16 points toward an un-deractivation of the primary motor cortex during move-ment in dystonia. Following Schieber’s model,9 theseobservations lend support to the hypothesis that patientswith dystonia may have a predominant impairment ofindividual finger movements.
To study the pathological kinematic pattern of fingermovements in dystonic patients and to see whether dys-tonia impairs individual more than non-individual fingermovements, we analyzed repetitive index-thumb oppo-sitions during individual and non-individual fingermovements.
SUBJECTS AND METHODS
Nine normal subjects (8 men, 1 woman; mean age �standard deviation [SD], 51.7 � 13.7 years) and 9 pa-tients with dystonia (8 men, 1 woman; 52.4 � 14.9years) participated in the study. They gave written in-formed consent and the local ethical committee approvedthe experimental protocol. All participants were right-handed. Six patients had hand dystonia as an isolatedmanifestation; one had hand and arm dystonia, one hadhand and jaw dystonia, and one had hand, arm, and neckdystonia. Patients were assessed clinically with the Dys-tonia Movement Scale of the Fahn-Marsden EvaluationScale for Dystonia (FMESD)17 (Table 1). All subjectswere clinically free of abnormalities restricting fingermovements.
We used the ELITE motion analysis system (BTS,Milan, Italy) to record movements in 3-D space. Thesystem consists of two infrared ray cameras (100-Hzsampling rate) that detect the motion of passive reflectingmarkers, and a TV image processor that digitalizes andreconstructs the coordinates of marker motion. Mathe-matical arrangement of spatial coordinates provided thevelocities on 3-D planes, and displayed them in graphicalform.
The experimental pattern has been detailed else-where.18 In brief, subjects sat comfortably in front of thetwo cameras with a passive marker placed firmly on thedistal phalanx of the index finger (D2). Two tasks werestudied: moving chiefly around the metacarpal-phalan-geal joints, the subjects tapped the D2 (individual oppo-sitions) or all the four fingers (DDD: D2, D3, D4, D5)against the thumb (non-individual oppositions). For bothtasks, the arm was flexed at the elbow (�90 degrees) andabducted at the shoulder (�20 degrees), with the forearmmidway between pronation and supination, and the wristat the neutral position. For individual oppositions, D2was extended, whereas D3, D4 and D5 were flexed.During the non-individual oppositions, D2, D3, D4, andD5 were adducted and extended, and moved together.
1352 A. CURRA ET AL.
Movement Disorders, Vol. 19, No. 11, 2004

During individual and non-individual oppositions, sub-jects had to keep the thumb (D1) at its maximal abduc-tion. Patients were instructed to move as fast and aswidely as possible in a repetitive fashion and to keep thethumb as stable as possible.
In a subset of patients with hand dystonia as an iso-lated manifestation (n � 5) and controls (n � 5), we alsostudied a further individual opposition task, when sub-jects held D1, D3, D4, and D5 flexed and placed D2 inthe middle of an aluminum cast. They were then requiredto flex and extend D2 repetitively as fast as possibletapping against the walls of the cast. Contrary to previousexperiment, in this setting both flexion and extensionphases ended against an endstop.
Before recordings, subjects did three 5-second practicetrials with their dominant hand and then three 5-secondtrials were recorded. Between trials, a short rest wasallowed (20–30 seconds). Subjects started the motor taskat will and the recording started as soon as they moved..This procedure excluded the very first movement of thetrial from recording and subsequent analysis. The twotasks were presented in pseudorandom order, so that ineach group a similar proportion of subjects started withindividual oppositions and the remainder started withnon-individual oppositions.
The ELITE software plotted finger displacement andvelocity profiles for each opposition on a computerscreen. We first counted how many finger oppositionssubjects carried out during each 5-second trial. Eachopposition comprised two movement phases, flexion andextension, and for each phase we measured amplitudeand duration. By moving a cursor, we marked the begin-ning and end of each phase, using an arbitrary fingervelocity value of 50 mm/sec as a threshold for fingermotion.19 We also calculated the duration of the pausesbefore flexion and extension.
We assessed the deterioration of motor performanceby investigating the reduction in speed and amplitude as
the task progressed. In both groups, we compared datafrom the early (first three) and late (last three) opposi-tions recorded in each trial for each task.
All data are expressed as mean � 1 SD. Differences inthe kinematic variables between groups and tasks wereanalyzed using separate multi-way analysis of variance(ANOVA), with group (normal vs. patient), and task(individual vs. non-individual oppositions) as betweenfactors, and phase (flexion vs. extension), and recordingtrials (1, 2, and 3) as factors for repeated measures. Toanalyze motor deterioration with task completion, datawere subjected to separate ANOVA with the betweenfactors, group and task, and repeated measures factors,phase and position (early vs. late oppositions). In thedouble-endstop experiment, between-groups differencesin the kinematic variables were analyzed using ANOVAwith factors group, phase, and recording trials. For eachcomparison Tukey’s Honest Significant Difference(HSD) test was used for post hoc analysis. P values lessthan 0.01 were considered to indicate statistical signifi-cance.
RESULTS
All subjects carried out the motor tasks correctly.Motor execution induced no dystonic symptom in pa-tients with isolated hand dystonia (Patients 1 to 6), nordid it worsen initial abnormal posture in Patients 7 and 8.Arm dystonia slightly worsened during both tasks inPatient 9.
Preliminary analysis of kinematic data across record-ing trials disclosed no main effect for factor trial, whichindicates that within both groups and tasks the number offinger oppositions, and the duration, amplitude, andpauses remained unchanged across the recording trials.We therefore pooled data from the three trials in subse-quent analyses.
TABLE 1. Clinical features of patients
Patient no. Age (yr)Illness
duration (yr)Affected by
dystoniaArm severity
(0–16)
Disability (0–4)
TreatmentaHandwriting Feeding
1 33 2 Hand 2 1 0 None2 77 9 Hand 2 2 0 BTX3 36 2 Hand 1 1 0 None4 54 6 Hand 2 2 0 BTX5 61 6 Hand 2 1 0 BTX6 60 7 Hand 2 3 0 BTX7 72 9 Hand, arm 6 3 2 BTX8 41 12 Hand, jaw 6 3 1 BTX9 39 15 Hand, arm,
neck8 2 2 BTX,
benzodiazepines
aPatients periodically treated with botulinum toxin (BTX) were tested at least 4 months after the last injection.
INDIVIDUAL FINGER MOVEMENTS IN DYSTONIA 1353
Movement Disorders, Vol. 19, No. 11, 2004

Oppositions Carried Out DuringEach Recording Trial
During both individual and non-individual finger tasks,patients carried out fewer oppositions than did normal sub-jects (mean trial oppositions, patients: individual 12.5 �5.1, non-individual 13.5 � 5; controls: individual 20.1 �3.4, non-individual 19.0 � 3.8; F[1,104] for factor group �59.01, P � 0.00001). Within-group analysis showed thatthe number of oppositions carried out during individual andnon-individual tasks were similar.
Amplitude and Duration of Flexion andExtension Phases
During individual and non-individual finger oppo-sitions, patients and controls carried out flexion andextension phases of similar amplitude (F[1,104] forfactor group � 1.87, P � 0.79) (Table 2). Patients didboth tasks more slowly than normal subjects did(F[1,104] for factor group � 32.6, P � 0.00001), and inboth groups, extension lasted longer than flexion did(F[1,104] for factor phase � 89.1, P � 0.00001). Ex-tension lasted disproportionately longer during theindividual than during non-individual oppositions(task by phase interaction F[1,104] � 9.5, P � 0.003),and this phenomenon was determined mainly by thepatient’s group (group by task by phase interactionF[1,104] � 6.1, P � 0.01) (Table 2). The predominantslowness of extension during individual oppositionswas similar in 2 patients with hand and arm dystonia(mean duration of flexion, 120 msec; mean duration ofextension, 182 msec; Patients 7 and 9 in Table 1) andin the other patients (flexion, 141 � 71 msec; exten-sion, 222 � 91 msec).
Duration of Pauses
Patients paused longer than normal subjects did(F[1,104] for factor group � 35.5, P � 0.00001), and bothgroups paused longer before extension than before flex-ion (F[1,104] for factor pause � 55.7, P � 0.00001).Pause before extension lasted disproportionately longer
than pause before flexion during individual comparedwith non-individual finger oppositions (task by phaseinteraction, F[1,104] � 8.3, P � 0.005), and this phenom-enon was determined mainly by the patient’s group(group by task by phase interaction, F[1,104] � 10.22,P � 0.002) (Table 2).
Deterioration of Motor Performance WithTask Completion
Comparison between duration of early and late oppo-sitions for all recording trials showed that patients car-ried out both tasks more slowly than did normal subjects(F[1,32] for factor group � 12.9, P � 0.001), and thatextension lasted longer than flexion (F[1,32] for factorphase � 24.4, P � 0.00001). Neither group showedmotor deterioration with task completion.
Comparison between the amplitude of early and lateoppositions for all recording trials showed that bothgroups carried out flexion and extension, as well as lateand early oppositions, with similar movement amplitude.Neither group showed changes in movement amplitudewith task completion.
Oppositions Carried Out, Duration, and PausesDuring the Double-Endstop Experiment
During double-endstop individual oppositions, pa-tients carried out fewer oppositions than normal subjectsdid (mean trial oppositions: patients, 11.7 � 5.0; con-trols, 16.71 � 3.7; F[1,28] for factor group � 8.9, P �0.005). They also moved more slowly than normal sub-jects did (F[1,28] for factor group � 13.3, P � 0.001). Inboth groups, flexions and extensions had a similar dura-tion (F[1,28] for factor phase � 0.52, P � 0.82) (Fig. 1).Patients and controls paused for a shorter time beforeextension than before flexion (F[1,28] for factor phase �19.5, P � 0.0002), without between-group differences.
DISCUSSION
Our kinematic findings show that during the flexionand extension phases of individual and non-individual
TABLE 2. Kinematic data during individual and non-individual finger oppositions
Parameter
Phase amplitude (mm) Phase duration (msec) Pause (msec)
Flexion Extension Flexion Extension Before flexion Before extension
Non-individualControls 62.0 � 10.9 62.9 � 11.5 93.0 � 21.1 129.1 � 31.5 6.9 � 5.9 29.2 � 20.9Patients 62.3 � 14.0 64.0 � 13.5 140.2 � 62.7 164.5 � 40.8 66.2 � 66.4 72.5 � 75.8
IndividualControls 61.8 � 13.6 62.6 � 13.7 99.1 � 26.7 140.9 � 27.7 8.8 � 10.0 29.2 � 22.6Patients 63.6 � 16.9 62.2 � 16.9 136.1 � 65.0 213.3 � 85.0 50.3 � 53.6 94.7 � 68.7
Values are expressed as mean � 1 SD.
1354 A. CURRA ET AL.
Movement Disorders, Vol. 19, No. 11, 2004

finger–thumb oppositions, dystonic patients were slowerand paused longer than did normal subjects. Patientsshowed a disproportionately prolonged extension phaseand pause before extension during individual comparedwith that during non-individual finger movements, butthey showed no hypometria, nor did their motor perfor-mance deteriorate with task completion. Bradykinesiatherefore predominantly affected individual finger oppo-sitions, indicating that dystonia impairs individual morethan non-individual finger movements.
Schieber’s model9 of how the motor cortex individ-uates movements predicts that individual finger move-ments imply larger and more intense motor cortexactivation than that with non-individual movements.This prediction receives support from experimentaldata in monkey20 and man,21 and by recent physiolog-ical research showing that patients with lesions rela-tively restricted to the motor cortex or the corticospi-nal tract lose independent finger movements.22 Thepredominant bradykinesia we found during individualfinger movements in patients therefore fits in well withunderactivation of cortical motor areas reported con-sistently during movement in patients with dystoniausing movement-related cortical potentials,10 –12,23
TMS,16,24,25 and positron emission tomography.13–15,26
Moreover, our finding does not contrast with recentevidence of overactive primary motor cortex inducedby task-specific dystonic contractions,27,28 becauseonly 1 of 9 patients had slightly worsened arm dysto-nia during finger oppositions. On the basis ofSchieber’s model,9 we conclude that because an ab-normally low level of motor cortex activation ispresent in dystonia during movement, and a higher
level of activity is required to carry out individual thannon-individual finger movements in healthy subjects,dystonic patients find it more difficult to cope withindividual than with nonindividual finger oppositions.
The kinematic abnormality causing the patients’predominant impairment of individual finger move-ments was the disproportionately long extensionphase. This finding is consistent with neurophysiolog-ical evidence showing that activation of the extensormuscles requires greater brain activity than that re-quired by activation of the flexor muscles,29,30 andstudies of isometric contraction in patients with Par-kinson’s disease showing greater deficits in the per-formance of extensor than flexor muscles.31 We there-fore attribute the predominant impairment seen in ourpatients, during finger extension in the context ofindividual finger oppositions, to the intense motorcortex activation that extension and individual fingeropposition per se require.
The mechanism that translates the reduced brainactivation into the predominant impairment of individ-ual finger extension in hand dystonia is unclear. Ow-ing to their motor cortex underactivity, dystonic pa-tients have reduced mechanisms of corticalinhibition,1 a phenomenon that may lead to loss offocusing during voluntary muscle activation, and pro-duces co-contraction. We hypothesize that co-contraction, the prototypical abnormal overlap of pro-longed agonist and antagonist bursts present indystonic patients,8 might have affected extension morethan flexion, and exacerbated bradykinesia during in-dividual finger movements. This is also supported bythe results from the double-endstop experiment. Using
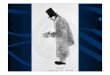
FIG. 1. Patients carried out bothphases more slowly than normalsubjects did, but in both groups,extension and flexion had similarduration. Patients paused longerthan normal subjects did, and bothgroups paused longer before flex-ion than before extension. Squaresand circles represent mean values;bars represent 0.5 SD.
INDIVIDUAL FINGER MOVEMENTS IN DYSTONIA 1355
Movement Disorders, Vol. 19, No. 11, 2004

the aluminium cast to stop finger flexion and extensionduring individual finger opposition, we found that bothphases had a similar duration. Without the cast, in bothhealthy subjects and patients, the extension phase waslonger than the flexion phase during both individualand non-individual oppositions. This kinematic pat-tern probably depends on how the endstop modulatesthe EMG activity during rapid movements. EMG stud-ies have shown that rapid movements that do not endagainst an endstop are slower than those that aremechanically stopped, because in the latter conditionthe antagonist muscle activity of the triphasic patternmarkedly diminishes whereas the agonist muscle ac-tivity increases.32–34 Furthermore, during fast repeti-tive movements, such as the finger oppositions studiedhere, triphasic EMG analysis typically shows an alter-nating biphasic activation of agonist and antagonistmuscles due to the lack of the second agonistburst.35,36 Interestingly, the same burst that acts asantagonist to brake the ongoing submovement concur-rently acts as agonist to produce the impulsive forcefor the forthcoming submovement in the opposite di-rection. When flexion alone is mechanically stopped,the antagonist muscles are therefore conceivably lessactivated than they are during extension. This makesflexion less prone to co-contraction than extension is,and lengthens the extension phase.
We also found that in patients with dystonia besidesprolonging extension, the individual opposition taskdisproportionately lengthened the pause before exten-sion; both are physiologically linked because bothdepend largely on activation of extensor muscles. In-deed, during flexion the extensor muscles act as an-tagonists to brake the movement, they are less acti-vated owing to the presence of the endstop, andtherefore require a longer-lasting pause to build up theagonist EMG activity needed to initiate extension.18
Again, this interpretation is supported by our findingsin the double-endstop experiment. Under this condi-tion, patients not only reduced the duration of exten-sion, but also shortened the pause before extension(from �90 to �40 msec).
That pause duration is related largely to the expectedEMG pattern during repetitive finger opposition is con-firmed by the observation that during the double-endstopexperiment in both groups, the pause before flexion alsolengthened. Accordingly, the endstop after extension de-layed the flexor muscle activation needed to produce theimpulsive force for the forthcoming flexion.18
We showed that similar to parkinsonian patients,18
patients with dystonia are more bradykinetic duringindividual than during non-individual finger opposi-
tions. Unlike patients with Parkinson’s disease, how-ever, patients with dystonia showed no hypometria,nor did their motor performance deteriorate with taskcompletion. In parkinsonian patients, the predominantimpairment of individual finger movements becamemanifest only with motor deterioration, whereas indystonic patients it was present from the beginning oftask performance. During individual finger move-ments, parkinsonian patients were predominantly slowduring flexion, i.e., the phase in which the highestspeed was reached, whereas dystonic patients werepredominantly slow during extension, i.e., the phasemost prone to co-contraction. Although bradykinesiais a common abnormality of motor control in patientswith movement disorders originating from basal gan-glia dysfunction, the physiological mechanisms under-lying bradykinesia in distinct diseases thus differ.
In conclusion, patients with hand dystonia showgreater impairment of individual compared with non-individual finger movements. Owing to the high motorcortex activation required for extending the fingers dur-ing individual oppositions, we attribute this kinematicabnormality to underactivation of the primary motorcortex during movement in dystonia.
REFERENCES
1. Berardelli A, Rothwell JC, Hallett M, Thompson PD, Manfredi M,Marsden CD. The pathophysiology of primary dystonia. Brain1998;121:1195–1212.
2. van der Kamp W, Berardelli A, Rothwell JC, Thompson PD, DayBL, Marsden CD. Rapid elbow movements in patients with torsiondystonia. J Neurol Neurosurg Psychiatry 1989;52:1043–1049.
3. Agostino R, Berardelli A, Formica A, Accornero N, Manfredi M.Sequential arm movements in patients with Parkinson’s disease,Huntington’s disease and dystonia. Brain 1992;115:1481–1495.
4. Inzelberg R, Flash T, Schechtman E, Korczyn RD. Kinematicproperties of upper limb trajectories in idiopathic torsion dystonia.J Neurol Neurosurg Psychiatry 1995;58:312–319.
5. Curra A, Berardelli A, Agostino R, Giovannelli M, Koch G,Manfredi M. Movement cueing and motor execution in patientswith dystonia: a kinematic study. Mov Disord 2000;15:103–112.
6. Poore GV. Clinical lecture on certain conditions of the hand andarm which interfere with the performance of professional acts,especially piano–playing. Br Med J 1887;1:441–444.
7. Tolosa ES, Marti MJ. Adult-onset idiopathic torsion dystonias. In:Watts RL, Koller WC, editors. Movement disorders. New York:McGraw-Hill; 1997. p 429–441.
8. Cohen G, Hallett M. Hand cramp: clinical features and electro-myographic patterns in a focal dystonia. Neurology 1988;38:1005–1012.
9. Schieber MH. How might the motor cortex individuate move-ments? Trends Neurosci 1990;13:440–445.
10. Feve A, Bathien N, Rondot P. Abnormal movement related poten-tials in patients with lesions of basal ganglia and anterior thalamus.J Neurol Neurosurg Psychiatry 1994;57:100–104.
11. Deuschl G, Toro C, Matsumoto J, Hallett M. Movement relatedcortical potentials in writer’s cramp. Ann Neurol 1995;38:837–838.
12. van der Kamp W, Rothwell JC, Thompson PD, Day BL, MarsdenCD. The movement-related cortical potential is abnormal in patientswith idiopathic torsion dystonia. Mov Disord 1995;10:630–633.
1356 A. CURRA ET AL.
Movement Disorders, Vol. 19, No. 11, 2004

13. Ceballos-Baumann AO, Passingham RE, Warner T, Playford ED,Marsden CD, Brooks DJ. Overactive prefrontal and underactivemotor cortical areas in idiopathic dystonia. Ann Neurol 1995;37:363–372.
14. Playford ED, Passingham RE, Marsden CD, Brooks DJ. Increasedactivation of frontal areas during arm movement in idiopathictorsion dystonia. Mov Disord 1998;13:309–311.
15. Ibanez V, Sadato N, Karp B, Deiber MP, Hallett M. Deficientactivation of the motor cortical network in patients with writer’scramp. Neurology 1999;53:96–105.
16. Curra A, Romaniello A, Berardelli A, Cruccu G, Manfredi M.Shortened cortical silent period in facial muscles of patients withcranial dystonia. Neurology 2000;54:130–135.
17. Weiner WJ, Lang AE. Movement disorders. A comprehensivesurvey. Mount Kisco, NY: Futura Publishing Company; 1989. p688–700.
18. Agostino R, Curra A, Giovannelli M, Modugno N, Manfredi M,Berardelli A. Impairment of individual finger movements in Par-kinson’s disease. Mov Disord 2003;18:560–565.
19. Curra A, Berardelli A, Agostino R, Modugno M, Conti Puorger C,Accornero N, Manfredi M. Performance of sequential arm move-ments with and without advance knowledge of motor pathway inParkinson’s disease. Mov Disord 1997; 12:646–654.
20. Muir RB, Lemon RN. Corticospinal neurones with a special role inprecision grip. Brain Res 1983;261:312–316.
21. Datta AK, Harrison LM, Stephens JA. Task-dependent changes inthe size of response to magnetic brain stimulation in human firstdorsal interosseous muscle. J Physiol 1989;418:13–23.
22. Lang CE, Schieber MH. Differential impairment of individuatedfinger movements in humans after damage to the motor cortex orthe corticospinal tract. J Neurophysiol 2003;90:1160–1170.
23. Ikeda A, Luders HO, Burgess RC, Shibasaki H. Movement-relatedpotentials recorded from supplementary motor area and primarymotor area. Role of supplementary motor area in voluntary move-ments. Brain 1992;115:1017–1043.
24. Niehaus L, von Alt-Stutterheim K, Roricht S, Meyer BU. Abnor-mal postexcitatory and interhemispheric motor cortex inhibition inwriter’s cramp. J Neurol 2001;248:51–56.
25. Gilio F, Curra A, Inghilleri M, Lorenzano C, Suppa A, Manfredi M,Berardelli A. Abnormalities of motor cortex excitability precedingmovement in patients with dystonia. Brain 2003;126:1745–1754.
26. Ceballos-Baumann AO, Sheean G, Passingham RE, Marsden CD,Brooks DJ. Botulinum toxin does not reverse the cortical dysfunc-tion associated with writer’s cramp. A PET study. Brain 1997;120:571–582.
27. Pujol J, Roset-Llobet J, Rosines-Cubells D, Deus J, Narberhaus B,Valls-Sole J, Capdevila A, Pascual-Leone A. Brain cortical acti-vation during guitar-induced hand dystonia studied by functionalMRI. Neuroimage 2000;12:257–267.
28. Odergren T, Stone-Elander S, Ingvar M. Cerebral and cerebellaractivation in correlation to the action-induced dystonia in writer’scramp. Mov Disord 1998;13:497–508.
29. Yue GH, Liu JZ, Siemionow V, Ranganathan VK, Ng TC, SahgalV. Brain activation during human finger extension and flexionmovements. Brain Res 2000;856:291–300.
30. Palmer E, Ashby P. Corticospinal projections to upper limb mo-toneurones in humans. J Physiol 1992;448:397–412
31. Corcos DM, Chen CM, Quinn NP, McAuley J, Rothwell JC.Strength in Parkinson’s disease: relationship to rate of force gen-eration and clinical status. Ann Neurol 1996;39:79–88.
32. Waters P, Strick PL. Influence of “strategy” on muscle activityduring ballistic movements. Brain Res 1981;207:189–194.
33. Marsden CD, Obeso JA, Rothwell JC. The function of the antag-onist muscle during fast limb movements in man. J Physiol 1983;335:1–13.
34. Pantaleo T, Benvenuti F, Bandinelli S, Mencarelli MA, Baroni A.Effects of expected perturbations on the velocity control of fastarm abduction movements. Exp Neurol 1988;101:313–326.
35. Benecke R, Rothwell JC, Day BL, Dick JPR, Marsden CD. Motorstrategies involved in the performance of sequential movements.Exp Brain Res 1986;63:585–595.
36. Freund HJ. Time control of hand movements. Prog Brain Res1986;64:287–294.
Presence of SpinocerebellarAtaxia Type 2 Gene Mutation in aPatient With Apparently Sporadic
Parkinson’s Disease:Clinical Implications
Din-E Shan, MD, PhD,1,2 Ren-Shyan Liu, MD,3
Chen-Ming Sun, MD,3 Shwn-Jen Lee, PhD, PT,4
Kwong-Kum Liao, MD,1,2
and Bing-Wen Soong, MD, PhD1,2*1The Neurological Institute, Taipei Veterans General
Hospital, Taipei, Taiwan, Republic of China; 2Department ofNeurology, National Yang-Ming University, Taipei, Taiwan,Republic of China; 3National PET/Cyclotron Center, Taipei
Veterans General Hospital, Taipei, Taiwan, Republic ofChina; 4Department of Physical Therapy, National Yang-
Ming University, Taipei, Taiwan, Republic of China
Abstract: Among 242 patients with apparently sporadicParkinson’s disease, a 70-year-old man with a CAG repeatnumber of 37 in the SCA2 gene was identified. He hasremained responsive to levodopa 14 years after onset andhas had no overt signs suggesting cerebellar dysfunction.Although it is not possible to confirm if this patient has a denovo mutation of the SCA2 gene, this genetic defect seems tobe contributing to his parkinsonian features and furthersupports the concept that apparently sporadic, late-onset,levodopa-responsive Parkinson’s disease may have multiplecauses. © 2004 Movement Disorder Society
Key words: Parkinson’s disease; PET; SCA2
Mutations in several genes have been identified inpatients with familial parkinsonism.1 Mutation in the
This article contains Supplementary Video Clips, available online athttp://www.interscience.wiley.com/jpages/0885-3185/suppmat.
*Correspondence to: Dr. Bing-Wen Soong, The Neurological Insti-tute, Taipei Veterans General Hospital, Taipei, Taiwan, 112, Republicof China. E-mail: [email protected]
Received 20 January 2004; Revised 8 March 2004; Accepted 27March 2004
Published online 11 June 2004 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/mds.20212
SCA2 AND SPORADIC PARKINSON’S DISEASE 1357
Movement Disorders, Vol. 19, No. 11, 2004















![J. Irwin J. Schwartzmanl Study Design: Case Report Wall Dystonia and CRPS.pdfforms of dystonia can occur that involve all limbs [7,8]; however dystonia of axial muscles (intercostal,](https://img.pdfslide.us/doc/110x75/60277a5699a9ad280a71f846/j-irwin-j-schwartzmanl-study-design-case-report-wall-dystonia-and-crpspdf-forms.jpg)











