Embed Size (px)
Citation preview

Impaired Mind vs. Impaired Body Who needs more help and time to complete routine ADLs: A physically disabled elder or one who is physically fit and cognitively disabled?
BY E L I Z A B E T H J E A N S H O O K / C O R N E L I A M B E C K
C ommon sense tells us that cog- nitively impaired patients need special care. But do they need
more or less care than physically im- paired patients?
Difficulty performing such daily ac- tivities as eating, dressing, or bathing are common in both physically and cognitively impaired patients. But the assistance each needs is as different as the cause of the impairments. A per- son who is physically impaired, for ex- amPle, may be unab le to ba the because he is too weak, unable to walk, or unable to hold a washcloth. A person who is cognitively impaired may not rememberto bathe, may be unable locate the bathroom or the washcloth or remember what to do he finds the bathing items. Someone must remind and convince him to bathe, to hold his attention on the task at hand, and keep him calm and pre- vent him from wandering off.
Other variables also add to the time required to care for cognitively impaired patients. They require close supervision, as poor judgment can trigger them to attempt activities that they no longer can perform safely. They are more l~ely than physically impaired patients to be disruptive, re- quiring special management(l). Their moods and abilities to care for them- selves can fluctuate widely, making it difficult for nurses to establish rou- tines.
We conducted a pilot study to see how cognitively impaired patients compared with physically impaired patients in terms of the types of prob- lems they encountered in performing activities of daily living (ADLs), the staff assistance required, and the staff- assistance time required. We chose to examine four ADLs: bathing, groom- ing, eating, and toUeting.
Geriatric Nursing July/August 1991 185

I~Sp~E.N T ~ ~ - ~"
11n 'n es "
TOTAL 55mintaes*
For grooming, eating and to~eting tognitively impaired residents took nearly twice as much staff time as did the physically impaired.
We studied 20 nursing home resi- dents---10 from a 22-bed unit designed for cognitively impaired residents and 10 from a 100-bed unit for physically impaired residents. All 20 residents had lived in the nursing home for more than a year, all but one were 65 years old or older, and all had some disability in per- forming ADLs.
The cognitively impaired residents were primarily male (60%), and most ranged in age from 70 to 80 (80%). The physically impaired residents were women between 70 and 80 years old.
The cognitively impaired residents had no physical impairments. By Medi- caid standards, therefore, they required
ELIZABETH JEAN SHOOK, RN, MNSc, is a nursing instructor and C O R N E L I A M. BECK, MSE, PhD, is associate dean for re- search and evaluation, University of Arkansas for Medical Sciences, Little Rock, AR.
minimal care, although all had prob- lems with at least two ADLs. Seven res- idents were classified as moderately hnpaired and three as mildly hnpaired, using the Mini-Mental State Exam(2).
The second group of 10 residents all had some type of disabling physical impairment, which the nursing staff identified as the primary reason for their inability to perform ADLs. By Medicaid standards, they all required skilled care. Three of the residents were classified as having mild cogni- tive hnpairment, and seven as having no cognitive impairment, using the Mi- ni-Mental State Exam.
We selected components of the Performance Assessment of Self-Care Skills (PASS) to measure the nature of the resident's problems performing ADLs and the type and frequency of help the residents needed to improve their performance(3).
The PASS allowed us to categorize the residents' problems performing ADLs as difficulty with balance, range of motion, and vision; poor coordina- tion; lack of strength, endurance, ini- tiative, or attention; memory deficit, impaired problem solving; and lack of motivation or will to do the activity.
We categorized how staff assisted residents with ADLs as providing emotional support and encourage- ment, focusing attention, guiding ver- bal ly or manually, modi fy ing an existing part of the environment (e.g., moving chairs), adding an adaptive device to the environment (e.g., a spe- cial spoon), and doing all or part of the activity of the resident.
We used a stop watch to measure the length of time the residents need- ed to comple te a task. We began counting when the staff told the resi- dent to begin the task, and we stopped timing when the resident completed it.
We recorded the time to the nearest whole minute.
All observations were made by staff during a two-week period. We defined bathing as the customary method by which the resident bathed, that is, bed bath, shower, or tub bath. For groom- ing activities in the morning, staff ob- served residents combing their hair, putting on powder or deodorant, and the men shaving or the women putting on makeup. Toileting was defined as the resident going to the bathroom to urinate. For eating, staff observed the residents during lunch.
Compared with physically im- paired residents, those who were cognitively impaired demonstrated significantly more visual-spatial, memory problem-solving difficulties in bathing (see "How Many Patients Need Help With ADLs?" at right) Cognitively impaired residents also had more at tent ion problems in eating, and more visual and memory problems in toileting.
Physically impaired residents had in general more problems with balance during eating; range of motion (ROM) during grooming, eating, and toileting; strength during bathing, grooming, and eating; and endurance during toileting.
Those who were cognit ively impaired needed significantly more emotional guidance from staff during toileting; focused attention during grooming, bathing and toileting; and environmental modification during eating. In terms of the total amount of time for complet ing the four ADLs, the cognit ively impaired residents needed 72 percent more time than the physically impaired residents (see "Average Time Staff Spent," at left). At $3.60 per hour for nurses aides, the weekly cost of
186 Geriatric Nursing July/August 1991

assistance for these four ADLs for 100 cognitively impaired residents would be $569, compared with $329 for 100 physically impaired residents, a difference of $240.
We can par t ia l ly explain the greater amount of time staff gave the cognitively impaired residents for grooming and eating by the extensive reassurance, encouragement, model- ing, and physical assistance they need- ed to successfully complete these activities. Assistance takes more time than doing the task for the subject.
Likewise, staff gave a significantly greater amount of time to the cogni- tively impaired residents to complete toileting because staff had to remind them to toilet, show them where the bathroom was, and guide them in re- moving clothing and using the toilet. In contrast, staff did not have to watch physically impaired residents for signs that they might urinate, nor did staff have to remind them where the bath- room was, how to remove their cloth- ing, or what to do once positioned.
This study confirms that the care of cognitively impaired residents is time consuming. Yet, current case-mix sys- tems tend to reimburse at higher lev- els for physical support or assistance than for supervision and direction. They do not factor in the extra re- sources those who are cognitively im- paired need and underestimate the true costs of caring for them.
REFERENCES
1. Rovner, B., and others Prevalence of mental illness in community nursing home. American JounwlofPsy- chiatry 143:1446-1449,1986.
2. Folstein, M. E, and others. "Mini-mental state." A practical method for grading the cognitive state of residents for the clinician. J.Psychiatr.Res. 12:189-198, Nov. 1975.
3. Rogers, J. C. Performance assessment of Self-Care Skills. (Unpublished paper) Pittsburgh: University of Pittsburgh, Western Psychiatric Institute and Clinic, 19S6.
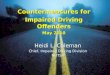
HOW MANY PATIENTS NEED HELP WITH ADLs?
What kinds of problems... Activities
Bathing Grooming Eating Toileting
Imbalance 9 9 g 7 8 0 9 6
RaM 8 4 9 3 |O 0 ~ 3 . ~ , . . . . . . J y J J
Strength 7 3 7 3 6 1 6 3
Coordination I0 9 ¢~ 8 9: 7 10 6
Endurance 9 5 8: 4 ~ 6 9 3 , , , , m ,
Visual-Spatial 2 9 5, 9 :5 10 t 8
Initiation 6 10 $ 7 3' 8 4 7
Attention 7 10 7 9 3 9 ? 6
Memory 2 10 10 10 !0 lO 2 9 i i
Problem Solving 4 10 5 10 5 10 8 9
Motivation 6 10 7 10 5 9 $ 7
In each ADL, motivation was a problem for 7 or more of the 10 cognitively impaired residents. Only in grooming did up to 7 physically impaired residents have problems.
Emotional
Focusing
Verbal Guide
Visual Guide
Modification
Adaptation
Manual Guide
Physical Help
What kind of help... Activities
Bathing Grooming Eating Toi[eting
5 I0 7 10 5 10 4' 10 , , , , , i ,,
3 10 4 10 5 9 4 10 i i
5 10 8 10 9 10 tl 9
5 9 7 9 3~ 6 4' 8
4 9 2 6 2 10 4: 5 . . , I
0 I 2 0 4 0 0 2
4: 9 6 7 5 8 ~ 8 ,, . . . . . . . . ~ L
9 10 _10 7 5 6 9 7
J Physically impaired
I Cognitivdy impaired
Digits indicate the number of patients having problems with and needing help to compTete each of the four ADLs listed.
All cognitively impaired residents needed emotional support and focusing help from staff to complete inch ADL 0nly with grooming did more than half if the physically impaired residents need emotional encouragement.
Geriatric Nursing July/August 1991 187