Embed Size (px)
Citation preview

Impact of Smoke-free laws on Preterm Birth
Kristin Ashford, PhD, APRN
Joyce Robl, EdD, MS, CGC
Ruth Ann Shepherd, MD, FAAP
Presenter Disclosures
The following personal financial relationships with commercial interests relevant to this presentation
existed during the past 12 months
No relationships to disclose
Background
The unintended health consequences of primary and secondhand smoke (SHS) exposure on adults and children are evident.
There is no safe level of SHS (Surgeon General, 2006)
SHS contains approximately 4,000 chemicals, is responsible for nearly 3,000 cases of lung cancer deaths among nonsmokers each year, and affects more than 22 million US children annually (Surgeon General, 2006).
A growing body of evidence and two recent meta-analyses support the associations between SHS and increased risk for low birth weight, smaller head circumference, stillbirth and preterm birth (Ashford et al., 2010, Hegaard et al., 2006, CDC, 2006, Salmasi et al., 2010, Leonardi-Bee et al., 2011).
Nonsmoking pregnant women exposed to SHS smoke have a 23% higher risk for stillbirth and 13% more likely to have a child with a congenital malformation (Leonardi-Bee et al., 2011).
Smokefree Laws and Perinatal Health
First US report on the effects of city-wide smoking ban on perinatal health was conducted in Pueblo, Colorado
(Page et al., 2012)
•Enacted July 1st 2003•Significant reductions in maternal smoking (38%): preterm birth (23%)
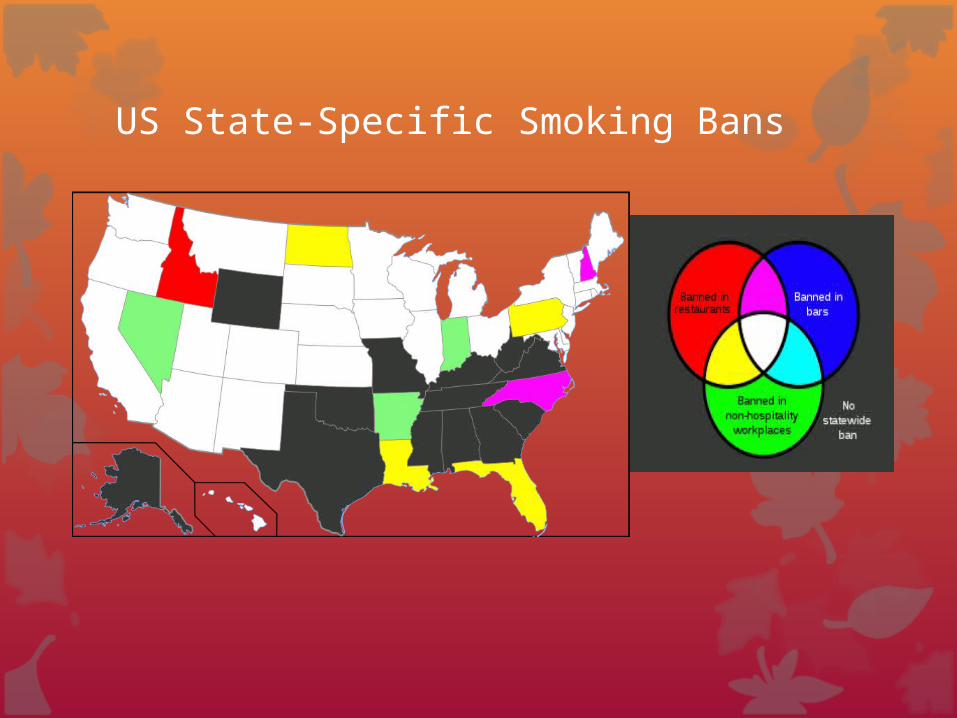
US State-Specific Smoking Bans
International Smokefree Laws and Perinatal Health
Ireland (2004): first country to adopted a comprehensive country-wide smoke-free policy
Italy (2005): significant reductions in first and SHS exposure
Scotland (2006) enacted the Smoking, Health and Social Care Bill prohibiting smoking in all enclosed public places (Mackay et al., 2012).
Preterm Delivery, Spontaneous Preterm Labor, Small for gestational age (SGA)
Spain reported a significant decrease in infants exposed to SHS during pregnancy following a comprehensive public ban (Puig et al., 2012).
China: nonsmoking pregnant women whose husbands were smokers reported increased exposure to SHS in home following smoke-free policy (Yao et al., 2009)
Purpose
To determine the impact of smoke-free laws on three key perinatal outcomes in Kentucky communities that have adopted legislation to ban public smoking:
1)community risk for preterm birth (PTB)
2)smoking prior to pregnancy (PRIOR)
3)low birth weight (LBW)
Secondary Aim: To determine the impact of strength
of smokefree law on perinatal outcomes
Methods
This study used Kentucky live birth certificate files from 2004 to 2009 in Kentucky counties/cities with smoke-free laws/ordinances.
Records were classified into pre-law and post-law based on at least one year prior to and after implementation, respectively with exclusion of implementation years.
Laws with smoke-free enclosed public places were classified as strong (smoke-free enclosed public places) or weak (significant exemptions).
Non-singleton births were excluded from the analyses.
Data Analysis
Descriptive demographic statistics
Chi square analyses compared the births pre-and post-law.
Multivariable logistic regressions were completed to relate LBW, PTB and PRIOR to ordinance timing, strength of law, and demographic explanatory variables.
All analyses were completed using SAS version 9.2
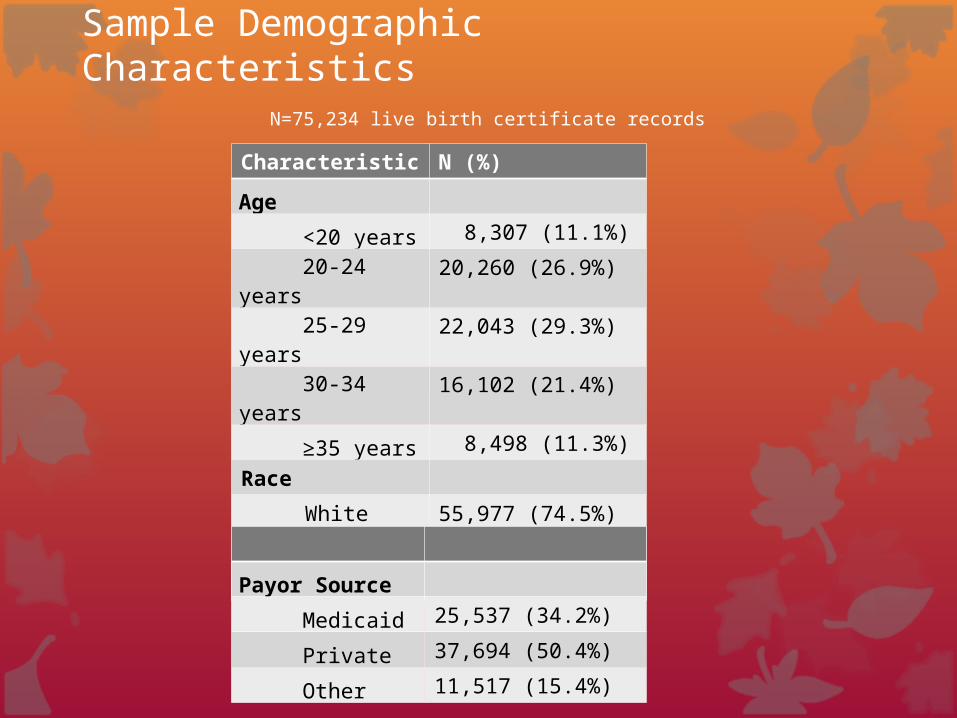
Sample Demographic Characteristics N=75,234 live birth certificate records
Characteristic N (%)
Age
<20 years 8,307 (11.1%)
20-24 years 20,260 (26.9%)
25-29 years 22,043 (29.3%)
30-34 years 16,102 (21.4%)
≥35 years 8,498 (11.3%)
Race
White 55,977 (74.5%)
Black 14,242 (18.9%)
Other 4,961 (6.6%)
Payor Source
Medicaid 25,537 (34.2%)
Private 37,694 (50.4%)
Other 11,517 (15.4%)
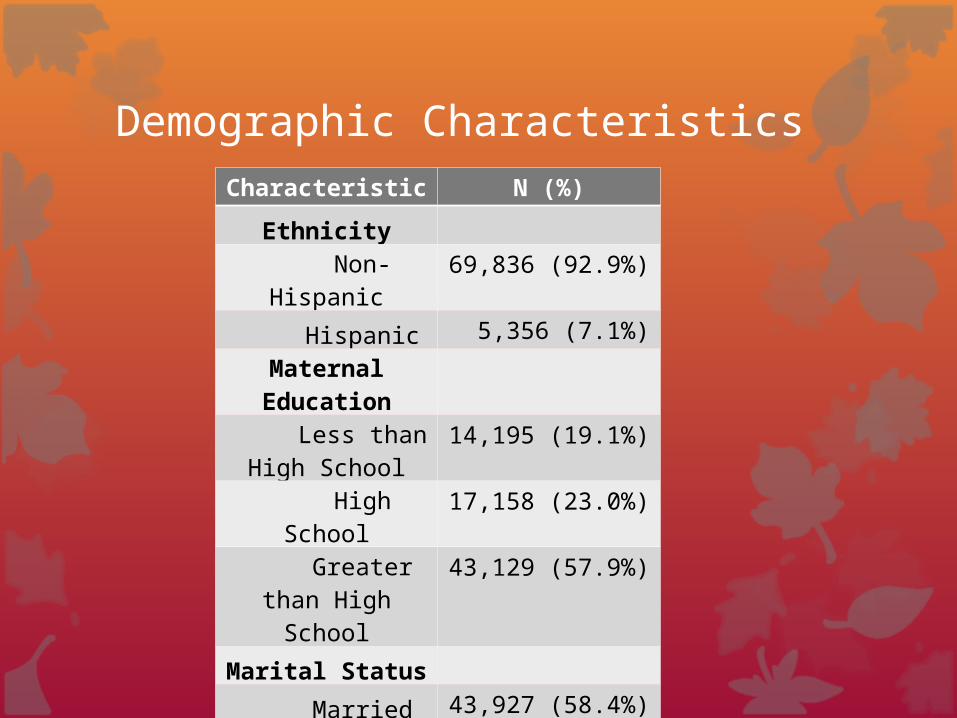
Demographic CharacteristicsCharacteristic N (%)
Ethnicity
Non-Hispanic 69,836 (92.9%)
Hispanic 5,356 (7.1%)
Maternal Education
Less than High School
14,195 (19.1%)
High School 17,158 (23.0%)
Greater than High School
43,129 (57.9%)
Marital Status
Married 43,927 (58.4%)
Unmarried 31,293 (41.6%)
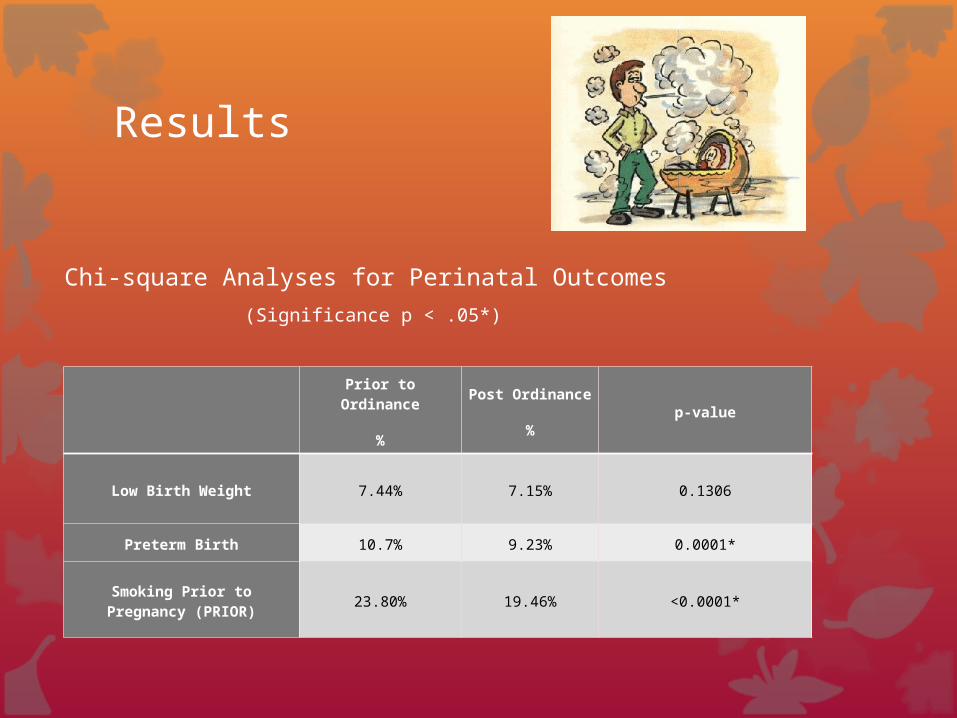
Results
Prior to Ordinance
%
Post Ordinance
%
p-value
Low Birth Weight 7.44% 7.15% 0.1306
Preterm Birth 10.7% 9.23% 0.0001*
Smoking Prior to Pregnancy (PRIOR)
23.80% 19.46% <0.0001*
Chi-square Analyses for Perinatal Outcomes
(Significance p < .05*)
Results
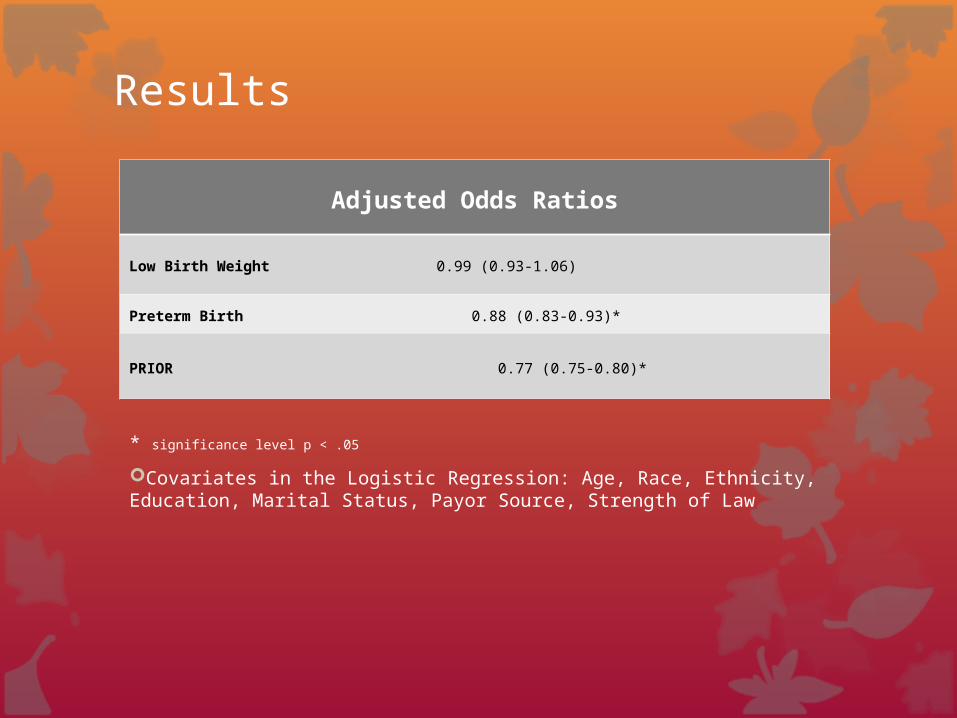
* significance level p < .05
Covariates in the Logistic Regression: Age, Race, Ethnicity, Education, Marital Status, Payor Source, Strength of Law
Adjusted Odds Ratios
Low Birth Weight 0.99 (0.93-1.06)
Preterm Birth 0.88 (0.83-0.93)*
PRIOR 0.77 (0.75-0.80)*
Results
Significant reductions in PTB and PRIOR were observed in communities post-law compared to pre-law (p <.0001). Births after implementation had reduced odds for PTB [Estimated Odds Ratio 0.87 (95% Confidence Interval 0.83-0.93)] and PRIOR [0.76 (0.73-0.79)].
Comprehensive strong laws demonstrated reduced odds for PTB [0.94 (0.88-0.997) and PRIOR [0.94 (0.90-0.99) compared to weak laws when controlling for the other variables.
Overall, there were no significant associations identified for LBW.
Limitations
Self report via Live Birth Certificate Records
Self report of smoking during perinatal period may not be reliable due to high deception rates
Lack of biomarker validation of smoking status

Discussion
This is one of the first studies in the US to examine the impact of large scale, community-based smoke-free laws on perinatal health outcomes.
Our study was consistent with the initial US report regarding significant reductions in PTB.
Communities can reduce smoking before pregnancy, reduce SHS to pregnant women and children, and decrease preterm birth rates through sustained and comprehensive smoke-free policies.
Strength of smoke-free policy positively impacts preterm birth and smoking three months prior to pregnancy rates when compared to less stringent laws that allow smoking exemptions.
QuestionsContact: Kristin.Ashford.uky.edu
University of Kentucky College of Nursing