Embed Size (px)
Citation preview

Impact of imaging on newer radiation
techniques in Gynaecological cancer

Morphology of local tumour (MRI)
Mapping of metastatic disease (PET/CT)
Tailored EBRT (IMRT, selective dose escalation)
Conformal brachytherapy (reduced toxicity, ? Improved control & survival?)
Newer insight into clinical behaviour of cancer

FIGO Staging of cervix cancer
Five year survival from around the world
Stage-1Stage-2 Stage-3 Stage-4
52-90%38-68% 22-61% 0-10%

Cervix, 6 cm 2bExamination under anaesthesia
Axial MRI
02/11/02663

-2
0
2
4
6
8
10
12
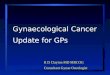
0 2 4 6 8 10 12
Cervical histology
MR
I / E
UA Histology
EUA
MRI






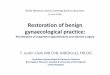
41 year old
FIGO IIIB
Extensive infiltration lower uterine segment
Exophytic component in vaginal lumen
Infiltrating beyond the vagina on left
Mass 5.7 x 4.8 x 6.2 cm
Left parametrial extension
L external iliac node

40 Gy Whole Pelvis
Ant & Post R&L lateral fields
Prone on Bellyboard
Ant-Post R&L Lat fields
10 Gy boost to Left ext iliac node
10 Gy boost
LPSW

40 Gy + cisplat (+10 Gy LN boost)
Bulk of tumour resolved
Residual tumour left cervix and upper vagina
Extension into left parametrium

Tandem inserted using real time Ultrasound guidance
MRI taken one hour after insertion and treatment
Patient moved from brachy theatre to MRI scanner

Dose escalationRadiation resistanceInfiltrating diseasePresence of metastases

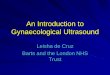
In conformal brachytherapy where dose is limited to residual tumour,the incident dose at point A is variable.
In patients treated with LDR the dose (80 Gy) was prescribed to Point A.This meant that patients who responded well to EBRT had small residual withdiameter of <4cm. All such tumours would have received much higher than the prescribed 80 Gy and hence had unintended dose escalation!






Mobilization of Viable Tumour Cells into the CirculationDuring Radiation Therapy. Martin et al 2013, Red journal10.1016/j.ijrobp.2013.10.033

A randomised, two-by-two factorial phase 3 study.Stage IIIA or IIIB non-small-cell lung cancer(RTOG 0617): (Bradley et al. 2015).
Standard-dose versus high-dose conformal radiotherapy high-dose (74 Gy in 37 fractions) or standard dose (60 Gy in 30 fractions) radiotherapy concurrently with weekly paclitaxel and carboplatin
with or without cetuximab, followed by consolidation chemotherapy in all groups.


Interpretation of results were: 74 Gy with concurrent chemotherapynot better than 60 Gy plus concurrent chemotherapy
Addition of cetuximab to concurrent chemoradiation and consolidation treatment provided no benefit in OS
Median overall survival was 28·7 months for 60 GyAnd 20·3 months (17·7–25·0) for 74 Gy

The authors of RTOG 0617 still believe the way forward is still the radiation dose intensification!
RTOG 1106 is using a mid-treatment PET adapted hypofractionated radiation therapy boost to intensify radiation dose to residual tumour volumes during a total duration of 30 fractions (NCT01507428).
RTOG 1308 is exploiting the protons compared with photons to escalate radiation dose to 70 Gy (NCT01993810).
Both of these trial designs were built on the knowledge gained from RTOG 0617.


Questions…