Embed Size (px)
Citation preview

Conservative Surgery to Preserve Conservative Surgery to Preserve Fertility in Gynaecological Cancers.Fertility in Gynaecological Cancers.
Sean KehoeSean KehoeOxford Gynaecological Cancer CentreOxford Gynaecological Cancer Centre
Churchill HospitalChurchill HospitalOxfordOxford

MalignanciesMalignancies
CervicalCervical EndometrialEndometrial OvarianOvarian Vulval Cancer ?Vulval Cancer ?

CounsellingCounselling
Counselling is very importantCounselling is very important
Often we are deviating from what Often we are deviating from what could be considered the ‘Standard could be considered the ‘Standard Recommendations’Recommendations’
In essence – experimentation with In essence – experimentation with the patient taking the risk.the patient taking the risk.

Cervical Carcinoma
Occurs not uncommonly in younger patients [33% < 40 years]
A real increase in adenocarcinomas
An impression of more cases occurring in nulliparous women – probably due to women delaying pregnancies as compared to previous times.

0
100
200
300
400
0-4
5-9
10-1
415
-19
20-2
425
-29
30-3
435
-39
40-4
445
-49
50-5
455
-59
60-6
465
-69
70-7
475
-79
80-8
485
+
Age at diagnosis
Num
ber o
f cas
es
0
5
10
15
20
Rate
per
100
,000
pop
ulat
ion
Female cases
Female rates
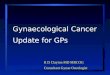
Figure 1.1: Numbers of new cases and age specific incidence rates, cervical cancer, UK 2004
About 33% of cervical carcinomas occur in women <40 years

Cervical CarcinomaCervical Carcinoma
Severe Dyskaryosis ? InvasionSevere Dyskaryosis ? Invasion
? Invasion on Colposcopy? Invasion on Colposcopy
Requires some form of biopsyRequires some form of biopsy

Stage 1A1 – Squamous CarcinomaStage 1A1 – Squamous Carcinoma
A loop cone excision of the cervix is sufficient treatment
Once all pre-invasive and invasive disease cleared.

Stage 1A1 AdenocarcinomaStage 1A1 Adenocarcinoma
Problem with ‘definition’
Now staging as 1A1 is acceptable
Skip lesions can occur : ? Just Pre-invasive
For lesions 3 -5 mm x 7 mm, 141 women – only 1 case oflymph node disease [0.73%]

Cervical Cancer: Cervical Cancer: TrachelectomyTrachelectomy
RulesRules Nulliparous [?] – family incompleteNulliparous [?] – family incomplete Careful clinical stagingCareful clinical staging MRI scan to evaluate tumour extent.MRI scan to evaluate tumour extent. Ib1 [2cms] or less.Ib1 [2cms] or less. Adenocarcinomas ?Adenocarcinomas ? ? Poorly Differentiated? Poorly Differentiated ?Lymph Vascular Space Invasion?Lymph Vascular Space Invasion

TrachelectomyTrachelectomy
Excise to Isthmus
Insert Cervical Circlage

Cervical Circlage
Parametrial Tissue
But will surgery be further modified?Why parametrial tissue which addresses only 2 of 4 planes ?
In tumour <10mm invasion and <2cms diameter – incidence ofparametrial involvement is estimates at 0.6%
Cervical Cancer

Cervical Cancer
Single or 2 stage procedure ?
If single – depending on Frozen Section Histology
Extra-peritoneal or Intra-peritoneal Lymphadenectomy?
If the procedure is about preserving fertility – it seemslogical to prevent intra-peritoneal surgery when an alternative is available.

Beiner ME and Covens A (2007) Surgery Insight: radical vaginal trachelectomy as a method of fertility preservation for cervical cancer Nat Clin Pract Oncol 4: 353–361 doi:10.1038/ncponc0822
Patients and tumor characteristics for the seven clinical studies of radical vaginal trachelectomy

Beiner ME and Covens A (2007) Surgery Insight: radical vaginal trachelectomy as a method of fertility preservation for cervical cancer Nat Clin Pract Oncol 4: 353–361 doi:10.1038/ncponc0822
Table 2 Operative data and complications in the seven clinical studies of radical vaginal trachelectomy

Beiner ME and Covens A (2007) Surgery Insight: radical vaginal trachelectomy as a method of fertility preservation for cervical cancer Nat Clin Pract Oncol 4: 353–361 doi:10.1038/ncponc0822
Table 7 Number of obstetric outcomes in patients who underwent trachelectomy

CounsellingCounselling
Pregnancy:Pregnancy:
If achieved –If achieved –
30% miscarriage rate30% miscarriage rate
Assume – Premature Assume – Premature deliverydelivery
Assume – Operative Assume – Operative DeliveryDelivery

Recurrence Rates
To date the recurrence rates at about 4% are not in excess of that expectedwith a radical hysterectomy.
The application of this procedure to large tumours is less frequent now.

How Safe: Trachelectomy?How Safe: Trachelectomy?
Case selection very importantCase selection very important ProbablyProbably as safe as Radical as safe as Radical
ProceduresProcedures Avoid in Large tumours [>2cms ?]Avoid in Large tumours [>2cms ?] Avoid in rare/high risk tumoursAvoid in rare/high risk tumours For nulliparous women only? For nulliparous women only?

ENDOMETRIAL CANCERENDOMETRIAL CANCER

Endometrial CancerEndometrial Cancer
A Rare issue in women where fertility A Rare issue in women where fertility is a factor.is a factor.
HistopathologyHistopathology ImagingImagingBoth of these are paramount in decision Both of these are paramount in decision
making.making.

Histology: Histology: Differentiation between Atypical Differentiation between Atypical Hyperplasia and Frank CarcinomaHyperplasia and Frank Carcinoma
Remember – when tissue confirms Atypical Remember – when tissue confirms Atypical Hyperplasia – Hyperplasia – Frank MalignancyFrank Malignancy is found in is found in the Hysterectomy specimen in 40-50% of the Hysterectomy specimen in 40-50% of cases [Cancer 2006,GOG study]cases [Cancer 2006,GOG study]
Most would agree that fertility Most would agree that fertility preservation should be limited to those preservation should be limited to those with with well differentiated tumours [stage 1A]well differentiated tumours [stage 1A]
Endometrial CancerEndometrial Cancer

Imaging:Imaging:
This is important for the ‘staging’ process.This is important for the ‘staging’ process.
CT/MTI/Ultrasound?CT/MTI/Ultrasound?
Kinkel et al,Kinkel et al,Radiology 1999: Meta-analysisRadiology 1999: Meta-analysis
Contrast enhanced MRI best – BUT of note Contrast enhanced MRI best – BUT of note myometrial invasion detected correctly myometrial invasion detected correctly in 90% of cases – i.e. 10% false negative in 90% of cases – i.e. 10% false negative rate.rate.
Endometrial CancerEndometrial Cancer

In the main – progestagens used as therapy.
Treatment time to regression ranges from 3.5 – 9 months
Recurrence occurs in about 20% of responders
This approach requires careful surveillance – and repeated endometrial curettage.
Endometrial CancerEndometrial Cancer

How to manage??How to manage??
Endometrial CancerEndometrial Cancer
Mirena IUCD
Progestogens:
GnRH analogues
All the above have been used with reasonable success [responses about 70%].
Tamoxifen can increase the PR, and hence potentially enhancethe efficacy of progestagenic agents

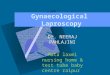
Endometrial CancerEndometrial Cancer
Curettage at 3/12
Curettage at 6/12
If - If +
Attempt pregnancy
OfferHysterectomy
InterveneIf
Anyconcerns
Stage 1aTreatment

Ref Cases Response Pregnancies
Kaku 2001 12 75% 2
Imai 2001 15 50% 2
Randall 1997 14 75% ?
Gotlieb 2003 13 100% 9 babies
Signorelli, 2009 21 57% 13 pregnancies
Laurelli 2011 14 90% 1 baby
Miniq, 2011 14 57% 11 pregnancies
Endometrial CancerEndometrial Cancer

Ushijima et al. J. Clinical Oncology 2007Ushijima et al. J. Clinical Oncology 2007 28 Stage 1 A, 17 Atypical hyperplasia, all < 40 years28 Stage 1 A, 17 Atypical hyperplasia, all < 40 years
600mgs MPA with low dose aspirin600mgs MPA with low dose aspirin
Continued for 28 weeks once respondingContinued for 28 weeks once responding Endometrium checked 8 and 16 weeksEndometrium checked 8 and 16 weeks
CR 55% Endometrial CA, and 82% AHCR 55% Endometrial CA, and 82% AH
In responders– either oestrogen/progesterone therapy or Fertility In responders– either oestrogen/progesterone therapy or Fertility therapy.therapy.
36 months follow-up – 12 pregnancies and 7 deliveries36 months follow-up – 12 pregnancies and 7 deliveries
However 47% recurrence rate – However 47% recurrence rate – need careful monitoringneed careful monitoring
Endometrial CancerEndometrial Cancer

Taiwan J Obstet Gynecol. 2011 Mar;50(1):62-6.Obstetric outcomes of pregnancy after conservative treatment of endometrial cancer: case series and literature review.Chao AS, Chao A, Wang CJ, Lai CH, Wang HS
Distribution of clinicopathological characteristics in the endometrial cancer patients with conception in the meta-analysisCharacteristics Patients no. Group 1 Group 2 p
Age at diagnosis, yr (mean SD) 50 32.8 , 4.1 (n = 14) 29.5, 5.3 (n = 36) 0.05Age at pregnancy, yr (mean SD) 43 34.3, 4.0 (n = 13) 30.9 , 5.3 (n = 30) 0.05Histology type 45 14 31 1.0Adenocarcinoma 44 14 30Adenosquamous 1 0 1Grade of differentiation 41 14 27 1.0Well 38 13 25Moderate and poor 3 1 2Hysterectomy after childbearing 50 14 36 0.70Yes 9 3 6No 41 11 30Metastasis/recurrence 50 14 36 0.57Yes 4 0 4No 46 14 32

Analyses of obstetric outcomes according to undergoing: IVF, ICSI, gamete intrafallopian transfer, or zygote intrafallopian transfer (Group 1)
and spontaneous conception/intrauterine insemination (Group 2)
Group 1 (n=15) Group 2 (n=50) p
Preterm labor 7 (46.7) 3 (6.0) 0.001Cesarean rate 14 (93.3) 11 (22.0) <0.001Primigravida 14 (93.3) 36 (72.0) 0.160Multiple pregnancy 6 (40.0) 3 (6.0) 0.003
Taiwan J Obstet Gynecol. 2011 Mar;50(1):62-6.Obstetric outcomes of pregnancy after conservative treatment of endometrial cancer: case series and literature review.Chao AS, Chao A, Wang CJ, Lai CH, Wang HS
yesplatform+mauthorauthor

How safe : Endometrial cancer?How safe : Endometrial cancer?
Numbers are too small to make any Numbers are too small to make any dogmatic statements.dogmatic statements.
We can preserve fertilityWe can preserve fertility
After single delivery – most After single delivery – most recommend hysterectomy.recommend hysterectomy.

Ovarian CancerOvarian Cancer
Agreed fertility preservation in all young Agreed fertility preservation in all young patients [?<40 years]- as:patients [?<40 years]- as:
1. Germ cell tumours very chemosensitive1. Germ cell tumours very chemosensitive 2. Borderline tumours – normally cured 2. Borderline tumours – normally cured
with local excision [ if early stage]with local excision [ if early stage] 3. If advanced ovarian cancer – then can 3. If advanced ovarian cancer – then can
always re-operate.always re-operate. 4. May be another condition – eg Hodgkins 4. May be another condition – eg Hodgkins
!!!!

Invasive Early stage disease
Schilder et al, Gynecol Oncol, 2002
N = 52 42 stage 1A 10 stage 1CGrade 1 = 35 Grade 2= 9 Grade 3 = 5
20 had adjuvant chemotherapy
5 recurrences [8-78 months after first surgery]Sites : Contralateral ovary – 3 , peritoneum 1 and lung 1.
2 deaths
24 attempted pregnancies – 71% conceived. Survival at 5 years 98% and 10 years 93%

Fertility-sparing surgery in young women with mucinous adenocarcinoma Fertility-sparing surgery in young women with mucinous adenocarcinoma of the ovary.of the ovary.
Gynecol Oncol. 2011 Aug;122(2):334-8. Gynecol Oncol. 2011 Aug;122(2):334-8. Kajiyama H et al,JapanKajiyama H et al,Japan
N=148,The median follow-up time of all mEOC patients was 71.6 (4.8-448.3) months
41 patients with Fertility Sparing, 27 = Stage 1a, 14 Stage 1c
5 year overall survival was 97.3%
Compared with 101 women who underwent Radical surgery for the Same disease – there was no difference in outcome.

Germ Cell Tumours
Ref Cases Chemo Preg Survival
Perrin 1999 45 29 7 babies 2 deaths
Sagae 2003 26 23 4 pregnancies – no deaths
Zanetta 2001 138 81 40 babies 95% 5 year
For Germ cell tumours – outcome excellent. Most problemswere in the more advanced stage diseases.
Fertility can be retained.

Borderline Ovarian Tumours
Ref Cases Recurrence Pregnancies
Gotlieb, 2003 39 8% 22 in 15 women
Zanetta,2001 189 18% 41in 21 women
Demeter, 2002 12 ? 50%
Donnez,2003 16 18.7% 64%
Boran 2004 62 6.5% 13 in 10 women
Rao , 2005 38 16% 6 in 5 women

What if Cystectomy performed ?What if Cystectomy performed ?
A. If malignant – proceed to A. If malignant – proceed to oophorectomy and full stagingoophorectomy and full staging
B. If borderline – oophorectomy – B. If borderline – oophorectomy – reduces recurrence ratesreduces recurrence rates
Ovarian CancerOvarian Cancer

Must Monitor the Contra-lateral Must Monitor the Contra-lateral ovary.ovary.
Ultrasound/tumour markers.Ultrasound/tumour markers.
Ovarian CancerOvarian Cancer

Fertility SparingFertility Sparing Radical Radical Recurrence Recurrence
Boran 2005Boran 2005 6262 8080 6.5% vs 0.0%6.5% vs 0.0%
Zanetta 2001Zanetta 2001 189*189* 150150 18.5 % vs 4.6%18.5 % vs 4.6%• 7 cases progressed to ‘invasive’ carcinoma7 cases progressed to ‘invasive’ carcinoma
Important to counsel the patient and is this evidence toImportant to counsel the patient and is this evidence to
support routine pelvic clearance after completion of thesupport routine pelvic clearance after completion of the
family ??family ??
Borderline Ovarian CancerBorderline Ovarian Cancer

Fertility conservation safe for Borderline Fertility conservation safe for Borderline tumours.tumours.
In invasive tumours – probably best to In invasive tumours – probably best to restrict fertility preservation surgery to restrict fertility preservation surgery to properly staged, Stage 1 disease.properly staged, Stage 1 disease.
Following completion of family – pelvic Following completion of family – pelvic clearance seems a logical approach to clearance seems a logical approach to reduce recurrences, and considering the reduce recurrences, and considering the limitations of screening such women.limitations of screening such women.
Ovarian CancerOvarian Cancer

Yes it can be done – but always the Yes it can be done – but always the question is :question is :Should it be done?Should it be done?
Need the full Multidisciplinary Team – Need the full Multidisciplinary Team – Oncological and Fertility Working Oncological and Fertility Working together. [?Obstetric/Neonatal?]together. [?Obstetric/Neonatal?]
Counsell– Counsell and CounsellCounsell– Counsell and Counsell
ConclusionsConclusions

A Healthy Mother and Child