Embed Size (px)
Citation preview

Impact of Anemia in Patients with Head and Neck Cancer Treated with Radiation TherapyKenneth Hu, MD*
Louis B. Harrison, MD
Address*The Charles and Bernice Blitman Department of Radiation Oncology, Beth Israel Medical Center, 10 Union Square East, New York, NY 10003, USA.E-mail: [email protected]
Current Treatment Options in Oncology 2005, 6:31–45Current Science Inc. ISSN 1527-2729Copyright © 2005 by Current Science Inc.
IntroductionRadiation therapy remains an integral component of carefor most locally advanced head and neck cancers as defin-itive treatment or adjuvant therapy after radical resection.Chemotherapy enhances rather than replaces thisapproach for local control and improves the chance fororgan preservation [1–3]. Local tumor recurrence in theradiated field is often implicated as a primary cause oftreatment failure after potentially curative radiation ther-apy for locally advanced head and neck cancers. Accumu-lating data strongly suggest that outcomes after curative-intent radiation therapy are adversely influenced by thepresence of anemia [4]. Anemia is common in patientspresenting for radiation therapy resulting from the under-lying disease or previous treatment [5•]. During thecourse of radiation therapy, especially when combinedwith concurrent chemotherapy, the prevalence of anemiaincreases markedly [5•,6,7]. Therefore, most patients are
at risk of becoming anemic or are already anemic at theirfirst visit to a radiation oncologist. In most radiationoncology settings, anemia-directed interventions are notinstituted in patients unless they are hemodynamicallysymptomatic or their hemoglobin (Hgb) levels fall belowa threshold of 9 to 10 g/dL. However, early correction ofmild-to-moderate anemia, such as a Hgb ranging from 12to 14 g/dL, may improve locoregional control and patientquality of life (QOL) and is a potential means of delayingthe development or progression of intratumoral hypoxia.
This review focuses on the prognostic significance ofHgb levels in patients undergoing definitive radiationtherapy, alone or combined with surgery and chemother-apy, for cancer of the head and neck. In addition, the roleof anemia-directed approaches in improving radiationoutcomes is summarized and emphasizes that effectivecorrection can be achieved.
Opinion statementLocoregional recurrence remains a major obstacle to achieving a cure of locally advanced head and neck cancers, despite multimodality therapy. Multiple studies report that a low hemoglobin (Hgb) before or during radiation therapy is an important risk factor for poor locoregional disease control and survival. Anemia is common in the head and neck cancer population and is suspected to contribute to intratumoral hypoxia with resultant radio-resistance. Although having a low Hgb level has been shown to be detrimental, it is unclear as to exactly what the threshold should be for low Hgb (studies in this area have used thresholds ranging from 9–14.5 g/dL). Quality-of-life studies suggest that correction of moderately severe anemia may result in significant gains. Optimal Hgb levels for improving outcomes may vary across and within tumor types, and this is an area that requires further evaluation. However, the correction of anemia may be a worth-while strategy for radiation oncologists to improve local control and survival. This article reviews the impact of anemia on outcomes after radiotherapy of head and neck cancers.

32 Head and Neck Cancer
Treatment
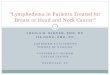
• The incidence of anemia in patients with head and neck cancer before treat-ment varies in extent, depending on its definition. When defined as Hgb lower than 14.5 g/dL for men or lower than 13 g/dL for women, the inci-dence of pretreatment anemia in several randomized head and neck cancer trials testing nitroimidazoles have ranged from 64% in the Radiation Ther-apy Oncology Group (RTOG) trial 85 to 27 (misonidazole) involving 521 patients with stage III/IV disease treated with definitive radiation to 56% in RTOG 79-15 (misonidazole) involving 297 patients and 41% in the Danish Head and Neck Cancer (DAHANCA; nimorazole) trial involving 414 patients [8–10]. However, if defined by the World Health Organization defi-nition of lower than 12 g/dL, the incidence of anemia is lower. In a review of a patients with head and neck cancer presenting for radiotherapy at our institution between December 1996 and June 1999, 16% of the patients were anemic at baseline (within 4 weeks before radiotherapy) and 32% became anemic within 3 to 5 weeks after receiving the first dose of radiation (Fig. 1). Although this result was modest compared to the entire group of patients surveyed (overall 41% of patients were found to be anemic at base-line and 54% during treatment), the mean decrease in Hgb was 1.8 g/dL for patients with head and neck cancer, the highest of all the subsets of patients (Fig. 2). When the prevalence of anemia for head and neck cancer was strati-fied by the Hgb level measured at baseline and the lowest level recorded dur-ing radiotherapy, most of the patients had mild anemia (World Health Organization grade 1; Hgb > 10 g/dL), which is amenable to correction.
• The incidence of anemia also varies by subsite and time-point of measure-ment with respect to radiotherapy. Dubray et al. [11] reported that the inci-dence of pretreatment anemia (Hgb < 13.5 g/dL for men and < 12 g/dL for women) for all patients was 15% (45 of 305) and 40% (20 of 50) for supra-glottic laryngeal (SGL) cancers versus 12% (25 of 205) for glottic laryngeal (GL) cancers. After radiotherapy, the incidence of post-treatment anemia was 30% (66 of 220) and 56% (25 of 45) for SGL versus 23% (41 of 175) for GL.
• As the use of concurrent chemotherapy with definitive radiation has become more common for nasopharyngeal, hypopharyngeal, laryngeal, and oropharyngeal cancers, most patients will become anemic to some extent [3,12–16]. In our experience, for patients receiving concurrent chemoradia-tion using accelerated radiation by concomitant boost with two cycles of cisplatin for organ preservation or nasopharyngeal treatment, 96% of patients became anemic (< 12 g/dL) by the end of treatment [6,7]. Other chemoradiation experiences have reported nearly all of the patients becom-ing anemic during treatment [17•].
• It is thought that the presence of anemia may decrease oxygen-carrying capacity and create hypoxic conditions, which would serve as an obstacle to achieving maximal locoregional control after radiotherapy. It has been estimated that the dose of radiation required to kill tumor cells under hypoxic conditions is two to three times the dose required in a normoxic environ-ment. However, studies measuring tumor oxygenation and anemia show only a loose correlation between these two conditions.
• A few reports show some correlation between anemia and increased hypoxia in solid tumors [18–20]. Stadler et al. [18] showed a weak correlation between hypoxic volume and Hgb concentration (Pearson one-sided;
Incidence of anemia in patients with head and neck cancer
Anemia and hypoxia

Radiation Treatment for Patients with Anemia Hu and Harrison 33
P < 0.0005). Brizel et al. [21] demonstrated a loose association between poor tumor oxygenation (< 10 mm Hg) and anemia (Spearman correlation coefficient 0.27; P=0.04), whereas Nordsmark and Overgaard [22] noted no correlation between hypoxia and anemia, but they were independent factors predictive for poorer local control and survival.
• Because of the numerous parameters that influence hypoxia (eg, Hgb, oxygenation, tumor metabolism, and diffusion/perfusion factors), it is not surprising that the relation is unclear. Acute changes in Hgb are known to alter intratumoral hypoxia and reduce radiosensitivity, but the effect of chronic anemia, which is more common in patients with cancer, is more difficult to estimate because of adaptive hematopoietic responses over time [23–25]. Therefore, the relationship between hypoxia and anemia and its relevance in the clinical setting remains controversial [25,26]. The prognostic significance of anemia may simply reflect progressive or advanced disease that is refractory to radiation therapy. However, emerging evidence suggests that correction of anemia may enhance radiosensitivity of solid tumors, supporting the theory that there is a direct relationship between lower Hgb levels and increased hypoxia [10,27].
Figure 1. The prevalence of anemia (hemoglobin < 12 g/dL) before and during radiotherapy in patients at Beth Israel Medical Center/St. Luke’s Roosevelt Hospital Center (New York, NY) between December 1996 and June 1999. Baseline was defined as within 4 weeks before the first radiation dose. During therapy was defined as within 3 to 5 weeks of the first radiation dose.
Figure 2. Mean decrease in hemoglobin levels during radiotherapy versus preradiotherapy in patients treated at Beth Israel Medical Center/St. Luke’s Roosevelt Hospital Center (New York, NY) between December 1996 and June 1999. Data shown are for patients whose hemoglobin levels decreased during treatment. Statistically significant difference versus baseline (P < 0.001).
34 Head and Neck Cancer
Tabl
e 1.
Pro
gnos
tic
sign
ific
ance
of
pret
reat
men
t or
pos
t-tr
eatm
ent
anem
ia in
pat
ient
s w
ith
head
and
nec
k ca
ncer
tre
ated
wit
h ra
diat
ion
(sel
ecte
d st
udie
s pu
blis
hed
sinc
e 19
95)
Stud
ySt
age
(pat
ient
s ev
alua
ted)
Trea
tmen
tH
gb*
Outc
ome
para
met
er(s
)P
valu
e on
mul
ti-
vari
ate
anal
ysis
Stad
ler
et a
l. [1
8]Ad
vanc
ed
(oft
en s
tage
IVA
) SC
CHN
(59)
Frac
tion
ated
RT:
2 G
y/d
× 5
d/w
k (t
otal
dos
e 66
–72
Gy)
or 2
Gy
twic
e da
ily ×
5 d
/wk
to 1
6 Gy
→ 1
.4 G
y ×
10 F
R/w
k (t
otal
dos
e 77
.6 G
y) o
r ch
emor
adia
tion
: m
itom
ycin
C/
5-flu
orou
raci
l plu
s co
nven
tion
al o
r hy
perf
ract
iona
ted
RT,
typi
cally
adm
inis
tere
d as
a s
plit
-cou
rse
(2-w
k br
eak
afte
r 30
Gy)
≤ 12.
5 g/
dLOv
eral
l sur
viva
l0.
01
Over
gaar
d et
al.
[38]
414
62–6
8 Gy
for
6–7
wk
< 9
mm
ol/L
(m
en);
<
8 m
mol
/L (
wom
en)
Loco
regi
onal
con
trol
0.02
Gran
t et
al.
[35]
T1/T
2 la
ryng
eal
(117
)Fr
acti
onat
ed R
T<
13 g
/dL
(men
);
< 11
.5 g
/dL
(wom
en)
Recu
rren
ce-f
ree
surv
ival
0.00
94
Lee
et a
l. [8
]St
age
III
or I
V SC
CHN
(451
)Fr
acti
onat
ed R
T ±
etha
nida
zole
: 33
–37
FR a
dmin
iste
red
5 d/
wk
for
a to
tal d
ose
of 6
6–74
Gy
< 14
.5 g
/dL
(men
);
< 13
g/d
L (w
omen
)5-
y lo
core
gion
al c
ontr
ol;
5-y
over
all s
urvi
val
0.00
32;
0.00
9
War
de e
t al
. [2
4]T1
/T2
glot
tic
(735
)Fr
acti
onat
ed R
T: 2
0 FR
adm
inis
tere
d ov
er 4
wk
for
a to
tal
dose
of
50 G
yCo
ntin
uum
†Lo
cal c
ontr
ol0.
006
Dubr
ay e
t al
. [1
1]Or
al c
avit
y,
orop
hary
ngea
l, hy
poph
aryn
geal
, or
lary
ngea
l (21
7)
Frac
tion
ated
RT:
2 G
y/FR
× 5
FR/
wk
for
a to
tal d
ose
of 7
0 Gy
< 13
.5 g
/dL
(men
);
< 12
g/d
L (w
omen
)2-
y lo
core
gion
al c
ontr
ol;
over
all s
urvi
val
0.06
; 0.
04
Fein
et
al.
[33]
T1/T
2 gl
otti
c (1
09)
Frac
tion
ated
RT:
T1
lesi
ons
1.74
–2.0
3 Gy
× 5
FR/
wk
for
a to
tal d
ose
of 6
0–70
.8 G
y; T
2 le
sion
s on
ce-
or t
wic
e-da
ily
frac
tion
atio
n fo
r a
tota
l dos
e of
64–
76.2
9 Gy
Cont
inuu
m†
2-y
loco
regi
onal
con
trol
; 2-
y ov
eral
l sur
viva
l0.
0016
; <
0.00
01
Had
dad
et a
l. [3
7]11
6Ch
emor
adia
tion
< 12
g/d
LRe
spon
se a
t pr
imar
y si
te0.
05va
n Ac
ht e
t al
. [3
4]‡
306
60–7
0 Gy
for
6–7
wk
< 11
mm
ol/L
(m
en);
<
10 m
mol
/L (
wom
en)
Dise
ase-
free
sur
viva
l<
0.00
12 (
glot
-ti
s);
0.05
(s
upra
glot
tis)
Tarn
awsk
i et
al. [4
0]‡84
760
–70
Gy f
or 5
–7 w
kNS
Loca
l con
trol
0
* Rep
rese
nts
the
hem
oglo
bin
cut-
off
valu
e as
soci
ated
wit
h po
or o
utco
me.
† V
ario
us h
emog
lobi
n le
vels
, ra
ther
tha
n a
spec
ific
thr
esho
ld,
wer
e an
alyz
ed in
the
mul
tiva
riate
ana
lysi
s.‡ P
ost-
trea
tmen
t an
emia
.EB
RT—
exte
rnal
bea
m r
adia
tion
the
rapy
; FR
—fr
acti
on;
Hgb
—he
mog
lobi
n; N
S—no
nsig
nific
ant;
RT—
radi
atio
n th
erap
y; S
CCH
N—sq
uam
ous
cell
carc
inom
a of
the
hea
d an
d ne
ck.

Radiation Treatment for Patients with Anemia Hu and Harrison 35
• The negative impact of pretreatment anemia (using Hgb level thresholds of 9–14.5 g/dL) on postradiation locoregional control and survival has been best documented over the past 35 years in patients with squamous cell carcinoma of the head and neck and the uterine cervix and other solid tumors (eg, bladder, lung, anus, and prostate) [1,2,10,24,28–32]. Table 1 provides selected retrospective studies that evaluated head and neck outcomes by preradiation Hgb level [1,2,8,11,24,28,33–36]. Blitzer et al. [36] reported that lower levels of Hgbs were associated with decreased local control in patients with advanced T-stage head and neck cancer treated with definitive radiation. Based on a Cox model of their data, they predicted an approximately 10% drop in locoregional control for every 2-g/dL drop (estimated 2-year locoregional con-trol 26% for Hgb = 12g/dL, 37% for Hgb = 14g/dL, and 47% for Hgb = 16). Dubray et al. [11] reported reduced 2-year locoregional control (50% vs 76%; P < 0.00001) and 2-year survival rates (49% vs 77%; P < 0.00001) associated with pretreatment anemia (men < 13.5g/dL and women < 12g/dL) for 217 patients in tumors involving the larynx, oral cavity, hypopharynx, oropharynx, and oral cavity. Pretreatment anemia was associated with higher T or N stage, older patients, and weight loss. On multivariate analysis, pretreatment anemia was significantly associated with poorer survival (P=0.04; relative risk 1.7) and was borderline significant for worse locoregional control (P = 0.06; relative risk 1.6). Haddad et al. [37] reported that on multivariate analysis of 116 patients treated on three chemoradiation consecutive studies that pretreat-ment Hgb of lower than 12 g/dL predicted a worse response rate at the primary site compared to Hgb higher than 12 g/dL (P=0.05). No statistically significant impact on survival was noted.
• Results generally have been highly consistent and reproducible, with nearly all univariate and multivariate analyses finding a low pretreatment Hgb level to be a significant prognostic indicator of disease control and survival after potentially curative radiation therapy, regardless of disease-specific char-acteristics (eg, tumor stage and lymph node involvement). Findings from approximately 50% of these studies suggest that the Hgb threshold in the radiation oncology setting should be within the range of 12 to 14 g/dL.
• Randomized studies that stratify patients by pretreatment anemia offer the least biased analysis of the impact of this factor on patients with head and neck cancer. Therefore, the best data have been large randomized trials testing the role of nitroimidazole radiosensitizers in head and neck cancers treated with definitive radiation therapy. Although the studies have yielded mixed results regarding the benefit of nitroimidazoles, they have consistently shown a correlation between pretreatment anemia and patient outcomes.
• In the DAHANCA II study, 626 patients with laryngeal or pharyngeal cancers were randomized in a multicenter study to definitive radiation with or with-out misonidazole [38]. Male patients with pharyngeal (ie, nasopharyngeal, oropharyngeal, and hypopharyngeal) tumors in the misonidazole arm had worse 5-year local control rates if pretreatment Hgb levels were lower than 14.5 g/dL compared to patients receiving a placebo with Hgb higher than 14.5 g/dL (5-year local control 14% vs 61%). For all male patients, the 3-year survival was improved in patients with Hgb higher than 14.5 g/d (76% vs 59%; P < 0.001) compared to patients with Hgb lower than 14.5 g/dL. Local control was also improved (58% vs 46%; P < 0.01). The RTOG 79-15 study, which randomized patients with head and neck cancer to definitive radiation with or without misonidazole, showed that anemic patients had poorer 3-year
Prognostic significance of pretreatment anemia
Nitroimidazole trials and anemia

36 Head and Neck Cancer
survival rates (17% vs 30%; P=0.003) compared to nonanemic patients (men Hgb > 14.5 g/dL and women > 13.5g/dL) [9]. This difference was not restricted to patients receiving misonidazole or to men with pharyngeal cancer reported in the DAHANCA II study.
• In RTOG 85-27, 521 patients with stage III/IV head and neck cancer were randomized to definitive radiation with or without etanidazole [8]. Anemia was defined as Hgb lower than 14.5 g/dL for men and lower than 13 g/dL for women. Pretreatment anemia was associated with reduced 5-year actuarial locoregional control (32% vs 48%; P=0.0003) and poorer survival (22% vs 36%; P=0.002) compared to patients with normal Hgb levels. Anemia remained a strong predictor of overall survival (P=0.0007) and locoregional control (P=0.006) after multivariate analysis. In the most recent DAHANCA study using nimorazole, more than 400 patients with pharyngeal and supraglottic laryngeal tumors were randomized to radiation with or without nimorazole [10]. In contrast to the previous nitroimidazole radiosensitizer trials, which showed no benefit of the drug, nimorazole increased loco-regional control in patients treated with conventionally fractionated radiation therapy (5-year locoregional control 49% vs 33%; P=0.002). Nimorazole increased disease-free survival (52% vs 41%; P=0.002) and trended toward improved 10-year overall survival (26% vs 16%; P=0.32) at a median follow-up time of 112 months. Anemia was prognostic of poorer 5-year locoregional control (5-year 46% vs 37%; P=0.02). Patients with pretreatment anemia (men < 14.5 g/dL and women < 13g/dL) were randomized to receive transfusion or not receive transfusion before randomization to receive the hypoxic sensitizer. Locoregional control among anemic patients receiving transfusion (n=82) was not significantly improved compared to anemic patients not receiving transfusion (n=89; 5-year locoregional control 39% vs 35%, respectively; P=0.86). However, the study sample was too small to reach definitive conclusions.
• Although not investigated as extensively as pretreatment Hgb, a decrease in Hgb levels during radiation therapy also appears to negatively affect post-radiation outcomes of patients with head and neck cancer [34,39,40]. van Acht [34] reports outcomes impacted not only by pretreatment anemia but also the absolute Hgb drop during treatment in 306 patients treated for laryngeal cancers. An Hgb drop during treatment of more than 1 mmol/L resulted in a significantly lower disease-free survival for all of the patients. For glottic laryngeal cancers, pretreatment and post-treatment were associated with poor disease-free survival, whereas in supraglottic laryngeal tumors, only post-treat-ment anemia was predictive of worse disease-free survival. The incidence of anemia did not relate to nutritional status because the incidence of more than 10% weight loss was similar in anemic versus nonanemic patients. Tarnawski et al. [40] also reported that anemia at the end of definitive radiation was found on multivariate analysis to be predictive of poorer local control for 847 patients with supraglottic laryngeal tumors. Lower post-treatment Hgb corre-lated with higher T stage, but it remained a prognostic factor after correction on multivariate analysis and was the strongest predictor of eight variables ana-lyzed, including T stage, age, sex, total radiation dose, and overall treatment time. Hgb concentration at the beginning of radiotherapy did not correlate with treatment outcome, but any decrease of Hgb during therapy was a strong prognostic factor for treatment failure. The degree of absolute Hgb drop was also prognostic, but it was not as significant as post-treatment Hgb level [40].
Prognostic significance of pretreatment versus post-treatment anemia

Radiation Treatment for Patients with Anemia Hu and Harrison 37
• Similar to cervix cancers, some physicians have argued that anemia in head and neck cancer represents a marker for advanced biologically aggressive disease, resulting possibly from tumor bleeding or cancer cachexia, and not predictive of poor outcome in this clinical setting. However, in early stage laryngeal cancer, the disease is often localized and nonbulky. There are several retrospective reports that document poor outcome. Fein et al. [33] reported on 109 patients with T1-2N0 glottic laryngeal cancers treated with definitive radiation at Fox Chase Cancer Center (Philadelphia, PA) [33]. A pretreatment Hgb of lower than 13.0 g/dL was associated with poorer 2-year locoregional control (95% vs 66%; P=0.0016 ) and 2-year survival rates (88% vs 46%; P=0.0018) compared to patients with higher pretreatment Hgb levels. Warde et al. [24] also reported poor outcome associated with pretreatment anemia in 735 patients with T1-2N0 glottic laryngeal cancers treated with definitive radiation at the Princess Margaret Hospital (Toronto, ON). Patients diagnosed with a pretreatment Hgb of lower than 12 g/dL were found through multivariate analysis to have a 1.8-fold increased risk for locoregional failure (95% confidence interval, 1.2–2.5) compared to patients with an Hgb of 15.0 g/dL. Skladowski et al. [39] also reported worse loco-regional control in 235 patients with T1N0 glottic laryngeal cancers who were anemic before definitive radiotherapy and proposed an equation to predict the impact on local control, depending on the decrement of Hgb.
• In contrast, a few studies report no correlation between local tumor control and pretreatment Hgb in patients with early stage glottic laryngeal cancers and later stage glottic laryngeal cancers [38,41–43]. However, even among these studies, low Hgb levels were associated with worse survival [38,41].
• The prognostic significance of anemia for early stage glottic laryngeal cancer is not merely a phenomenon of radiation therapy outcomes. It appears to also apply to the surgical setting [44]. In a recent study, preoperative anemia (Hgb level < 13 g/dL and < 12 g/dL in men and women, respectively) was associated with a significantly worse 5-year prognosis (60% vs 85% in patients without anemia; P=0.002) and high risk of treatment failure (relative risk 3.0) in patients with surgically treated glottic squamous cell carcinomas [44]. Furthermore, subgroup analysis of 162 male patients with T1 tumors and clean margins revealed that each 1-g/dL Hgb decrease was associated with a relative risk of locoregional relapse of 1.4 in male patients with T1 tumors. This finding suggests that Hgb may be a continuous risk factor that retains clinical relevance within the accepted range of normal [44].
• The negative prognostic finding of anemia in low-bulk localized disease treated with radiation or surgery is interesting because it suggests that anemia may be associated with more aggressive tumors and that anemia may be a poor prog-nostic factor independent of its interaction with radiation or tumor volume.
• Overall, anemia appears to be a clinically relevant risk factor in patients undergoing radiation therapy for head and neck cancers and is potentially modifiable through therapeutic interventions that increase Hgb within the normal range. Early correction of mild-to-moderate anemia in the radiation oncology setting has the potential to modify the hypoxic environment. An increase of Hgb by 20% produces a theoretic decrease in hypoxic tissue volume of approximately 30% [45].
Anemia in early-stage glottic laryngeal cancer
Anemia correction in patients with head and neck cancer

38 Head and Neck Cancer
• The clinical importance of correcting low pretreatment Hgb levels during curative radiation therapy was first identified in patients with cervical cancer treated during the early 1940s [46]. Bush et al. [30] conducted the only completed randomized trial testing the benefit of transfusion in anemic patients with cervix cancer, comparing the use of transfusions during radio-therapy to keep the Hgb level above 12.5 g/dL versus transfusion only if Hgb fell below 10. The study showed by intent to treat analysis that patients in the transfusion arm had a significant increase in pelvic control after radiotherapy. Retrospective data generally are inconclusive. Some studies suggested improved local response in patients receiving transfusions, whereas others showed no significant positive effect [27,47].
• Red blood cell transfusions were the most common therapy for cancer-related anemia until the early 1980s [48]. In some institutions, red blood cell transfusions to correct anemia are administered before radiation therapy if Hgb levels are lower than 10 g/dL and symptoms of severe anemia are present [49,50]. Blood transfusion has become a somewhat unpopular alternative among patients and healthcare providers, largely because of well-known risks (eg, HIV, hepatitis infections, acute/chronic reactions, and immunosuppres-sion), associated costs, and continuing supply deficits [51]. Furthermore, evidence linking perioperative transfusions to lower rates of survival after surgical resection of breast, lung, colorectal, or head and neck tumors merits concern and strengthens the theory that transfusions adversely affect the immunobiology of some solid tumors [50,51]. A lack of compelling evidence coupled with risks that may be problematic in patients with cancer have diminished routine transfusion of anemic patients before radiation therapy unless severe anemia is present.
• With the adventitious cloning of the erythropoietin (EPO) gene, the potential benefit in correcting anemia can be reinvestigated, while circumventing the adverse risks of transfusion. In patients treated with chemotherapy, EPO has been shown in randomized and open-label trials to improve health-related QOL (HRQOL), fatigue, and functional capacity in anemic patients with cancer and can increase Hgb levels by 1.8 g/dL to 2.0 g/dL, while decreasing the need for transfusion [52•,53,54]. Analysis of two large community-based studies show that the largest gains in HRQOL from EPO treatment occurred when Hgb levels are corrected from 11 to 12 g/dL [55]. No randomized trial has shown a survival benefit in anemic patients with cancer after receiving EPO [56]. However, a recent double-blind placebo controlled trial of 375 patients receiving chemotherapy for nonmyeloid malignancies showed that EPO (150–300 IU/kg three times a week × 12–24 weeks) not only improved QOL and decreased the need for transfusions, but it may also improve sur-vival (median survival time 17 months with epoetin alfa vs 11months with placebo; 1-year survival of 60% vs 49%; P=0.13). The trial was not powered to evaluate survival difference and larger randomized studies are ongoing.
• In most experimental and clinical studies of recombinant human erythro-poietin (rHuEPO) during radiation therapy, change in Hgb has been used as the primary endpoint. Correction of anemia with rHuEPO may improve the radiosensitivity of solid tumors [57,58]. A murine model demonstrated that EPO could overcome anemia-induced radioresistance in implanted human tumor xenografts [59]. Anemia was induced in nude mice by total body
Anemia correction with erythropoietin
Erythropoietin in anemic patients with head and neck cancer treated with radiation

Radiation Treatment for Patients with Anemia Hu and Harrison 39
radiation before human tumor cells were implanted in the hind leg. Fourteen days later, a single fraction of varying doses were delivered to the tumor to obtain a dose-response relationship for tumor cure probability. Tumors in anemic mice required a higher dose of radiation to control 50% of tumors (TCD50 [dose required to have 50% tumor control] increased from 40.1 Gy in nonanemic mice to 49.4 Gy in radiation-induced anemic mice). When EPO was administered 2 weeks before the anemia-inducing total body irradia-tion, anemia was prevented and the TCD50 was restored to 39.8 Gy, thus over-coming the radioresistance present in anemic mice [59].
• Several phase I/II clinical trials have evaluated the effects of rHuEPO on Hgb levels in patients with cancer with documented anemia at the initiation of radiation therapy (Table 2) [49,57,60]. In the first published study, 80% and 5% of patients treated with rHuEPO or oral iron therapy, respectively, achieved the target Hgb of 14 g/dL during continuous radiation therapy (P < 0.001) [49]. The beneficial therapeutic effects of rHuEPO in improving Hgb levels during radiation therapy were confirmed in subsequent studies that used alternative weight-based dosing schedules, enrolled patients with a variety of primary tumor types, and included various radiation regimens [57,60,61]. Overall, hematopoietic responses to rHuEPO in these studies were rapid and pronounced (mean overall Hgb increase 1.5–3.9 g/dL), with excellent tolerance during the study periods [49,57,60,61]. rHuEPO is approved for patients with nonmyeloid malignancy who are experiencing chemotherapy-induced anemia, whether patients are receiving radiation therapy. However, the use of rHuEPO to correct anemia specifically in patients receiving radiation therapy is under investigation [62].
• Phase II studies have evaluated the prophylactic use of rHuEPO during chemoradiation regimens expected to produce high rates of anemia in patients with head and neck cancer [63–65]. In a pilot study of rHuEPO in patients with head and neck cancer undergoing radiation therapy, loco-regional tumor control was improved in patients achieving a rapid rise in Hgb [57]. Researchers from Northwestern University (Evanston, IL) evaluated an 18-week course of once-weekly rHuEPO 40,000 U with oral iron in patients receiving five cycles of chemoradiation (5-fluorouracil, paclitaxel, hydroxy-urea, and hyperfractionated radiation) for locally advanced head and neck cancer. Patients randomized to EPO experienced less grade 2/3 anemia (52% vs 77%; P=0.02), but transfusion requirements were not significantly different [17•]. A prospective study is evaluating the benefits of rHuEPO during combined modality therapy in patients with oral squamous cell carcinoma (Table 3) [64,65,66••]. All 191 patients in this study received a regimen consisting of mitomycin C (15 mg/m2 on day 1), 5-fluorouracil (750 mg/m2 on days 1–5), and radiotherapy (50 Gy in 25 fractions during weeks 1–5), followed by dissection of the primary site and a neck dissection. Epoetin alfa (10,000 IU/kg subcutaneously three to six times per week until the week of surgery) was administered to a group of patients (n=57) who had a pretreat-ment Hgb level lower than 14.5 g/dL. The outcome in this group of patients was compared with the outcomes in two other groups treated with this approach during an earlier period when EPO was not routinely used. One of these non–epoetin-alfa groups had a pretreatment Hgb level lower than 14.5 g/dL (n=87) and the other group had a pretreatment Hgb level higher than 14.5 g/dL (n=43). The results are summarized in Table 3. In the two groups of patients who did not receive epoetin alfa, patients with a low pretreatment Hgb level (< 14.5g/dL; group 2) exhibited significantly lower complete response rates, 2-year locoregional rates (72% vs 87%; P < 0.05), and 2-year survival rates (60% vs 81%; P < 0.05) compared to patients who had normal Hgb levels (> 14.5 g/dL; group 1). However, in the patients with a low pre-treatment Hgb level who received epoetin alfa (group 3), the rates of complete

40 Head and Neck Cancer
Tabl
e 2.
Pha
se I
/II
stud
ies
of r
ecom
bina
nt h
uman
ery
thro
poie
tin
for
anem
ia in
pat
ient
s un
derg
oing
rad
iati
on t
hera
py
Mea
n H
gb, g
/dL
Stud
y Pa
tien
t po
pula
tion
Trea
tmen
t gr
oups
Base
line
Fina
lCh
ange
(%
)P
valu
e*
Hen
ke e
t al
. [5
7];
phas
e I
Hea
d/ne
ck o
r pe
lvic
can
cer;
Hgb
= 9
.5–1
3 g/
dL;
cura
tive
-int
ent
prim
ary
defini
tive
RT
(2 G
y/FR
× 5
FR/
wk;
tot
al d
ose
60–7
0 Gy
) or
RT
/sur
gery
10–1
4 d
befo
re R
T: in
itia
te r
HuE
PO a
nd c
onti
nue
unti
l tar
get
Hgb
leve
ls a
re r
each
ed†‡
§
150
U/k
g IV
TIW
(n=
19)
10.9
14.1
3.2
(29)
< 0.
0001
300
U/k
g IV
TIW
(n=
14)
11.4
14.9
3.5
(31)
< 0.
0001
150
U/k
g SC
TIW
(n=
6)11
.515
.43.
9 (3
4)<
0.00
01Co
ntro
l (IV
iron
onl
y; n
=11)
12.3
12.9
0.6
(5)
Swee
ney
et a
l. [6
0];
phas
e II
Lung
, cer
vix,
pro
stat
e, o
r br
east
can
cer;
Hgb
≤ 1
3 g/
dL (
men
) or
≤ 12
g/d
L (w
omen
); R
T fo
r ≥
4 w
k (d
ose/
sche
dule
det
erm
ined
by
the
site
and
st
age
of d
isea
se)
± CT
14 d
bef
ore
RT (
whe
n po
ssib
le):
init
iate
rHuE
PO 2
00
U/k
g SC
fiv
e ti
mes
wee
kly
and
cont
inue
unt
il ta
rget
Hgb
leve
ls a
re r
each
ed (
n=24
)द
12.1
13.6
1.5
(12)
0.00
12
Cont
rol (
no r
HuE
PO o
r iro
n th
erap
y; n
=24)
10.7
110.
3 (3
)Du
senb
ery
et a
l. [6
1];
phas
e I/
IIIn
vasi
ve c
ervi
cal c
ance
r; H
gb <
12.
5 g/
dL;
EBRT
(1.
75 G
y/FR
) pl
us t
wo
intr
acav
itar
y br
achy
ther
apy
appl
icat
ions
± c
ispl
atin
5–10
d b
efor
e RT
: in
itia
te r
HuE
PO 2
00 U
/kg/
d SC
×
10 d
(M
onda
y–Fr
iday
), f
ollo
wed
by
200
U/k
g TI
W;
cont
inue
unt
il H
gb le
vels
are
> 1
4 g/
dL o
r RT
is
com
plet
ed (
n=15
)‡¶
10.3
13.2
2.9
(28)
NR
Stud
y co
ntro
l (Fe
SO4
325
mg
oral
ly T
ID;
n=5)
10.7
10.4
-0.3
(-3
)La
vey
[63]
; ph
ase
I/II
Canc
er (
abov
e di
aphr
agm
) w
ith
no d
ista
nt
met
asta
ses;
Hgb
< 1
3.5
g/dL
; con
tinu
ous
RT fo
r 5–
8 w
k w
itho
ut c
oncu
rren
t CT
0–10
d b
efor
e RT
: ini
tiat
e rH
uEPO
300
mg/
kg S
C TI
W
× 1
wk,
fol
low
ed b
y 15
0 U
/kg
TIW
unt
il H
gb >
15
g/dL
or
RT c
ompl
eted
(n=
20)¶
11.9
15.1
3.2
(27)
< 0.
001
Cont
rol (
FeSO
4 32
5 m
g or
ally
TID
; n=
20)
11.8
11.8
0 (0
)
* rH
uEPO
ver
sus
cont
rol g
roup
s.† I
ron-
III-
sacc
hara
te a
dmin
iste
red
intr
aven
ousl
y ov
er 3
0 m
inut
es o
n th
e fi
rst
day
of t
reat
men
t an
d re
peat
ed w
hen
iron
depl
etio
n w
as d
ocum
ente
d.‡ D
osag
e re
gim
en w
as a
djus
ted
once
the
tar
get
leve
l was
rea
ched
.§ T
arge
t he
mog
lobi
n le
vels
wer
e 15
g/d
L an
d 14
g/d
L fo
r m
en a
nd w
omen
, re
spec
tive
ly.
¶Su
pple
men
tal i
ron
adm
inis
tere
d (F
eSO4
350
mg
oral
ly T
ID)
thro
ugho
ut t
he s
tudy
.CT
—ch
emot
hera
py;
EBRT
—ex
tern
al b
eam
rad
iati
on t
hera
py;
FeSO
4—fe
rrou
s su
lfate
; FR
—fr
acti
on;
Hgb
—he
mog
lobi
n; I
V—in
trav
enou
sly;
NR—
not
repo
rted
; rH
uEPO
—re
com
bina
nt h
uman
er
ythr
opoi
etin
; RT
—ra
diat
ion
ther
apy;
SC—
subc
utan
eous
ly;
TID—
thre
e ti
mes
dai
ly;
TIW
—th
ree
tim
es w
eekl
y.

Radiation Treatment for Patients with Anemia Hu and Harrison 41
response, 2-year locoregional control (95% vs 87%; P=nonsignificant), and 2-year survival (88% vs 81%; P=nonsignificant) were equivalent to or higher than the rates in patients with normal pretreatment Hgb levels who did not receive EPO (group 1) [66••].
• These findings suggest that epoetin alfa is an effective and well-tolerated means of achieving normal Hgb levels in patients undergoing radiotherapy and may reverse the negative prognostic influence of a low pretreatment Hgb level.
• An ongoing RTOG phase III study (RTOG 99-03) will provide prospective data concerning the effects of rHuEPO on locoregional control as a primary endpoint and survival, in addition to QOL as secondary endpoints in patients with head and neck squamous cell carcinoma with pretreatment anemia [67]. Patients with all stages of head and neck cancer treated with definitive radiation or chemoradiation are included.
• Henke et al. [68] reported the results of the first multicenter double-blind study testing the effect of EPO-beta in 351 anemic patients with head and neck cancer treated with postoperative radiation (78% of all patients) or definitive radiotherapy. Patients were stratified by tumor site, sex, age, stage, recurrent versus primary presentation, resection status, and degree of anemia. EPO was administered on a standard dosing schedule (300 IU/kg three times a week). Patients in the EPO arm did show an improvement in Hgb compared to placebo (anemia was corrected in 82% of patients vs 15%). By intent-to-treat analysis, patients in the EPO group had a statisti-cally significant higher risk for locoregional failure (relative risk [RR] = 1.62 [1.22–2.14; P=0.0008]), worse locoregional failure progression free-survival (RR = 1.69 [1.16–2.47; P=0.007]), and poorer overall survival (RR = 1.39 [1.05–1.84; P=0.02]) compared to placebo. There was no difference in rate of distant metastases. However, when 31% (109 of 351) of entered patients are excluded because of protocol violations, the impact of EPO on locore-gional failure and overall survival no longer is significant in the patients who were treated according to protocol.
• The results are concerning and raise the issue of whether EPO can be tumor protective or even serve as a growth factor for tumor proliferation. Do anemic patients with head and neck cancer have a worse outcome not because they are hypoxic, but because the anemia stimulates EPO production, which enhances clonogenic survival/proliferation of the tumor? These are certainly possibilities that warrant thorough investigation.
• However, in raising these issues, physicians must critically analyze the study to ensure that we do not prematurely dismiss a potentially beneficial treatment. Several issues are of concern. For example, the negative influence of EPO on
Table 3. Effects of recombinant human erythropoietin on the efficacy of neoadjuvant chemoradiation (mitomycin C, 5-fluorouracil, and fractionated radiation) in oral squamous cell carcinoma
Patients, %Outcome rHuEPO (n=57) Control (n=87)* P value
Overall CR 61 17 < 0.01CR of T2/T3 primary tumors 70 31 < 0.01CR of T4 primary tumors 62 19 < 0.01CR of N1-3 neck tumors 83 59 < 0.012-year actuarial locoregional control 95 72 > 0.052-year survival 93 62 < 0.01
*Patients with baseline anemia who did not undergo rHuEPO therapy.CR—complete response; rHuEPO—recombinant human erythropoietin.

42 Head and Neck Cancer
locoregional control and survival was particularly evident for patients with hypopharyngeal cancer. However, despite stratification, patients with hypopharyngeal cancer in the EPO arm had worse baseline characteristics compared to the placebo group, including a greater percentage of smokers (40% vs 55%), more patients who presented with relapse (15% vs 7%), and more patients with stage IV disease (85% vs 70%). The poorer outcome in patients with hypopharyngeal cancer may have been attributed to this imbal-ance. With regard to smoking, there was an imbalance for all patients because there were more current smokers in the EPO arm (66% vs 53%) compared to the placebo group. Smoking impairs the efficacy of radiation and should have been a stratification variable. Because of these two examples, it is possible the patient population was too heterogenous to achieve a proper balance between the study arms. Furthermore, because more than 50% of patients in the con-trol arm and two of three patients in the EPO arm were current smokers, the issue of whether the impact of EPO in potentially correcting tumor hypoxia by raising Hgb levels and enhancing radiosensitization would have been abro-gated by smoking. Another issue is that the negative impact of EPO on locore-gional control was significant only on univariate analysis, but no mention was made of its significance on multivariate analysis. Because of the heterogenous patient population and the possible imbalance in baseline characteristics, this analysis is the only way to control against these confounding factors. With regard to treatment, did any patients receive concurrent chemotherapy and was this done consistently for patients in either treatment arm? Was the time interval between surgery and the end of radiation similar in patients receiving postoperative radiation in the two arms because this is an important variable affecting locoregional control? Was the median follow-up time similar between the groups and was it an adequate amount of time? Because the negative influence of EPO on locoregional failure and survival loses statistical significance in patients treated according to protocol, more patients were needed to solidify the authors’ conclusion.
• The results of the paper are thought provoking and emphasize the impor-tance of clarifying the issue of anemia in head and neck cancer. The authors conclude that their study suggests that EPO may impair cancer control, but it needs further study. Whether EPO is beneficial or detrimental needs to be accurately determined, so that whatever its impact, important insights into tumor biology of head and neck cancer may be realized to create an opportunity for better targeted therapy.
• There is a continued need for targeted and feasible strategies that improve locoregional tumor control, survival, and QOL after curative-intent radiation therapy. Early correction of anemia can be readily achieved with minimal added toxicity and it is an approach that has not been fully investigated by the radiation oncology community. Anemia is a problem that affects a large percentage of patients with head and neck cancer. Low preradiation Hgb, even when ranging from 12 to 14 g/dL, poses a substantial risk of poor locoregional control and survival. A direct association between anemia and tumor hypoxia appears likely, but it needs to be better characterized through additional preclinical and clinical studies. The threshold for Hgb level versus outcome may vary across different tumor sites, making an exact definition of anemia or hypoxia difficult. The definitions may vary from tumor to tumor or from patient to patient, thus our clinically defined thresholds may serve as guidelines rather than firm definitions (ie, the hematologic definition of ane-mia may not necessarily be the oncologic definition). Within defined limits,
Conclusions

Radiation Treatment for Patients with Anemia Hu and Harrison 43
rHuEPO has the ability to correct Hgb levels rapidly, simply, and safely during a course of chemoradiation or radiation, although it has not been approved for patients with cancer receiving radiation therapy alone. Transfusions may also be useful, especially for patients with low Hgb levels (ie, < 10 g/dL), but they are more costly and less desirable compared to sim-pler methods. Ongoing studies are expected to elucidate the effects of rHuEPO. Overall, surgeons, medical oncologists, and radiation oncologists should view pretreatment anemia as potentially modifiable risk factors for poor outcomes and as an opportunity to explore strategies to overcome this problem and improve results.
References and Recommended ReadingPapers of particular interest, published recently, have been highlighted as:• Of importance•• Of major importance
1. Mundt AJ, Connell PP, Campbell T, et al.: Race and clinical outcome in patients with carcinoma of the uterine cervix treated with radiation therapy. Gynecol Oncol 1998, 71:151–158.
2. Takeshi K, Katsuyuki K, Yoshiaki T, et al.: Definitive radiotherapy combined with high-dose-rate brachy-therapy for stage III carcinoma of the uterine cervix: retrospective analysis of prognostic factors concern-ing patient characteristics and treatment parameters. Int J Radiat Oncol Biol Phys 1998, 41:319–327.
3. Forastiere AA, Berkey B, Maor M, et al.: Phase III trial to preserve the larynx: induction chemotherapy and radiotherapy versus concomitant chemoradiotherapy versus radiotherapy alone. Intergroup trial R91-11. Proc Am Soc Clin Oncol 2001, 20:2a.
4. Teicher BA: Physiologic mechanisms of therapeutic resistance: blood flow and hypoxia. Hematol Oncol Clin North Am 1995, 9:475–506.
5.• Harrison LB, Shasha D, Homel P: Prevalence of anemia in cancer patients undergoing radiotherapy: prognostic significance and treatment. Oncology 2002, 63(Suppl 2):11–18.
This paper discusses the incidence of anemia in a wide cross-section of patients treated with radiotherapy.6. Hu K, Nwokeoi E, Culliney B, et al.: Delayed accelerated
hyperfractionated radiation with concurrent cis-plati-num without induction chemotherapy for organ pres-ervation therapy of stage III/IV head and neck cancer. Radiother Oncol 2002, 64(Suppl 1):S251.
7. Hu K, Sachoeva G, Culliney B, et al.: Accelerated frac-tionated radiation by concomitant boost (AFX-CB) with concurrent cis-platinum for advanced nasopha-ryngeal cancer. Paper presented at the 85th Annual Meet-ing of the American Radium Society. Chicago, IL; 2003.
8. Lee DJ, Cosmatos D, Marcial VA, et al.: Results of an RTOG phase III trial (RTOG 85-27) comparing radio-therapy plus etanidazole with radiotherapy alone for locally advanced head and neck carcinomas. Int J Radiat Oncol Biol Phys 1995, 32:567–576.
9. Fazekas JT, Scott C, Marcial V, et al.: The role of hemo-globin concentration in the outcome of misonida-zole-sensitized radiotherapy of head and neck cancers: based on RTOG trial #79-15. Int J Radiat Oncol Biol Phys 1989, 17:1177–1181.
10. Overgaard J, Hansen HS, Overgaard M, et al.: A random-ized double-blind phase III study of nimorazole as a hypoxic radiosensitizer of primary radiotherapy in supraglottic larynx and pharynx carcinoma: results of the Danish Head and Neck Cancer Study (DAHANCA) Protocol 5-85. Radiother Oncol 1998, 46:135–146.
11. Dubray B, Mosseri V, Brunin F, et al.: Anemia is associ-ated with lower local-regional control and survival after radiation therapy for head and neck cancer: a prospective study. Radiology 1996, 201:553–558.
12. Al-Sarraf M, LeBlanc M, Giri PG, et al.: Chemoradiother-apy versus radiotherapy in patients with advanced nasopharyngeal cancer: phase III randomized Inter-group study 0099. J Clin Oncol 1998, 16:1310–1317.
13. Calais G, Alfonsi M, Bordet E, et al.: Radiation (RT) alone versus RT with concomitant chemotherapy (CT) in stages III and IV oropharynx carcinoma: final results of the 94-01 GORTEC randomized study. Int J Radiat Oncol Biol Phys 2001, 51(Suppl 1):1.
14. Munro AJ: An overview of randomised controlled trials of adjuvant chemotherapy in head and neck cancer. Br J Cancer 1995, 71:83–91.
15. El-Sayed S, Nelson N: Adjuvant and adjunctive chemo-therapy in the management of squamous cell carci-noma of the head and neck region: a meta-analysis of prospective and randomized trials. J Clin Oncol 1996, 14:838–847.
16. Bourhis J, Eschwege F: Radiotherapy-chemotherapy combinations in head and neck squamous cell carci-noma: overview of randomized trials. Anticancer Res 1996, 16:2397–2402.

44 Head and Neck Cancer
17.• Rosen FR, Haraf DJ, Kies MS, et al.: Multicenter ran-domized phase II study of paclitaxel (1-hour infu-sion), fluorouracil, hydroxyurea, and concomitant twice daily radiation with or without erythropoietin for advanced head and neck cancer. Clin Cancer Res 2003, 9:1689–1697.
A randomized study evaluating whether EPO impacts QOL/transfusion requirements in patients with head and neck cancer treated with chemoradiation.18. Stadler P, Feldmann HJ, Creighton C, et al.: Changes in
tumor oxygenation during combined treatment with split-course radiotherapy and chemotherapy in patients with head and neck cancer. Radiother Oncol 1998, 48:157–164.
19. Hockel M, et al.: Tumor oxygenation: a new predictive parameter in locally advanced cancer of the uterine cervix. Gynecol Oncol 1993, 51:141–149.
20. Becker A, Hansgen G, Richter C, Dunst J: Oxygenation status of squamous cell carcinoma of the head and neck: comparison of primary tumors, their neck node metastases and normal tissue. Strahlenther Onkol 1998, 174:484–486.
21. Brizel DM, Dodge RK, Clough RW, Dewhirst MW: Oxygenation of head and neck cancer: changes during radiotherapy and impact on treatment outcome. Radiother Oncol 1999, 53:113–117.
22. Nordsmark M, Overgaard J: A confirmatory prognostic study on oxygenation status and loco-regional control in advanced head and neck squamous cell carcinoma treated by radiation therapy. Radiother Oncol 2000, 57:39–43.
23. Hirst DG: What is the importance of anaemia in radio-therapy? The value of animal studies. Radiother Oncol 1991, 20(Suppl 1):29–33.
24. Warde P, O’Sullivan B, Bristow RG, et al.: T1/T2 glottic cancer managed by external beam radiotherapy: the influence of pretreatment hemoglobin on local control. Int J Radiat Oncol Biol Phys 1998, 41:347–353.
25. Hirst DG: Anemia: a problem or an opportunity in radiotherapy? Int J Radiat Oncol Biol Phys 1986, 12:2009–2017.
26. Rockwell S, Keyes SR, Sartorelli AC: Modulation of the antineoplastic efficacy of mitomycin C by dicoumarol in vivo. Cancer Chemother Pharmacol 1989, 24:349–353.
27. Overgaard J, Horsman MR: Modification of hypoxia-induced radioresistance in tumors by the use of oxy-gen and sensitizers. Semin Radiat Oncol 1996, 6:10–21.
28. Stadler P, Becker A, Feldmann HJ, et al.: Influence of the hypoxic subvolume on the survival of patients with head and neck cancer. Int J Radiat Oncol Biol Phys 1999, 44:749–754.
29. Overgaard J: Sensitization of hypoxic tumour cells: clinical experience. Int J Radiat Biol 1989, 56:801–811.
30. Bush RS, Jenkin RD, Allt WE, et al.: Definitive evidence for hypoxic cells influencing cure in cancer therapy. Br J Cancer Suppl 1978, 37:302–306.
31. Bush RS: The significance of anemia in clinical radiation therapy. Int J Radiat Oncol Biol Phys 1986, 12:2047–2050.
32. Harrison LB, Chadha M, Hill RJ, et al.: Impact of tumor hypoxia and anemia on radiation therapy outcomes. Oncologist 2002, 7:492–508.
33. Fein DA, Lee WR, Hanlon AL, et al.: Pretreatment hemoglobin level influences local control and sur-vival of T1-T2 squamous cell carcinomas of the glottic larynx. J Clin Oncol 1995, 13:2077–2083.
34. van Acht MJ, Hermans J, Boks DE, Leer JW: The prog-nostic value of hemoglobin and a decrease in hemo-globin during radiotherapy in laryngeal carcinoma. Radiother Oncol 1992, 23:229–235.
35. Grant DG, Hussain A, Hurman D: Pre-treatment anaemia alters outcome in early squamous cell carcinoma of the larynx treated by radical radiotherapy. J Laryngol Otol 1999, 113:829–833.
36. Blitzer P, Wang C, Suit H: Blood pressure and hemo-globin concentration: multivariate analysis of local control after irradiation for head and neck cancer. Int J Radiat Oncol Biol Phys 1984, 10(Suppl 2):98.
37. Haddad R, Suntharalingam M, Chen T, et al.: Pretreatment hemoglobin is associated with response to chemo-radiation therapy (CRT) in patients with advanced unresectable squamous cell carcinoma of the head and neck. Proc Am Soc Clin Oncol 2001, 19:417a.
38. Overgaard J, Hansen HS, Andersen AP, et al.: Misonida-zole combined with split-course radiotherapy in the treatment of invasive carcinoma of larynx and phar-ynx: report from the DAHANCA 2 study. Int J Radiat Oncol Biol Phys 1989, 16:1065–1068.
39. Skladowski K, Tarnawski R, Maciejewski B, et al.: Clini-cal radiobiology of glottic T1 squamous cell carci-noma. Int J Radiat Oncol Biol Phys 1999, 43:101–106.
40. Tarnawski R, Skladowski K, Maciejewski B: Prognostic value of hemoglobin concentration in radiotherapy for cancer of supraglottic larynx. Int J Radiat Oncol Biol Phys 1997, 38:1007–1011.
41. Canaday DJ, Regine WF, Mohiuddin, et al.: Significance of pretreatment hemoglobin level in patients with T1 glottic cancer. Radiat Oncol Investig 1999, 7:42–48.
42. Tucker J, Hixson W, Kim R: Pretreatment hemoglobin in early stage glottic cancer: red flag or red herring? Int J Oncol Biol Phys Proc 1996, 36:336.
43. Sakata K, Aoki Y, Karasawa K, et al.: Radiation therapy in early glottic carcinoma: uni-and multivariate analy-sis of prognostic factors affecting local control. Int J Radiat Oncol Biol Phys 1994, 30:1059–1064.
44. Lutterbach J, Guttenberger R: Anemia is associated with decreased local control of surgically treated squa-mous cell carcinomas of the glottic larynx. Int J Radiat Oncol Biol Phys 2000, 48:1345–1350.
45. Degner FL, Sutherland RM: Mathematical modelling of oxygen supply and oxygenation in tumor tissues: prognostic, therapeutic, and experimental implica-tions. Int J Radiat Oncol Biol Phys 1988, 15:391–397.
46. Evans SM, Jenkins WT, Shapiro M, Koch CJ: Evaluation of the concept of “hypoxic fraction” as a descriptor of tumor oxygenation status. Adv Exp Med Biol 1997, 411:215–225.
47. Girinski T, Pejovic-Lenfant MH, Bourhis J, et al.: Prognostic value of hemoglobin concentrations and blood transfusions in advanced carcinoma of the cervix treated by radiation therapy: results of a retrospective study of 386 patients. Int J Radiat Oncol Biol Phys 1989, 16:37–42.

Radiation Treatment for Patients with Anemia Hu and Harrison 45
48. Surgenor DM, Wallace EL, Hao SH, Chapman RH: Collection and transfusion of blood in the United States, 1982-1988. N Engl J Med 1990, 322:1646–1651.
49. Lavey RS, Dempsey WH: Erythropoietin increases hemoglobin in cancer patients during radiation ther-apy. Int J Radiat Oncol Biol Phys 1993, 27:1147–1152.
50. Pedersen D, Sogaard H, Overgaard J: Prognostic value of pretreatment factors in patients with locally advanced carcinoma of the uterine cervix treated by radiotherapy alone. Acta Oncol 1995, 34:787–795.
51. Henry DH: Changing patterns of care in the manage-ment of anemia. Semin Oncol 1992, 19(Suppl 8):3–7.
52.• Littlewood TJ, Bajetta E, Nortier JW, et al.: Effects of epo-etin alfa on hematologic parameters and quality of life in cancer patients receiving nonplatinum chemo-therapy: results of a randomized, double-blind, pla-cebo-controlled trial. J Clin Oncol 2001, 19:2865–2874.
This paper demonstrates that EPO can improve QOL in patients treated with chemotherapy. It showed a trend toward improved survival in patients receiving EPO.53. Quirt I, Robeson C, Lau CY, et al.: Epoetin alpha ther-
apy increases hemoglobin levels and improves quality of life in patients with cancer-related anemia who are not receiving chemotherapy and patients with anemia who are receiving chemotherapy. J Clin Oncol 2001, 19:4126–4134.
54. Gabrilove J, Cleeland CS, Livingston RB, et al.: Clinical evaluation of once-weekly dosing of epoetin alpha in chemotherapy patients: improvements in hemoglobin and quality of life are similar to three-times-weekly dosing. J Clin Oncol 2001, 19:2875–2882.
55. Cleeland C, Demetti G, Glaspy J, et al.: Identifying hemoglobin level for optimal quality of life: results of an incremental analysis. Proc Am Soc Clin Oncol 1999, 18:574a.
56. Cella D, Dobrez D, Glaspy J: Control of cancer-related anemia with erythropoietic agents: a review of evidence for improved quality of life and clinical outcomes. Ann Oncol 2003, 14:511–519.
57. Henke M, Guttenberger R, Barke A, et al.: Erythropoi-etin for patients undergoing radiotherapy: a pilot study. Radiother Oncol 1999, 50:185–190.
58. Thews O, Koenig R, Kelleher DK, et al.: Enhanced radiosensitivity in experimental tumours following erythropoietin treatment of chemotherapy-induced anaemia. Br J Cancer 1998, 78:752–756.
59. Stuben G, Pottgen C, Knuhmann K, et al.: Erythropoietin restores the anemia-induced reduction in radiosensitiv-ity of experimental human tumors in nude mice. Int J Radiat Oncol Biol Phys 2003, 55:1358–1362.
60. Sweeney PJ, Nicolae D, Ignacio L, et al.: Effect of subcu-taneous recombinant human erythropoietin in cancer patients receiving radiotherapy: final report of a ran-domized, open-labelled, phase II trial. Br J Cancer 1998, 77:1996–2002.
61. Dusenbery K, McGuire WA, Holt PJ, et al.: Erythropoi-etin increases hemoglobin during radiation therapy for cervical cancer. Int J Radiat Oncol Biol Phys 1994, 29:1079–1084.
62. Shasha D, George MJ, Harrison LB: Once-weekly dosing of epoetin-alpha increases hemoglobin and improves quality of life in anemic cancer patients receiving radiation therapy either concomitantly or sequentially with chemotherapy. Cancer 2003, 98:1072–1079.
63. Lavey RS: Clinical trial experience using erythropoi-etin during radiation therapy. Strahlenther Onkol 1998, 174(Suppl 4):24–30.
64. Glaser C, Millesi W, Gossweiner S, et al.: rHuEPO sup-ply increases efficacy of neoadjuvant radiochemother-apy in patients with oral squamous cell carcinoma. Proc Am Soc Clin Oncol 1998, 17:397a.
65. Glaser C, Millesi W, Wanschitz F, et al.: rHuEPO treat-ment increases efficacy of neoadjuvant radiochemo-therapy and improves cancer free survival of patients with oral squamous cell carcinoma: a 17-month fol-low-up. Proc Am Soc Clin Oncol 1999, 18:399a.
66.••Glaser CM, Millesi W, Kornek GV, et al.: Impact of hemoglobin level and use of recombinant erythropoi-etin on efficacy of preoperative chemoradiation ther-apy for squamous cell carcinoma of the oral cavity and oropharynx. Int J Radiat Oncol Biol Phys 2001, 50:705–715.
An important paper that shows that the use of EPO to correct anemia in patients with head and neck cancer treated with multimodality therapy appears to improve locoregional con-trol and survival outcomes.67. Machtay M: A randomized phase III trial to assess the
effect of erythropoietin on local-regional control in anemic patients treated with radiotherapy for carci-noma of the head and neck. RTOG 99-03. Radiat Ther Oncol Group 2000.
68. Henke M, Laszig R, Rube C, et al.: Erythropoietin to treat head and neck cancer patients with anaemia undergoing radiotherapy: randomised, double-blind, placebo-controlled trial. Lancet 2003, 362:1255–1260.