Embed Size (px)
Citation preview
IMMUNOTHERAPY OF MELANOMA
Anti PD1 Takes Center Stage
Dr Peter Hersey
Professor of Melanoma Biology
University of Sydney
What we have learnt about immunotherapy over the past 3
years
Inhibition of Physiologic Checkpoints is a more effective form of therapy than stimulation of the immune system
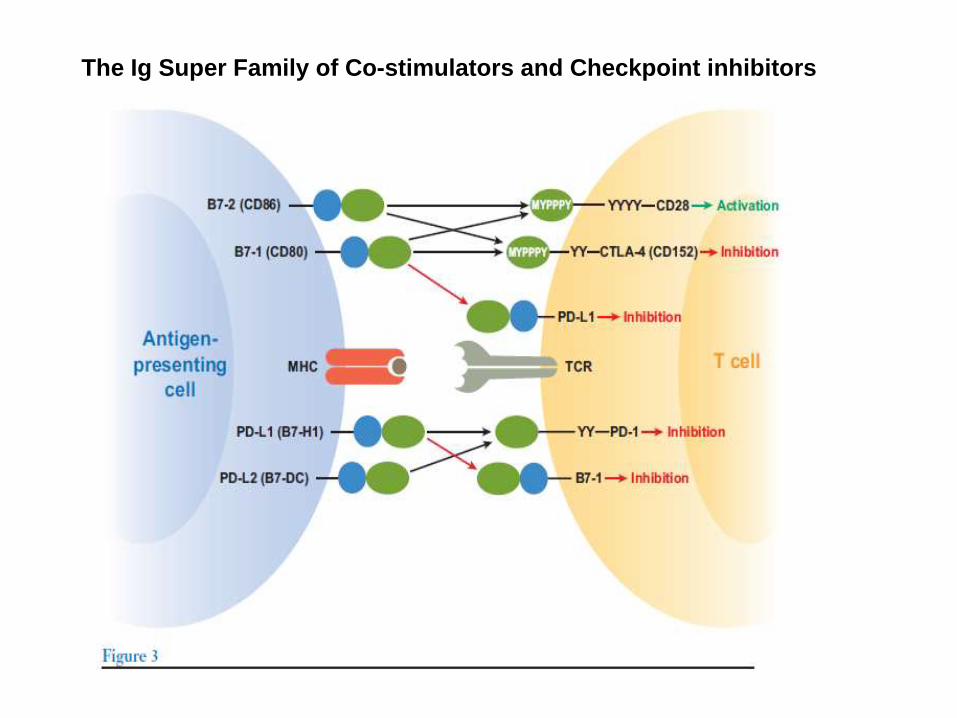
The Ig Super Family of Co-stimulators and Checkpoint inhibitors
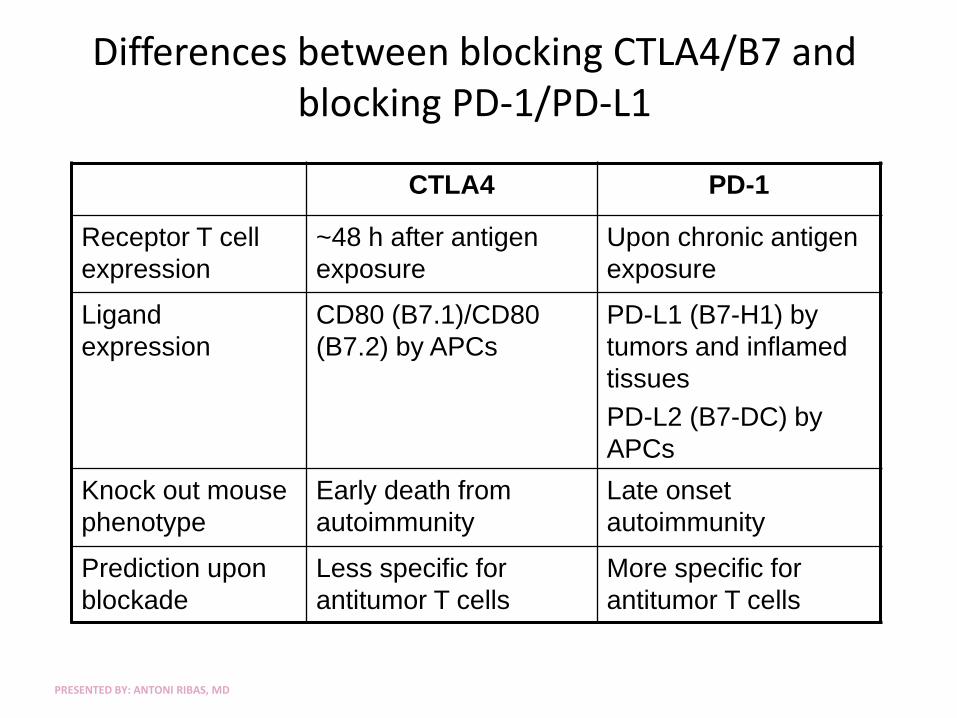
Differences between blocking CTLA4/B7 and blocking PD-1/PD-L1
CTLA4 PD-1
Receptor T cell
expression
~48 h after antigen
exposure
Upon chronic antigen
exposure
Ligand
expression
CD80 (B7.1)/CD80
(B7.2) by APCs
PD-L1 (B7-H1) by
tumors and inflamed
tissues
PD-L2 (B7-DC) by
APCs
Knock out mouse
phenotype
Early death from
autoimmunity
Late onset
autoimmunity
Prediction upon
blockade
Less specific for
antitumor T cells
More specific for
antitumor T cells
PRESENTED BY: ANTONI RIBAS, MD
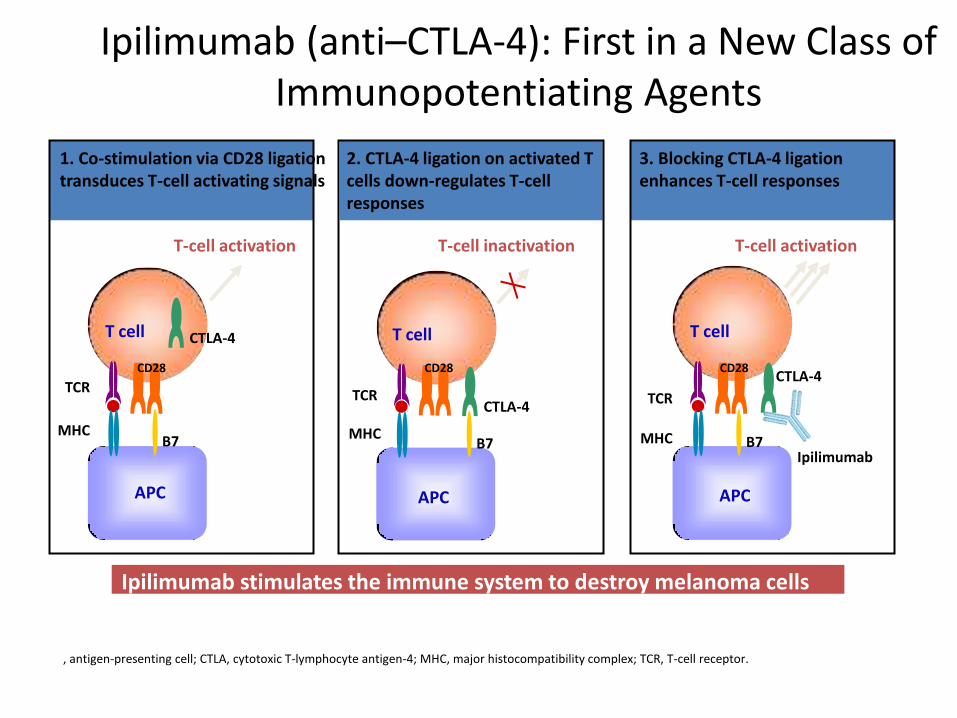
1. Co-stimulation via CD28 ligation transduces T-cell activating signals
MHC
TCR
3. Blocking CTLA-4 ligation enhances T-cell responses
MHC
TCR
T cell
APC
CD28
CTLA-4
T-cell inactivation
B7
2. CTLA-4 ligation on activated T cells down-regulates T-cell responses
MHC
TCR
T cell CTLA-4
APC
B7
T-cell activation
CD28
Ipilimumab
T cell
CTLA-4
APC
T-cell activation
B7
CD28
Ipilimumab (anti–CTLA-4): First in a New Class of Immunopotentiating Agents
Ipilimumab stimulates the immune system to destroy melanoma cells
APC, antigen-presenting cell; CTLA, cytotoxic T-lymphocyte antigen-4; MHC, major histocompatibility complex; TCR, T-cell receptor.
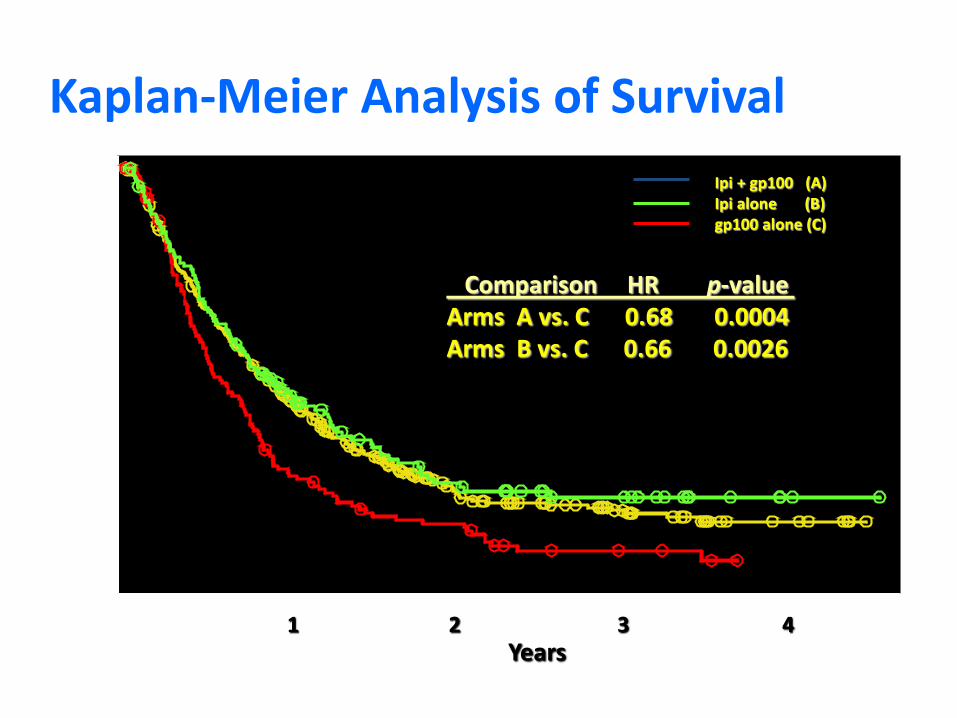
Kaplan-Meier Analysis of Survival Ipi + gp100 (A) Ipi alone (B) gp100 alone (C)
1 2 3 4 Years
Comparison HR p-value Arms A vs. C 0.68 0.0004 Arms B vs. C 0.66 0.0026
Pr
op
or
ti
on
Al
iv
e
0. 0
0. 1
0. 2
0. 3
0. 4
0. 5
0. 6
0. 7
0. 8
0. 9
1. 0
Years
0 1 2 3 4
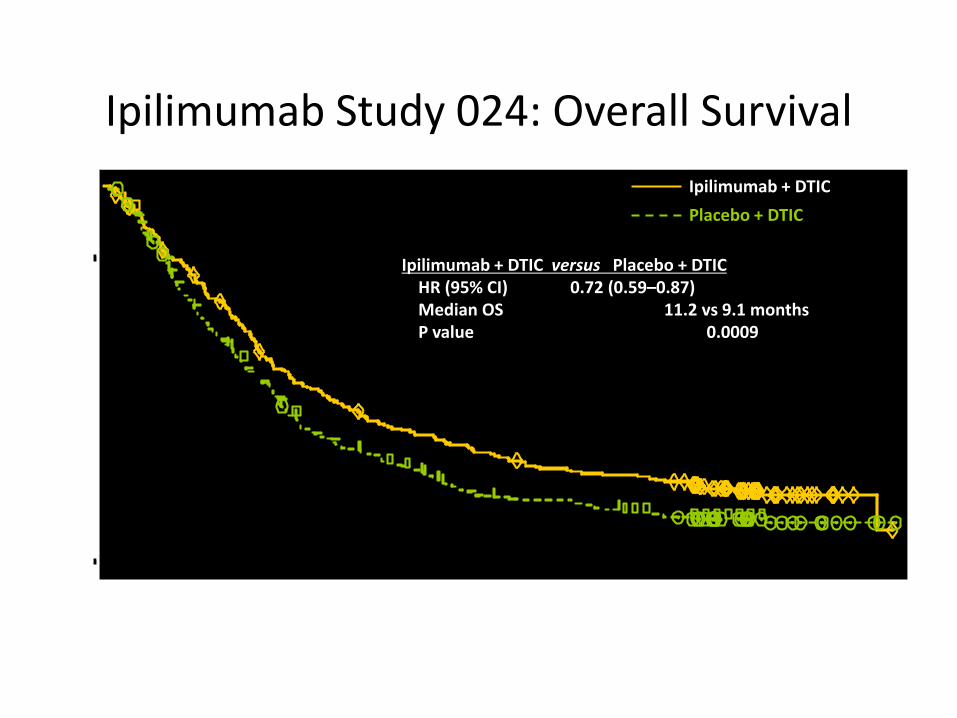
Ipilimumab Study 024: Overall Survival
Ipilimumab + DTIC versus Placebo + DTIC HR (95% CI) 0.72 (0.59–0.87) Median OS 11.2 vs 9.1 months P value 0.0009
Ipilimumab + DTIC
Placebo + DTIC
8
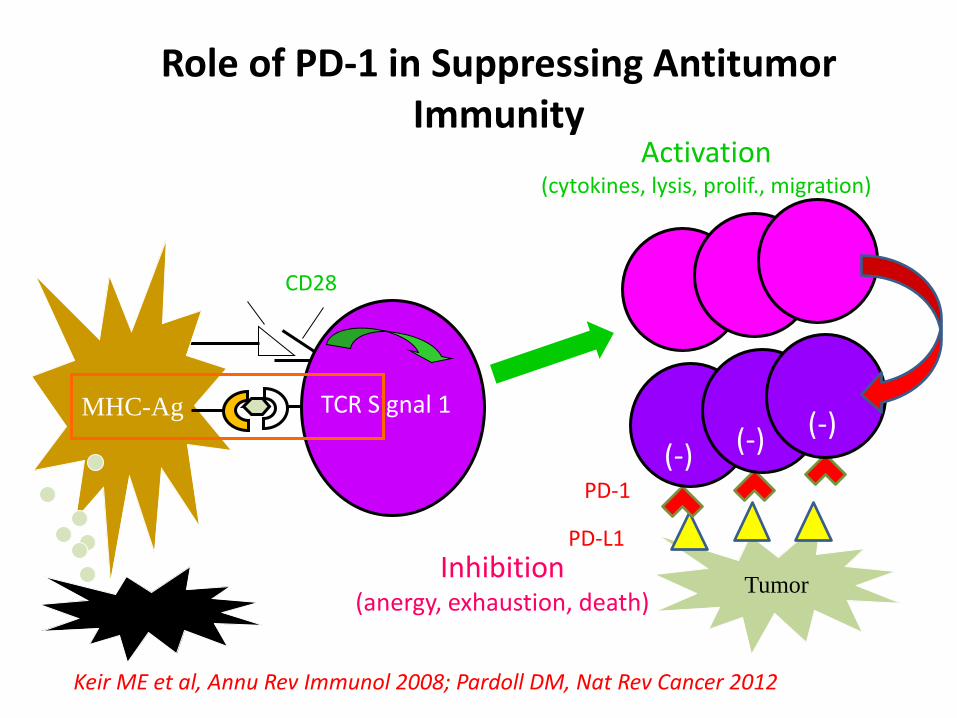
APC T cell
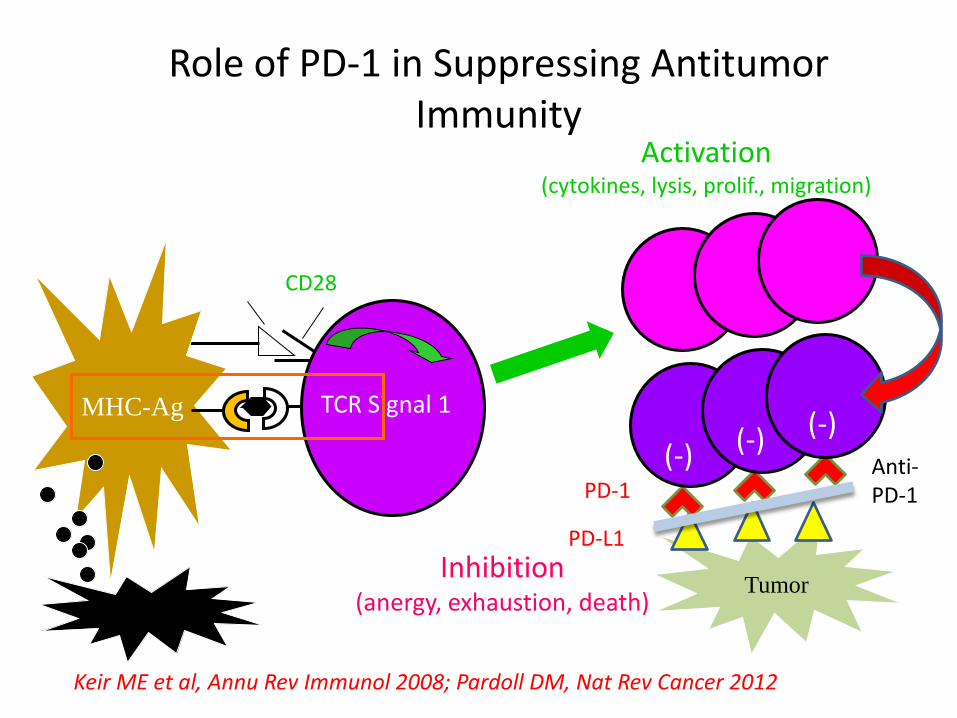
Activation (cytokines, lysis, prolif., migration)
B7.1 CD28
TCR Signal 1 MHC-Ag
Tumor
Role of PD-1 in Suppressing Antitumor Immunity
Tumor
PD-L1
PD-1
Keir ME et al, Annu Rev Immunol 2008; Pardoll DM, Nat Rev Cancer 2012
(-) (-) (-)
Inhibition (anergy, exhaustion, death)
APC T cell
Activation (cytokines, lysis, prolif., migration)
B7.1 CD28
TCR Signal 1 MHC-Ag
Tumor
Role of PD-1 in Suppressing Antitumor Immunity
Tumor
PD-L1
PD-1
Keir ME et al, Annu Rev Immunol 2008; Pardoll DM, Nat Rev Cancer 2012
(-) (-) (-)
Inhibition (anergy, exhaustion, death)
Anti-PD-1
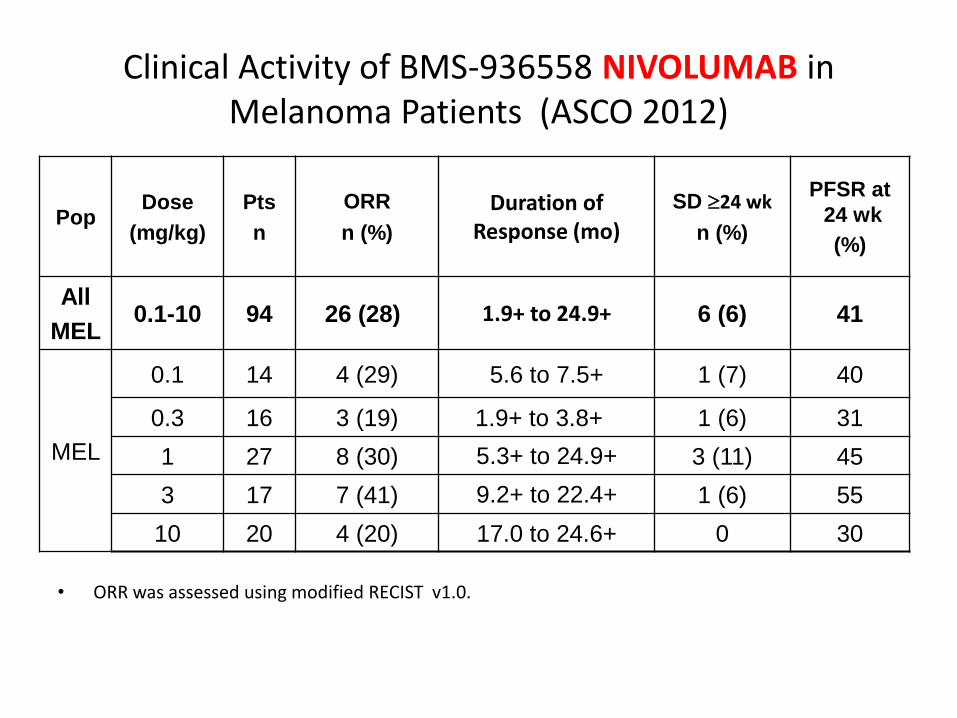
Clinical Activity of BMS-936558 NIVOLUMAB in Melanoma Patients (ASCO 2012)
• ORR was assessed using modified RECIST v1.0. 3 melanoma patients had a persistent reduction in baseline target lesions in the presence of new
lesions but were not classified as responders for the ORR calculation.
Pop Dose
(mg/kg)
Pts
n
ORR
n (%)
Duration of Response (mo)
SD 24 wk
n (%)
PFSR at
24 wk
(%)
All
MEL 0.1-10 94 26 (28) 1.9+ to 24.9+ 6 (6) 41
MEL
0.1 14 4 (29) 5.6 to 7.5+ 1 (7) 40
0.3 16 3 (19) 1.9+ to 3.8+ 1 (6) 31
1 27 8 (30) 5.3+ to 24.9+ 3 (11) 45
3 17 7 (41) 9.2+ to 22.4+ 1 (6) 55
10 20 4 (20) 17.0 to 24.6+ 0 30
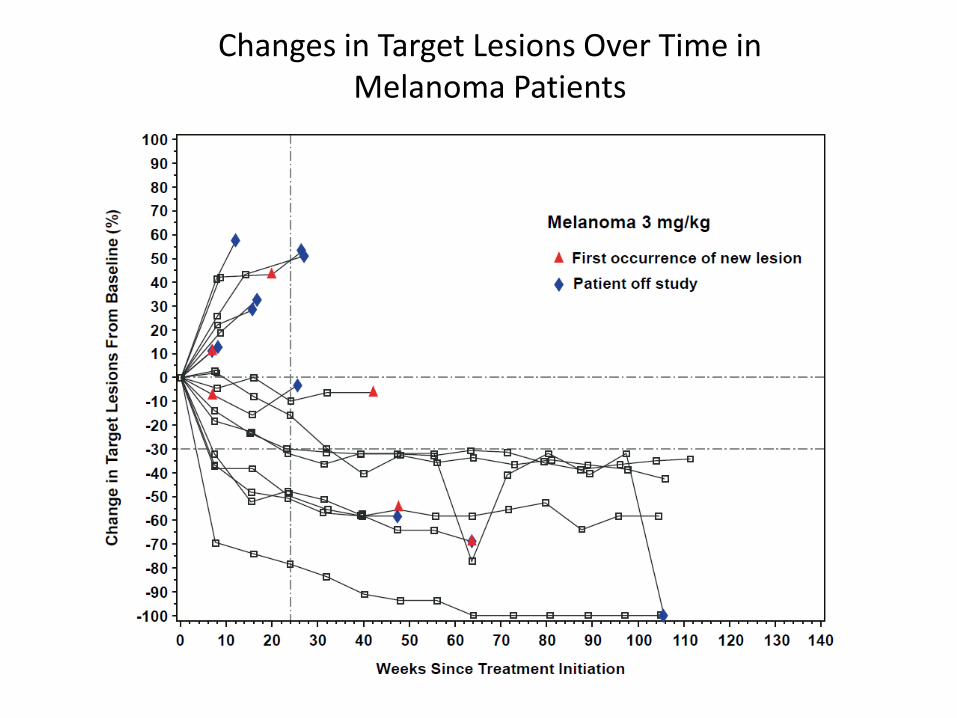
Changes in Target Lesions Over Time in Melanoma Patients
Possible Effect of BMS 936558 Nivolumab on survival
• Phase 1 study only at different doses so effect on survival is a guess only
• 13 of 18 patients (72%) who had a response and were followed for 1 year or more, had ongoing responses at 1 year
• Compares with about 70% 1 year survival of responders to Ipilimumab and 40% 1 year survival of patients responding to DTIC
• ASCO 2013 Sznol. Overall Median 16.8 mths. Responders 24mths 1Year 61%, 2 years 44%
Lambrolizumab (MK3475)
• A new player on the block sponsored by Merck
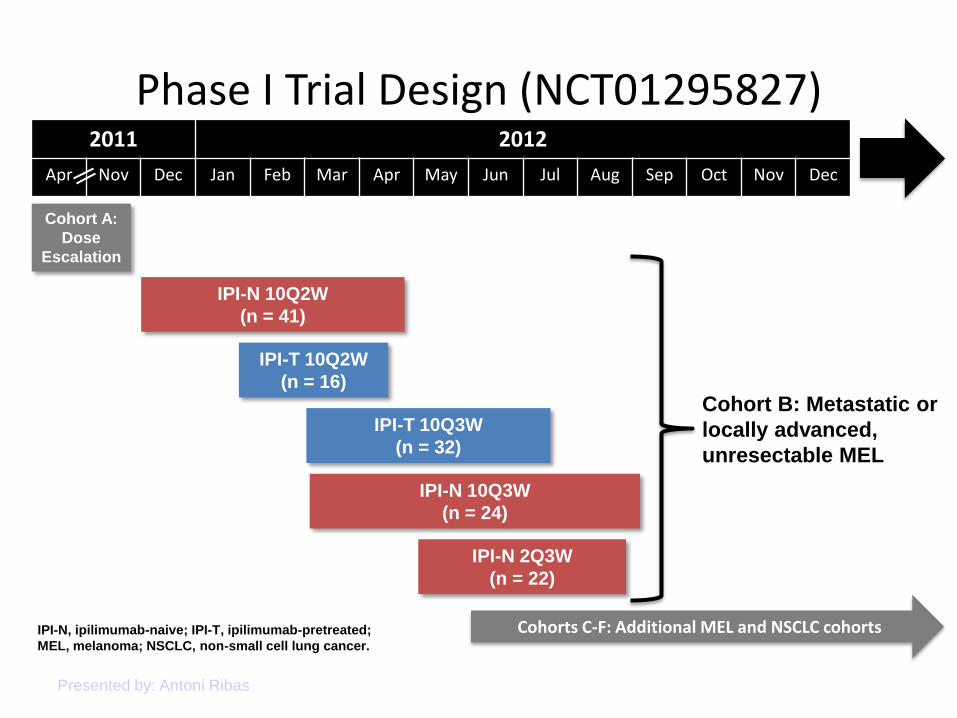
Phase I Trial Design (NCT01295827)
Presented by: Antoni Ribas
2011 2012
Apr Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
IPI-N 10Q2W
(n = 41)
IPI-N 10Q3W
(n = 24)
Cohort A:
Dose
Escalation
IPI-N 2Q3W
(n = 22)
IPI-T 10Q2W
(n = 16)
IPI-T 10Q3W
(n = 32)
Cohorts C-F: Additional MEL and NSCLC cohorts IPI-N, ipilimumab-naive; IPI-T, ipilimumab-pretreated;
MEL, melanoma; NSCLC, non-small cell lung cancer.
Cohort B: Metastatic or
locally advanced,
unresectable MEL
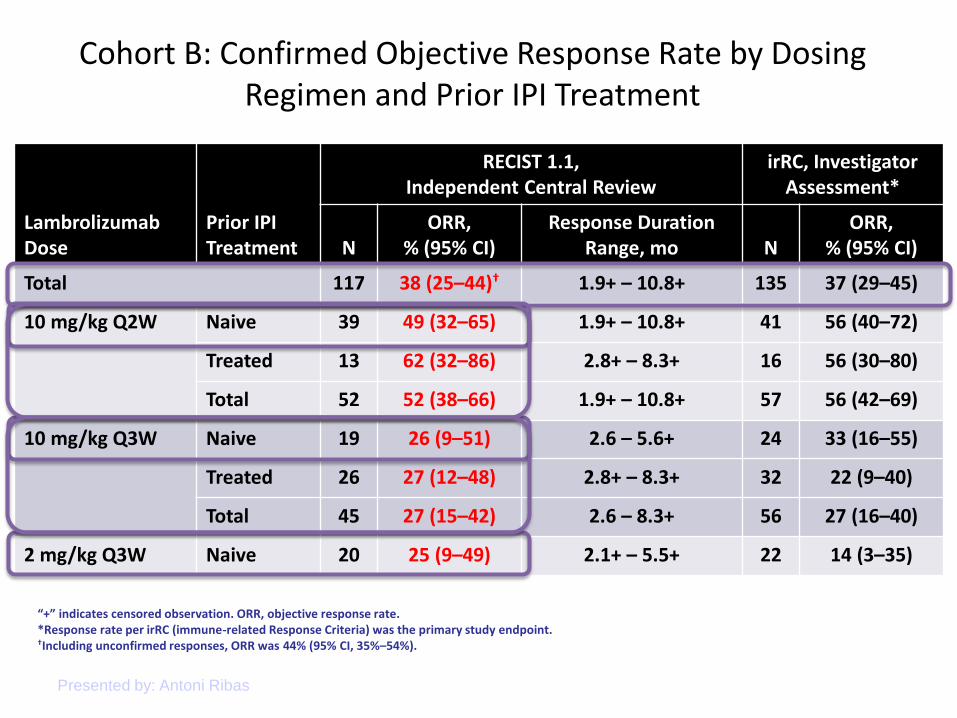
Cohort B: Confirmed Objective Response Rate by Dosing Regimen and Prior IPI Treatment
Presented by: Antoni Ribas
Lambrolizumab Dose
Prior IPI Treatment
RECIST 1.1, Independent Central Review
irRC, Investigator Assessment*
N ORR,
% (95% CI) Response Duration
Range, mo N ORR,
% (95% CI)
Total 117 38 (25–44)† 1.9+ – 10.8+ 135 37 (29–45)
10 mg/kg Q2W Naive 39 49 (32–65) 1.9+ – 10.8+ 41 56 (40–72)
Treated 13 62 (32–86) 2.8+ – 8.3+ 16 56 (30–80)
Total 52 52 (38–66) 1.9+ – 10.8+ 57 56 (42–69)
10 mg/kg Q3W Naive 19 26 (9–51) 2.6 – 5.6+ 24 33 (16–55)
Treated 26 27 (12–48) 2.8+ – 8.3+ 32 22 (9–40)
Total 45 27 (15–42) 2.6 – 8.3+ 56 27 (16–40)
2 mg/kg Q3W Naive 20 25 (9–49) 2.1+ – 5.5+ 22 14 (3–35)
“+” indicates censored observation. ORR, objective response rate. *Response rate per irRC (immune-related Response Criteria) was the primary study endpoint. †Including unconfirmed responses, ORR was 44% (95% CI, 35%–54%).
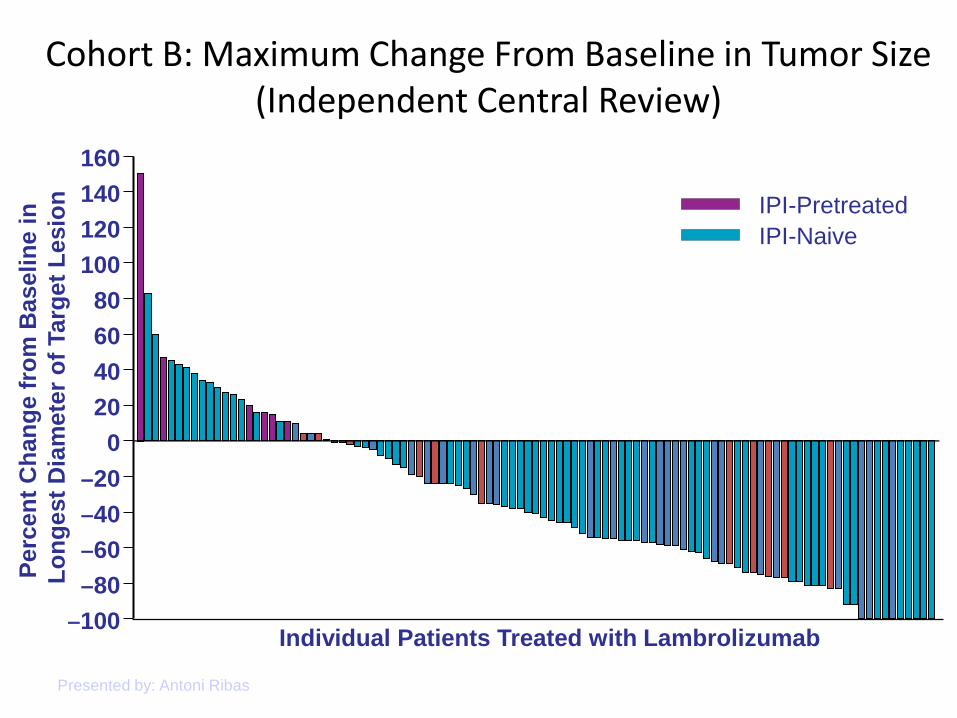
Cohort B: Maximum Change From Baseline in Tumor Size (Independent Central Review)
Presented by: Antoni Ribas
Individual Patients Treated with Lambrolizumab ‒100
‒80
‒60
‒40
‒20
0
20
40
60
80
100
120
140
160
Perc
en
t C
han
ge f
rom
Baseli
ne i
n
Lo
ng
est
Dia
mete
r o
f Targ
et
Lesio
n
IPI-Naive
IPI-Pretreated
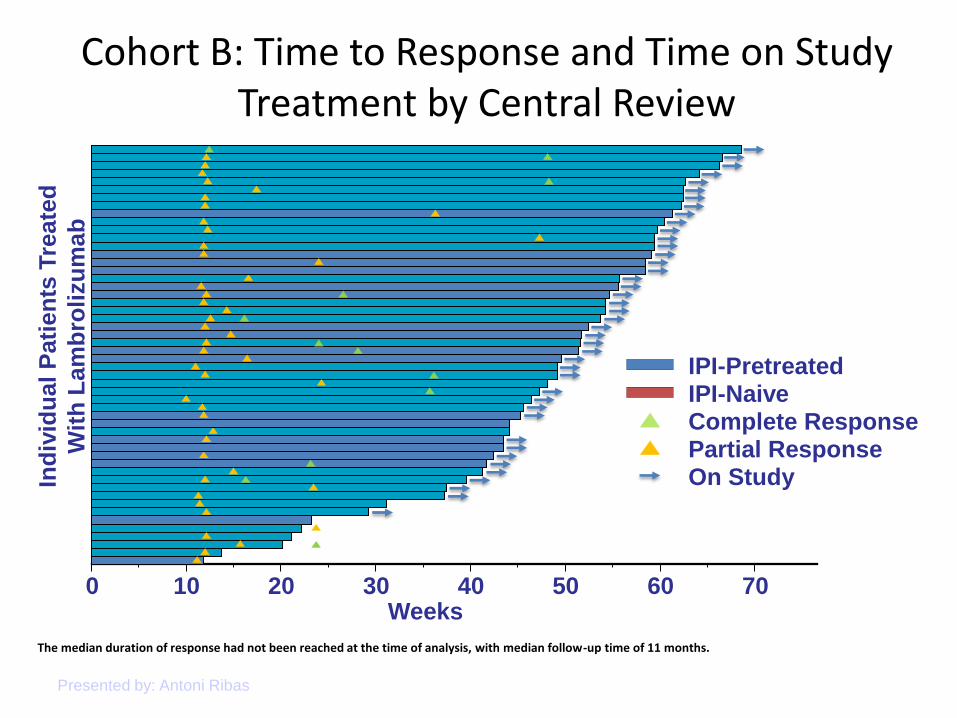
Cohort B: Time to Response and Time on Study Treatment by Central Review
Presented by: Antoni Ribas
0 10 20 30 40 50 60 70 Weeks
Ind
ivid
ual
Pati
en
ts T
reate
d
Wit
h L
am
bro
lizu
mab
IPI-Pretreated IPI-Naive Complete Response Partial Response On Study
The median duration of response had not been reached at the time of analysis, with median follow-up time of 11 months.
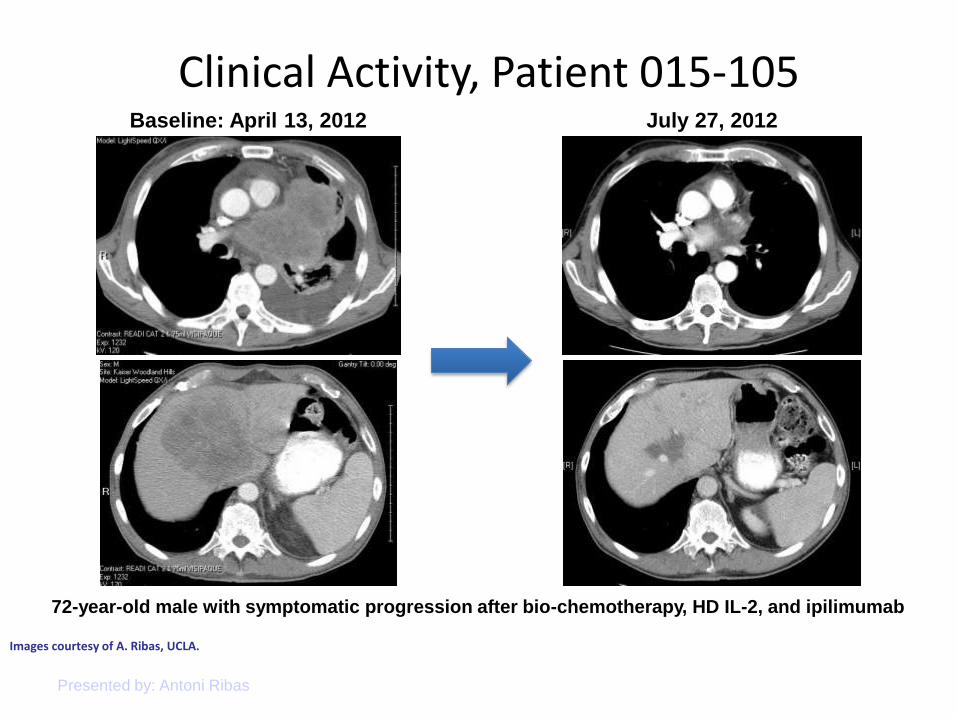
Clinical Activity, Patient 015-105
Presented by: Antoni Ribas
Baseline: April 13, 2012 July 27, 2012
Images courtesy of A. Ribas, UCLA.
72-year-old male with symptomatic progression after bio-chemotherapy, HD IL-2, and ipilimumab
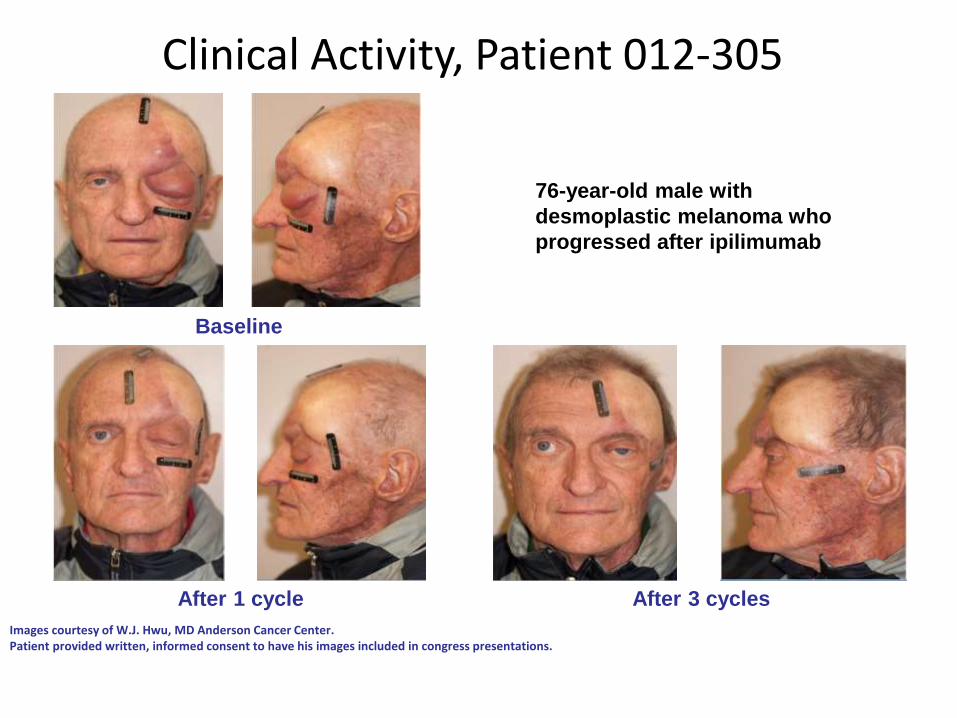
Baseline
After 3 cycles After 1 cycle
Clinical Activity, Patient 012-305
Images courtesy of W.J. Hwu, MD Anderson Cancer Center. Patient provided written, informed consent to have his images included in congress presentations.
76-year-old male with
desmoplastic melanoma who
progressed after ipilimumab
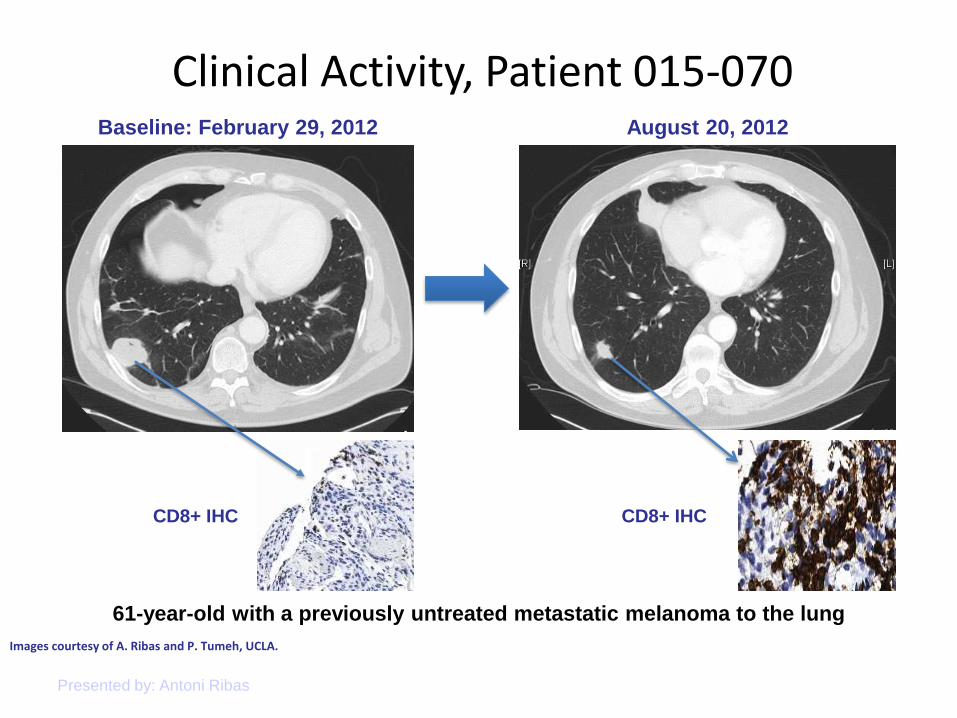
Clinical Activity, Patient 015-070
Presented by: Antoni Ribas
Images courtesy of A. Ribas and P. Tumeh, UCLA.
Baseline: February 29, 2012 August 20, 2012
CD8+ IHC CD8+ IHC
61-year-old with a previously untreated metastatic melanoma to the lung
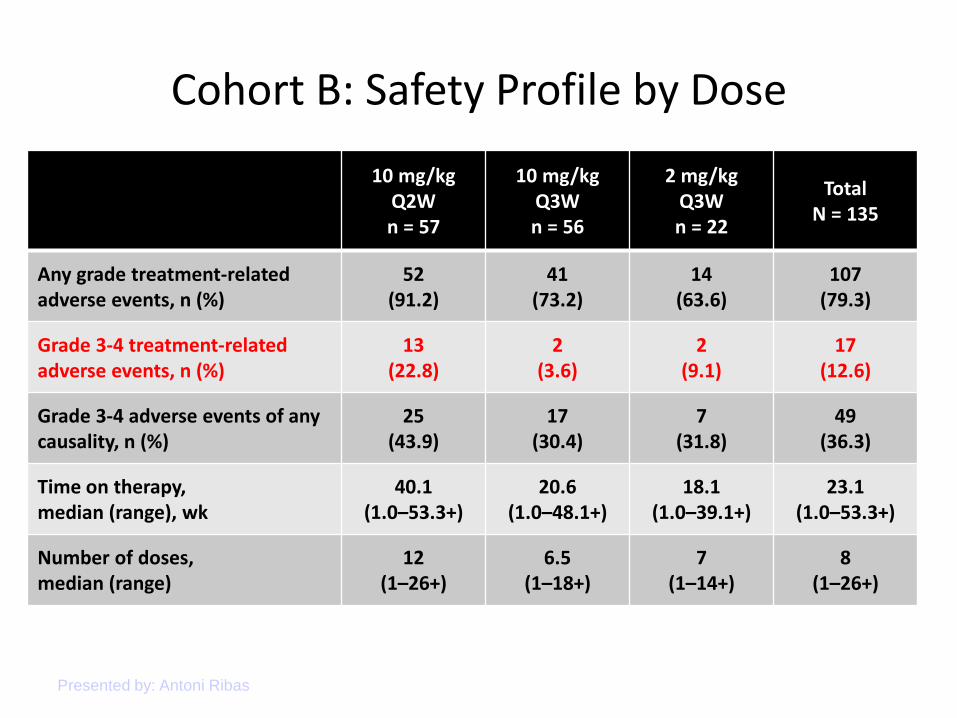
Cohort B: Safety Profile by Dose
Presented by: Antoni Ribas
10 mg/kg Q2W n = 57
10 mg/kg Q3W n = 56
2 mg/kg Q3W n = 22
Total N = 135
Any grade treatment-related adverse events, n (%)
52 (91.2)
41 (73.2)
14 (63.6)
107 (79.3)
Grade 3-4 treatment-related adverse events, n (%)
13 (22.8)
2 (3.6)
2 (9.1)
17 (12.6)
Grade 3-4 adverse events of any causality, n (%)
25 (43.9)
17 (30.4)
7 (31.8)
49 (36.3)
Time on therapy, median (range), wk
40.1 (1.0–53.3+)
20.6 (1.0–48.1+)
18.1 (1.0–39.1+)
23.1 (1.0–53.3+)
Number of doses, median (range)
12 (1–26+)
6.5 (1–18+)
7 (1–14+)
8 (1–26+)
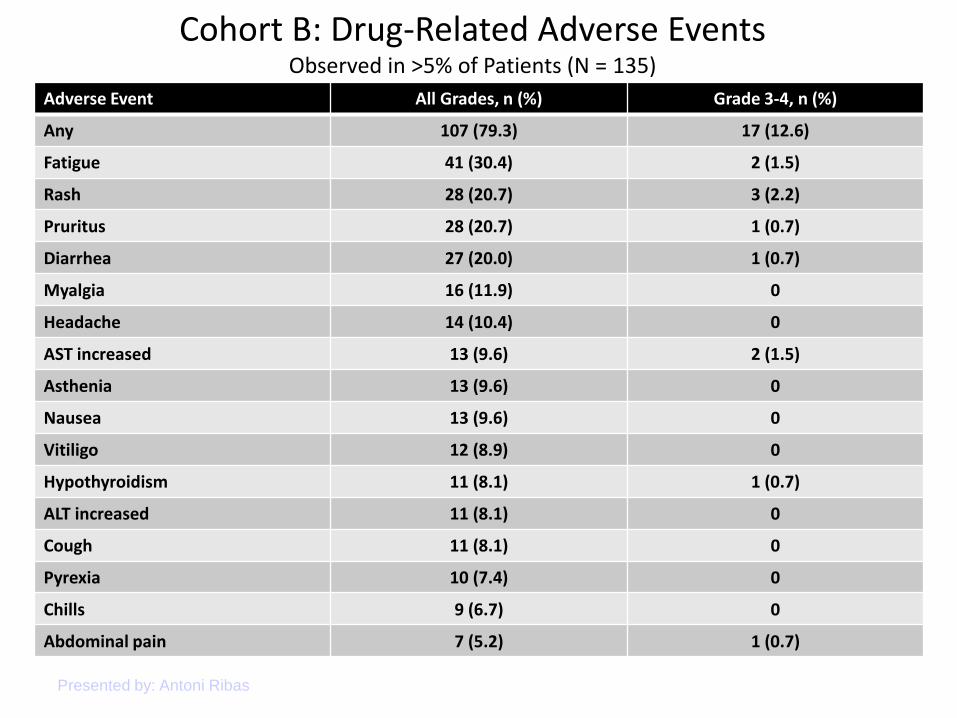
Cohort B: Drug-Related Adverse Events Observed in >5% of Patients (N = 135)
Presented by: Antoni Ribas
Adverse Event All Grades, n (%) Grade 3-4, n (%)
Any 107 (79.3) 17 (12.6)
Fatigue 41 (30.4) 2 (1.5)
Rash 28 (20.7) 3 (2.2)
Pruritus 28 (20.7) 1 (0.7)
Diarrhea 27 (20.0) 1 (0.7)
Myalgia 16 (11.9) 0
Headache 14 (10.4) 0
AST increased 13 (9.6) 2 (1.5)
Asthenia 13 (9.6) 0
Nausea 13 (9.6) 0
Vitiligo 12 (8.9) 0
Hypothyroidism 11 (8.1) 1 (0.7)
ALT increased 11 (8.1) 0
Cough 11 (8.1) 0
Pyrexia 10 (7.4) 0
Chills 9 (6.7) 0
Abdominal pain 7 (5.2) 1 (0.7)
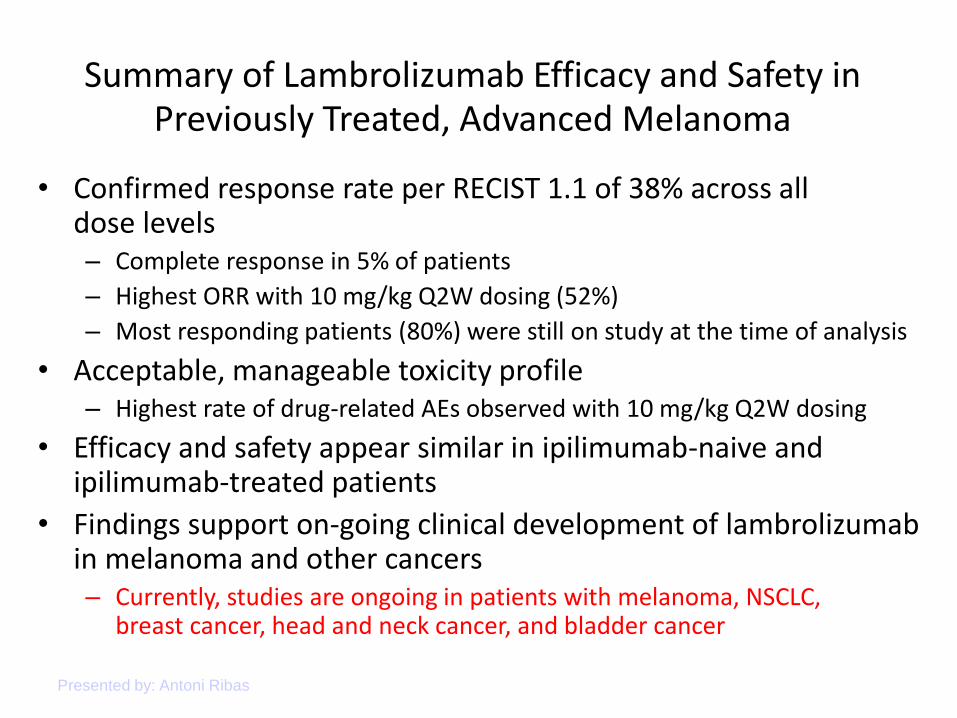
Summary of Lambrolizumab Efficacy and Safety in Previously Treated, Advanced Melanoma
• Confirmed response rate per RECIST 1.1 of 38% across all dose levels – Complete response in 5% of patients
– Highest ORR with 10 mg/kg Q2W dosing (52%)
– Most responding patients (80%) were still on study at the time of analysis
• Acceptable, manageable toxicity profile – Highest rate of drug-related AEs observed with 10 mg/kg Q2W dosing
• Efficacy and safety appear similar in ipilimumab-naive and ipilimumab-treated patients
• Findings support on-going clinical development of lambrolizumab in melanoma and other cancers – Currently, studies are ongoing in patients with melanoma, NSCLC,
breast cancer, head and neck cancer, and bladder cancer
Presented by: Antoni Ribas
What Happens When Ipi and Nivolumab are Combined?
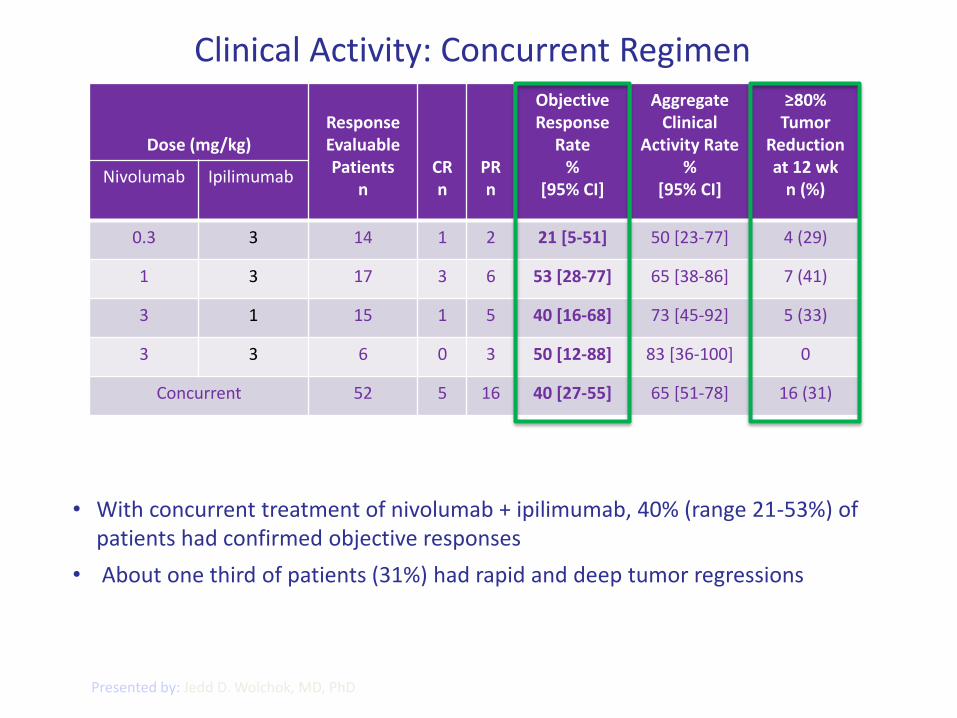
Clinical Activity: Concurrent Regimen
Dose (mg/kg)
Response Evaluable Patients
n
CR n
PR n
Objective Response
Rate
% [95% CI]
Aggregate Clinical
Activity Rate
% [95% CI]
≥80% Tumor
Reduction at 12 wk
n (%) Nivolumab Ipilimumab
0.3 3 14 1 2 21 [5-51] 50 [23-77] 4 (29)
1 3 17 3 6 53 [28-77] 65 [38-86] 7 (41)
3 1 15 1 5 40 [16-68] 73 [45-92] 5 (33)
3 3 6 0 3 50 [12-88] 83 [36-100] 0
Concurrent 52 5 16 40 [27-55] 65 [51-78] 16 (31)
Presented by: Jedd D. Wolchok, MD, PhD
• With concurrent treatment of nivolumab + ipilimumab, 40% (range 21-53%) of patients had confirmed objective responses
• About one third of patients (31%) had rapid and deep tumor regressions
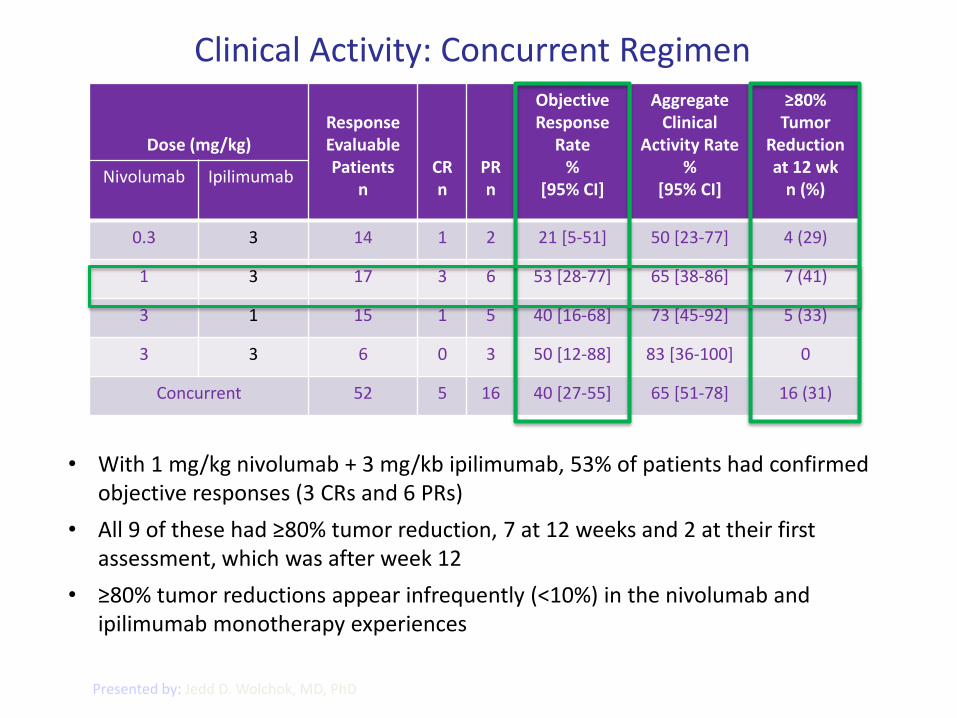
Clinical Activity: Concurrent Regimen
Dose (mg/kg)
Response Evaluable Patients
n
CR n
PR n
Objective Response
Rate
% [95% CI]
Aggregate Clinical
Activity Rate
% [95% CI]
≥80% Tumor
Reduction at 12 wk
n (%) Nivolumab Ipilimumab
0.3 3 14 1 2 21 [5-51] 50 [23-77] 4 (29)
1 3 17 3 6 53 [28-77] 65 [38-86] 7 (41)
3 1 15 1 5 40 [16-68] 73 [45-92] 5 (33)
3 3 6 0 3 50 [12-88] 83 [36-100] 0
Concurrent 52 5 16 40 [27-55] 65 [51-78] 16 (31)
Presented by: Jedd D. Wolchok, MD, PhD
• With 1 mg/kg nivolumab + 3 mg/kb ipilimumab, 53% of patients had confirmed objective responses (3 CRs and 6 PRs)
• All 9 of these had ≥80% tumor reduction, 7 at 12 weeks and 2 at their first assessment, which was after week 12
• ≥80% tumor reductions appear infrequently (<10%) in the nivolumab and ipilimumab monotherapy experiences
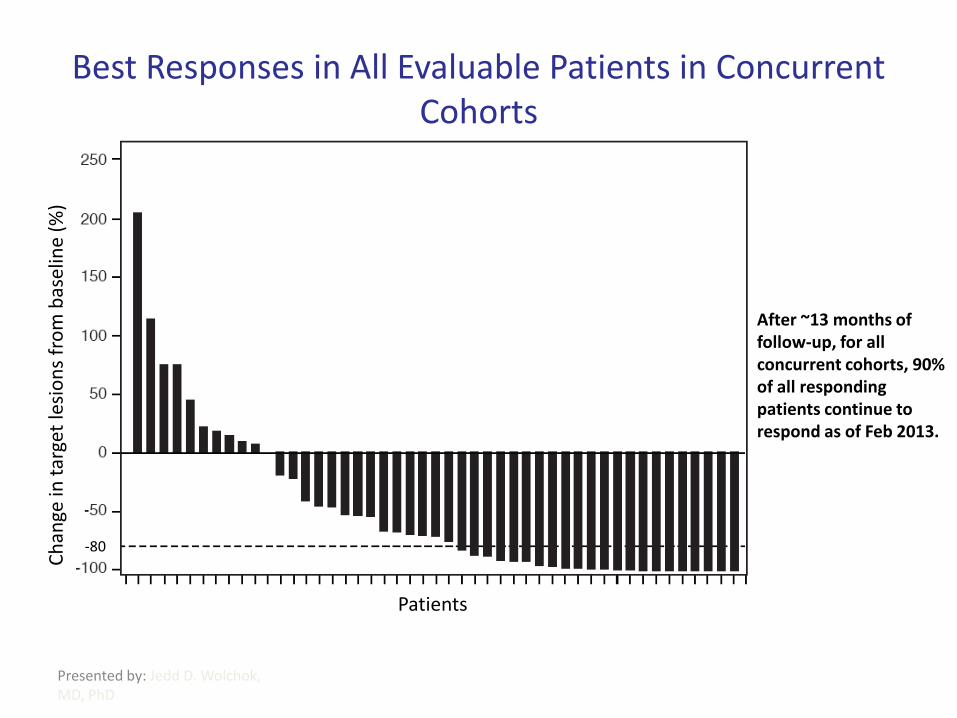
Best Responses in All Evaluable Patients in Concurrent Cohorts
Presented by: Jedd D. Wolchok, MD, PhD
After ~13 months of follow-up, for all concurrent cohorts, 90% of all responding patients continue to respond as of Feb 2013.
Patients
Ch
ange
in t
arge
t le
sio
ns
fro
m b
asel
ine
(%)
-80
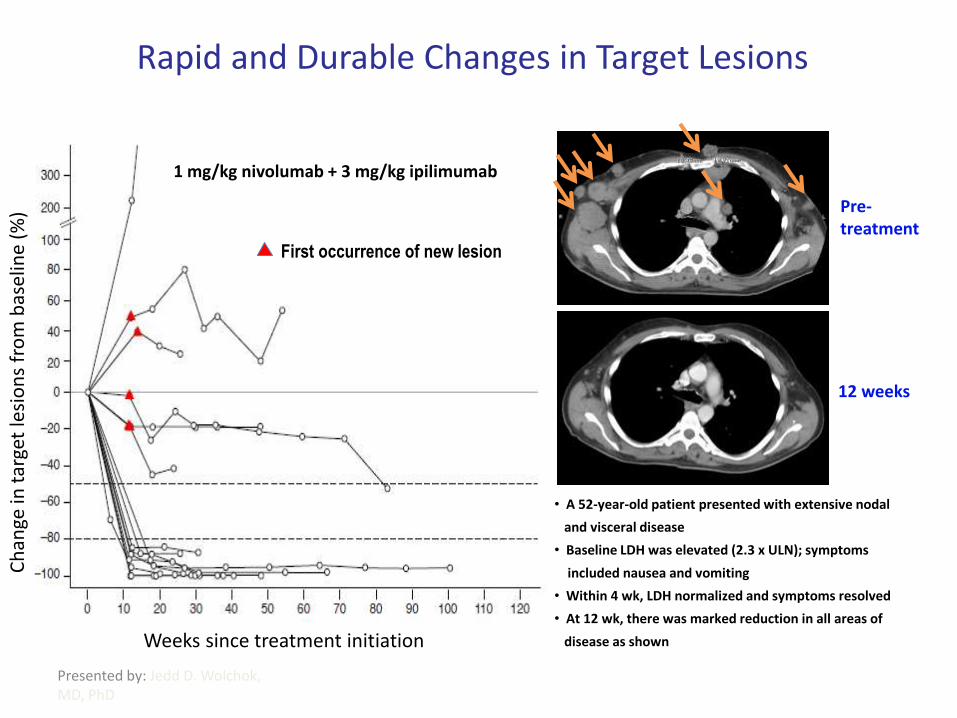
Rapid and Durable Changes in Target Lesions
Presented by: Jedd D. Wolchok, MD, PhD
1 mg/kg nivolumab + 3 mg/kg ipilimumab
First occurrence of new lesion
• A 52-year-old patient presented with extensive nodal
and visceral disease
• Baseline LDH was elevated (2.3 x ULN); symptoms
included nausea and vomiting
• Within 4 wk, LDH normalized and symptoms resolved
• At 12 wk, there was marked reduction in all areas of
disease as shown Weeks since treatment initiation
Ch
ange
in t
arge
t le
sio
ns
fro
m b
asel
ine
(%) Pre-
treatment
12 weeks
Patients at Risk
1 mg + 3 mg
All concurrent
17
53
16
47
16
36
14
29
10
19
5
10
3
7
2
4
2
4
1
3
0
1
0
1
0
0
n=17
n=53
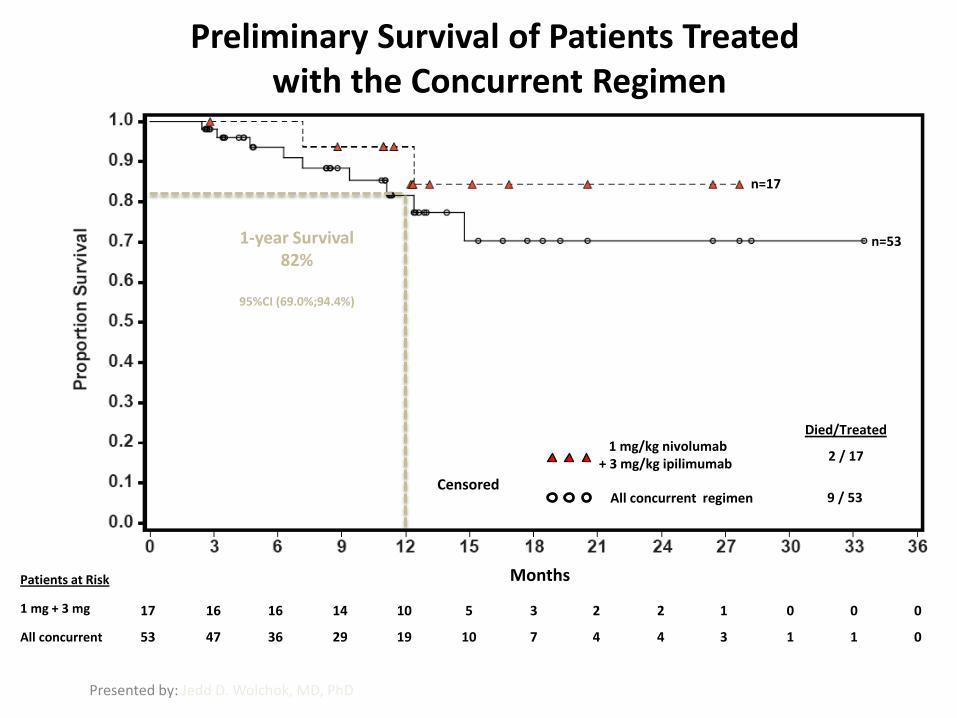
Preliminary Survival of Patients Treated with the Concurrent Regimen
Presented by: Jedd D. Wolchok, MD, PhD
Months
9 / 53 Censored
All concurrent regimen
1 mg/kg nivolumab + 3 mg/kg ipilimumab
Died/Treated
2 / 17
1-year Survival 82%
95%CI (69.0%;94.4%)
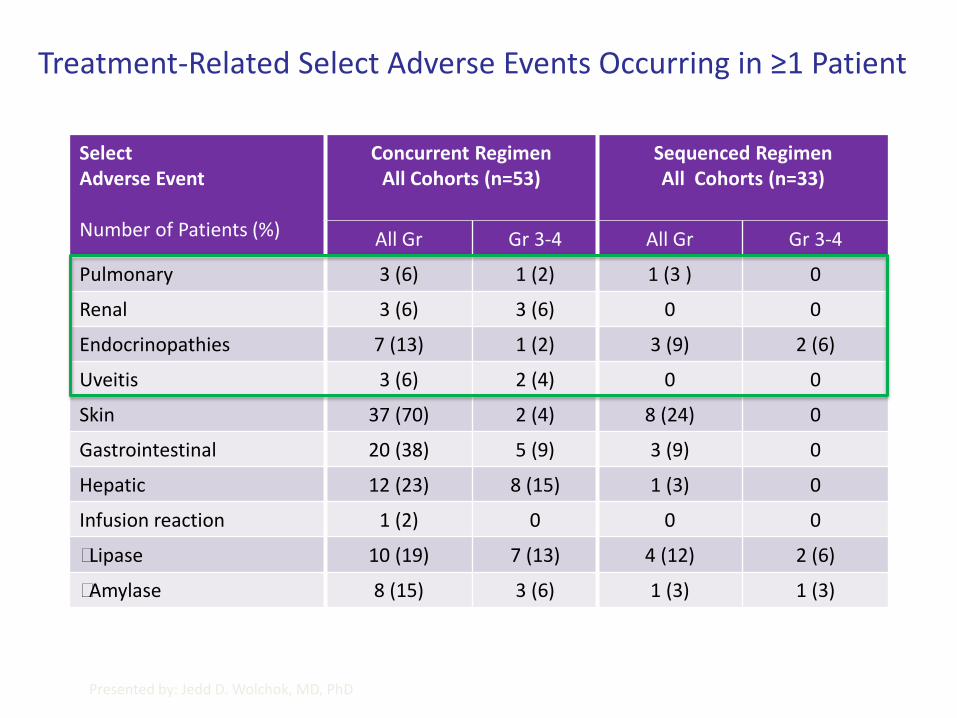
Treatment-Related Select Adverse Events Occurring in ≥1 Patient
Select Adverse Event Number of Patients (%)
Concurrent Regimen All Cohorts (n=53)
Sequenced Regimen All Cohorts (n=33)
All Gr Gr 3-4 All Gr Gr 3-4
Pulmonary 3 (6) 1 (2) 1 (3 ) 0
Renal 3 (6) 3 (6) 0 0
Endocrinopathies 7 (13) 1 (2) 3 (9) 2 (6)
Uveitis 3 (6) 2 (4) 0 0
Skin 37 (70) 2 (4) 8 (24) 0
Gastrointestinal 20 (38) 5 (9) 3 (9) 0
Hepatic 12 (23) 8 (15) 1 (3) 0
Infusion reaction 1 (2) 0 0 0
Lipase 10 (19) 7 (13) 4 (12) 2 (6)
Amylase 8 (15) 3 (6) 1 (3) 1 (3)
Presented by: Jedd D. Wolchok, MD, PhD
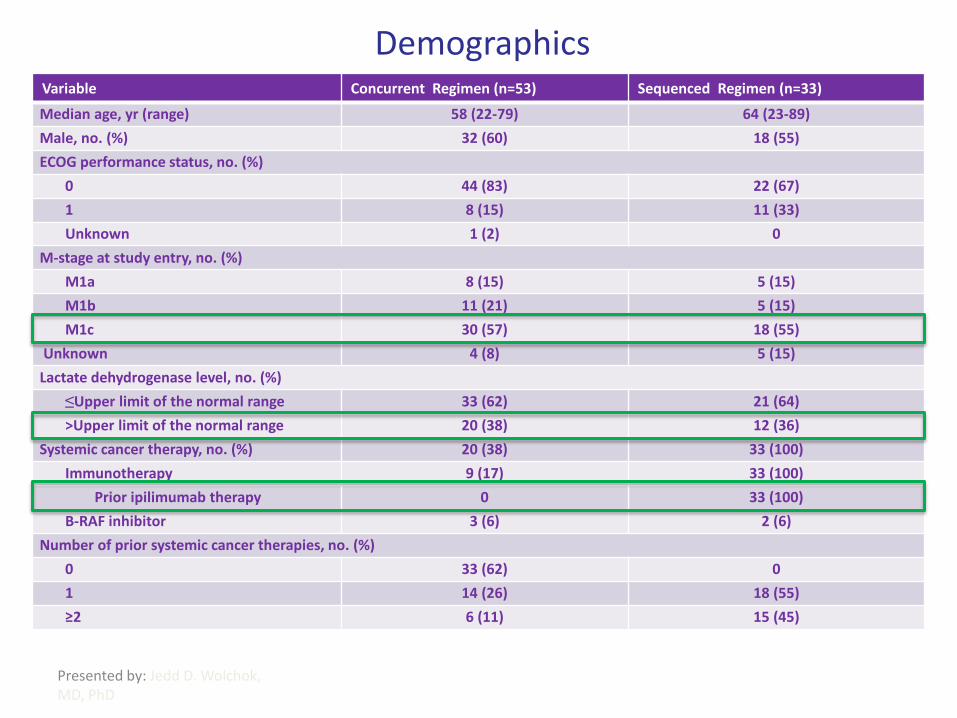
Demographics
Variable Concurrent Regimen (n=53))) Sequenced Regimen (n=33)
Median age, yr (range) 58 (22-79) 64 (23-89)
Male, no. (%) 32 (60) 18 (55)
ECOG performance status, no. (%)
0 44 (83) 22 (67)
1 8 (15) 11 (33)
Unknown 1 (2) 0
M-stage at study entry, no. (%)
M1a 8 (15) 5 (15)
M1b 11 (21) 5 (15)
M1c 30 (57) 18 (55)
Unknown 4 (8) 5 (15)
Lactate dehydrogenase level, no. (%)
≤Upper limit of the normal range 33 (62) 21 (64)
>Upper limit of the normal range 20 (38) 12 (36)
Systemic cancer therapy, no. (%) 20 (38) 33 (100)
Immunotherapy 9 (17) 33 (100)
Prior ipilimumab therapy 0 33 (100)
B-RAF inhibitor 3 (6) 2 (6)
Number of prior systemic cancer therapies, no. (%)
0 33 (62) 0
1 14 (26) 18 (55)
≥2 6 (11) 15 (45)
Presented by: Jedd D. Wolchok, MD, PhD
Conclusions
• The concurrent combination of nivolumab and ipilimumab induced objective response rates appearing higher than published monotherapy values
• The nature of the responses appeared to be distinctly different from those of the nivolumab and ipilimumab monotherapies
– Responses were rapid and deep
– At the combined doses chosen for phase 3 study, all responding patients achieved deep or complete responses
• Treatment-related adverse events managed using standard protocols
– No treatment-related deaths
• Clinical activity in patients who previously progressed on ipilimumab and then received nivolumab
• Based on these results, a phase 3 trial is open to investigate the efficacy of the concurrent nivolumab/ipilimumab combination vs. nivolumab vs. ipilimumab in patients with advanced melanoma (NCT01844505)
– This combination is also being investigated in non-small-cell lung cancer and renal cell carcinoma
Presented by: Jedd D.
Wolchok, MD, PhD
THE NEW TREATMENT ALGORITHMS
• BMS 3 arm study. Ipi v Nivo v Ipi plus Nivo
• Merck 3 arm study Lambrolizumab 2mg v 10mg v Ipi
• NRAS failures
Novartis MEK 162 Nemo study
• BRAFV600 melanoma
Roche GO28141 Combi study-20% accrued .
Novartis LGX818 +-MEK162
WHAT ABOUT SELECTIVE BRAF INHIBITORS?
• BRAF mutation rates
• Side effects including new malignancies
• Resistance to BRAFi and BRAF plus MEK combinations
• LGX 818
NRAS
BRAF
ERK
MITF
MEK
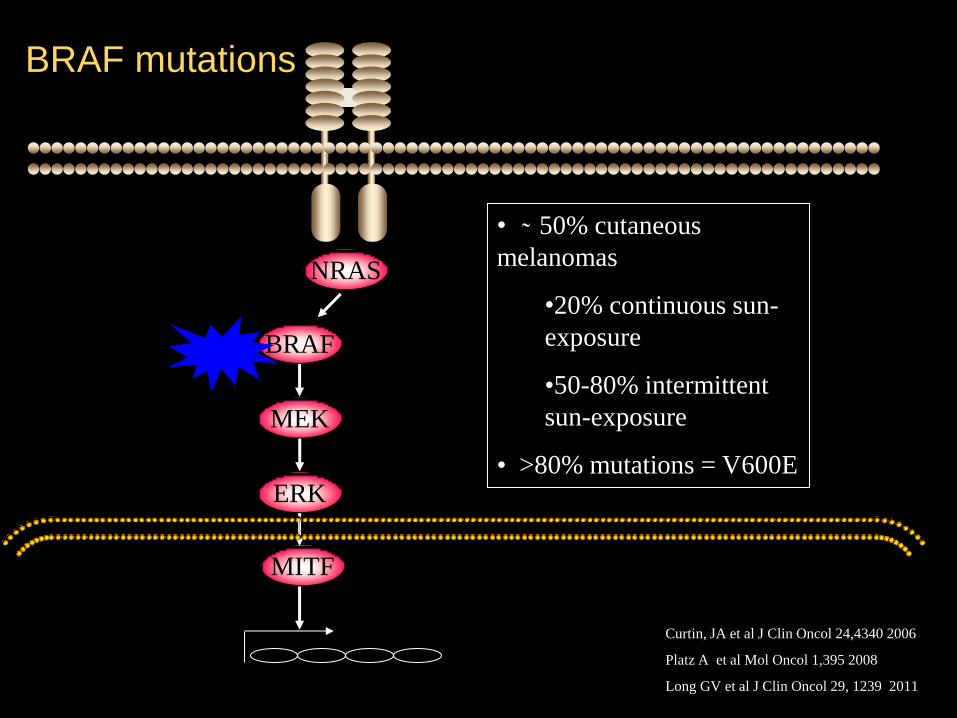
BRAF mutations
• ̴ 50% cutaneous
melanomas
•20% continuous sun-
exposure
•50-80% intermittent
sun-exposure
• >80% mutations = V600E
Curtin, JA et al J Clin Oncol 24,4340 2006
Platz A et al Mol Oncol 1,395 2008
Long GV et al J Clin Oncol 29, 1239 2011
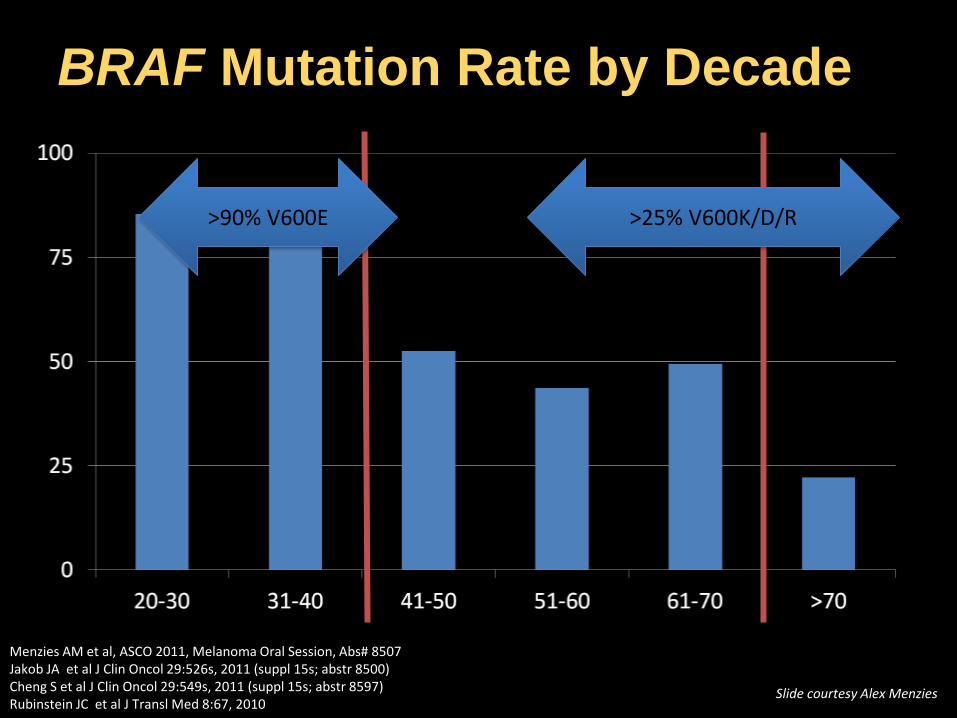
BRAF Mutation Rate by Decade
Menzies AM et al, ASCO 2011, Melanoma Oral Session, Abs# 8507 Jakob JA et al J Clin Oncol 29:526s, 2011 (suppl 15s; abstr 8500) Cheng S et al J Clin Oncol 29:549s, 2011 (suppl 15s; abstr 8597) Rubinstein JC et al J Transl Med 8:67, 2010
>25% V600K/D/R >90% V600E
Slide courtesy Alex Menzies
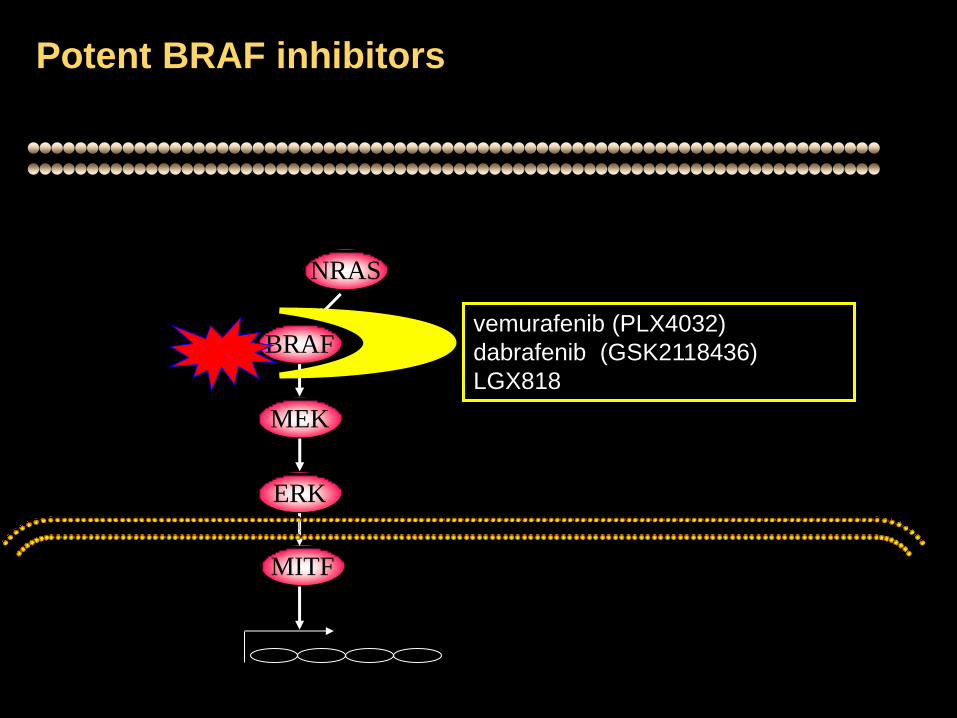
NRAS
BRAF
ERK
MITF
MEK
Potent BRAF inhibitors
vemurafenib (PLX4032)
dabrafenib (GSK2118436)
LGX818
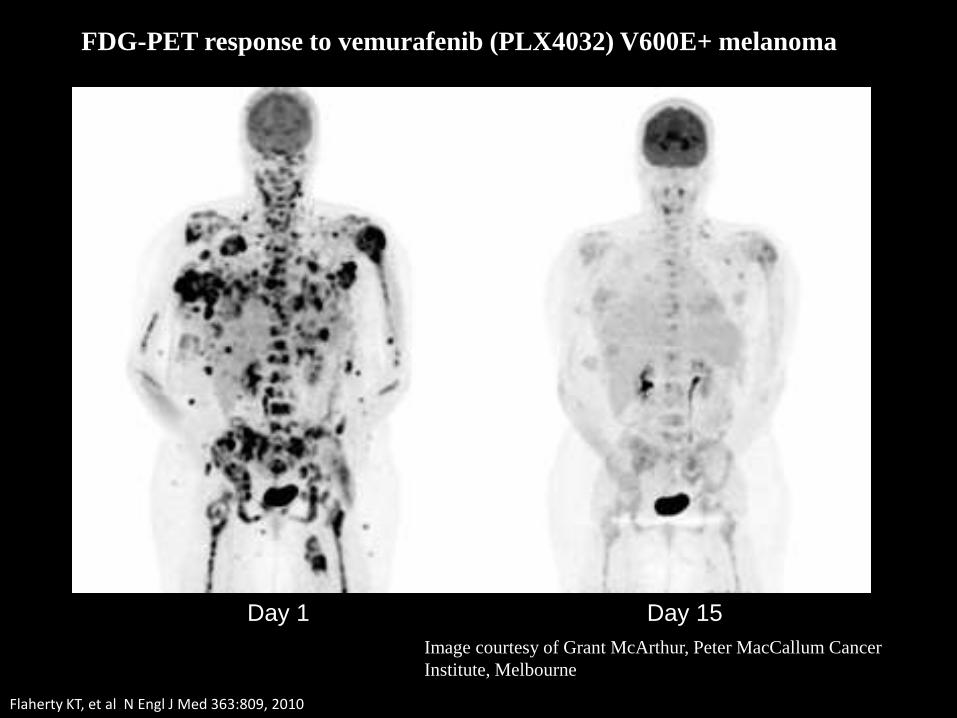
Image courtesy of Grant McArthur, Peter MacCallum Cancer
Institute, Melbourne
Day 1 Day 15
FDG-PET response to vemurafenib (PLX4032) V600E+ melanoma
Flaherty KT, et al N Engl J Med 363:809, 2010
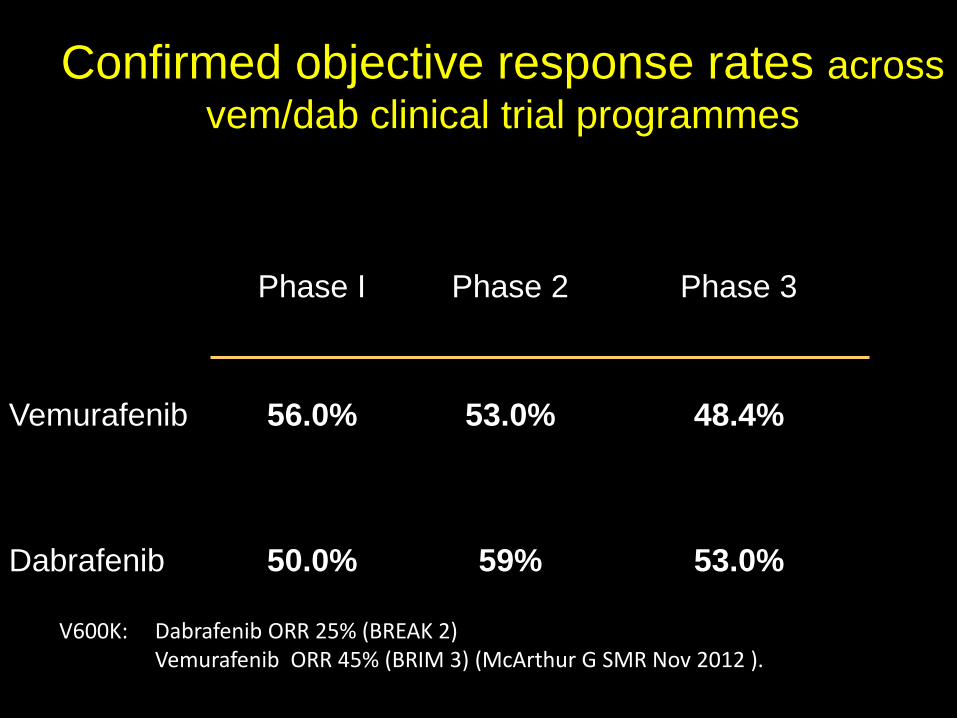
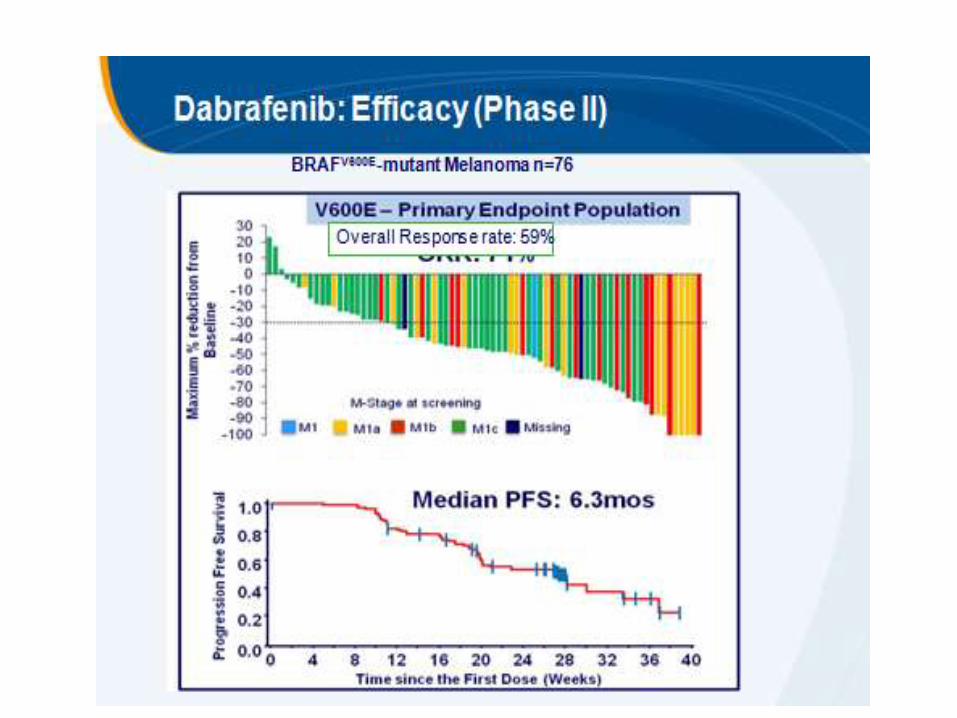
Confirmed objective response rates across
vem/dab clinical trial programmes
V600E
Phase I Phase 2 Phase 3
Vemurafenib 56.0% 53.0% 48.4%
Dabrafenib 50.0% 59%
53.0%
V600K: Dabrafenib ORR 25% (BREAK 2) Vemurafenib ORR 45% (BRIM 3) (McArthur G SMR Nov 2012 ).
What have we learnt?
AROUND 50% OF BRAFi-TREATED
V600 MUT MELANOMA PATIENTS
PROGRESS AT ABOUT 6 MTHS
OS 1.5X DTIC; 1/3rd alive > 2yrs
V600E SIMILAR TO V600K
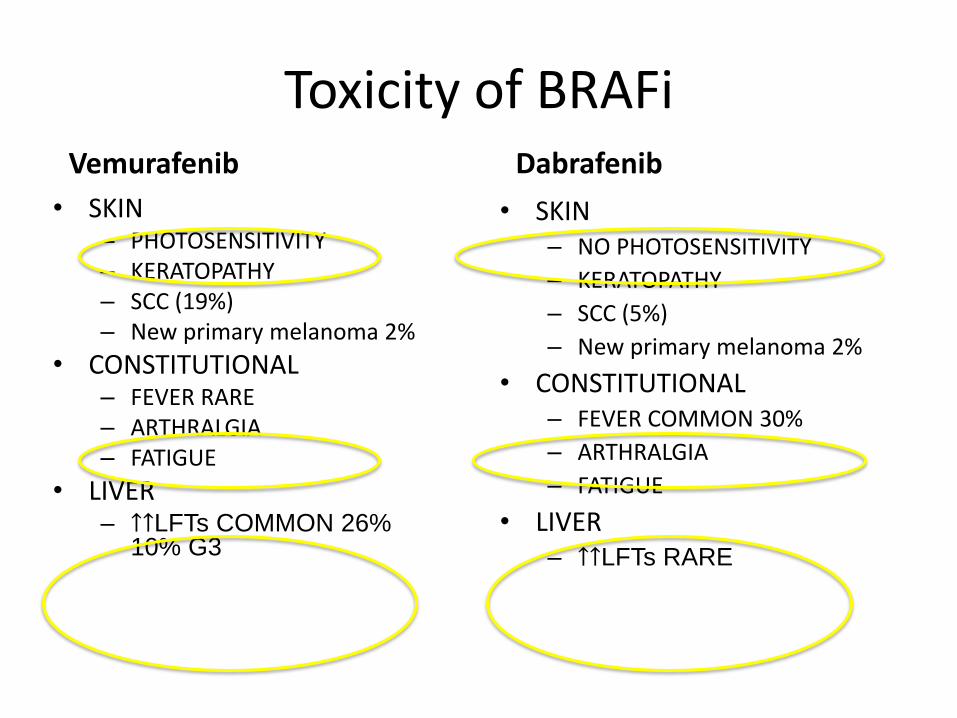
Toxicity of BRAFi Vemurafenib
• SKIN – PHOTOSENSITIVITY – KERATOPATHY – SCC (19%) – New primary melanoma 2%
• CONSTITUTIONAL – FEVER RARE – ARTHRALGIA – FATIGUE
• LIVER – ↑↑LFTs COMMON 26%
10% G3
Dabrafenib
• SKIN – NO PHOTOSENSITIVITY
– KERATOPATHY
– SCC (5%)
– New primary melanoma 2%
• CONSTITUTIONAL – FEVER COMMON 30%
– ARTHRALGIA
– FATIGUE
• LIVER – ↑↑LFTs RARE
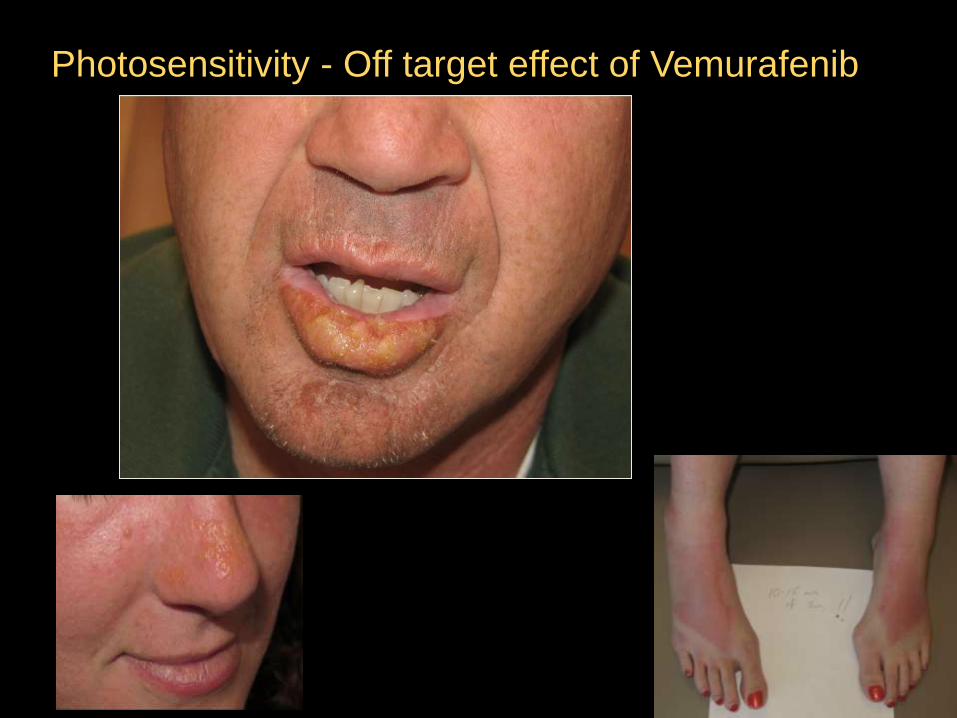
Photosensitivity - Off target effect of Vemurafenib
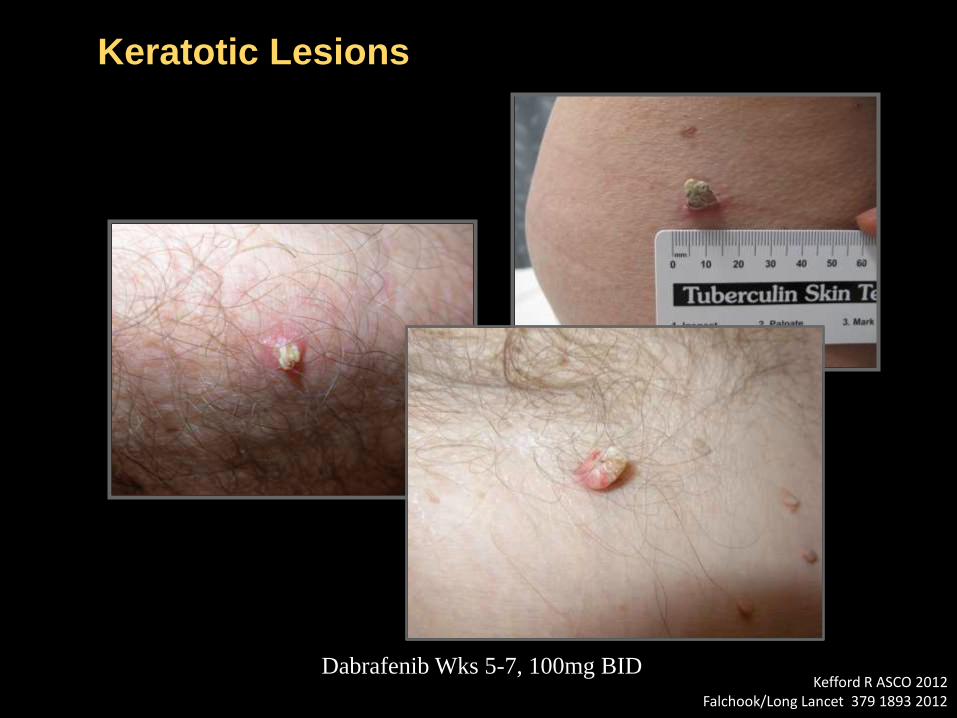
Keratotic Lesions
Dabrafenib Wks 5-7, 100mg BID Kefford R ASCO 2012
Falchook/Long Lancet 379 1893 2012
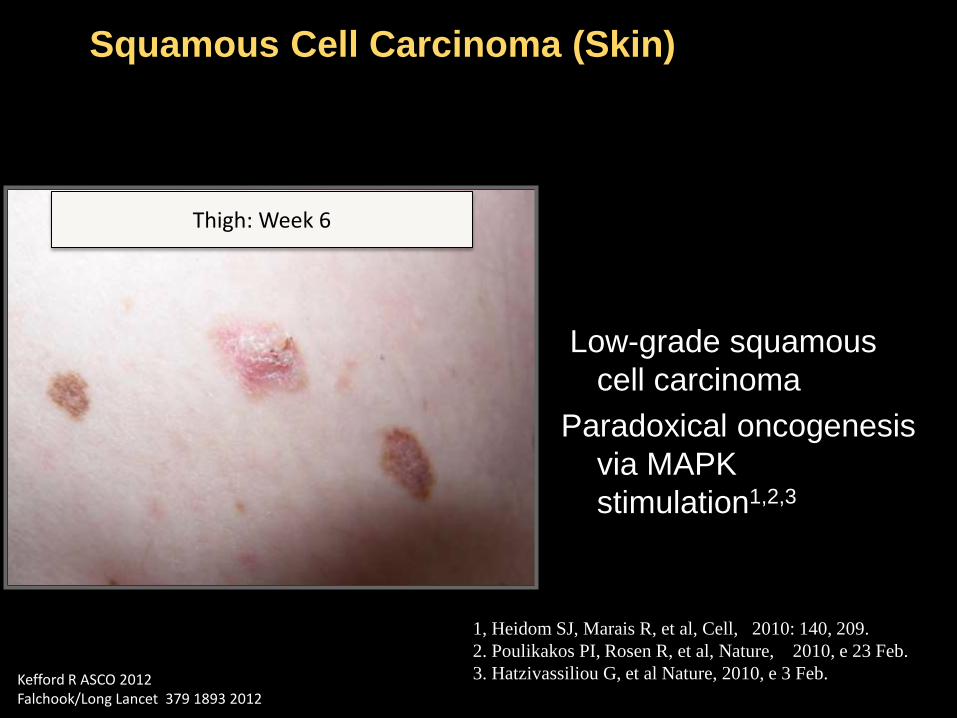
Squamous Cell Carcinoma (Skin)
Thigh: Week 6
Low-grade squamous
cell carcinoma
Paradoxical oncogenesis
via MAPK
stimulation1,2,3
1, Heidom SJ, Marais R, et al, Cell, 2010: 140, 209.
2. Poulikakos PI, Rosen R, et al, Nature, 2010, e 23 Feb.
3. Hatzivassiliou G, et al Nature, 2010, e 3 Feb. Kefford R ASCO 2012 Falchook/Long Lancet 379 1893 2012
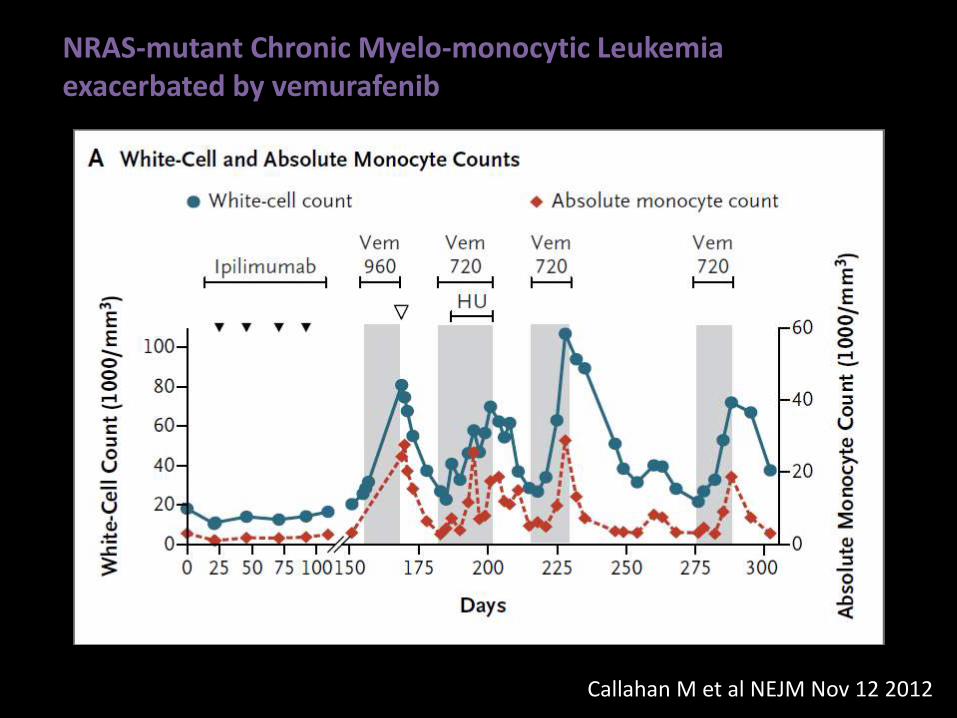
Callahan M et al NEJM Nov 12 2012
NRAS-mutant Chronic Myelo-monocytic Leukemia exacerbated by vemurafenib
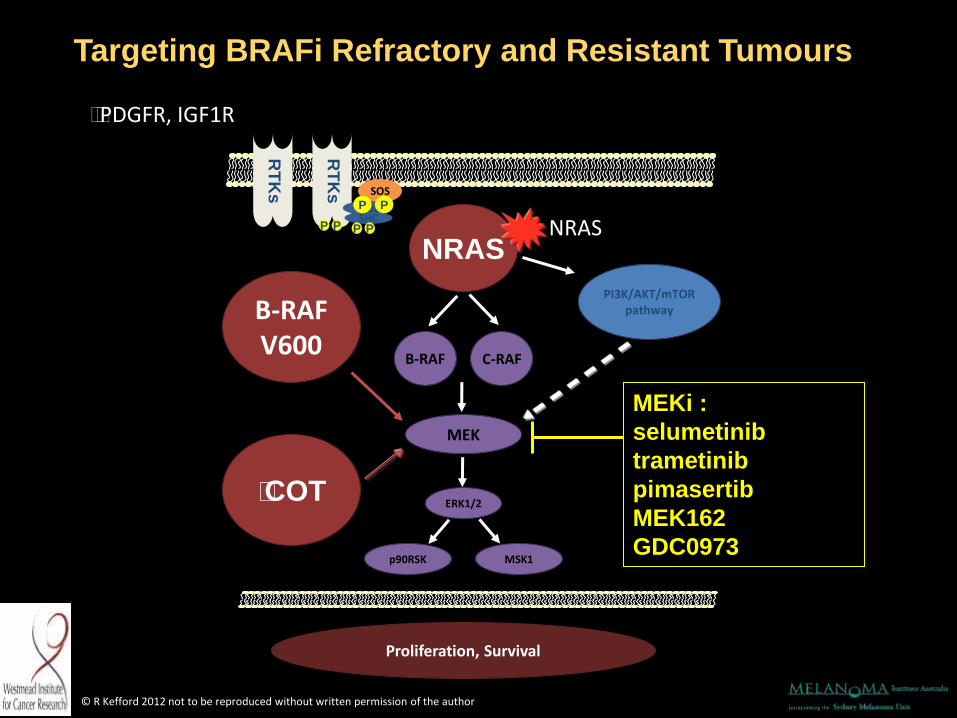
PI3K/AKT/mTOR pathway
RT
Ks
SOS
Grb2 SHC
P P P P
Proliferation, Survival
MEK
p90RSK MSK1
P P
B-RAF C-RAF
B-RAF V600
ERK1/2
NRAS NRAS
RT
Ks
PDGFR, IGF1R
COT
Targeting BRAFi Refractory and Resistant Tumours
MEKi :
selumetinib
trametinib
pimasertib
MEK162
GDC0973
© R Kefford 2012 not to be reproduced without written permission of the author
MEKi: What have we learnt?
MEKi: - SINGLE AGENT ACTIVITY AGAINST
MUT BRAF MELANOMA
PFS 4.8 mths
OS superior to chemo
WON’T SALVAGE BRAFi RESISTANCE
NRAS
BRAF
ERK
MITF
MEK
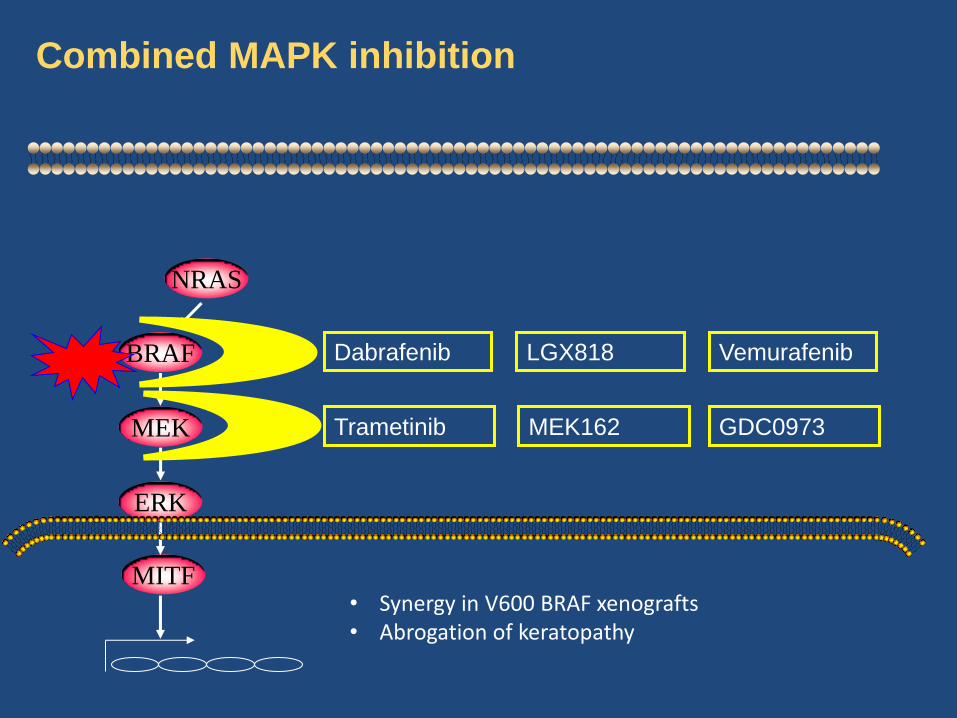
Combined MAPK inhibition
Dabrafenib
Trametinib
LGX818
MEK162
Vemurafenib
GDC0973
• Synergy in V600 BRAF xenografts • Abrogation of keratopathy
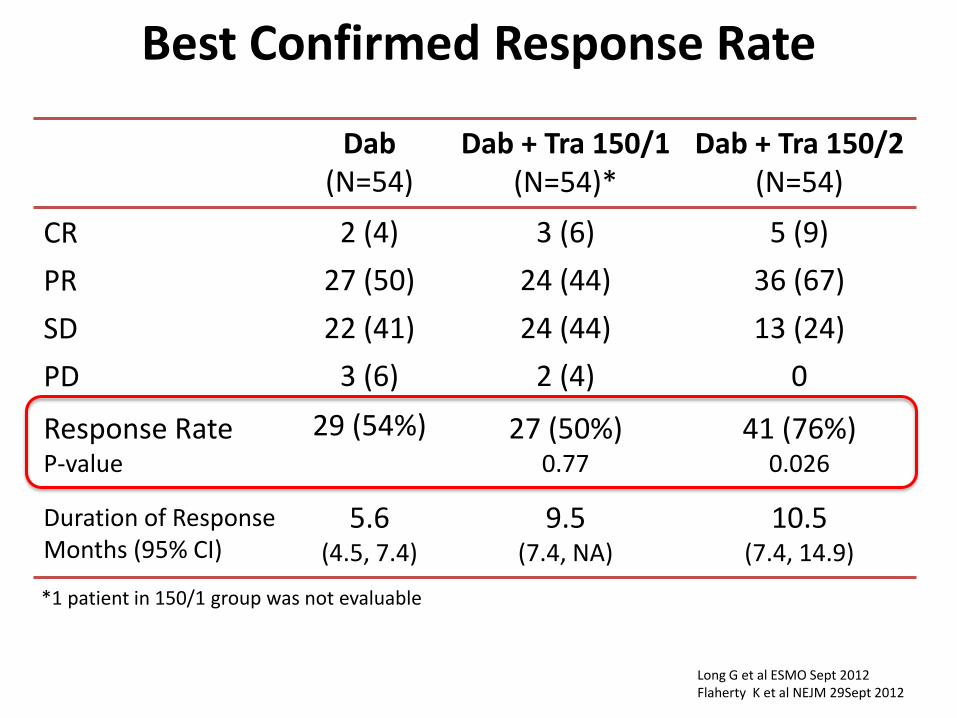
*1 patient in 150/1 group was not evaluable
Best Confirmed Response Rate
Dab (N=54)
Dab + Tra 150/1 (N=54)*
Dab + Tra 150/2 (N=54)
CR 2 (4) 3 (6) 5 (9)
PR 27 (50) 24 (44) 36 (67)
SD 22 (41) 24 (44) 13 (24)
PD 3 (6) 2 (4) 0
Response Rate P-value
29 (54%)
27 (50%) 0.77
41 (76%) 0.026
Duration of Response Months (95% CI)
5.6 (4.5, 7.4)
9.5 (7.4, NA)
10.5 (7.4, 14.9)
Long G et al ESMO Sept 2012 Flaherty K et al NEJM 29Sept 2012
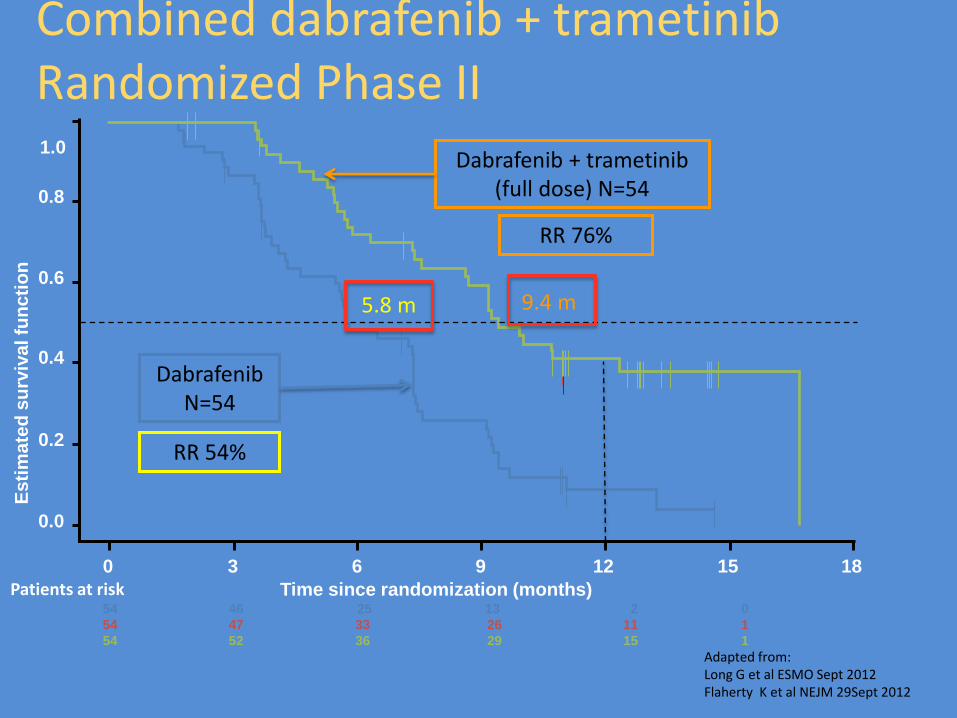
Es
tim
ate
d s
urv
iva
l fu
nc
tio
n
Patients at risk Time since randomization (months)
1.0
0.8
0.6
0.4
0.2
0.0
0 3 6 9 12 15 18
54 46 25 13 2 0
54 47 33 26 11 1
54 52 36 29 15 1
Adapted from: Long G et al ESMO Sept 2012 Flaherty K et al NEJM 29Sept 2012
Dabrafenib N=54
Dabrafenib + trametinib (full dose) N=54
Combined dabrafenib + trametinib Randomized Phase II
9.4 m 5.8 m
RR 54%
RR 76%
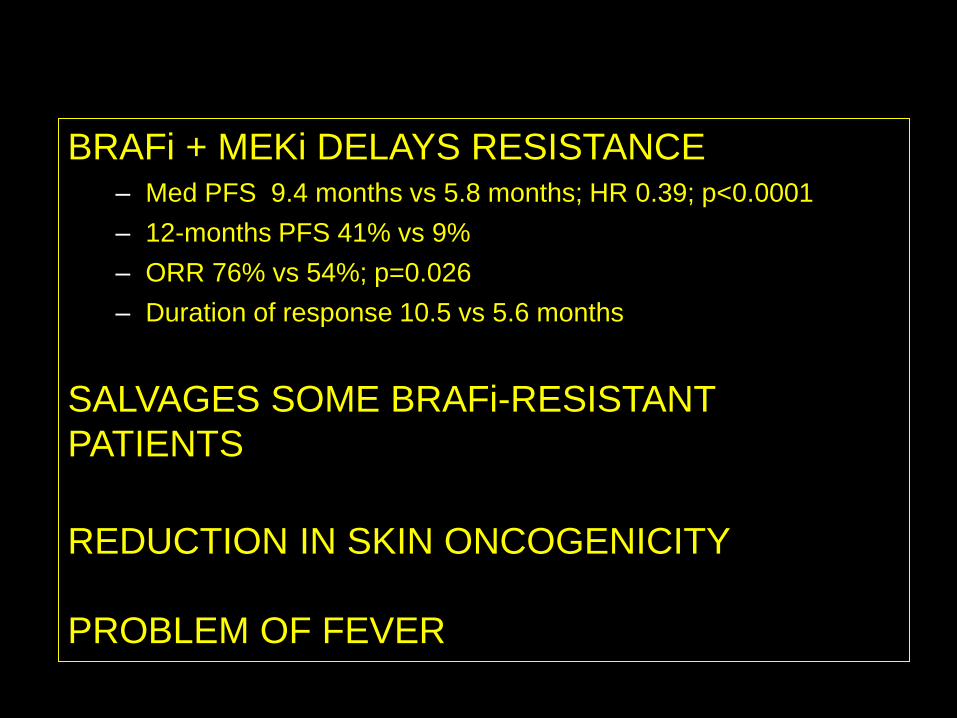
What have we learnt? BRAFi + MEKi DELAYS RESISTANCE
– Med PFS 9.4 months vs 5.8 months; HR 0.39; p<0.0001
– 12-months PFS 41% vs 9%
– ORR 76% vs 54%; p=0.026
– Duration of response 10.5 vs 5.6 months
SALVAGES SOME BRAFi-RESISTANT
PATIENTS
REDUCTION IN SKIN ONCOGENICITY
PROBLEM OF FEVER
Can We Combine Immunotherapy plus BRAFi?
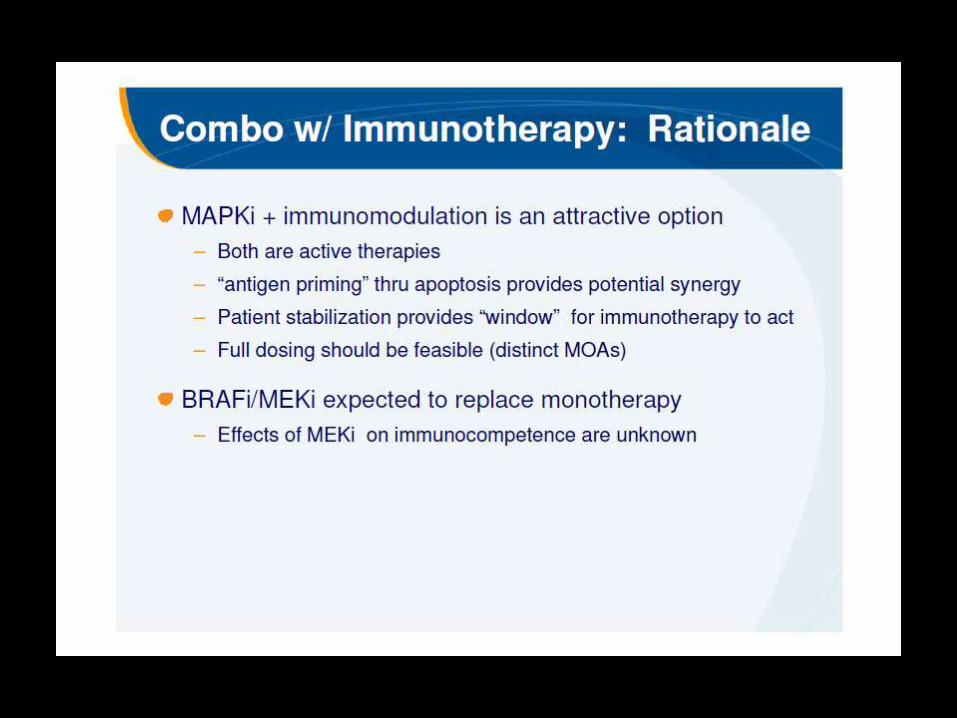
PRESENTED BY: Michael B. Atkins
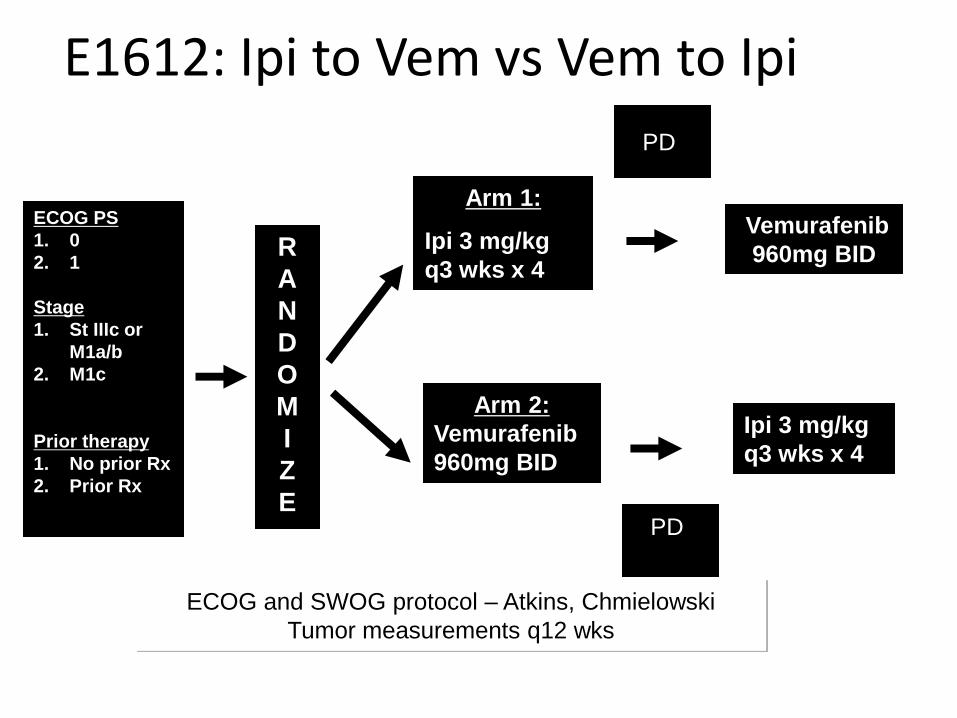
E1612: Ipi to Vem vs Vem to Ipi
ECOG PS
1. 0
2. 1
Stage
1. St IIIc or
M1a/b
2. M1c
Prior therapy
1. No prior Rx
2. Prior Rx
R
A
N
D
O
M
I
Z
E
Arm 1:
Ipi 3 mg/kg
q3 wks x 4
Arm 2:
Vemurafenib
960mg BID
ECOG and SWOG protocol – Atkins, Chmielowski
Tumor measurements q12 wks
Ipi 3 mg/kg
q3 wks x 4
Vemurafenib
960mg BID
PD
PD
CONCLUSIONS-MUCH TO BE EXCITED ABOUT
• Emphasis in treatment now on immunotherapy
• Need to understand why patients fail anti PD1
• What combinations should be investigated
• How do we select patients?
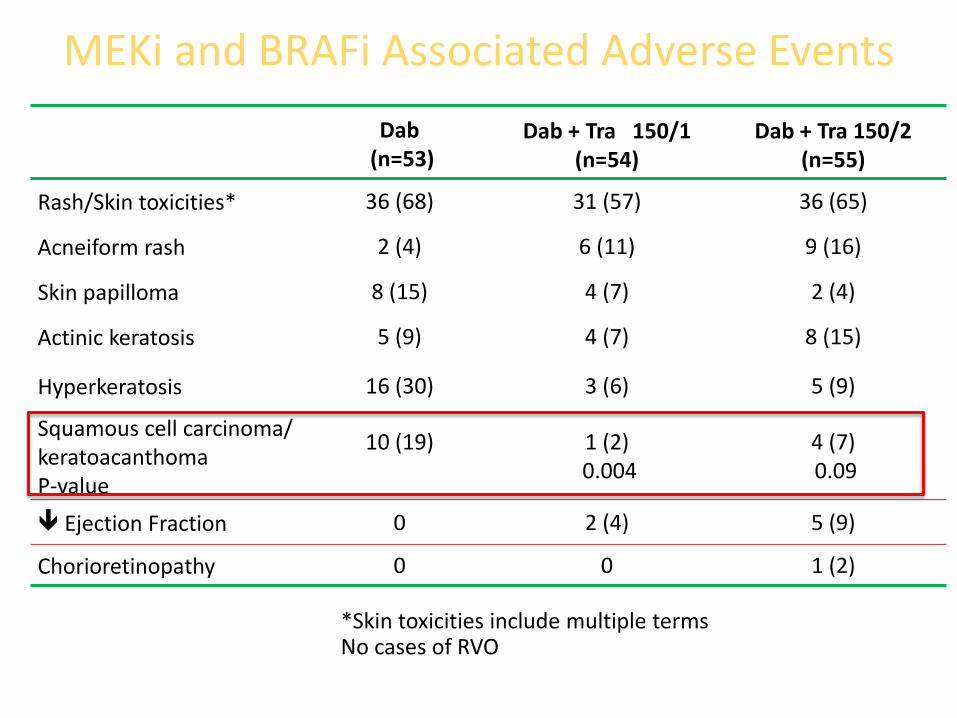
*Skin toxicities include multiple terms No cases of RVO
MEKi and BRAFi Associated Adverse Events
Dab (n=53)
Dab + Tra 150/1 (n=54)
Dab + Tra 150/2 (n=55)
Rash/Skin toxicities* 36 (68) 31 (57) 36 (65)
Acneiform rash 2 (4) 6 (11) 9 (16)
Skin papilloma 8 (15) 4 (7) 2 (4)
Actinic keratosis 5 (9) 4 (7) 8 (15)
Hyperkeratosis 16 (30) 3 (6) 5 (9)
Squamous cell carcinoma/ keratoacanthoma P-value
10 (19)
1 (2) 0.004
4 (7) 0.09
Ejection Fraction 0 2 (4) 5 (9)
Chorioretinopathy 0 0 1 (2)
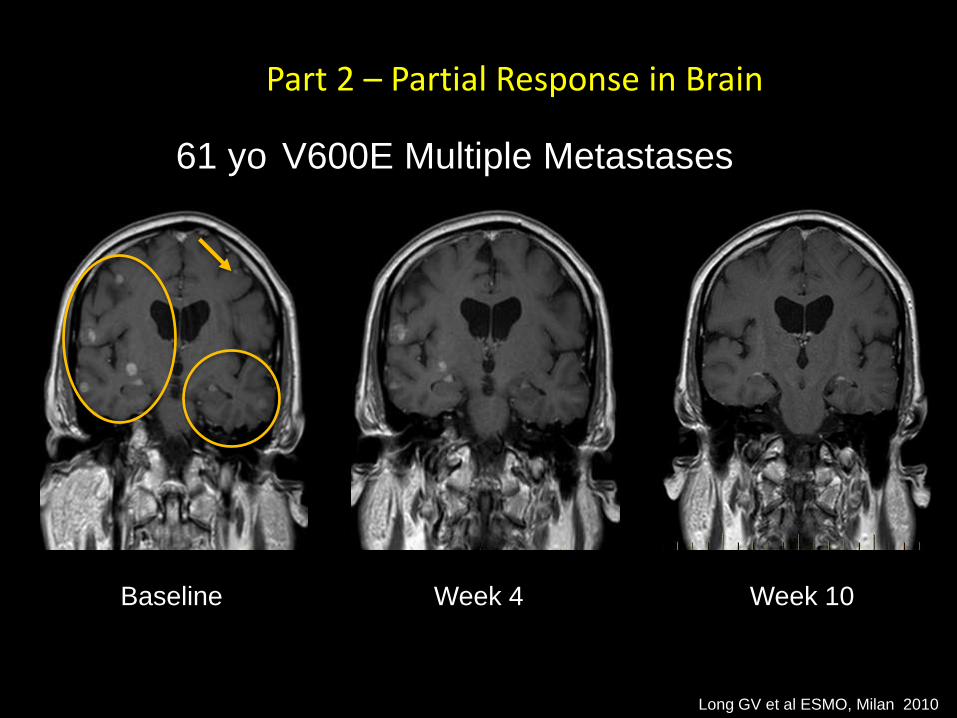
Part 2 – Partial Response in Brain
61 yo V600E Multiple Metastases
Baseline Week 4 Week 10
Long GV et al ESMO, Milan 2010
Max
imu
m p
erce
nt
chan
ge f
rom
b
ase
line
intr
acra
nia
l mea
sure
men
t
100
80
60
40
20
0
-20
-40
-60
-80
-100
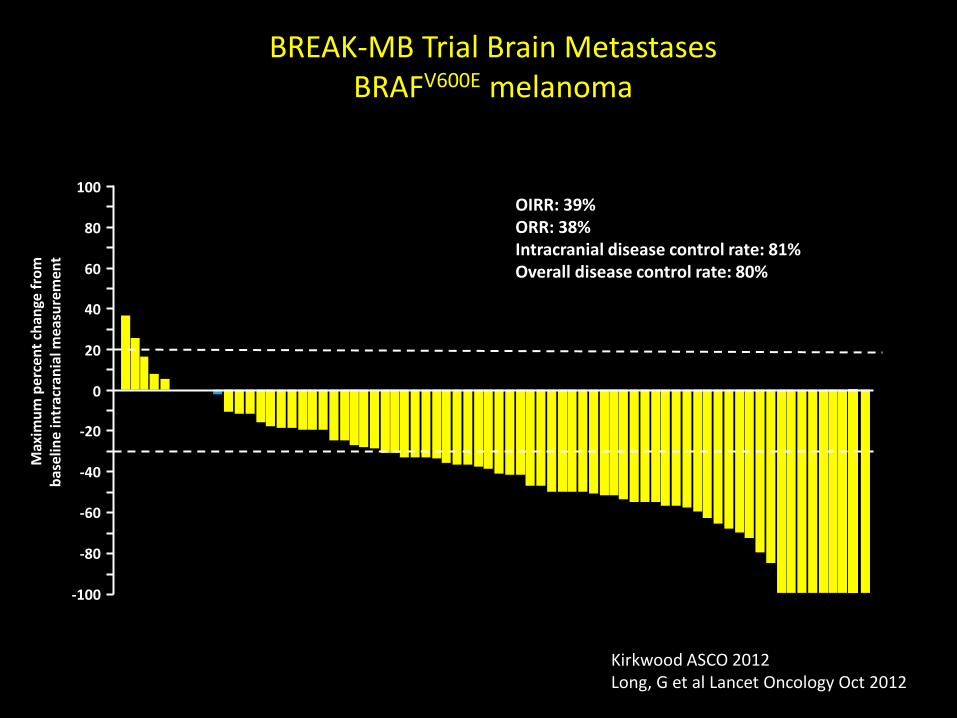
BREAK-MB Trial Brain Metastases BRAFV600E melanoma
No prior brain treatment
OIRR: 39% ORR: 38% Intracranial disease control rate: 81% Overall disease control rate: 80%
Kirkwood ASCO 2012 Long, G et al Lancet Oncology Oct 2012
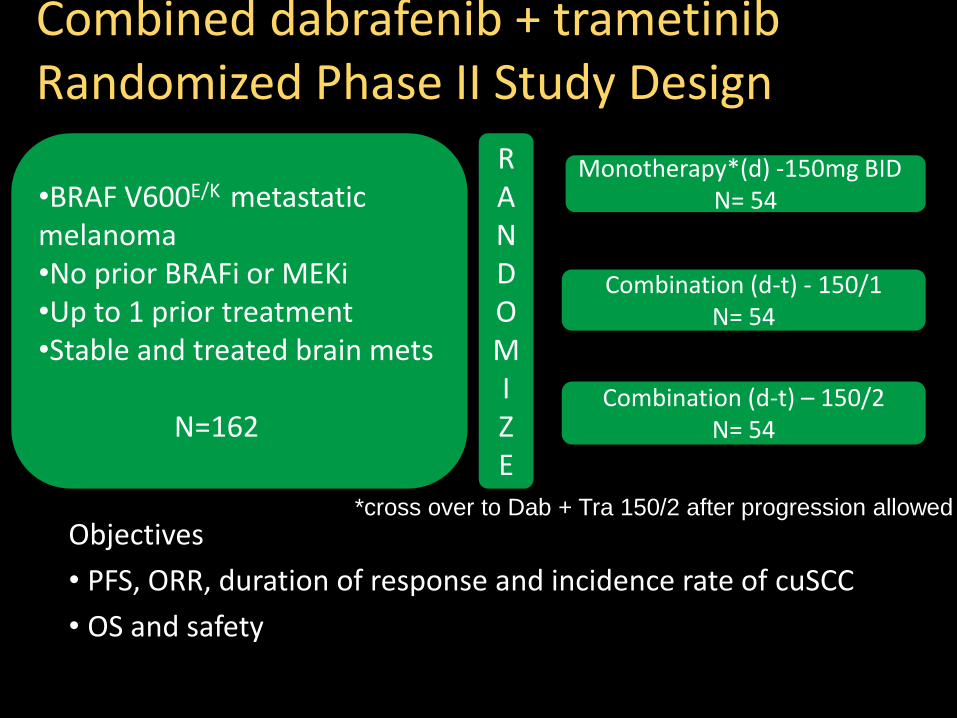
Combined dabrafenib + trametinib Randomized Phase II Study Design
Combination (d-t) – 150/2 N= 54
Combination (d-t) - 150/1 N= 54
RANDOMI Z E
•BRAF V600E/K metastatic melanoma •No prior BRAFi or MEKi •Up to 1 prior treatment •Stable and treated brain mets N=162
*cross over to Dab + Tra 150/2 after progression allowed
Objectives
• PFS, ORR, duration of response and incidence rate of cuSCC
• OS and safety
Monotherapy*(d) -150mg BID
N= 54
Long G et al ESMO Sept 2012 Flaherty K et al NEJM 29Sept 2012
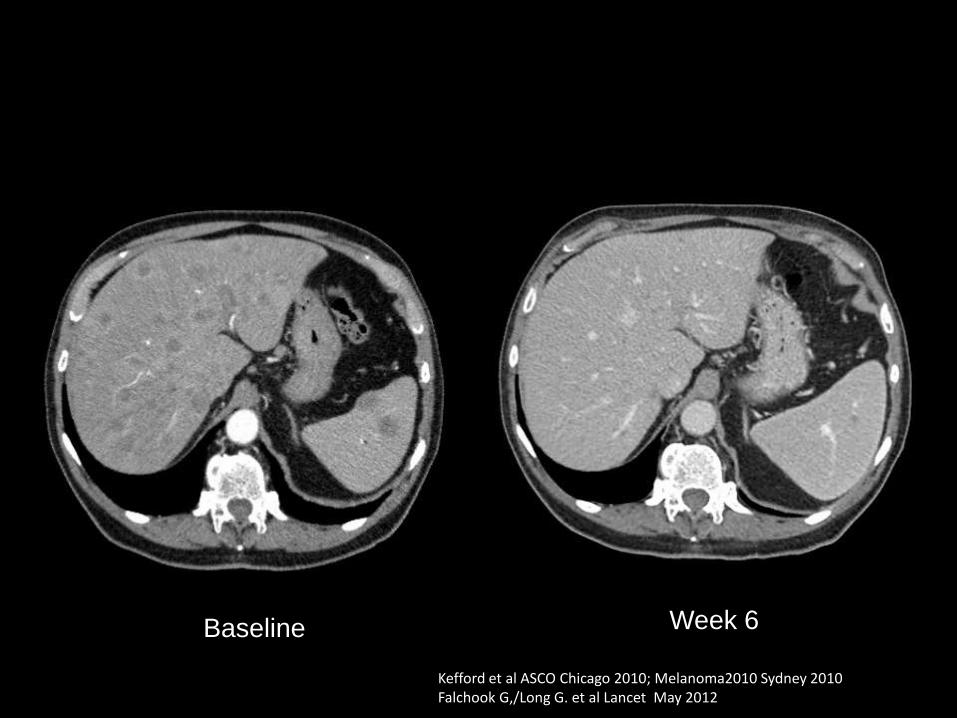
Baseline Week 6
Kefford et al ASCO Chicago 2010; Melanoma2010 Sydney 2010 Falchook G,/Long G. et al Lancet May 2012
M82 V600K Metastatic melanoma dabrafenib 150 mg bid


















![Ivyspring International Publisher Theranosticsantigens in melanoma has sparked hope in immunotherapy for melanoma treatment [28]. Tyrosinase-related protein-2 (TRP2) is an antigen](https://img.pdfslide.us/doc/110x75/60fb51d5e32fcb33e065fcbe/ivyspring-international-publisher-theranostics-antigens-in-melanoma-has-sparked.jpg)