Embed Size (px)
Citation preview

ava i l ab l e a t www.sc i enced i r ec t . com
www.e l sev i e r. com/ loca te /yc l im
Clinical Immunology (2008) 128, 294–305
SHORT ANALYTICAL REVIEW
Immunotherapy for neurological diseasesPablo Villoslada a,⁎, Beatriz Moreno a, Ignacio Melero b, Jose L. Pablos c,Gianvito Martino d, Antonio Uccelli e, Xavier Montalban f, Jesus Avila g,SergeRivest h, Laia Acarin i, StanleyAppel j, Samia J. Khoury k, PatrickMcGeer l,Isidro Ferrer m, Mario Delgado n, Jose Obeso a, Michal Schwartz o,⁎
a Department of Neuroscience, Center for Applied Medical Research, University of Navarra, Spainb Hepatology and Gene Therapy, Center for Applied Medical Research, University of Navarra, Spainc Servicio de Reumatología, Unidad de Investigación, Hospital 12 de Octubre, Madrid, Spaind Neuroimmunology Unit. Institute for Experimental Neurology (INSPE). San Raffaele Hospital, Milan, Italye Neuroimmunology Unit, Department of Neurosciences, Ophthalmology and Genetics, University of Genoa, Italyf Multiple Sclerosis Center of Catalonia, Vall d'Hebron University Hospital, Barcelona, Spaing Centro de Biología Molecular “Severo Ochoa”, Universidad Autónoma de Madrid, Spainh Laboratory of Molecular Endocrinology, CHUL Research Center and Department of Anatomy and Physiology, Laval University,Québec, Canadai Department of Cell Biology, Physiology and Immunology, Autonomous University of Barcelona, Spainj Department of Neurology, Methodist Neurological Institute, Houston, Texas, USAk Center for Neurologic Diseases, Department of Neurology, Brigham andWomen's Hospital and Harvard Medical School, Boston, MA, USAl Kinsmen Laboratory of Neurological Research, Department of Psychiatry, University of British Columbia, Vancouver, Canadam Institut Neuropatologia, IDIBELL-Hospital Universitari de Bellvitge, Hospitalet de LLobregat, Spainn Instituto de Parasitologia y Biomedicina, CSIC, Granada, Spaino The Weizmann Institute of Science, Rehovot, 76100, Israel
Received 5 February 2008; accepted with revision 9 April 2008Available online 4 June 2008
⁎ Corresponding authors. P. VillosladaMedical Research, University of Navarr
E-mail addresses: pvilloslada@unav
1521-6616/$ – see front matter © 200doi:10.1016/j.clim.2008.04.003
Abstract The burden of neurological diseases in western societies has accentuated the needto develop effective therapies to stop the progression of chronic neurological diseases. Recentdiscoveries regarding the role of the immune system in brain damage coupled with thedevelopment of new technologies to manipulate the immune response make immunotherapiesan attractive possibility to treat neurological diseases. The wide repertoire of immune responsesand the possibility to engineer such responses, as well as their capacity to promote tissue repair,indicates that immunotherapy might offer benefits in the treatment of neurological diseases,similar to the benefits that are being associated with the treatment of cancer and autoim-mune diseases. However, before applying such strategies to patients it is necessary to betterunderstand the pathologies to be targeted, as well as how individual subjects may respondto immunotherapies, either in isolation or in combination. Due to the powerful effects of the
KEYWORDSNeurological diseases;Immunotherapy;Cell therapy;Stem cells;Vaccination;Neuroprotection;Multiple sclerosis;Alzheimer disease;Parkinson disease;Amyotrophic lateralsclerosissclerosis
is to be contacted at Department of Neurology, Clinica Universitaria de Navarra and Center for Applieda, Pio XII 36, 31008 Pamplona, Spain. Fax: +34 948 296500. M. Schwartz, fax: +972 8 9346018..es (P. Villoslada), [email protected] (M. Schwartz).
8 Elsevier Inc. All rights reserved.

295Immunotheraphy in neurology
immune system, one priority is to avoid tissue damage due to the activity of the immune system,particularly considering that the nervous system does not tolerate even the smallest amount of tissuedamage.
© 2008 Elsevier Inc. All rights reserved.Introduction
Neurodegenerative diseases such as Alzheimer disease (AD),Parkinson disease (PD), Amyotrophic Lateral Sclerosis (ALS)and Multiple Sclerosis (MS) are among the most importanthealth problems in developed countries. Due to the progres-sive aging of the population in western countries, thefrequency of these diseases is reaching epidemic proportions,and they will cause an ever increasing social and economicburden on our societies. New treatments for AD are thebiggest priority due to it prevalence in the aging population.Indeed, except for MS there are currently no therapiesavailable to modify the progression of these diseases asexisting therapies only treat the symptoms. In recent years,progress has been made in developing new therapies thattarget the immune system, or treatments that use compo-nents of the immune system as therapeutic agents (Table 1and Fig. 1). Because the local immune response is sub-optimalor even destructive in neurodegenerative disease, it isreasonable to believe therapeutic immunomodulation mightbe beneficial in such circumstances.
An overview of immunotherapy
To date, immunotherapies have been tested in chronicconditions such as cancer and autoimmune diseases. Hence,the experience with these diseases will benefit any attemptsto develop immunotherapies for neurological diseases. Manydifferent cell types are involved in chronic inflammatorydiseases, including immune cells, endothelial cells andfibroblasts, reflecting the complexity of these diseases. Incancer, tumor cells are known to use multiple mechanisms toinduce immune tolerance in order to facilitate immuneevasion [1]. Indeed, tumor cells retain a complete copy ofthe human genome enabling them to fully exploit the rangeof immunomodulatory gene expression programs. Interest-ingly, it is becoming clear that many of the oncogenesresponsible for the transformation and maintenance oftumor cells are also connected with immunosuppression.Thus, the knowledge accumulated in cancer immunology canserve as a base to understand the progression of neurode-generative diseases, aiding in the development of immune-based therapies that use the same molecular tricks that helptumors to escape the cellular immune response. There areseveral mechanisms that can be employed to evade theimmune system, such as down modulating tumor antigenpresentation, releasing immunosuppressive substances intothe tumor microenvironment, disabling antigen presentingcells, inducing CD4 T cell tolerance, or enhancing theactivity of regulatory Tcells (Treg) [2]. Several immunother-apy approaches have been studied in cancer, includingtriggering immune responses against tumor antigens byvaccination, or by gene or cell therapy. Alternatively,boosting the immune response in a non-antigen specific
way has been contemplated, both by using cytokines orblocking the suppressor activity of CTLA4. Significantly,interference with the immunosuppressive strategiesadopted by the tumor seems to be essential for efficienttherapeutic results. After several attempts, some of theseimmunotherapies have now entered the clinical phase ofstudy and currently, there is a commercially availablevaccine against melanoma. Indeed, several reports haveindicated some success in controlling tumor cells in humanswith various vaccination approaches. However, unwantedside effects, such as the induction of vitiligo in patientstreated with an anti-CTLA4 antibody indicate that manip-ulation of the immune system must be carefully controlled[3]. The curative effect in cancer animal models of amonoclonal antibody directed against CD137 in mice appearsto result from a strong cytotoxic T cell response, and thisantibody is currently undergoing clinical trials [1]. Interest-ingly the same antibody ameliorates models of autoimmunediseases in mice, such as experimental autoimmune ence-phalomyelitis (EAE) [4], collagen induced arthritis andmurine lupus, through a mechanism that involves theinhibition of pathogenic CD4 T cells.
In the case of autoimmune diseases, the development ofnew immunotherapies for rheumatoid arthritis (RA) exempli-fies the opportunities offered by this approach [5,6]. Newimmunotherapies that have changed the natural history of RAinclude the use of antibodies against pro-inflammatory cyto-kines such as interleukin 6 (IL-6), interleukin 1 (IL-1) or tumornecrosis factor α (TNF-α), and CTLA 4 blocking strategies.Antibodies inhibiting IL-1 (Anakinra) and IL-6 (Tocilizumab)are effective in slowing disease activity and they are welltolerated by RA patients. TNF-α is a pleiotropic effectortarget due to its influence on multiple downstream pro-inflammatory pathways and given its regulatory role oneffector and regulatory Tcell activation. Anti-TNF (Infliximaband Adalimumab) and soluble TNF receptors (Etanercept) arealso widely used to treat RA. Abatacept is a CTLA4-Ig fusionprotein capable of blocking CD28-B7 co-stimulation and it hasrecently been approved for use in RA. Downregulating auto-antibody responses by depleting B cells with the anti-CD20antibody Rituximab has also been shown to be remarkableeffective in controlling the inflammatory process associatedwith RA and a variety of autoimmune diseases. However, whenconsidering the benefits of immunotherapy for autoimmunedisease wemust bear inmind that theymay have side effects,especially when used in combination, such as the suscept-ibility to opportunistic infections secondary to the potentimmunosuppression induced by combined therapy [7,8].
Protecting neural tissue by controlledautoimmunity — a paradigm shift?
Autoimmunity has long been viewed as a destructive processand numerous therapies have been developed to halt the

Table 1 Immunotherapy strategies for treating neurological diseases
Strategy Mechanisms of action Limitations Clinical use
Immunosuppression Blocks cell cycle, decreasingnumber and function of immunecells
Severe side effects: aplasia,immunodeficiency, bleedings,cardiopathy
Extensive in cancer andautoimmune diseases
Antibodies Block or enhance the activity of theligand
Neutralizing antibodies,anaphylaxis, prolongedimmunosuppression
Anti-TNF for RA, anti-VLA4 for MS,anti-Amyloid β in AD (under study)
Recombinantproteins
Activate specific receptor inducingimmunomodulatory effects
Neutralizing antibodies, sideeffects due to pleiotropicactivity.
Interferon-beta for MS,neurotrophic factors forneurodegenerative diseases (understudy)
Peptides Bind to the binding-site of specificreceptors and activate thedownstream pathway inducingimmunomodulation
Pleiotropic effects, Neutralizingantibodies?
VIP (under study)
Altered peptideligands
Bind the binding-site of specificreceptors stopping the signalingcascade or promoting anergy
Side effects due to agonisticeffects or pleiotropic activity
Glatiramer acetate for MS, MBPAPL(under study)
Vaccines Induce a phenotype bias in theimmune response to a morebeneficial one and promotescavenger and Neuroprotectiveactivity of the immune system
Inter-individual variability andunexpected side effects such asencephalomyelitis
Amyloid β or Tau vaccination forAD, synapsin vaccination for PD orBCG vaccine in MS (under study)
DNA vaccination Induces the expression of theencoded antigen in the musclepromoting the immune response
Loss of activity of gene expressionover time, low antigen levels orunexpected immune responses
MBP vaccination, TCR vaccinationfor MS (under study)
Cell therapy Induces immunomodulation,promoting neuroprotection andtheoretically inducing regenerationof the brain.
Induction of tumors or allogenicresponses
Neural stem cells, Mesenchymalstem cells, Schwan celltransplantation, Treg cells forseveral neurological diseases(under study)
Gene therapy Expression of an immunomodulatoryprotein by a resident cell typetransfected by a viral vector.
Induction of chronic infections,cancer, leukemia orimmunodeficiency
Cytokine and peptides gene therapyfor MS or trophic factor genetherapy for PD and HD (under study)
RNA interference Binds and induces the degradationof specific RNA, suppressing theactivity of the target gene in a dosedependent fashion
Difficulties in reaching targettissue, pleiotropic effects if thesequence is not specific or if thetarget gene is pleiotropic.
Interfering pro-inflammatorycytokines (under study)
Nanotechnology Nanodevices for reaching the brainand releasing immunomodulatoryand neuroprotective molecules orcontaining engineered cellsproducing trophic factors
Loss of efficacy, clotting adversereactions to foreign element
Encapsulation of trophic factorproducing cells for long-termsustained release (under study)
Small chemicals Target the intermediate metabolismwhich is critical for immune systemfunction
Side effects due to the pleiotropyof these function in other tissuesand pathways
Statins, kyneurins,Methylthioadenosine for MS,Minocycline for AD (under study)
296 P. Villoslada et al.
autoimmune process. However, there is evidence indicatingthat the immune response is beneficial rather than damagingafter brain damage [9]. The studies from Schwartz andcolleagues challenged the current dogma, suggesting thatautoimmune T cells can evoke a purposeful response neces-sary in CNS maintenance and repair (Fig. 2). This responseapparently effectively restores the balance when a smalldeviation from the homeostatic equilibrium occurs. In con-trast, a severe deviation such as an acute insult, stress orischemia, may lead to paralysis or chronic degeneration.Under such conditions either the evoked autoimmunity is
insufficient or alternatively, it is out of control and leads toautoimmune disease. In animals susceptible to autoimmunediseases, the same autoimmune T cells are responsible forboth neuroprotection and for disease development. Thetiming and strength of their activity will determine theeffect produced and if the immune response is wellcontrolled, T cell effectors could offer protection againstaxonal damage [9]. In the same way, the local innate immuneresponse coordinated by activated microglia/macrophagescan produce different phenotypes depending on the type ofactivation (Figs. 3 and 4). A more classic activation is

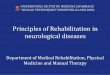
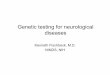
Figure 1 Therapeutic strategies for modulating the immuneresponse. Several steps in the immune response are critical andcan be targeted, such as: the innate immune response, T cellactivation, migration to tissues, and effector mechanisms. Fourstrategies are believed to play a significant role in treating braininflammation. A) Modulating the immune synapse and antigenpresenting cells. Possible alternatives to regulate antigenspecific response are included in the figure B) Cytokines andcytokine signaling. C) Cell therapy with Treg cells. D) Sparing oftarget organs reducing chronic inflammation, restoring thebrain-blood barrier and promoting tissue restoration, processesthat could be targeted in combination.
297Immunotheraphy in neurology
manifested by phagocytic activity, production of nitric oxide(NO) and other oxidation products that can damage neuronsat the site of the local immune response. Alternatively, whilephagocytic activity is maintained, activated microglia/macrophages may produce growth factors such as BDNF andIGF-I without provoking toxicity [10,11]. Accordingly, auto-immunity is naturally regulated to serve as a safety valve,
allowing injured individuals to benefit from protectiveautoimmunity without being exposed to the risk of develop-ing autoimmune diseases. However, certain circumstancesmay lead individuals to lose control of this beneficialautoimmune response. The concept of neuroprotectiveautoimmunity calls for therapeutic protocols for neurode-generative diseases to be revised, arguing in favor oftherapies based on immunomodulation rather than immuno-suppression. Such protocols would aim to maximize thebeneficial component of autoimmunity without eliminatingthe immune effect altogether. Boosting autoimmunity with-out provoking a risk of developing an autoimmune disease isthe treatment of choice and one option would be the use ofaltered peptide ligands [12].
Immunomodulatory therapies for MS
MS is a chronic inflammatory and neurodegenerative diseasefor which several immunomodulatory drug therapies havebeen established to try and control disease activity, includingInterferon-beta, Glatiramer acetate, chemotherapy andNatalizumab. Observational and head-to-head studies haveproduced controversial results regarding the degree ofefficacy of these products [13] and despite the efficiencyreported, a large proportion of patients do not respond totreatment [14,15]. Nevertheless, this information is usefulwhen considering the requirements of new treatments for MS,such as those being developed and those that adopt differentapproaches: therapies targeting T cell activation or migra-tion; those inducing immune deviation; or cell-based thera-pies. Some of the promising therapies that are currently beingassessed in phase III clinical trials include the use ofFingolimod, Rituximab, etc. Moreover, new therapeutic ap-proaches are being studied that are based on the immuno-pathogenesis of MS, trying to block the T cell co-stimulatorysignal, modulate the immune system by inhibiting inflamma-tory cytokines or vaccinating with brain antigens, adoptingmore neuroprotective strategies like restoring neuronal func-tion, or promoting remyelination and axonal regeneration.
A promising new strategy to modulate the immune systeminvolves targeting the intermediate metabolism. Statins,inhibitors of 3-Hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase, modulate autoimmune activity by down-regulating the class II major histocompatibility complexmolecules, co-stimulatory molecules and the Th1 cytokines,while pushing the immune response toward a Th2 response[16]. Indeed, in the initial clinical trials statins have shownpromise in reducing disease activity in MS [17]. Recentresearch indicates that catabolites of the essential aminoacid tryptophan can also modulate autoimmunity [18]. Thekynurenines, breakdown products of tryptophan, induce a Th2shift and suppress EAE. They decrease inflammation, as wellas reducing the expression of class II major histocompatibilitymolecules on microglia cells, and of co-stimulatory moleculeson T cells that infiltrate the brain [18]. Methylthioadenosine(MTA) is a lipophilic sulphur-containing adenine nucleosideproduced from S-adenosylmethionine during the synthesis ofthe polyamines. MTA has been shown to modulate theinflammatory response and MTA administration impairs thedevelopment of clinical signs in two models of EAE, acute EAEandmore importantly in chronic-relapsing EAE [19]. Themodeof action of MTA is likely to bemultifaceted, including a direct

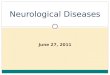
Figure 2 Brain damage can be prevented or regenerationenhanced by the immune system. T cells can migrate to areas ofbrain injury where they can release neuroprotective molecules orprovide helpful signals to resident cells, such as microglia andastrocytes, which protect and promote the recovery of the brain.Due to antigen-specificity and activation molecules, lymphocytescanmigrate to the brainwhere they can sense the functional stateof the tissue, due to information provided by microglia cells.There they may provide helpful signals to resident cells (micro-glia, astrocytes, bone-marrow immigrating cells) to promotetissue repair.
298 P. Villoslada et al.
antioxidant effect in vivo, modulation of T cell activation,down-regulation of pro-inflammatory cytokines, enhance-ment of interleukin 10 (IL-10) production and modulation ofNF-κB-mediated signaling [19]. The inhibition of methylationduring the activation of signaling pathways seems to beresponsible for such activity and this approach is becoming apowerful therapeutic strategy for several diseases. Indeed,recent studies using a synthetic drug that modulates methyla-tion, mimicking the activity of MTA, have also shown that it haspreventive and curative effect in the EAE model [20].
Other therapies for MS aim to modulate the immunetolerance via anti-inflammatory neuropeptides [21]. In thelast decade, various neuropeptides produced by immunecells that have potent anti-inflammatory activity were foundto participate in the maintenance of tolerance in differentimmunological disorders [21]. One of these neuropeptides isthe vasoactive intestinal peptide (VIP), and in a remitting-relapsing model of EAE, VIP reduced disease severity andincidence by inhibiting pro-inflammatory cytokines, activat-ing anti-inflammatory cytokines, inhibiting Th1 autoreactiveresponses and inducing Tr cells [22].
Over the past few years, several subsets of Treg cells havebeen identified, including natural CD4+CD25+Foxp3+ T cellsand acquired Treg cells such as Tr1 and Th3 [23]. Treg cellshave different mechanisms of action that include cell-contact suppression, production of immunosuppressive cyto-kines, niche competition mediated by interleukin 2 (IL-2),induction of regulatory antigen presenting cells (APC) andbystander suppression [23]. They might also mediateneuroprotection through the release of trophic factors andthe induction of a neuroprotective microglia phenotype. Allthese characteristics make these cells excellent candidatesto be used in cell therapy for MS as well as exerting theiractivity in diseases with less inflammation. Moreover, theactivity of Treg cells, including CD25+Foxp3+ and Tr1, isimpaired in MS and other autoimmune diseases [24,25] andthe this loss of activity is not reversed by immunomodulatorytherapy. Furthermore, not only is the suppressor function ofTreg cells impaired but also their effector signaling pathwaysare dysfunctional in MS, such as the IL-10 receptor pathway[25], indicating the presence of resistance against peripheralimmune tolerance mechanism in MS. Thus, cell therapiesusing Treg cells must recover these functions and theresponses of the different signaling pathways involved.
Under the neuroprotective autoimmunity paradigm, auto-immune T cells are on the alert to maintain the organismsdefenses against the ubiquitous agents of self-destruction.When a pathological situation arises such as that caused bytraumatic injury for example, intervention by the auto-immune T cells is needed urgently, although it is apparentlyinsufficient and must be boosted to be effective. Boostingcan be achieved by up-regulating the effector autoimmuneT cells by active immunization [26]. Indeed, it has recentlybeen demonstrated that immunization with a myelin-associated peptide modified to evoke a T cell-mediatedresponse without inducing EAE was beneficial to rats withoptic nerve or spinal cord injury [26]. Currently, severalclinical trials using the myelin basic protein altered peptideligand (APL) or a DNA vaccination strategy are under way[27]. However, previous experiences with APL have showncontrasting effects, including reactivation of MS [28]. Hence,the careful development of such therapies will be necessaryto avoid side effects, which can vary between patients due toindividual differences in the generation of the immuneresponse that in turn, depends on both the genetic back-ground and immune memory.
Therapeutic plasticity of neural stem cells andmesenchymal stem cells
Neural stem cells/precursor cells (NPCs) are a heterogeneouspopulation of mitotically-active, self-renewing, multipotentcells that exist in both the developing and the adult centralnervous system (CNS) that show complex spatio-temporalpatterns of gene expression [29]. NPCs can exert a thera-peutic effect by cell replacement but they can also promoteCNS repair through their intrinsic neuroprotective capacity,releasing neuroprotective agents at the site of tissue damagein a manner that is temporally and spatially adjusted tothe environmental needs. The neuroprotective moleculesinvolved may be immunomodulatory substances, neuro-trophic growth factors and/or stem cell regulators that are

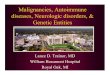
Figure 3 Heterogeneity of the microglial response to stimuli. Changes in microglial morphology in control animals (A), and followingmassive neuronal death induced by acute excitotoxicity resulting from the injection of an exogenous glutamate analogue into theimmature rat brain (B-H). Microglia are visualized using tomato lectin histochemistry (TL). Microglia display very rapid morphologicalchanges (B, 4 h post-lesion) and the fully developed response to injury involves reactive ramified forms (C) or ameboid to roundmicroglia/macrophagic morphologies (D), which express MHC class II (E) and several pro-inflammatory molecules like cyclooxygenase-2 (COX2) (F), interleukin 1 beta (IL-1β) (G) or interleukin-6 (IL-6) (H). A single immune stimulus (LPS) induces transient de novotranscriptional activation of the Toll-like receptor-2 (TLR2) in microglia (I, J) as demonstrated by Iba-1 immunohistochemistry (J, K).TLR2 is only induced when microglia cells are activated and this transcript is not expressed under basal conditions. Indeed, when thistranscript is induced in most case of acute immune stimuli, there is no neurodegeneration, suggesting that it might have aneuroprotective effect. Photographs courtesy of Prof. L. Acarin and S. Revest.
299Immunotheraphy in neurology

Figure 4 Neuroprotection mediated by activated microglia. Microglial activation induced by inflammatory mediators such as LPSinduced a more efficient removal of debris and recruitment of oligodendrocyte precursor cells (OPC), promoting the survival of myelinsheaths and neurons (reproduced by permission from Glezer I, Lapointe A, Rivest S. Innate immunity triggers oligodendrocyteprogenitor reactivity and confines damages to brain injuries. FASEB J. 2006 Apr; 20(6):750-2).
300 P. Villoslada et al.
constitutively expressed by NPCs to maintain tissue home-ostasis both during development and in adulthood. NPCsmight also induce apoptosis of inflammatory T lymphocytesby up-regulating the membrane expression of certaindeath receptor ligands, as triggered by pro-inflammatory(interferon γ, IFN-γ, IL-1β and TNF-α), but not anti-inflam-matory (IL-4, IL-5 and IL-13) cytokines. NPCs can alsopromote remyelination driven by endogenous oligodendro-cyte progenitors.
Recent studies of the intravenous or intra-cerebroven-tricular administration of syngenic NPCs in different mousemodels of MS demonstrated a clear therapeutic effect inboth chronic-progressive and relapsing-remitting EAE[30,31]. NPCs specifically enter the affected regions of theCNS where they promote a marked reduction in demyelina-tion, axonal loss and astrogliosis, accompanied by an almostcomplete restoration of neurological function. NPCs displaysuch a selective regional tropism for inflamed areas becausethey express a number of molecules that are also expressedby and that are important for the function of immune cells,such as the high-affinity cell adhesion molecules CD44 andthe very late antigen 4 (VLA-4). Again, the therapeutic po-tential of NPCs could be explained by cell replacement or,CNS repair may be promoted through a bystander effectexerted by the release of neuroprotective and immunomo-dulatory molecules at the site of tissue damage by undiffer-entiated “stem” cells in response to environmental stimuli.
Thus, the concept of “therapeutic plasticity” of NPCs re-flects the capacity of somatic stem cells to adapt their fateand functions to specific environmental needs as a result ofdifferent pathological conditions.
The bone marrow is composed of a stromal componentthat interacts closely with osteoblasts and endothelial cellsto create the proper microenvironment for the survival ofhaematopoietic stem cells. Such a stromal scaffold is formedby cells of mesenchymal origin, named mesenchymal multi-potent progenitor cells or mesenchymal stem cells (MSCs)because of their capacity to differentiate into multipletissues of a mesenchymal origin. MSCs can inhibit the pro-liferation of T, B and dendritic cells by inducing of the arrestof cell division [32]. MSCs can also inhibit the proliferation ofNK cells and impair dendritic cell maturation, as well asantigen presentation [32]. These features provide the con-ceptual support for their use in vivo in immune-mediateddiseases. Recently, MSCs were shown to ameliorate EAE,since their intravenous injection into mice immunized withthe 35–55 peptide of myelin oligodendrocyte glycoprotein(MOG) significantly improved the clinical severity of EAE,decreasing CNS inflammation and demyelination by inhibit-ing peripheral pathogenic Tcells [33]. Later, these data werefurther validated by demonstrating that MSC can alsoameliorate relapsing-remitting EAE and inhibit pathogenicantibodies [34]. Thus, the therapeutic benefits of MSCs donot arise through tissue repair sustained by regeneration of

301Immunotheraphy in neurology
damaged neurons and oligodendrocytes but instead, they aredue to the modulation of the autoimmune attack on myelin[35]. Moreover, MSCs are currently used in clinical practice totreat acute myocardial infarction, graft versus host disease,or Crohn's disease with no obvious side effects. Indeed, theycan be easily obtained from the bone marrow of the patient(autologous) or commercial preparations can even be used(allogenic). All these facts make MSCs a promising celltherapy in the short term, encouraging their use in patientswith neurological disease.
Neuroinflammation in neurodegenerativediseases: Targeting microglia andblood-born monocytes/macrophages
Microglia are the immune system cells resident in the CNSthat are in a continuous process of extension and retraction,even under normal conditions, providing permanent surveil-lance of the extracellular environment [36]. Followingchanges in the CNS parenchyma, like chronic or acute neuro-degeneration, microglia cells are activated and respond byundergoing morphological changes, migrating, proliferatingand changing their patterns of gene expression to augmentthe expression of inflammatory compounds such as cytokines,chemokines and their receptors. These are well-establishedfeatures of the innate immune response that is responsiblefor tissue repair in the periphery. However, far from beingstereotyped, the microglial response is highly dependent onthe CNS region, the type of insult, the degree of tissuedamage, the presence of neuronal debris, the state of theblood-brain barrier, and the presence or absence of animmune challenge triggering the immune adaptive response.Accordingly, recent evidence suggests that the microglialresponse can either have a protective or detrimental roledepending on the pathological condition and the context inwhich it develops (Figs. 3 and 4). Indeed, these cells are ableto display a large array of responses in order to maintain thehomeostatic equilibrium in the brain and to promote brainrepair [37]. Microglia can impede the invasion of infectiousagents, provide trophic support and protection to neurons,eliminate neurons that are irreversible destined to die, andassist in glial scar formation and tissue repair. However,excessive, chronic or unregulated microglia activation maybe harmful to neurons.
In this sense, microglia are becoming one of the mainimmunotherapeutic targets for neurological diseases, andseveral approaches are under study to target the activationof microglia. Anti-inflammatory therapies, such as the useof non-steroidal anti-inflammatory drugs (NSAIDs) that canantagonize the neurotoxic products of scavengers, antago-nists of reacting-oxygen species (ROS), NO and inflam-matory compounds seem to provide neuroprotection indifferent pathologies [38,39]. However, these neurotoxicproducts are neither exclusively produced by microglia/macrophages nor do they constitute a unique feature of themicroglia cell response. Thus, neuroprotective strategiesshould target individual facets of the microglial response inorder to modulate the activation of this cell type ratherthan deplete its activity, which may be devastating dueto the diminished phagocytosis and deregulation of theinflammatory response [40], among other factors. Accord-
ingly, in certain experimental models it has been suggestedthat neuroprotection can be achieved in conjunction withincreased microglial activation. New strategies, like Toll-like receptor (TLR) subtype deficiencies can produceselective reduction of lesion-induced cytokine and chemo-kine expression, as well as delayed T cell recruitment andmicroglia proliferation in several experimental injuries[41].
Immunotherapy for Alzheimer andParkinson disease
Senile plaques and neurofibrillary tangles are the pathologi-cal hallmarks of AD. Plaque material consists mostly ofextracellular aggregates of beta-amyloid protein (Aβ), whilethe neurofibrillary tangles mostly consist of intracellularaggregations of phosphorylated tau. Severe inflammationdevelops around both the extracellular Aβ deposits and neu-rofibrillary tangles, and activatedmicroglia produce a varietyof toxic material, including free oxygen radicals and pro-teases. Accordingly, therapeutic strategies should be direc-ted at reducing the level of inflammation and to achieve this,the toxic effects of over stimulated microglia should beattenuated. This is the presumed role of anti-inflammatoryagents, including NSAIDs, whose main effect is to inhibit thecyclooxygenase (COX) activity that is up-regulated in ADmicroglia cells, although they can also target severalsecretases involved in the amyloid cascade [42]. In multipleepidemiological studies, NSAIDs have been found to amelio-rate AD and they reduce behavioral and pathological deficitsin transgenic models of AD in a dose dependent manner.
Many of the highly ramified microglia found within thecore of amyloid plaques in the transgenic mouse models ofAD originate from the bone marrow, and the β-amyloid 40and 42 isoforms are able to trigger this chemoattraction.These newly recruited cells also exhibit a specific immunereaction to both exogenous and endogenous β-amyloid in thebrain, as well as having the ability to eliminate amyloiddeposits by a cell-specific phagocytic mechanism. The factthat newly recruited blood-born monocytes are more effi-cient than their resident immune cell counterparts is clearlybeneficial in restricting the progression of AD. Thus, a novelstrategy to improve such a process and target it towards β-amyloid deposits could lead to the elimination of toxic senileplaques by bone marrow stem cells capable of differentiatinginto microglia in the CNS. These cells might also be modifiedto express trophic factors and amyloid precursor proteindegrading enzymes [43].
An independent therapeutic strategy, with the same goalof recruiting blood-born monocytes, thereby minimizingplaque formation and encouraging cell renewal, has beenapplied using Tcell- based vaccination in a double transgenicAD mouse model. The approach is based on the concept of‘protective autoimmunity', whereby Tcells recognizing brainproteins are needed for CNS maintenance, repair and re-newal under conditions where the levels, timing andphenotypes are well controlled [12]. In an AD mousemodel, boosting the levels of T cells that can weekly cross-react with brain antigens using Glatiramer acetate reducedplaque formation and cognitive loss, while enhancingneurogenesis [10]. The underlying mechanism was

302 P. Villoslada et al.
associated with the modulation of the microglia/macro-phage phenotype associated with the plaques [10] and therecruitment of blood-born monocytes locally expressingthis phenotype.
Another important aspect of AD treatment is the preven-tion of Aβ misfolding and the disruption of Aβ aggregationthrough different approaches, including the use of selectivesmall molecules, synthetic peptides, chaperones and Aβbinding proteins, as well as Aβ immunization. Immunizationwith Aβ peptides and vaccination with antibodies against Aβhave emerged as important strategies to treat AD, both aimedat reducing Aβ aggregation and the burden of β-amyloidplaques [44]. In terms of improved behavior and reducedplaque formation positive results were obtained followingactive and passive Aβ immunization in AD transgenic mice.Pioneering trials in moderate AD cases showed a variableclinical improvement and a decrease in the β-amyloidplaques with this approach, although β-amyloid angiopathyand the hyperphosphorylated tau pathology were main-tained. However, this trial was stopped due to the appear-ance ofmeningoencephalitis in a subset of patients as a resultof T cell-mediated immune responses in addition to theexpected antibody-related immune response [45]. Theseresults prompted the development of new approaches aimedat reducing the side effects, such as encephalitis andmicrohemorrhages, and at optimizing immunization. Differ-ent approaches geared to optimizing immunization have beenadopted by engineering phages expressing specific peptides.In an attempt to reduce the adverse effects, recombinantadeno-associated viral Aβ vaccine expressing a fusion proteincontaining Aβ1-42 and the cholera toxin B subunit wasassayed in a mouse model of AD [46]. Immunization resultedin reduced behavioral impairment and a reduction in thenumber of Aβ cortical plaques in transgenic mice [46].Together, such experimental designs have defined Aβimmunization as a potent therapeutic tool in the early stagesof the disease, either when administered alone or moreprobably, in combination with other drugs [47].
Tau phosphorylation and aggregation also participates inAD. Tau is a microtubule-associated protein that accumu-lates in a phosphorylated and aggregated form not only inAD, but also in other pathologies known as tauopathies.Analyzing the role of tau phosphorylation and tau aggrega-tion in a transgenic mouse overexpressing GSK-3beta andFTDP-17 tau, phosphorylation of tau but not its aggregationappears to be involved in the cognitive impairment found inthis model [48]. Recent studies indicate that immunizationwith amyloid-beta has a positive effect in transgenic mousemodels of AD by reducing the levels of pathological tau [49].This represents a challenge since tau is mainly intracellular,suggesting that tau immunotherapy might work by stimulat-ing neuroprotective autoimmunity.
Parkinson disease (PD) is a CNS disease that produces severedifficulties in movement control and cognitive impairment,and current therapies are aimed at restoring dopaminergicactivity in the brain [50]. PD is characterized by the presenceof intracytoplasmic inclusions or protein aggregates calledLewy bodies and the depletion of pigmented DA-containingneurons in the substantia nigra pars compacta. Several factorsare believed tobe involved in the pathogenesis of PD, includinginflammation. The COX enzyme, as well as inflammatorymediators such as NO are thought to be increased in PD and
indeed, the non-selective COX inhibitor, Aspirin, and thepreferential COX-2 inhibitor, Meloxicam, seems to conferneuroprotection in 1-methyl-4-phenyl-1,2,3,6-tetrahydropyr-idine (MPTP)-induced DA depletion in mice [51]. Tetracyclinederivatives are other anti-inflammatory agents that offerneuroprotection in experimental models of PD. As such,minocycline treatment inhibits iNOS and NADPH oxidaseexpression, modulates the microglial response and preventsthe degeneration of dopamine containing neurons induced byMPTP [52]. VIP can also act by blocking microglial activationand through a neuroprotectiveeffect in theMPTPmousemodel[53]. The involvement of abnormal α-synuclein (α-syn) foldingin the pathogenesis of PD suggests that immunization withhuman α-synmight represent a potential therapy. Accordingly,human α-syn transgenic mice were vaccinated with human α-syn todemonstrate that the vaccination is effective in reducingneuronal accumulation of human α-syn aggregates, whichmaybe further developed to treat PD [54]. Glatiramer acetate wasalso tested in MPTPmice, producing an accumulation of Tcellswithin the substantia nigra pars compacta, suppression ofmicroglial activation, and increased local expression ofastrocyte-associated glial cell line-derived neurotrophic fac-tor. This immunization resulted in significant protection ofnigrostriatal neurons against MPTP neurodegeneration [55].However, the value of these experimental findings to predictthe potential of its therapeutic application for patientswith PDis questionable. Indeed, animal models may not faithfullymimic the pathology of PD in terms of pattern and rate of celldeath, and Lewy bodies do not actually form. Significantly, therole of Lewy body formation (i.e. protective or deleterious) inthe pathogenesis of PD is still not clear.
Immunotherapy forAmyotrophic Lateral Sclerosis
ALS is a neurodegenerative disease that affects adult motorneurons. A small proportion of familial cases are caused bydominant mutations in the ubiquitously expressed Cu2+/Zn2+
superoxide dismutase (SOD1), which has led to the generationof transgenic models of ALS. The only currently availabletherapy for this devastating disease is Riluzole, which slightlymodifies the disease course. Thus, developing new therapiesthat can halt the evolution of ALS is a priority. Recent studiessuggest that microglia also play an important role in thisdisease contributing to motorneuron injury in animal modelsof familial ALS [56]. Indeed, the expression of mutant SODmicroglia in the CNS contributes to motorneuron injury.Compared with wild type microglia, the mutant cells produceand release more superoxide and nitrite, and they inducedmore neuronal death [57]. Hence, microglia act as a double-edged sword, highlighting the importance of targetingmicroglia to minimize cytotoxicity and maximize neuropro-tection in neurodegenerative diseases. Several attempts havebeen made to target neuroinflammation in ALS. For example,Glatiramer acetate (only when used in a specific regimen andspecific adjuvant), and other formulations and variants of theoriginal compound, can ameliorate the disease course inanimal models of ALS [58]. Importantly, the use of Glatirameracetate without adjuvant in a regime that was effective inanimal models of AD [10], was not effective in mouse modelsof ALS. For this reason, a clinical trial with Glatiramer acetateshould not be commenced until the regime has been carefully

303Immunotheraphy in neurology
selected. The regime that is effective in MS patients (dailyinjection of Glatiramer acetate) was only mildly effective inmale mice suffering from ALS and it was destructive in theirfemale counterparts (M Schwartz, in preparation). Otherstrategies are being tested, such as the inhibition of the keymediator of inflammation, COX-2. Rofecoxib, administeredby intraperitoneal injection in the SOD1 (G93A G1H) mousemodel induced a small but significant delay in locomotorimpairment, however survival was not effected by thetreatment [59]. Despite all these positive experimentalresults, we have to be careful before proposing anti-inflammatory therapies in ALS patients, since modulatingthe innate immune system in the brain has failed to changethe outcome of different mouse models of ALS [60]. Moreover,inhibiting pro-inflammatory signaling (e.g., MyD88) in bonemarrow-derived microglia might dramatically acceleratedisease progression in SOD1 (G37R) mice (Kang and Rivest,submitted).
Conclusions
Immunotherapies are powerful strategies to treat chronicdiseases. However, to apply these approaches we mustbetter understanding the involvement of the immunesystem in the pathogenesis of neurological diseases. Thecapacity of the immune system to target damaged tissueand restore the integrity of the tissue provides an excellentopportunity to treat patients suffering chronic and dis-abling brain diseases. However, several considerationsneed to be satisfied before immunotherapies can be con-sidered. First, the treatment of choice should be carefullyselected and we must consider differences betweenindividuals in terms of the immune system response inorder to predict the response to therapy and to identifypatients at risk of developing side effects. Second, inaddition to modulating the immune response, immu-notherapies might have a well-defined neuroprotectiveeffect. Third, we must be careful when combining ther-apies due to the unexpected alterations of the immunesystem that may compromise its normal function, leadingto adverse events. Finally, the same compound may notwork in all neurodegenerative diseases or alternatively, thesame compound may only be effective for different dis-eases under distinct regimes, since the precise immuneresponse may depend on the dose and timing of treatment.Thus, although neurodegenerative diseases share a char-acteristic malfunctioning of the immune response, whichmay serve as a therapeutic target, the way to achieve itsuch modifications should be carefully selected for eachseparate disease in order to maximize the benefits fromimmunotherapies and reduce the risk of side effects.Finally, treatments should be applied as early as possibleto maximize their potential therapeutic value. This byitself represents a challenge in the treatment of neurode-generative diseases.
Disclosure and conflict of interest
PV has received travel grants and speaker's honoraria fromBiogen, Aventis, Serono, and Teva. IM has received consultantfees and from Pfizer, Bristol Myers Squibb and Digna Biotech.
AU has received travel grants and consulting honoraria fromBiogen-Dompè, MerckSerono, Genetech, BayerSchering,Sanofi-Aventis. XM has received travel grants and speaker'shonoraria from Biogen, Aventis, Serono, and Teva. SM hasreceived personal compensation for consulting with PDL,Repligen, Biogen Idec, Argos, LifeCycle, Daiichi Suntori, andCytochroma. JO has served ocassionally as adviser forNovartis Pharmaceutical, Glaxo Smith Kline, BoehringerIngelheim and Eli Lilly. BM, JLP, GM, LA, SR, SA, MS, PM, IF,JA, MD have no conflict of interest.
Acknowledgments
This review is based in a symposium organized in May 2007by the Fundacion Ramon Areces, Madrid, a non-profit organization dedicated to promote scientific research(http://www.fundacionareces.es/).
References
[1] I. Melero, S. Hervas-Stubbs, M. Glennie, D.M. Pardoll, L. Chen,Immunostimulatory monoclonal antibodies for cancer therapy,Nat. Rev., Cancer 7 (2) (2007) 95—106.
[2] R. Kim, M. Emi, K. Tanabe, K. Arihiro, Tumor-driven evolution ofimmunosuppressive networks during malignant progression,Cancer Res. 66 (11) (2006) 5527—5536.
[3] G. Suntharalingam, M.R. Perry, S. Ward, S.J. Brett, A. Castello-Cortes, M.D. Brunner, N. Panoskaltsis, Cytokine storm in a phase1 trial of the anti-CD28 monoclonal antibody TGN1412, N. Engl.J. Med. 355 (10) (2006) 1018—1028.
[4] Y. Sun, X. Lin, H.M. Chen, Q. Wu, S.K. Subudhi, L. Chen, Y.X. Fu,Administration of agonistic anti-4-1BB monoclonal antibodyleads to the amelioration of experimental autoimmuneencephalomyelitis, J. Immunol. 168 (3) (2002) 1457—1465.
[5] J.S. Smolen, G. Steiner, Therapeutic strategies for rheumatoidarthritis, Nat. Rev. Drug Discov. 2 (6) (2003) 473—488.
[6] I. Gutierrez-Canas, Y. Juarranz, B. Santiago, et al., VIP down-regulates TLR4 expression and TLR4-mediated chemokineproduction in human rheumatoid synovial fibroblasts, Rheuma-tology (Oxford) 45 (5) (2006) 527—532.
[7] O. Stuve, C.M. Marra, P.D. Cravens, et al., Potential risk ofprogressive multifocal leukoencephalopathy with natalizumabtherapy: possible interventions, Arch. Neurol. 64 (2) (2007)169—176.
[8] J. Kaiser, Gene therapy. Questions remain on cause of death inarthritis trial, Science 317 (5845) (2007) 1665.
[9] M. Schwartz, J. Kipnis, Protective autoimmunity and neuro-protection in inflammatory and noninflammatory neurode-generative diseases, J. Neurol. Sci. 233 (1–2) (2005)163—166.
[10] O. Butovsky, M. Koronyo-Hamaoui, G. Kunis, E. Ophir, G. Landa,H. Cohen, M. Schwartz, Glatiramer acetate fights againstAlzheimer's disease by inducing dendritic-like microglia expres-sing insulin-like growth factor 1, Proc. Natl. Acad. Sci. U. S. A.103 (31) (2006) 11784—11789.
[11] O. Butovsky, S. Bukshpan, G. Kunis, S. Jung, M. Schwartz,Microglia can be induced by IFN-gamma or IL-4 to express neuralor dendritic-like markers, Mol. Cell. Neurosci. 35 (3) (2007)490—500.
[12] Y. Ziv, H. Avidan, S. Pluchino, G. Martino, M. Schwartz, Synergybetween immune cells and adult neural stem/progenitor cellspromotes functional recovery from spinal cord injury, Proc.Natl. Acad. Sci. U. S. A. 103 (35) (2006) 13174—13179.

304 P. Villoslada et al.
[13] X. Montalban, MS treatment: postmarketing studies, J. Neurol.Sci. 23 (2007) 23.
[14] E. Waubant, S. Vukusic, L. Gignoux, F.D. Dubief, I. Achiti, S.Blanc, C. Renoux, C. Confavreux, Clinical characteristics ofresponders to interferon therapy for relapsing MS, Neurology 61(2003) 184—189.
[15] P. Villoslada, J.R. Oksenberg, J. Rio, X. Montalban, Clinicalcharacteristics of responders to interferon therapy for relap-sing MS, Neurology 62 (9) (2004) 1653.
[16] S. Youssef, O. Stuve, J.C. Patarroyo, et al., The HMG-CoAreductase inhibitor, atorvastatin, promotes a Th2 bias and re-verses paralysis in central nervous system autoimmune disease,Nature 420 (6911) (2002) 78—84.
[17] T. Vollmer, L. Key, V. Durkalski, et al., Oral simvastatintreatment in relapsing-remitting multiple sclerosis, Lancet363 (9421) (2004) 1607—1608.
[18] M. Platten, P.P. Ho, S. Youssef, et al., Treatment of autoimmuneneuroinflammation with a synthetic tryptophan metabolite,Science 310 (5749) (2005) 850—855.
[19] B. Moreno, H. Hevia, M. Santamaria, et al., Methylthioadenosinereverses brain autoimmune disease, Ann. Neurol. 60 (3) (2006)323—334.
[20] B.R. Lawson, Y. Manenkova, J. Ahamed, X. Chen, J.P. Zou, R.Baccala, A.N. Theofilopoulos, C. Yuan, Inhibition of trans-methylation down-regulates CD4 T cell activation and curtailsdevelopment of autoimmunity in a model system, J. Immunol.178 (8) (2007) 5366—5374.
[21] E. Gonzalez-Rey, A. Chorny, M. Delgado, Regulation of immunetolerance by anti-inflammatory neuropeptides, Nat. Rev.,Immunol. 7 (1) (2007) 52—63.
[22] E. Gonzalez-Rey, M. Delgado, Vasoactive intestinal peptideand regulatory T-cell induction: a new mechanism andtherapeutic potential for immune homeostasis, Trends Mol.Med. 26 (2007) 26.
[23] W. Zou, Regulatory T cells, tumour immunity and immunother-apy, Nat. Rev., Immunol. 6 (4) (2006) 295—307.
[24] C. Baecher-Allan, D.A. Hafler, Human regulatory T cells andtheir role in autoimmune disease, Immunol. Rev. 212 (2006)203—216.
[25] I. Martinez-Forero, R. Garcia-Munoz, A. Martinez, et al., IL-10suppressor activity and ex vivo Tr1 cell function are impaired inMultiple Sclerosis, Eur. J. Immunol. 38 (2) (2008) 576—586.
[26] E. Hauben, E. Agranov, A. Gothilf, U. Nevo, A. Cohen, I.Smirnov, L. Steinman, M. Schwartz, Posttraumatic therapeuticvaccination with modified myelin self-antigen prevents com-plete paralysis while avoiding autoimmune disease, J. Clin.Invest. 108 (4) (2001) 591—599.
[27] A. Bar-Or, T. Vollmer, J. Antel, et al., Induction of antigen-specifictolerance in multiple sclerosis after immunization with DNA en-coding myelin basic protein in a randomized, placebo-controlledphase 1/2 trial, Arch. Neurol. 64 (10) (2007) 1407—1415.
[28] B. Bielekova, B. Goodwin, N. Richert, et al., Encephalitogenicpotential of themyelin basic protein peptide (amino acids 83–99)in multiple sclerosis: results of a phase II clinical trial with analtered peptide ligand, Nat. Med. 6 (10) (2000) 1167—1175.
[29] N.B. Ivanova, J.T. Dimos, C. Schaniel, J.A. Hackney, K.A. Moore,I.R. Lemischka, A stem cell molecular signature, Science 298(5593) (2002) 601—604.
[30] S. Pluchino, A. Quattrini, E. Brambilla, et al., Injection of adultneurospheres induces recovery in a chronic model of multiplesclerosis, Nature 422 (6933) (2003) 688—694.
[31] S. Pluchino, L. Zanotti, B. Rossi, et al., Neurosphere-derivedmultipotent precursors promote neuroprotection by an immu-nomodulatory mechanism, Nature 436 (7048) (2005) 266—271.
[32] A. Uccelli, L. Moretta, V. Pistoia, Immunoregulatory functionof mesenchymal stem cells, Eur. J. Immunol. 36 (10) (2006)2566—2573.
[33] E. Zappia, S. Casazza, E. Pedemonte, et al., Mesenchymal stemcells ameliorate experimental autoimmune encephalomyelitisinducing T-cell energy, Blood 106 (5) (2005) 1755—1761.
[34] E. Gerdoni, B. Gallo, S. Casazza, et al., Mesenchymal stem cellseffectively modulate pathogenic immune response in experimen-tal autoimmune encephalomyelitis, Ann. Neurol. 61 (3) (2007)219—227.
[35] A. Uccelli, V. Pistoia, L. Moretta, Mesenchymal stem cells: a newstrategy for immunosuppression? Trends Immunol. 28 (5) (2007)219—226.
[36] G. Raivich, Like cops on the beat: the active role of restingmicroglia, Trends Neurosci. 28 (11) (2005) 571—573.
[37] I. Glezer, A.R. Simard, S. Rivest, Neuroprotective role of theinnate immune system bymicroglia, Neuroscience 23 (2007) 23.
[38] A. Klegeris, P.L. McGeer, Non-steroidal anti-inflammatory drugs(NSAIDs) and other anti-inflammatory agents in the treatmentof neurodegenerative disease, Curr. Alzheimer Res. 2 (3) (2005)355—365.
[39] L. Acarin, B. Gonzalez, B. Castellano, Decrease of proinflam-matory molecules correlates with neuroprotective effect of thefluorinated salicylate triflusal after postnatal excitotoxicdamage, Stroke 33 (10) (2002) 2499—2505.
[40] M. Lalancette-Hebert, G. Gowing, A. Simard, Y.C. Weng, J. Kriz,Selective ablation of proliferating microglial cells exacerbatesischemic injury in thebrain, J.Neurosci. 27 (10) (2007) 2596—2605.
[41] S. Lehnardt, S. Lehmann, D. Kaul, et al., Toll-like receptor 2mediates CNS injury in focal cerebral ischemia, J. Neuroimmu-nol. 190 (1–2) (2007) 28—33.
[42] A. Lleo, E. Galea, M. Sastre, Molecular targets of non-steroidalanti-inflammatory drugs in neurodegenerative diseases, Cell.Mol. Life Sci. 20 (2007) 20.
[43] A.R. Simard, D. Soulet, G. Gowing, J.P. Julien, S. Rivest, Bonemarrow-derived microglia play a critical role in restricting senileplaque formation in Alzheimer's disease, Neuron 49 (4) (2006)489—502.
[44] E.G. McGeer, P.L. McGeer, Abeta immunotherapy and othermeans to remove amyloid, Curr. Drug Targets CNS Neurol.Disord. 4 (5) (2005) 569—573.
[45] D.S. Gelinas, K. DaSilva, D. Fenili, P. George-Hyslop, J.McLaurin, Immunotherapy for Alzheimer's disease, Proc. Natl.Acad. Sci. U. S. A. 101 (Suppl 2) (2004) 14657—14662.
[46] J. Zhang, X. Wu, C. Qin, et al., A novel recombinant adeno-associated virus vaccine reduces behavioral impairment andbeta-amyloid plaques in a mouse model of Alzheimer's disease,Neurobiol. Dis. 14 (3) (2003) 365—379.
[47] J.A. Nicoll, E. Barton, D. Boche, et al., Abeta species removalafter abeta42 immunization, J. Neuropathol. Exp. Neurol. 65(11) (2006) 1040—1048.
[48] T. Engel, J.J. Lucas, F. Hernandez, J. Avila, A mouse model tostudy tau pathology related with tau phosphorylation andassembly, J. Neurol. Sci. 13 (2007) 13.
[49] S. Oddo, L. Billings, J.P. Kesslak, D.H. Cribbs, F.M. LaFerla,Abeta immunotherapy leads to clearance of early, but not late,hyperphosphorylated tau aggregates via the proteasome,Neuron 43 (3) (2004) 321—332.
[50] C.W. Olanow, J.A. Obeso, F. Stocchi, Continuous dopamine-receptor treatment of Parkinson's disease: scientific rationaleand clinical implications, Lancet Neurol. 5 (8) (2006) 677—687.
[51] FB, P. Teismann, Inhibition of the cyclooxygenase isoenzymesCOX-1 and COX-2 provide neuroprotection in the MPTP-mousemodel of Parkinson's disease, Synapse 39 (2) (2001) 167—174.
[52] D.C. Wu, V. Jackson-Lewis, M. Vila, et al., Blockade ofmicroglial activation is neuroprotective in the 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine mouse model of Parkinsondisease, J. Neurosci. 22 (5) (2002) 1763—1771.
[53] M. Delgado, D. Ganea, Neuroprotective effect of vasoactiveintestinal peptide (VIP) in a mouse model of Parkinson's disease

305Immunotheraphy in neurology
by blocking microglial activation, FASEB J. 17 (8) (2003)944—946.
[54] RE, E. Masliah, A. Adame, M. Alford, L. Crews, M. Hashimoto, P.Seubert, M. Lee, J. Goldstein, T. Chilcote, D. Games, D.Schenk, Effects of alpha-synuclein immunization in a mousemodel of Parkinson's disease, Neuron 46 (6) (2005) 857—868.
[55] E.J. Benner, R.L. Mosley, C.J. Destache, et al., Therapeuticimmunizationprotects dopaminergic neurons inamousemodel ofParkinson's disease, Proc. Natl. Acad. Sci. U. S. A. 101 (25) (2004)9435—9440.
[56] A.M. Clement, M.D. Nguyen, E.A. Roberts, et al., Wild-typenonneuronal cells extend survival of SOD1 mutant motorneurons in ALS mice, Science 302 (5642) (2003) 113—117.
[57] D.R. Beers, J.S. Henkel, Q. Xiao, et al., Wild-type microgliaextend survival in PU.1 knockout mice with familial amyotrophic
lateral sclerosis, Proc. Natl. Acad. Sci. U. S. A. 103 (43) (2006)16021—16026.
[58] D.N. Angelov, S. Waibel, O. Guntinas-Lichius, et al., Therapeu-tic vaccine for acute and chronic motor neuron diseases:implications for amyotrophic lateral sclerosis, Proc. Natl. Acad.Sci. U. S. A. 100 (8) (2003) 4790—4795.
[59] PC, M.F. Azari, M.R. Le Grande, E.C. Lopes, J. Hirst, S.Petratos, S.S. Cheema, Effects of intraperitoneal injection ofRofecoxib in a mouse model of ALS, Eur. J. Neurol. 12 (5) (2005)357—364.
[60] M.D. Nguyen, J.P. Julien, S. Rivest, Induction of proin-flammatory molecules in mice with amyotrophic lateralsclerosis: no requirement for proapoptotic interleukin-1beta in neurodegeneration, Ann. Neurol. 50 (5) (2001)630—639.







![Laboratory Tests in Neurological Diseases [Stunents Cpoy]](https://img.pdfslide.us/doc/110x75/55cf8557550346484b8cfb2b/laboratory-tests-in-neurological-diseases-stunents-cpoy.jpg)