Embed Size (px)
Citation preview

ImmunopharmacologyDr. Alia Shatanawi
16-12-2019

Cytokines• Cytokines are soluble, antigen-nonspecific signalling proteins that bind to cell surface receptors on a variety of cells.
The term cytokine includes
• Interleukins (ILs) • Interferons (IFNs) •Tumor necrosis factors (TNFs) •Transforming growth factors •Colony-stimulating factors

Immunosuppressive Agents
• Clinical Uses: –Organ transplantation. –Autoimmune Disorders. –Isoimmune Disease, e.g. hemolytic disease of newborn.
–Prevention of cell proliferation, e.g. coronary stents, neovascular macular degeneration.

Immunosuppressive Agents
• Glucocorticoids. • Calcineurin Inhibitors. • Proliferation Signal Inhibitors. • Mycophenolate Mofetil. • Thalidomide. • Cytotoxic Agents. • Immunosuppresive Antibodies. • Monoclonal antibodies.

Glucocorticoids
• First hormonal agents recognized as having lympholytic properties.
• Cytotoxic to certain subsets of T cells. • Decrease antibody responses. • Increase catabolic rate of IgG. • Have additional antinflammatory and antiallergic activities. • Used in a variety of conditions. • Have their own toxicities.

Actions of Glucocorticoids• Glucocorticoids suppress the cell-mediated immunity. inhibiting genes that code for the cytokines, the most important of which is IL-2.
• Smaller cytokine production reduces the T cell proliferation.
• Glucocorticoids also suppress the humoral immunity, causing B cells to express smaller amounts of IL-2 and IL-2 receptors.
• Cellular immunity is more affected than humoral immunity.
• Anti-inflammatory effects

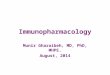
Glucocorticoids Regulate Transcription
GR, glucocorticoid receptor; HSP, heat shock protein; IP, immunophilin;GRE, glucocorticoid receptor
Cortisol
GR HSPHS PIP
CortisolGR
Cortisol
GRCortisol
GRE
NUCLEUS
mRN A
Proteins mRN A
↑ transcription (eg, lipocortin)or
↓transcription (IL-1, IL-2,TNF- α, IF- γ)GR
Cortisol

Clinical Uses of Glucocorticoids
• First-line immunosuppressive therapy for: – Solid organ – Hematopoietic stem cell transplant recipients – Graft-versus-host disease (GVHD).
• Idiopathic thrombocytopenic purpura and rheumatoid arthritis.
• Bronchial asthma. • Premedication for agents (e.g. blood products, and drugs)
known to cause undesirable immune responses.

Side Effects to Glucocorticoids • Immunodeficiency • adrenal glands • Hyperglycemia and abnormal Fat redistribution • Growth failure, delayed puberty. • Excitatory effects on central nervous system
(euphoria, psychosis) • Osteoporosis • Cataract • Gastric irritation and ulceration.

Buffalo Hump

Dr. Shatanawi 2012
Moon Face

Drugs affecting IL-2These drugs can be further divided into three main classes:
A. Calcineurin inhibitors (cyclosporine and tacrolimus)
B. Co-stimulation blockers (belatacept)
C. mTOR inhibitors (sirolimus and everolimus)


• Activate natural killer cells, macrophages, and cytotoxic T lymphocytes
• Interleukin -2: a growth factor • Stimulates the proliferation of antigen-primed (helper) T
cells
produce more IL-2, IFN-γ, and TNF-α.
Cytokines: IL-2
14


NFATc: cytosolic Nuclear Factor of Activated T cells

Cyclosporine• Mechanism of action: suppresses cell-mediated immune reactions, whereas humoral immunity is affected to a far lesser extent.
• Cyclosporine binds to a cyclophilin . • The formed Complex binds to calcineurin .
• Calcineurin : is responsible for dephosphorylating NFATc.
• The end result is a decrease in IL-2, which is the primary chemical stimulus for increasing the number of T lymphocytes.

Therapeutic Uses• To prevent rejection of kidney, liver, and cardiac allogeneic
transplants • Combined in a double-drug or triple-drug regimen with • 1.Corticosteroids • 2. antimetabolite such as Mycophenolate mofetil.
• Cyclosporine may also be used for recalcitrant psoriasis.

Pharmacokinetics• Cyclosporine may be given either orally or by intravenous (IV)
infusion. • Oral absorption is variable due to metabolism by a cytochrome
P450 (CYP3A4) isoenzyme in the gastrointestinal (GI) tract and efflux by P-glycoprotein (P-gp)
• Cyclosporine is extensively metabolized, primarily by hepatic CYP3A4.
• Excretion of the metabolites is primarily through the biliary route into the feces.

Adverse Effects
• Nephrotoxicity (dose dependant) …most common >>>>Be careful of drug combinations
• Hepatotoxicity
• In patients taking cyclosporine, infections are common and may be life threatening.

Cyclosporine• Nephrotoxicity. • Hypertension. • Hyperglycemia. • Liver dysfunction. • Hyperkalemia. • Altered mental status, seizures. • Hairsutism. • Gum hyperplasia • Lymphoma and other cancers (Kaposi's sarcoma,
skin cancer) due to induction of TGF-β.

Cyclosporin Monitoring Parameters• Cyclosporine trough levels.
• Serum electrolytes.
• Renal function.
• Hepatic function.
• Blood pressure.
• Serum cholesterol.

Tacrolimus• MOA: binds immunophilin, FKBP-12 (FK-binding protein) • Also calcineurin inhibitor, is a macrolide that is isolated from
the soil fungus Streptomyces tsukubaensis. • This drug is preferred over cyclosporine because of its
1.increased potency
2. decreased episodes of rejection
3. Steroid sparing effects

NFATc: cytosolic Nuclear Factor of Activated T cells


Therapeutic Uses• preventing liver and kidney rejections (along with
glucocorticoids). • It is also used in heart and pancreas transplants and rescue
therapy in patients after failure of standard rejection therapy.
• An ointment preparation is approved for moderate to severe atopic dermatitis unresponsive to conventional therapies.

Pharmacokinetics• Orally or IV.
• The oral route is preferable, but absorption is incomplete and variable, requiring tailoring of doses.
• Tacrolimus is subject to gut metabolism by CYP3A4/5 isoenzymes and is a substrate for P-gp. Bioavailability ?!
• Absorption is decreased if the drug is taken with high-fat or high-carbohydrate meals.
• The drug and its metabolites are primarily eliminated in the feces.

Adverse Effects• Nephrotoxicity and neurotoxicity (tremor, seizures, and hallucinations) more severe than with cyclosporine
• Development of posttransplant insulin-dependent diabetes mellitus is a problem, especially in black and Hispanic patients.
• Other toxicities are similar to cyclosporine, except that tacrolimus does not cause hirsutism or gingival hyperplasia, but it can cause alopecia.
• lower incidence of cardiovascular toxicities, such as hypertension and hyperlipidemia

Belatacept
• Costimulation blocker ( 2nd Generation), is a recombinant fusion protein that targets signal 2 in the immune activation cascade. It is used for long-term maintenance immunosuppressive therapy.

NFATc: cytosolic Nuclear Factor of Activated T cells

Mechanism of Action
Belatacept blocks CD28-mediated costimulation of T lymphocytes (signal 2) by binding to CD80 and CD86 on APCs. This prevents the downstream stimulatory signals promoting T-cell survival, proliferation, and IL-2 production.

Therapeutic Uses• kidney transplantation in combination with basiliximab,
mycophenolate mofetil, and corticosteroids.
• This drug can take the place of the calcineurin inhibitors in an effort to avoid the detrimental long-term cardiovascular, metabolic, and renal complications
• Note: The first-generation costimulation blocker abatacept is approved for rheumatoid arthritis.

Pharmacokinetics• The first IV maintenance immunosuppressant and is dosed in
two phases. • The initial high-dose phase is administered on a more frequent
interval. • In the maintenance phase, the dose is decreased and
administered once a month. • Monthly dosing may be beneficial in patients for whom
medication compliance is an issue. • Belatacept clearance is not affected by age, sex, race, renal,
or hepatic function.

Adverse Effects• Belatacept increased the risk of post-transplant
lymphoproliferative disorder (PTLD), particularly of the central nervous system. Therefore, it is contraindicated in those patients who have never been exposed to the Epstein-Barr virus (EBV), a common cause of PTLD.
• Common adverse events include : • Anemia • Diarrhea • Urinary tract infection, • Edema.

Proliferation Signal Inhibitors(PSIs)• Sirolimus( Rapamycin). • Everolimus. • Bind the circulating immunophylline FK506-binding
protein12. • Instead of forming a complex with calcineurin,
sirolimus binds to mTOR (a serine/threonine kinase), interfering with signal 3.
–The complex inhibits interleukin-driven T-cell and B-cell proliferation as well as immunoglobulin production.

mTOR proteinsToR proteins are essential for many cellular functions, such as cell cycle progression, DNA repair, and as regulators involved in protein translation.
Binding of sirolimus to mTOR blocks the progression of activated T cells from the G1 to the S phase of the cell cycle and, consequently, the proliferation of these cells Unlike cyclosporine and tacrolimus, sirolimus does not lower IL-2 production but, rather, inhibits the cellular response to IL-2.

37


• Available for oral and topical administration.
• Approved for use in renal transplantation, in combination with
cyclosporine and corticosteroids
• Sirolimus-eluting coronary stents: The antiproliferative action
of sirolimus is also valuable in cardiology where sirolimus-
coated stents are used to inhibit restenosis of the blood vessels
by reducing proliferation of the endothelial cells.
• Everolimus also indicated second-line treatment in patients with
advanced renal cell carcinoma.
• Sirolimus( Rapamycin)& Everolimus.

Adverse effects
• A common adverse effect of sirolimus is hyperlipidemia (elevated cholesterol and triglycerides), which may require treatment.
• The combination of cyclosporine and sirolimus is more nephrotoxic
• Others: headache, nausea and diarrhea, leukopenia, and thrombocytopenia.
• Impaired wound healing ……obese patients and those with diabetes.

Pharmacokinetics• The drug is available as an oral solution or tablet.
• Although it is readily absorbed, high-fat meals can decrease the absorption. • Sirolimus has a long half-life (57 to 62 hours), allowing for once-daily
dosing. • A loading dose is recommended at the time of initiation of therapy. • Like both cyclosporine and tacrolimus, sirolimus is metabolized by the
CYP3A4 isoenzyme, is a substrate for P-gp, and has similar drug interactions.
• Sirolimus also increases the concentrations of cyclosporine, and careful blood level monitoring of both agents must be done to avoid harmful drug toxicities.

Everolimus• Everolimus is rapidly absorbed, but absorption is decreased with
high-fat meals. Everolimus is a substrate of CYP3A4 and P-gp and, thus, is subject to the same drug interactions
• It has a much shorter half-life than sirolimus and requires twice-daily dosing.
• Everolimus increases drug concentrations of cyclosporine, thereby enhancing the nephrotoxic effects of cyclosporine, and is, therefore, recommended to be used with reduced doses of cyclosporine.

Everolimus side effects• An additional adverse effect noted with everolimus is
angioedema, which may increase with concomitant use of angiotensin-converting enzyme inhibitors.
• There is also an increased risk of kidney arterial and venous thrombosis, resulting in graft loss, usually in the first 30 days posttransplantation.

Cytotoxic Agents• Azathioprine. • Cyclophosphamide. • Leflunomide. • Hydroxychloroquine • Others:
– Vincristine. – Vinblastine – Methotrxate. – Cytarabine. – Pentostatin.

Azathioprine• The first agent to achieve widespread use in organ transplantation.
• It is a prodrug that is converted first to 6-mercaptopurine (6-MP) and then to the corresponding nucleotide, thioinosinic acid.

46TMPT: Thiopurine methyltransferase
TPMT
Gertrude B. Elion

Azathioprine• The immunosuppressive effects of azathioprine are due to this nucleotide analog.
• Because of their rapid proliferation in the immune response and their dependence on the de novo synthesis of purines required for cell division, lymphocytes are predominantly affected by the cytotoxic effects of azathioprine.
• Its major nonimmune toxicity is bone marrow suppression.

Azathioprine • Prodrug of mercaptopurine. • Metabolized by Xanthine oxidase (so dose is
reduced when given with allopurinol) . • Antimetabolite: interferes with purine
nucleic acid metabolism, and consequently will destroy and inhibit lymphoid cell proliferation stimulated by antigens.
• Blocks cellular immunity as well as primary and secondary serum antibody responses.

Azathioprine • Used in renal allograft, acute
glomerulonephritis, SLE, RA, Crohn’s Disease, MS, and ITP.
• Toxicity: – Bone marrow suppression. – Skin rashes, fever. – N, V, D. – Hepatic dysfunction and jaundice.

Azathioprine • Used in renal allograft, acute
glomerulonephritis, SLE, RA, Crohn’s Disease, MS, and ITP.
• Toxicity: – Bone marrow suppression. – Skin rashes, fever. – N, V, D. – Hepatic dysfunction and jaundice.

Drug Interactions• Concomitant use with angiotensin-converting enzyme inhibitors
or cotrimoxazole in renal transplant patients can lead to an exaggerated leukopenic response.
• Allopurinol, an agent used to treat gout, significantly inhibits the metabolism of azathioprine. Therefore, the dose of azathioprine must be reduced. Nausea and vomiting are also encountered.

Cyclophosphamide.• Alkylating agent. • Destroys proliferating lymphoid cells. • Alkylates some resting cells. • Large doses can induce an apparent specific
tolerance to a new antigen if the drug is administered simultaneously with, or shortly after, the antigen.
• Toxicity: Pancytopenia, hemorrhagic cystitis, N, V, cardiac toxicity, electrolyte disturbances.

Mycophenolate mofetil• Replaced azathioprine because of its safety and efficacy in prolonging graft survival.
• Uses: heart, kidney, and liver transplants. • As an ester, it is rapidly hydrolyzed in the GI tract to mycophenolic acid.
• This is a potent, reversible, noncompetitive inhibitor of inosine monophosphate dehydrogenase, which blocks the de novo formation of guanosine phosphate.
• Deprives proliferating T and B cells of a key component of nucleic acids.

MYCOPHENOLATE○ More effective than Azathioprine in preventing acute rejection ○It is used in combination with cyclosporine and prednisolne ○Mycophenolate mofetil is used in solid organ transplant patients for refractory rejection and,
○In combination with prednisone, as an alternative to cyclosporine or tacrolimus in patients who do not tolerate those drugs. ○In renal transplants, it’s used with low-dose cyclosporine to reduced cyclosporine-induced nephrotoxicity.


Pharmacokinetics
• Mycophenolic acid is quickly and almost completely absorbed after oral administration.
• The glucuronide metabolite is excreted predominantly in urine.
• Concomitant administration with antacids containing magnesium or aluminum, or with cholestyramine, can decrease absorption of the drug.

Adverse effects• GI adverse effects: (most Common) diarrhea, nausea,
vomiting, and abdominal pain.
• High doses of mycophenolate mofetil are associated with a higher risk of CMV infection.

Thalidomide• Historical sedative drug withdrawn in 1960s because of its
teratogenicity (Phocomelia). • Inhibits angiogenesis. • Antiinflammatory. • Inhibits tumor necrosis factor-alpha(TNF-α) • Reduces phagocytosis by neutrophils. • Increases production of IL-10 • Enhances cell-mediated immunity via interaction with T cells.

Thalidomide• Use continued only for leprosy.
• Very successful in multiple myeloma.
• Clinical trials in other diseases:
myelodysplastic syndrome, AML, graft-versus-
host disease, and solid tumors.

Thalidomide• Toxicity:
– Teratogenicity. – Peripheral neuropathy. – Constipation. – Rash. – Fatigue. – Hypothyroidism. – DVT.
• Lenalidomide • CC-4047(Actimid).
– Are much less toxic derivatives.

ANTIBODIES
• The use of antibodies has played a central role in prolonging allograft survival.
• They are prepared by immunization of either rabbits or horses with human lymphoid cells (producing a mixture of polyclonal antibodies or monoclonal antibodies).

Immunosuppresive Antibodies• Hybridoma Technology, 1975. • Molecular Biology >>>> Monoclonal
Antibodies. • Humanized Antibodies: “-umab” or “-umab”.
– Replacing most of the regions, but keeping only the variable, antigen-specific regions intact.
• Chimeric Antibodies: “-imab” or “-ximab”. – Less complete replacement of the murine
components.

Immunosuppresive Antibodies
• Antilymphocyte & Antithymocyte Antibodies. • Muromonab. • Immune Globulin Intravenous. • Rho(D) Immune Globulin Micro-Dose.
• Hyperimmune Immunoglobulins.

MuromonabInitial binding of muromonab to the antigen transiently activates the T cell and results in cytokine release (cytokine storm).
It is therefore customary to premedicate the patient with methylprednisolone, diphenhydramine, and acetaminophen to alleviate the cytokine release syndrome.

Rho(D) Immune Globulin Micro-Dose.• One of the earliest major advances in
immunopharmacology. • Concentrated (15%) solution of human IgG
containing a higher titer of antibodies against the Rho(D) antigen of the red cell.
• Given, to the mother, within 24-72 hours after the birth of an Rh-positive infant.
• Infant’s red cells are cleared from circulation before the mother can generate a B-cell response against the Rho(D) antigen.
• This will protect against future hemolysis.

Antitumor MABs• Alemtuzumab. • Bevacizumab. • Ranibizumab. • Cetuximab. • Gemtuzomab. • Panitumumab. • Rituximab. • Trastuzumab. • Novilumab.

MABs to Deliver Isotopes to Tumors• Arcitumomab. • Capromab. • Ibritumomab. • Nofetumomab. • Satomomab. • Tositumomab

MABs used as Immunosuppressants and Antiinflammatory Agents
• Anti-TNF-Alpha MABs: – Adalimumab. – Etanercept – Infliximab
• Abatacept • Alefacept • Basiliximab • Daclizumab • Efalizumab • Omalizumab • Abiximab • Eculizumab • Palivizumab

Hybridoma• Hybridoma technology (producing antigen-specific monoclonal antibodies). Hybridomas are produced by fusing mouse antibody-producing cells with tumor cells. Hybrid cells are selected and cloned, and the antibody specificity of the clones is determined.
• Clones of interest can be cultured in large quantities to produce clinically useful amounts of the desired antibody.

• Recombinant DNA technology can also be used to replace part of the mouse gene sequence with human genetic material, thus “humanizing” the antibodies and making them less antigenic.
• The names of monoclonal antibodies conventionally contain “xi” or “zu” if they are chimerized or humanized, respectively. The suffix “-mab” (monoclonal antibody) identifies the category of drug.

Anti-thymocyte globulins• Polyclonal antibodies that are primarily used at the time of transplantation to prevent early allograft rejection along with other immunosuppressive agents.
• They may also be used to treat severe rejection episodes or corticosteroid-resistant acute rejection.
• The antibodies bind to the surface of circulating T lymphocytes, which then undergo various reactions, such as complement mediated destruction, antibody-dependent cytotoxicity, apoptosis, and opsonization.
• The antibody-bound cells are phagocytosed in the liver and spleen, resulting in lymphopenia and impaired T-cell responses.

Pharmacokinetics & Adverse effects• Slowly infused intravenously • Half-life extends from 3 to 9 days.
• Because the humoral antibody mechanism remains active, antibodies can be formed against these foreign proteins.
• Other adverse effects include chills and fever, leukopenia and thrombocytopenia, infections due to CMV or other viruses, and skin rashes.

Muromonab-CD3 (OKT3)• Muromonab-CD3 is a murine (mouse) monoclonal antibody that is
directed against the glycoprotein CD3 antigen of human T cells.
• Muromonab-CD3 was the first monoclonal antibody approved for clinical use in 1986, indicated for the treatment of corticosteroid-resistant acute rejection of kidney, heart, and liver allografts.
• The drug has been discontinued from the market due to the availability of newer biologic drugs with similar efficacy and fewer side effects.

Basiliximab• The antigenicity and short serum half-life of the murine monoclonal
antibody have been averted by replacing most of the murine amino acid sequences with human ones by genetic engineering.
• Basiliximab [is said to be “chimerized” because it consists of 25% murine and 75% human protein.
• “Humanized” monoclonal antibodies (for example, trastuzumab used for breast cancer, have a smaller stretch of nonhuman protein.
• Basiliximab is approved for prophylaxis of acute rejection in renal transplantation in combination with cyclosporine and corticosteroids. It is not used for the treatment of ongoing rejection.

Basiliximab
• An anti-CD25 antibody that binds to the α chain of the IL-2 receptor on activated T cells and, thus, interferes with the proliferation of these cells.
• Blockade of this receptor foils the ability of any antigenic stimulus to activate the T-cell response system.
• Basiliximab is given as an IV infusion. The serum half-life of basiliximab is about 7 days.
• Usually, two doses of this drug are administered—the first at 2 hours prior to transplantation and the second at 4 days after the surgery. The drug is generally well tolerated, with GI toxicity as the main adverse effect.

MONOCLONAL ANTIBODIES (MABs )
Antitumor MABsAlemtuzumab is a humanized IgG 1 with a kappa chain that binds to CD52 found on normal and malignant B and T lymphocytes, NK cells, monocytes, macrophages, and a small population of granulocytes.
76

MONOCLONAL ANTIBODIES (MABs )
Currently, alemtuzumab is approved for the treatment of B-cell chronic lymphocytic leukemia in patients who have been treated with alkylating agents.
77

MABs Used to Deliver Isotopes to Tumors
Arcitumomab is a murine Fab fragment from an anti-carcinoembryonic antigen (CEA) antibody labeled with technetium 99m (99m Tc) that is used for imaging patients with metastatic colorectal carcinoma (immunoscintigraphy) to determine extent of disease. CEA is often upregulated on tumor in patients with gastrointestinal carcinomas. The use of the Fab fragment decreases the immunogenicity of the agent so that it can be given more than once; intact murine monoclonal antibodies would elicit stronger HAMA. 78

MABs Used to Deliver Isotopes to Tumors
Capromab pendetide is a murine monoclonal antibody specific for prostate specific membrane antigen. It is coupled to isotopic indium ( 111 In) and is used in immunoscintigraphy for patients with biopsy-confirmed prostate cancer and post-prostatectomy in patients with rising prostate specific antibody level to determine extent of disease.
79

MABs Used to Deliver Isotopes to Tumors
Ibritumomab tiuxetan is an anti-CD20 murine monoclonal antibody labeled with isotopic yttrium ( 90 Y). The radiation of the isotope coupled to the antibody provides the major antitumor activity. Ibritumomab is approved for use in patients with relapsed or refractory low-grade, follicular, or B-cell non-Hodgkin’s lymphoma, including patients with rituximab-refractory follicular disease. It is used in conjunction with rituximab in a two-step therapeutic regimen.
80

Cytokines• Are a large and heterogeneous group of
proteins with diverse functions. • Mediate their effects through receptors, like
hormones. • May have antiproliferative, antimicrobial, and
antitumor effects. • Produced using gene cloning techniques. • Have very short half lives, and given sc. • All induce fever, flu-like symptoms, anorexia,
fatigue, and malaise.

Cytokines• Interferones: INF- α, β, and γ. • Interleukins: 1-35. • Tumor Necrosis factor: α, and β. • Granulocyte colony-stimulating factor. • Granulocyte-macrophage colony-stimulating
factor. • Macrophage colony-stimulating factor. • Erythropoietin. • Thrombopoietin

Cytokines
• Interferon (INF): INF-α,β,γ – Antiviral, anticancer, immunomodulating effects. – Antiviral effects : INF-α,β> INF-γ – immunomodulating effects: INF-γ – Adverse Effects: flu-like symptoms, fatigue, malaise
• Interleukin-2 (IL-2) – T cell proliferation, TH, NK, LAK cell activation – Treatment of malignant melanoma, renal cell
carcinoma, Hodgkin disease – Adverse Effects: fever, anorexia, etc .

Cytokine Inhibitors
• Anakinra: – Is a recombinant form of the naturally
occurring IL-1 receptor antagonist. – Approved for adult rheumatoid arthritis