Embed Size (px)
Citation preview

DENTAL TECHNIQUE
Assistant Pro
THE JOURNA
Immediate provisionalization with a CAD/CAM interimabutment and crown: A guided soft tissue healing technique
Periklis Proussaefs, DDS, MS
ABSTRACTA technique is described in which a single interim abutment and crown were fabricated in advanceand placed the day of dental implant surgery. The contours of the interim crown were identical tothe contours of a tentatively designed definitive prosthesis and allowed the tissue to heal andobtain contours that accommodated the contours of the definitive prosthesis. After osseointegra-tion was established, a definitive impression was made with a custom computer-assisted designand computer-assisted manufacturing impression coping. The definitive prosthesis then wasfabricated. (J Prosthet Dent 2015;113:91-95)
Dental implants were in-troduced for the treatmentof patients with completeedentulism.1 However, soonafter their introduction, dentalimplants became a valid treat-ment for patients with partialedentulism.2,3 For these in-dividuals, providing interim
restorations is important because these restorations helpconfirm the diagnostic design,4,5 esthetics,4-6 and con-tours,4-8 which can be replicated in the definitive pros-thesis.9-11 The healing response around the abutmentscan be evaluated,8,10-12 and the soft tissue around thefixtures can heal according to the contours of the defini-tive prosthesis.6,10,11,13,14 Interim restorations also allowthe osseointegration of the fixture to be observed.14The conventional protocol indicated that a healingperiod of 3 to 6 months is recommended to achieveosseointegration before loading the implants with aprosthesis.15 Immediate loading is a technique for elim-inating the 3- to 6-month healing period. The techniquehas been described in combination with mandibularbar-retained overdentures,16-18 complete arch implant-supported screw-retained prostheses,19-23 and with par-tial edentulism.24-32 Regardless of the technique, variousmethods have been proposed and used33-36 to transfersoft tissue architecture to the laboratory so the definitiveprosthesis can be fabricated in accordance with the ac-quired soft tissue morphology. The purpose of the cur-rent technique report was to describe a method forthe immediate loading of single root form implantswith a computer-assisted design and computer-assistedmanufacturing (CAD/CAM) interim restoration.
fessor, Advance Education Program in Implant Dentistry, Loma Linda Univ
L OF PROSTHETIC DENTISTRY
TECHNIQUE
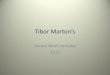
1. Evaluate the tissue around the edentulous areafor signs or symptoms of pathosis (Fig. 1). Makecomplete arch preliminary impressions preopera-tively from the patient’s maxillary and mandibulararches by using polyvinyl siloxane impressionmaterial (Silgimix; Sultan Healthcare). Make aninterocclusal record with polyvinyl siloxane oc-clusal registration material (Exabite II NSD; GCAmerica Inc) at the maximum intercuspation po-sition. In addition, after providing local anesthesia,map the alveolar ridge by using an endodontic filewith a rubber stop.37 With this technique, thethickness of the soft tissue is measured around thearea of the prospective implant surgery.
2. Scan the impressions (D700 scanner; 3Shape) andsimulate the definitive prosthesis with the pro-vided software. The computer software, which isincorporated into the scanner, allows the size andshape of each component to be designed digitallyby using precise measurements. With the contoursof the definitive prosthesis as reference, fabricatea custom interim abutment from a polymethylmethacrylate (PMMA) block with a milling
ersity, School of Dentistry, Loma Linda, Calif.
91
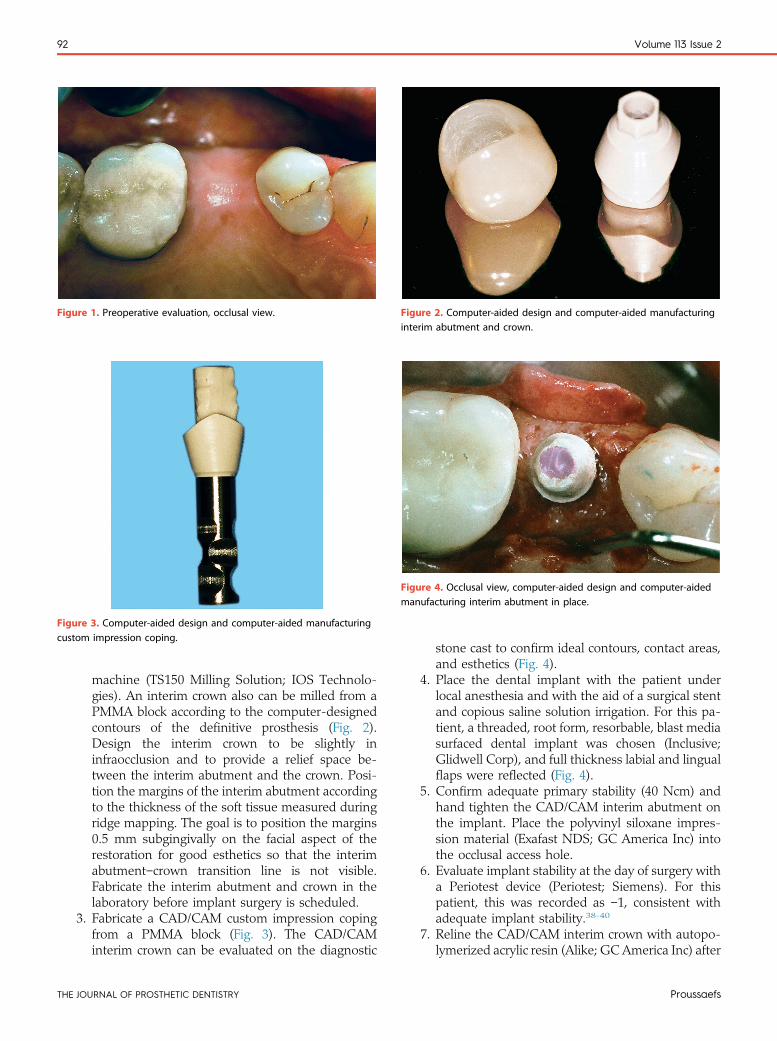
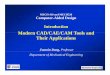
Figure 1. Preoperative evaluation, occlusal view. Figure 2. Computer-aided design and computer-aided manufacturinginterim abutment and crown.
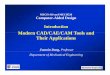
Figure 3. Computer-aided design and computer-aided manufacturingcustom impression coping.
Figure 4. Occlusal view, computer-aided design and computer-aidedmanufacturing interim abutment in place.
92 Volume 113 Issue 2
TH
machine (TS150 Milling Solution; IOS Technolo-gies). An interim crown also can be milled from aPMMA block according to the computer-designedcontours of the definitive prosthesis (Fig. 2).Design the interim crown to be slightly ininfraocclusion and to provide a relief space be-tween the interim abutment and the crown. Posi-tion the margins of the interim abutment accordingto the thickness of the soft tissue measured duringridge mapping. The goal is to position the margins0.5 mm subgingivally on the facial aspect of therestoration for good esthetics so that the interimabutmentecrown transition line is not visible.Fabricate the interim abutment and crown in thelaboratory before implant surgery is scheduled.
3. Fabricate a CAD/CAM custom impression copingfrom a PMMA block (Fig. 3). The CAD/CAMinterim crown can be evaluated on the diagnostic
E JOURNAL OF PROSTHETIC DENTISTRY
stone cast to confirm ideal contours, contact areas,and esthetics (Fig. 4).
4. Place the dental implant with the patient underlocal anesthesia and with the aid of a surgical stentand copious saline solution irrigation. For this pa-tient, a threaded, root form, resorbable, blast mediasurfaced dental implant was chosen (Inclusive;Glidwell Corp), and full thickness labial and lingualflaps were reflected (Fig. 4).
5. Confirm adequate primary stability (40 Ncm) andhand tighten the CAD/CAM interim abutment onthe implant. Place the polyvinyl siloxane impres-sion material (Exafast NDS; GC America Inc) intothe occlusal access hole.
6. Evaluate implant stability at the day of surgery witha Periotest device (Periotest; Siemens). For thispatient, this was recorded as e1, consistent withadequate implant stability.38-40
7. Reline the CAD/CAM interim crown with autopo-lymerized acrylic resin (Alike; GC America Inc) after
Proussaefs
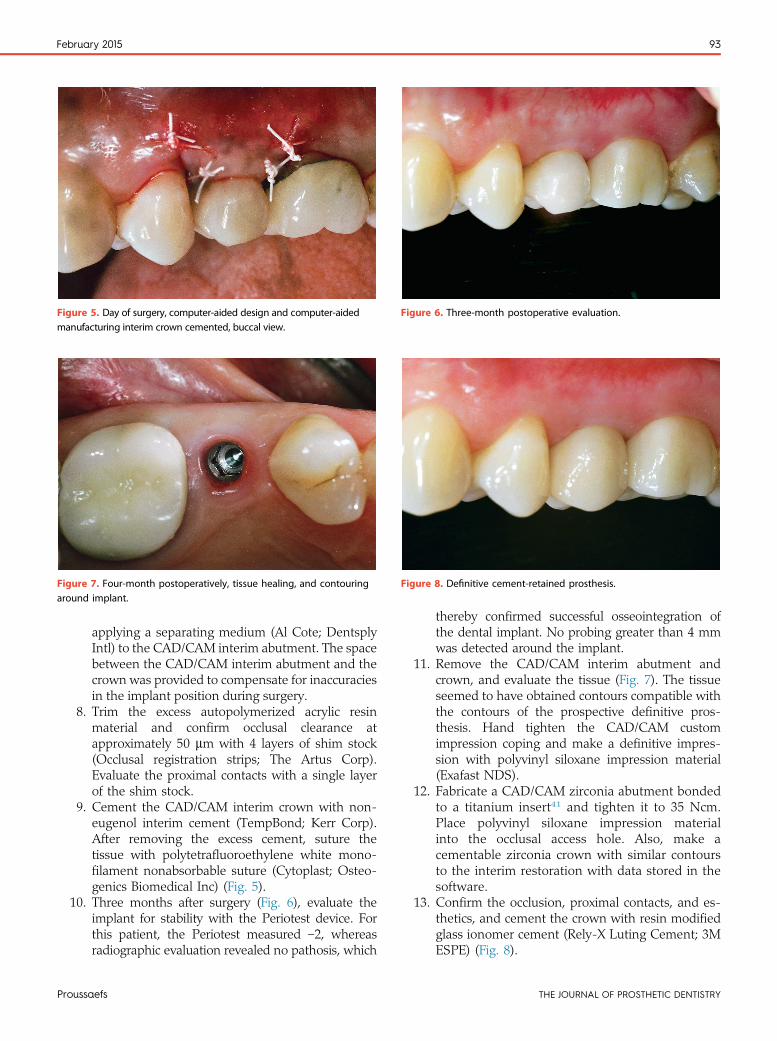
Figure 5. Day of surgery, computer-aided design and computer-aidedmanufacturing interim crown cemented, buccal view.
Figure 6. Three-month postoperative evaluation.
Figure 8. Definitive cement-retained prosthesis.Figure 7. Four-month postoperatively, tissue healing, and contouringaround implant.
February 2015 93
Pr
applying a separating medium (Al Cote; DentsplyIntl) to the CAD/CAM interim abutment. The spacebetween the CAD/CAM interim abutment and thecrown was provided to compensate for inaccuraciesin the implant position during surgery.
8. Trim the excess autopolymerized acrylic resinmaterial and confirm occlusal clearance atapproximately 50 mm with 4 layers of shim stock(Occlusal registration strips; The Artus Corp).Evaluate the proximal contacts with a single layerof the shim stock.
9. Cement the CAD/CAM interim crown with non-eugenol interim cement (TempBond; Kerr Corp).After removing the excess cement, suture thetissue with polytetrafluoroethylene white mono-filament nonabsorbable suture (Cytoplast; Osteo-genics Biomedical Inc) (Fig. 5).
10. Three months after surgery (Fig. 6), evaluate theimplant for stability with the Periotest device. Forthis patient, the Periotest measured e2, whereasradiographic evaluation revealed no pathosis, which
oussaefs
thereby confirmed successful osseointegration ofthe dental implant. No probing greater than 4 mmwas detected around the implant.
11. Remove the CAD/CAM interim abutment andcrown, and evaluate the tissue (Fig. 7). The tissueseemed to have obtained contours compatible withthe contours of the prospective definitive pros-thesis. Hand tighten the CAD/CAM customimpression coping and make a definitive impres-sion with polyvinyl siloxane impression material(Exafast NDS).
12. Fabricate a CAD/CAM zirconia abutment bondedto a titanium insert41 and tighten it to 35 Ncm.Place polyvinyl siloxane impression materialinto the occlusal access hole. Also, make acementable zirconia crown with similar contoursto the interim restoration with data stored in thesoftware.
13. Confirm the occlusion, proximal contacts, and es-thetics, and cement the crown with resin modifiedglass ionomer cement (Rely-X Luting Cement; 3MESPE) (Fig. 8).
THE JOURNAL OF PROSTHETIC DENTISTRY

94 Volume 113 Issue 2
DISCUSSION
Placement of an interim restoration on the day of implantsurgery offers esthetic, psychological, and functional ad-vantages compared with the use of an interim removableprosthesis. It also eliminates second-stage surgery, whichreduces patient discomfort and additional proceduralcost. The soft tissue around the implants can healaccording to the contours of the interim restora-tion.11,13,14,28,29 However, if the interim restoration isplaced after the implant becomes osseointegrated, thenan additional healing period of 3 to 8 weeks is needed forsoft tissue healing.6,10,11,14 The protocol presented elim-inated the period necessary for soft tissue healing andcontouring because healing occurred concurrently withthe implant.
In the described technique, a CAD/CAM impressioncoping was used to transfer soft tissue anatomy speci-mens to the laboratory before fabricating the definitiveprosthesis. Others have suggested the use of the interimprosthesis while making the impression,28,36 fabricate acustom impression coping by placing autopolymerizedacrylic resin around the impression coping,30,34,36 or useintraoral scanners.35 To the author’s best knowledge, noconsensus exists as to which technique better transferssoft tissue architecture in the laboratory before thefabrication of a definitive prosthesis. The describedtechnique may provide reduced chair time by having thecustom impression coping fabricated in advance beforeimplant surgery.
With the described technique, the operator also hasthe option of fabricating a screw-retained interim resto-ration, which would entail the use of acrylic resin materialbetween the CAD/CAM interim abutment and the crownafter implant placement. In this situation, no separatingmedium would be placed between the interim abutmentand the crown. After removing the excess acrylic resinmaterial, the operator could open an occlusal accesshole on the interim restoration, which transforms theinterim prosthesis into a screw-retained restoration. Theliterature regarding complications of interim prosthesisplaced on dental implants on the day of surgery is scarce.Oyama et al25 evaluated 17 consecutively treated rootform dental implants of patients who received interimrestoration on the day of surgery. In their study, 46% ofthe cement-retained interim crowns fractured and15% experienced debonding of the acrylic resin veneermaterial. Therefore, patients need to be aware ofthese complications, and a thorough informed consentshould include the relatively high possibility of thoseoccurring.
SUMMARY
The described technique offers an alternative method forfabricating interim restorations on dental implants. A
THE JOURNAL OF PROSTHETIC DENTISTRY
prospective clinical study is needed to validate the use ofthe described technique.
REFERENCES
1. Adell R, Lekholm U, Rockler B, Branemark PI. A 15 year study of osseoin-tegrated implants in the treatment of the edentulous jaw. Int J Oral Surg1981;10:387-416.
2. Jemt T, Lekholm U, Adell R. Osseointegrated implants in the treatmentof partially edentulous patients: a preliminary study of 876 consecutivelyinstalled fixtures. Int J Oral Maxillofac Implants 1989;4:211-7.
3. Jemt T, Pettersson P. A 3-year follow-up study on single implant treatment.J Dent 1993;21:203-8.
4. Moscovitch MS, Saba S. The use of a provisional restoration in implantdentistry: a clinical report. Int J Oral Maxillofac Implants 1996;11:395-9.
5. Capp NJ. The diagnostic use of provisional restorations. Restorative Dent1985;1:94-8.
6. Neale D, Chee WW. Development of implant soft tissue emergence profile: atechnique. J Prosthet Dent 1994;71:364-8.
7. Breeding LC, Dixon DL. Transfer of gingival contours to a master cast.J Prosthet Dent 1996;75:341-3.
8. Saba S. Anatomically correct soft tissue profiles using fixed detachable pro-visional implant restorations. J Can Dent Assoc 1997;63:767-70.
9. Sze AJ. Duplication of anterior provisional fixed partial denture for the finalrestoration. J Prosthet Dent 1992;68:220-3.
10. Proussaefs P. The use of healing abutments for an implant supported fixedpartial denture. J Prosthet Dent 2002;87:333-5.
11. Biggs WF. Placement of a custom implant provisional restoration at thesecond-stage surgery for improved gingival management: a clinical report.J Prosthet Dent 1996;75:231-3.
12. Listgarten MA, Lang NP, Schroeder HE, Schroeder A. Periodontal tissuesand their counterparts around endosseous implants. Clin Oral Implants Res1991;2:1-19.
13. Daftary F, Bahat O. Prosthetically formulated natural esthetics in implantprostheses. Pract Periodontics Aesthet Dent 1994;6:75-83.
14. Lewis S. Anterior single-tooth implant restorations. Int J PeriodonticsRestorative Dent 1995;15:31-41.
15. Branemark PI. Osseointegration and its experimental background. J ProsthetDent 1983;50:399-410.
16. Levkove M, Beals R. Immediate loading of cylinder Implants with over-dentures in the mandibular symphisis: the titanium plasma-spray screwsystem. J Oral Implantol 1990;4:265-70.
17. Chiapasco M, Gatti C, Rossi E, Haefliger W, Markwalder TH. Implant-retained mandibular overdentures with immediate loading. Clin Oral Im-plants Res 1997;8:48-57.
18. Schnitman P, Wohrle P, Rubenstein J. Immediate fixed interim prosthesessupported by two-stage threaded implants: methodology and results. J OralImplantol 1990;16:96-105.
19. Schnitman P, Wohrle P, Rubenstein J, DaSilva J, Wang NH. Ten-year resultsfor Branemark implants immediately loaded with fixed prostheses at implantplacement. Int J Oral Maxillofac Implants 1997;12:495-503.
20. Tarnow DP, Emtiaz S, Classi A. Immediate loading of threaded implants atstage 1 surgery in edentulous arches: ten consecutive case reports with 5-yeardata. Int J Oral Maxillofac Implants 1997;3:319-24.
21. Randow K, Ericsson I, Nilner K, Petersson A, Glantz PO. Immediate func-tional loading of Branemark dental implants. An 18-month clinical follow-upstudy. Clin Oral Impl Res 1999;10:8-15.
22. Ji TJ, Kan JY, Rungcharassaeng K, Roe P, Lozada JL. Immediate loading ofmaxillary and mandibular implant-supported fixed complete dentures: a 1- to10-year retrospective study. J Oral Implantol 2012;38:469-76.
23. Malo P, de Araujo Nobre M, Lopes A, Moss SM, Molina GJ. A longitudinalstudy of the survival of all-on-4 implants in the mandible with up to 10 yearsof follow-up. J Am Dent Assoc 2011;142:310-20.
24. Gomes A, Lozada J, Caplanis N, Kleinman A. Immediate loading of a singlehydroxyapatite-coated threaded root form implant: a clinical report. J OralImplantol 1998;24:159-66.
25. OyamaK,Kan JY, RungcharassaengK,Lozada J. Immediateprovisionalization ofa 3.0-mm-diameter implants replacing single missing maxillary and mandibularincisors: 1-year prospective study. Int J Oral Maxillofac Implants 2012;27:173-80.
26. Ross S, Pette GA. Immediate implant placement and provisionalization usinga customized anatomic temporary abutment (CATA) to achieve gingivalmarginal stability. Compendium 2013;34:344-50.
27. Babushkin JA. Restorative responsibilities for achieving exceptional implantesthetics. Compendium 2013;34:418-23.
28. Proussaefs P, Lozada J. Immediate loading of hydroxyapatite-coated implantsat maxillary premolar area: three-year results of a pilot study. J Prosthet Dent2004;91:228-33.
29. ProussaefsP,Kan J, Lozada J,KleinmanA,FarnosA.Effectsof immediate loadingwith threaded hydroxyapatite-coated root-form implants on single premolarreplacements: a preliminary report. Int J OralMaxillofac Implants 2002;4:567-72.
Proussaefs
February 2015 95
30. Kan JY, Rungcharassaeng K, Lozada J. Immediate placement and provi-sionalization of maxillary anterior single implants: 1-year prospective study.Int J Oral Maxillofac Implants 2003;18:31-9.
31. Balshi TJ, Wolfinhger GJ, Wulc D, Balshi SF. A prospective analysis ofimmediate provisionalization of single implants. J Prosthodont 2011;20:10-5.
32. Abboud M, Koeck B, Stark H, Wahl G, Paillon R. Immediate loading ofsingle-tooth implants in the posterior region. Int J Oral Maxillofac Implants2005;20:61-8.
33. Bruno V, O’Sullivan D, Badino M, Catapano S. Preserving soft tissue afterplacing implants in fresh extraction sockets in the maxillary esthetic zone anda prosthetic template for interim crown fabrication: a prospective study.J Prosthet Dent 2014;11:195-202.
34. Noh K, Kwon KR, Kim HS, Kim DS, Pae A. Accurate transfer of soft tissuemorphology with interim prosthesis to definitive cast. J Prosthet Dent2014;111:159-62.
35. Lin WS, Harris BT, Morton D. Use of implant-supported interim restorationsto transfer periimplant soft tissue profiles to a milled polyurethane definitivecast. J Prosthet Dent 2013;109:333-7.
36. Man Y, Qu Y, Dam HG, Gong P. An alternative technique for the accuratetransfer of periimplant soft tissue contour. J Prosthet Dent 2013;109:135-7.
37. Koutouzis T, Neiva R, Nonhoff J, Lundgren T. Placement of implants withplatform-switched Morse taper connections with the implant-abutment
Access to The Journal of Prosthetic Dentistry
This is your subscription account number
Full-text access to The Journal of Prosthetic Dentistry Online individual online subscription, please visit The Journal of Prohttp://www.journals.elsevierhealth.com/periodicals/ympr/hoand follow the instructions. To activate your account, you wilfind on your mailing label (note: the number of digits in yourexample below in which the subscriber account number has
Personal subscriptions to The Journal of Prosthetic Dentistry ferred. Use of The Journal of Prosthetic Dentistry Online is suindicated online.
Proussaefs
interface at different levels in relation to the alveolar crest: a short-term(1-year) randomized prospective controlled clinical trial. Int J Oral MaxillofacImplants 2013;28:1553-63.
38. Olive J, Aparicio C. Periotest method as a measure of osseointegrated oralimplant stability. Int J Oral Maxillofac Implants 1990;5:390-400.
39. Teerlinck J, Quirynen M, Darius P, van Steenberghe D. Periotest: an objectiveclinical diagnosis of bone apposition towards implants. Int J Oral MaxillofacImplants 1991;6:55-61.
40. Elias J, Brunski JB, Scarton HA. A dynamic modal testing technique fornoninvasive assessment of bone-dental implant interfaces. Int J Oral Max-illofac Implants 1996;11:728-34.
41. Kim JS, Raigrodski AJ, Flinn BD, Rubenstein JE, Chung KH, Mancl LA.In vitro assessment of three types of zirconia implant abutments under staticload. J Prosthet Dent 2013;109:255-63.
Corresponding author:Dr Periklis Proussaefs3585 Telegraph Road, Suite CVentura, CA 93003Email: [email protected]
Copyright © 2015 by the Editorial Council for The Journal of Prosthetic Dentistry.
Online is reserved for print subscribers!
Sample mailing label
is available for all print subscribers. To activate your sthetic Dentistry Online. Point your browser to me, follow the prompts to activate online access here, l need your subscriber account number, which you can subscriber account number varies from 6 to 10). See the been circled.
Online are for individual use only and may not be trans-bject to agreement to the terms and conditions as
THE JOURNAL OF PROSTHETIC DENTISTRY