Embed Size (px)
Citation preview

Medical Dosimetry
Medical Dosimetry 41 (2016) 142–147
http://d0958-39BY-NC-N
Mbureau
RepSheba M
E-m
journal homepage: www.meddos.org
Immediate breast reconstruction with anatomical implants followingmastectomy: The radiation perspective
Merav Ben-David, M.D.,*† Hila Granot, B.A.,* Ilana Gelernter, M.A.,‡ andMichael Scheflan, M.D.§
*Radiation Oncology Unit, Chaim Sheba Medical Center, Ramat Gan, Israel; †Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel; ‡StatisticalLaboratory, School of Mathematics, Tel Aviv University, Tel Aviv, Israel; and §Department of Surgery, Assuta and Herzliya Medical Centers, Ramat Gan, Israel
A R T I C L E I N F O
Article history:Received 19 March 2015Received in revised form19 October 2015Accepted 29 November 2015
Keywords:Acellular dermal matrixAnatomical implantImmediate breast reconstructionInternal mammary nodesPostmastectomy radiation therapy3-Dimensional conformal radiotherapy
x.doi.org/10.1016/j.meddos.2015.11.00247/Copyright � 2016 The Authors. PublishedD license (http://creativecommons.org/licens
.B.-D., H.G., and I.G. have no conflict of inteand is a consultant and investigator for Allergrint requests to: Merav Ben-David, M.D., Radedical Center, 5 Mendes Street, Ramat Gan, Iail: [email protected]
A B S T R A C T
Immediate implant-based breast reconstruction followed by postmastectomy radiation therapy (PMRT)is controversial because of the risk of compromised treatment plans and concerns regarding cosmeticoutcomes. We evaluated the effects of immediate direct-to-implant breast reconstruction with anatom-ical implants on the quality of PMRT delivered by 3-dimensional conformal radiotherapy (3D-CRT). Inthis retrospective, single-institution study, patients who had undergone reconstruction with directanatomic implant, performed by a single surgeon, received 3D-CRT between 2008 and 2013. For eachpatient, 2 plans (including or excluding internal mammary nodes [IMN]) were created and calculated.The primary end point was the dose distribution among reconstructed breasts, heart, lungs, and IMNs,and between right and left breasts. Of 29 consecutive patients, 11 received right-sided and 18 receivedleft-sided PMRT to a total dose of 50 Gy. For plans excluding IMN coverage, mean Dmean for right and leftreconstructed breasts was 49.09 Gy (98.2% of the prescribed dose) and 48.51 Gy (97.0%), respectively. Forplans including IMNs, mean Dmean was 49.15 Gy (98.3%) for right and 48.46 Gy (96.9%) for leftreconstructed breasts; the mean IMN Dmean was 47.27 Gy (right) and 47.89 Gy (left). Heart Dmean wasbelow 1.56 Gy for all plans. Mean total lung volume receiving a dose of Z 20 Gy was 13.80% to 19.47%.PMRT can be delivered effectively and safely by 3D-CRT after direct-to-implant breast reconstructionwith anatomical implants, even if patients require IMN treatment.& 2016 Published by Elsevier Inc. on behalf of American Association of Medical Dosimetrists. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
For women with locally advanced breast cancer, adjuvantpostmastectomy radiation therapy (PMRT) is an important treat-ment strategy that has been shown to prolong disease-free andoverall survival.1,2 Given the high risk of locoregional recurrenceassociated with lymph node–positive breast cancer, PMRT isrecommended for patients with positive axillary lymph nodes.3-5
Immediate implant-based reconstruction after mastectomy candeliver excellent esthetic outcomes because of the availability ofskin-sparing and nipple/areola-sparing mastectomy and the use ofacellular dermal matrices (ADM) to expand and shape the implant
by Elsevier Inc. on behalf of Ameries/by-nc-nd/4.0/).
rest. M.S. is on the speakers'an, Inc.iation Oncology Unit, Chaimsrael.
pocket without serratus anterior muscle elevation.6,7 Furthermore, thepresence of a breast prosthesis during PMRT with photon beam is notassociated with significant changes in dose distribution.8,9 However,immediate implant-based breast reconstruction in patients requiringPMRT remains controversial because of concerns for higher risk ofunfavorable reconstructive outcomes,10-12 although some found thatthe risk of reconstructive failure after PMRT was acceptable.13
For radiation oncologists delivering PMRT, a key question iswhether specific approaches of immediate reconstruction, includ-ing implant-based reconstruction, allow for optimal coverage ofthe chest wall and internal mammary nodes (IMN) with acceptabledoses to the heart and lungs. A potential determinant for thequality of PMRT treatment plans after direct-to-implant recon-struction is the shape of the implant, as it may limit the options forfield arrangements. Round and teardrop-shaped cohesive gelimplants have been shown to yield similar esthetic results inbreast augmentation.14 However, in patients requiring PMRT, theuse of anatomical implants with their gradually tapered slope
can Association of Medical Dosimetrists. This is an open access article under the CC

M. Ben-David et al. / Medical Dosimetry 41 (2016) 142–147 143
above the medial part of the chest wall has the potential to obviatethe need for a medial electron field15 and allow for partially widetangential field plan, hence, avoiding matching electron-photonfields, high skin doses with electrons, and reducing on-treatmenttime. In the present radiation planning study, we sought todetermine whether the use of anatomical implants in combinationwith modern radiation techniques would enable us to improve thequality of treatment after ADM-assisted direct-to-implant recon-struction with anatomical implants compared with the reportedseries of nonanatomic (mostly round/tissue expanders) implants.We compared the doses with the reconstructed breast (RB), IMNs,heart, and lungs between treatment plans with and withoutintended IMN coverage in patients with left- or right-sidedreconstruction.
Patients and Methods
Study design and patients
This retrospective study was approved by the responsible institutional reviewboard and included 29 patients who received PMRT from 2008 to 2013 at ourinstitution. All patients with Stage 0 to III breast cancer who underwent skin-sparing mastectomy followed by immediate direct-to-implant breast reconstruc-tion with anatomically shaped silicon-filled implants (Natrelle 410, Allergan, Inc.,Irvine, CA) were included. A fenestrated ADM derived from fetal bovine dermis(SurgiMend, TEI Biosciences Inc., Boston, MA) was used in shaping the implantpocket. All breast reconstructions were performed by a single plastic surgeon (M.S.). The primary end point was the dose distribution among RB, IMNs, heart, andlungs, with 3-dimensional conformal radiotherapy (3D-CRT) including or excludingIMN coverage.
Target and normal tissue delineation
The clinical borders of the treatment region, which were defined by theplacement of catheters during computed tomography (CT) simulation, includedthe medial border at the patient midline, the lateral border situated approximatelyat the midaxillary line, the superior border at the inferior aspect of the clavicularhead, and the inferior border 1.5 cm below the RB fold. The RB planning volume(target volume) was delineated on axial CT scans using the clinical borders as aguide. This target volume (including the implant and associated remnant breasttissue) was contoured and edited, with the anterior border placed 0.5 cm inside theexternal body contour. The posterior border was defined by connecting a point thatis 5 mm lateral to the medial border with a point that is 5 mm medial to the lateralborder and subsequently edited to be anterior to the intercostal muscles. Theinferior border was placed 10 mm below the implant and the superior borderextended up to the bottom of the clavicular head. This definition was based on anestimate of the 95% isodose surface derived from traditional tangential breastfields. The internal mammary chain was delineated lateral to the sternum atintercostal spaces 1 to 3, including the node, vein, and artery. The whole heart wascontoured based on a heart atlas.16 Bilateral lungs were contoured using automateddensity gradient tracking with subsequent review and editing as necessary. Allcontours were done by a single radiation oncologist (M.B.-D.).
Radiation treatment planning
In total, 2 treatment plans were generated for each patient, 1 with coverage ofthe RB alone and the other with both the RB and the internal mammary chain. CTsimulation was performed with 3- to 5-mm cuts on a breast board with both armsabove the head. Standard treatment planning using partially wide tangentialfields with 6-MV photons or a combination of 6 and 15-MV photons were used.No bolus was used during planning or treatment. In accordance with theInternational Commission on Radiation Units and Measurements guidelines,the RB (target volume) was to be covered with 95% to 107% of the planned doseof 50 Gy (2.0 Gy per fraction). The implant was not defined as a separate target.IMNs were to be covered with 90% of the planned dose. Dynamic wedges andsegments were used as needed to improve dose homogeneity and a multileafcollimator of 0.5 cm width was used as needed. For left-sided treatment, theheart was excluded from the fields; in case of anterior heart position, radiationwas delivered with the Varian Real-time Position Management (RPM) system(Varian Medical Systems, Inc., Palo Alto, CA) and treatment plans were calculatedon the RPM scan.17 A supraclavicular field was added to all plans for conformality.No electron fields were added for IMN coverage and no field (exit/entry) wasallowed through the contralateral breast.
Plan evaluation and statistical analysis
Dose-volume histograms were generated for the RB and IMNs and for normalorgans, including the heart and lungs. Dose distributions were compared betweenthe 2 plans for each patient or between right- and left-sided treatment plans usingpaired t-tests. Statistical comparisons were made for Dmean and doses to 95% (D95)or 90% (D90) of the volume of the RB, IMNs, and heart, and for the percentage oftotal lung volume receiving a dose of Z 20 Gy (V20). Pearson correlation analysiswas used to evaluate the effects of variants on dosimetric results, and nonpaired t-tests were used for independent group outcomes. A 5% significance level was usedfor all tests.
Results
Patients
Of 29 patients included in this analysis, 18 had undergonereconstruction of the left breast and 11 had undergone recon-struction of the right breast. A total of 2 patients had bilateralreconstruction. The mean implant volume was 392 mL (range: 225to 615 mL), with no significant difference between implant vol-umes for left- and right-sided reconstruction (389 vs 396 mL,respectively, p ¼ 0.856). The mean planned treatment volumebased on RB contoured areas for treatment planning was 603 mLoverall (range: 245 to 1209 mL) and similar for left and right RBs(564 vs 604 mL, respectively, p ¼ 0.683). The mean medial distance(i.e., the distance from the medial edge of the implant to the bodymidline) was 3.24 cm (range: 1.44 to 5.72 cm). Medial distanceswere similar on both sides and were not affected by implantvolume.
Dosimetric findings
Implant volume and medial distance did not affect breast Dmean
or D95, heart Dmean, lung V20, or IMN coverage across treatmentplans. For plans with RB coverage only, mean Dmean for right andleft RBs was 49.09 Gy (98.2% of the prescribed dose) and 48.51 Gy(97.0%), respectively (Fig. 1); the corresponding values for plansincluding IMN coverage were very similar (i.e., 49.15 Gy [98.3%] forright RBs and 48.46 Gy [96.9%] for left RBs) (Table). Although theDmean values showed statistically significant differences in favor ofright- vs left-side coverage, the difference between mean valueswas o 0.70 Gy for both plans and therefore is probably notclinically meaningful (Table and Fig. 2). RB D95 values weresignificantly smaller with left- vs right-sided treatment in plansthat included IMN coverage. Statistically significant differences inD95 for left vs right RBs also were seen with plans that excludedIMN coverage, but the difference between mean values was small(Table and Fig. 2). For treatment plans including IMN coverage, themean IMN Dmean values for left- and right-sided treatment werevery similar, and there was no significant difference between left-and right-sided IMN coverage based on D90 (Table and Fig. 3).Dmean evaluated for the RB excluding the anatomical implant was93.12% and 92.80% of the prescribed dose for plans with andwithout IMN, respectively (p ¼ 0.12).
Doses to the heart in patients who received radiation treatmentof the left RB were very low, even when IMNs were included in thetreatment plan. The mean heart Dmean was 1.25 Gy (range: 0.83 to1.46 Gy) for treatment plans with no IMN coverage and 1.56 Gy(range: 1.23 to 2.10 Gy) for plans including IMN coverage (p o0.001) (Table and Fig. 4).
The overall mean lung V20 was 16.45%. Mean lung V20 wasgenerally higher for right- vs left-sided treatment and for plansincluding IMN coverage vs those excluding it (Table and Fig. 5).Plans including IMN coverage had a mean lung V20 of 17.95% (range:8.10% to 21.32%) compared with 15.45% (range: 7.51% to 20.30%) forplans with no IMN coverage (p ¼ 0.040). The highest lung V20 values

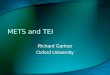
Fig. 1. (A) Owing to the anatomical implant shape and gradual takeoff from midline, complete left-sided internal mammary node (IMN) coverage is achieved without heartexposure (color wash, 90% isodose is shown in blue and 90% to 107% dose is shown in yellow). (B) Excellent IMN coverage in a patient with right-sided reconstruction usingan anatomical implant (color wash, 90% dose is shown). Contoured are the heart (red), breast implant (yellow), reconstructed breast (orange), internal mammary nodes(green), and lungs (light green).
M. Ben-David et al. / Medical Dosimetry 41 (2016) 142–147144
were seen for the right lung when IMN coverage was included(Fig. 5). Adding IMNs to the treatment fields increased lung V20
values by a mean of 2.52% for left-sided and 2.37% for right-sidedtreatment (p ¼ 0.543).
A total of 6 patients with left-sided treatment of RB andanterior heart position were treated with the RPM system. Therewere no statistically significant differences between these patientsand those (12 patients) treated without the RPM system regardingimplant volume (p ¼ 0.30), planned treatment volume (p ¼ 0.68),midline distance (p ¼ 0.49), RB Dmean (p ¼ 0.40), RB D95 (p ¼ 0.84),IMN Dmean (p ¼ 0.49), IMN D90 (p ¼ 0.28), or lung V20 (p ¼ 0.06).
Discussion
Immediate breast reconstruction before PMRT may result incompromised treatment plans, particularly if IMN treatment is
required.18,19 Radiation exposure of the heart during radiationtherapy for breast cancer is known to increase the risk ofcardiovascular morbidity, specifically in patients who receivedleft-sided irradiation.20-22
Using CT simulation and 3D-CRT, good RB coverage wasachieved in our study regardless of whether the treatment planincluded IMNs. In addition, treatment plans that targeted IMNstogether with the RB provided adequate coverage of both, withIMN mean D90 exceeding 94% of the prescribed dose. Importantly,the high quality of target volume coverage was achieved withoutcompromising safety, as doses to the heart and lungs were lowregardless of the treatment plan. Although inclusion of IMNtreatment in the plan was associated with a statistically significantincrease in doses to the heart, the absolute mean heart doses bothin patients with and without IMN coverage were very low (Dmean
o 1.6 Gy). These low heart doses are attributed to the heart block

TableSummary of dosimetric findings
Mean � SD No IMN coverage IMN coverage
Left Right Left Right
Reconstructed breastDmean (Gy) 48.51 � 0.31 49.09 � 0.94 48.46 � 1.08 49.15 � 0.42D95 (Gy) 42.96 � 6.17 44.75 � 4.23 42.05 � 3.96 45.15 � 6.55
IMNDmean (Gy) N/A N/A 47.89 � 1.88 47.27 � 1.31D90 (Gy) N/A N/A 40.96 � 16.78 44.90 � 6.74
HeartDmean (Gy) 1.25 � 0.17 N/D 1.56 � 0.22 N/D
LungsV20 (%) 13.80 � 2.80 17.1 � 2.95 16.32 � 3.35 19.47 � 4.35
D90 ¼ doses to 90%; D95 ¼ doses to 95%; N/A ¼ not applicable; N/D ¼ notdetermined; SD ¼ standard deviation; V20 ¼ total lung volume receiving a dose ofZ 20 Gy.
30
35
40
45
50
55
60
Dmean D90
p = 0.089 p = 0.340
Left Left RightRight
Dos
e (G
y)
Fig. 3. Dmean and D90 to left- and right-sided internal mammary nodes.
1.8
2.0p < 0.001
M. Ben-David et al. / Medical Dosimetry 41 (2016) 142–147 145
in the treatment fields and to the use of the RPM system in6 patients with anterior heart position. Such low doses have beenshown to have no short-term effects on cardiac structure, perfu-sion, or function.23 In addition, they generally are not associatedwith clinically meaningful increases in the risk of major cardio-vascular events.24 A recent retrospective case-control study in2168 women who received radiation therapy for breast cancerfound that mean heart doses o 2.0 Gy were associated with anestimated increase in the rate of major coronary events of only 10%(the lowest).24
Overall, doses to the lungs in our study were also low. However,lung V20 values varied between the 2 treatment plans and betweenleft and right sides, with the highest values observed in patientswith right-sided treatment including IMN coverage. As heartshielding blocks radiation to the lungs and reduces V20 in the leftside as well, no such effects exist in the right side. This aspect,coupled with the addition of the IMN volume, leads to widertangential fields, hence resulting in higher V20 values.
A recent study by Chung et al.15 evaluated the quality of PMRTin 20 patients with autologous or tissue expander/implant recon-struction. Although RB and IMN coverage observed in that studywas excellent, doses to the heart were higher. The mean heartDmean in patients who received left-sided treatment includingIMNs was 5.81 Gy in the study by Chung et al. (1.56 Gy in ourstudy). As both studies used 3D-CRT planning, reasons for thedifferences in heart exposure between the 2 studies likely include
30
35
40
45
Dos
e (G
y)
50
55
Dmean D95IMN IMNoNoN IMNIMN
Left LeftRight Right Left LeftRight Right
p = 0.025 p = 0.013 p = 0.004p = 0.024
Fig. 2. Left- and right-sided Dmean and D95 of reconstructed breast for treatmentplans without and with internal mammary node (IMN) inclusion.
differences in reconstruction procedures and their effect on fieldarrangements, as well as the use of the RPM system, enabling abetter target coverage with no heart exposure. Chung et al. usedstandard field arrangements, including the use of medial electronfields, and reportedly, they observed no differences in dosimetricresults between patients who underwent autologous reconstruc-tion and those who underwent 2-stage expander/implant recon-struction.15 Patients in our study exclusively had ADM-assisteddirect-to-implant reconstruction with anatomical implants.Because anatomical implants provide a gradual takeoff from themedial aspect of the chest wall (as opposed to round implants withsteep takeoff), we were able to cover IMNs without using a medialelectron field in all plans and minimize radiation exposure of skincovering the implant and to avoid hot spots at the field overlapareas with maximal target coverage.
A large dosimetric study conducted by Motwani et al.18 foundthat 52% of 112 patients who received PMRT after immediatebreast reconstruction, performed primarily with transverse rectusabdominis muscle flaps, had compromised treatment plans com-pared with 7% of matched controls (PMRT without immediatereconstruction). Moreover, 19% of patients had treatment planswith major compromises, and of those 67% were left sided. Overall,
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
Dmean
No IMN IMN
Dos
e (G
y)
Fig. 4. Dmean to the heart for treatment plans without and with internal mammarynode (IMN) inclusion.

0
5
10
15
20
25
30
No IMN IMNRightRight LeftLeft
p < 0.001 p = 0.004V
20 (%
)
Fig. 5. Mean total lung volume receiving doses of Z 20 Gy (V20) for left- and right-sided radiation treatment for plans without and with internal mammary node(IMN) inclusion.
M. Ben-David et al. / Medical Dosimetry 41 (2016) 142–147146
66% of patients had lymph node–positive disease, and incompleteIMN coverage (55%) was the most common problem; however,only 44% of the patients had modern 3D-CRT planning.
In contrast, in a retrospective study of intensity-modulatedradiation therapy delivered after the first or second stage ofimmediate expander/implant reconstruction in 41 patients treatedat Memorial Sloan-Kettering Cancer Center, PMRT was associatedwith excellent local control, with a 30-month control rate of 97%.25
However, although deemed acceptable by the authors, doses to theheart were higher compared with our study. The mean heart Dmean
was 2.81 Gy compared with 1.56 and 1.25 Gy for plans with andwithout IMN coverage, respectively, in our study. Of note, the onlypatient who received left-sided treatment with IMN irradiationhad a heart Dmean of 8.04 Gy.25 In contrast, the highest heart Dmean
observed in our study for left-sided treatment including IMNs wasonly 2.10 Gy. Achieving very low heart doses in this subgroup inour study was facilitated by the use of an RPM system in one-thirdof the patients who received left-sided treatment. This techniqueallows for significantly improved left breast coverage while keep-ing doses to the heart at acceptable levels,26,27 and is particularlyuseful for patients with anterior heart position.17 All patients inthe study by Koutcher et al.25 were treated with a supraclavicularfield, with a low mean lung V20 of 13.5%. The authors concludedthat PMRT using intensity-modulated radiation therapy is feasibleand results in clinically acceptable doses to the heart and lungs.25
In concordance with a recent study by Ho et al.,28 the heart andlung doses were higher when adding IMN to the target volume, inright and left reconstructions, as can be expected. However, themean doses to these structures were lower in our study, mostprobably because of the strict use of photon fields and the RPMsystem.
We acknowledge the limitations of our study, as individualanatomy differences before reconstructive surgery can influencepatient selection for either immediate 1-stage reconstruction vsexpander or autologous tissue use. In this study, patients may havecertain anatomic characteristics that differ from other grouped“immediate reconstruction” patients. Even for a homogenouspatient group, it has yet to be evaluated how the different anatomyof silicone implants or expanders may affect our ability to optimizetreatment plans. Additionally, to reduce the influence of using theRPM system in several patients, we evaluated all other details forthese patients and demonstrated no differences between groups.Finally, evaluating clinical outcomes as well as toxicity in correla-tion with the reported dosimetry end points is warranted andrequires further follow-up.
Using direct-to-implant reconstruction with anatomicalimplants, we observed excellent IMN coverage, even with left-sided reconstruction. This is probably because of the combined useof 3D-CRT, the use of the RPM system in patients with anteriorheart position, and the gradual medial takeoff of the anatomicalshaped implant. Our dosimetric findings are in concordance withthose reported by Koutcher et al.,25 Chung et al.,15 and Ohri et al.,19
who also used modern radiation techniques. An additionalstrength of our study is the uniformity of the reconstructionapproach, as a single plastic surgeon performed all constructions,and anatomical implants were used exclusively. Thus, implantvolume was the only major variable in the reconstruction proce-dure. Importantly, neither the planned target volume nor themedial distance had any effect on dosimetric outcomes owing tothe unique anatomical shape of the implant, which makes theapplication of medial electron fields unnecessary.
Conclusions
PMRT can be delivered effectively and safely after immediateimplant-based breast reconstruction, even for patients whorequire internal mammary chain radiation. The excellent targetvolume coverage and the low heart and lung exposures observedin our study demonstrate that immediate breast reconstructionper se is not an impediment to the delivery of high-quality PMRTby modern 3D-CRT technology. Reconstructive surgeons shouldconsider the use of anatomical implants for immediate breastreconstruction in patients requiring subsequent PMRT.
Acknowledgments
We thank Maayan Meir for preparing part of the radiationtreatment plans. Medical writing assistance was provided byRoland Tacke, Ph.D., of Evidence Scientific Solutions, Philadelphia,PA, United States, and funded by Allergan plc, Dublin, Ireland.
References
1. Early Breast Cancer Trialists' Collaborative Group (EBCTCG) Effects of radio-therapy and of differences in the extent of surgery for early breast cancer onlocal recurrence and 15-year survival: An overview of the randomised trials.Lancet. 366:2087–106; 2005.
2. Ragaz, J.; Olivotto, I.A.; Spinelli, J.J.; et al. Locoregional radiation therapy inpatients with high-risk breast cancer receiving adjuvant chemotherapy: 20-year results of the British Columbia randomized trial. J. Natl. Cancer Inst.97:116–26; 2005.
3. Marks, L.B.; Zeng, J.; Prosnitz, L.R. One to three versus four or more positivenodes and postmastectomy radiotherapy: Time to end the debate. J. Clin. Oncol.26:2075–7; 2008.
4. National Comprehensive Cancer Network. NCCN clinical practice guidelines inoncology. Breast cancer. Version 3.2013. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed July 31, 2013.
5. EBCTCG (Early Breast Cancer Trialists' Collaborative Group). Effect of radio-therapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: Meta-analysis of individual patient data for 8135women in 22 randomised trials. Lancet. 383:2127–35; 2014.
6. Colwell, A.S.; Damjanovic, B.; Zahedi, B.; et al. Retrospective review of 331consecutive immediate single-stage implant reconstructions with acellulardermal matrix: indications, complications, trends, and costs. Plast. Reconstr.Surg. 128:1170–8; 2011.
7. Salzberg, C.A. Focus on technique: One-stage implant-based breast reconstruc-tion. Plast. Reconstr. Surg. 130(5 suppl. 2):95S–103S; 2012.
8. Klein, E.E.; Kuske, R.R. Changes in photon dose distributions due to breastprostheses. Int. J. Radiat. Oncol. Biol. Phys. 25:541–9; 1993.
9. Trombetta, D.M.; Cardoso, S.C.; Facure, A.; et al. Influence of the presence oftissue expanders on energy deposition for post-mastectomy radiotherapy. PLoSOne 8:e55430; 2013.
10. Whitfield, G.A.; Horan, G.; Irwin, M.S.; et al. Incidence of severe capsularcontracture following implant-based immediate breast reconstruction with orwithout postoperative chest wall radiotherapy using 40 Gray in 15 fractions.Radiother. Oncol. 90:141–7; 2009.
11. Behranwala, K.A.; Dua, R.S.; Ross, G.M.; et al. The influence of radiotherapyon capsule formation and aesthetic outcome after immediate breast

M. Ben-David et al. / Medical Dosimetry 41 (2016) 142–147 147
reconstruction using biodimensional anatomical expander implants. J. Plast.Reconstr. Aesthet. Surg. 59:1043–51; 2006.
12. Kronowitz, S.J. Current status of implant-based breast reconstruction inpatients receiving postmastectomy radiation therapy. Plast. Reconstr. Surg.130:513e–23e; 2012.
13. Baschnagel, A.M.; Shah, C.; Wilkinson, J.B.; et al. Failure rate and cosmesis ofimmediate tissue expander/implant breast reconstruction after postmastec-tomy irradiation. Clin. Breast Cancer 12:428–32; 2012.
14. Friedman, T.; Davidovitch, N.; Scheflan, M. Comparative double blind clinical studyon round versus shaped cohesive gel implants. Aesthet. Surg. J. 26:530–6; 2006.
15. Chung, E.; Marsh, R.B.; Griffith, K.A.; et al. Quantifying dose to the reconstructedbreast: can we adequately treat? Med. Dosim. 38:55–9; 2013.
16. Feng, M.; Moran, J.M.; Koelling, T.; et al. Development and validation of a heartatlas to study cardiac exposure to radiation following treatment for breastcancer. Int. J. Radiat. Oncol. Biol. Phys. 79:10–8; 2011.
17. Pyatigorskaya, V.; Granot, H.; Ben-Ayun, M.; et al. Whole breast irradiationusing the RPM system—Better coverage of the target: left breast [abstract 782].Radiother. Oncol. 99(suppl. 1):S307–8; 2012.
18. Motwani, S.B.; Strom, E.A.; Schechter, N.R.; et al. The impact of immediatebreast reconstruction on the technical delivery of postmastectomy radiother-apy. Int. J. Radiat. Oncol. Biol. Phys. 66:76–82; 2006.
19. Ohri, N.; Cordeiro, P.G.; Keam, J.; et al. Quantifying the impact of immediatereconstruction in postmastectomy radiation: A large, dose-volume histogram-based analysis. Int. J. Radiat. Oncol. Biol. Phys. 84:e153–9; 2012.
20. Darby, S.C.; McGale, P.; Taylor, C.W.; et al. Long-term mortality from heartdisease and lung cancer after radiotherapy for early breast cancer: Prospective
cohort study of about 300,000 women in US SEER cancer registries. LancetOncol. 6:557–65; 2005.
21. Jagsi, R.; Griffith, K.A.; Koelling, T.; et al. Rates of myocardial infarction andcoronary artery disease and risk factors in patients treated with radiationtherapy for early-stage breast cancer. Cancer 109:650–7; 2007.
22. Hooning, M.J.; Botma, A.; Aleman, B.M.P.; et al. Long-term risk of cardiovasculardisease in 10-year survivors of breast cancer. J. Natl. Cancer Inst. 99:365–75;2007.
23. Chung, E.; Corbett, J.R.; Moran, J.M.; et al. Is there a dose-response relationshipfor heart disease with low-dose radiation therapy? Int. J. Radiat. Oncol. Biol.Phys. 85:959–64; 2013.
24. Darby, S.C.; Ewertz, M.; McGale, P.; et al. Risk of ischemic heart disease inwomen after radiotherapy for breast cancer. N. Engl. J. Med. 368:987–98; 2013.
25. Koutcher, L.; Ballangrud, A.; Cordeiro, P.G.; et al. Postmastectomy intensitymodulated radiation therapy following immediate expander-implant recon-struction. Radiother. Oncol. 94:319–23; 2010.
26. Korreman, S.S.; Pedersen, A.N.; Nøttrup, T.J.; et al. Breathing adapted radio-therapy for breast cancer: Comparison of free breathing gating with the breath-hold technique. Radiother. Oncol. 76:311–8; 2005.
27. Remouchamps, V.M.; Letts, N.; Vicini, F.A.; et al. Initial clinical experience withmoderate deep-inspiration breath hold using an active breathing control devicein the treatment of patients with left-sided breast cancer using external beamradiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 56:704–15; 2003.
28. Ho, A.Y.; Patel, N.; Ohri, N.; et al. Bilateral implant reconstruction does not affectthe quality of postmastectomy radiation therapy. Med. Dosim. 39:18–22; 2014.