Embed Size (px)
Citation preview

IMAGING OF SALIVARY GLANDS AND ASSESSMENT OF AUTONOMIC NERVOUS SYSTEM FUNCTION IN PRIMARY SJÖGREN'S SYNDROME
RAIJANIEMELÄ
Department of Internal Medicine,Department of Diagnostic Radiology,
University of Oulu
OULU 2004


RAIJA NIEMELÄ
IMAGING OF SALIVARY GLANDS AND ASSESSMENT OF AUTONOMIC NERVOUS SYSTEM FUNCTION IN PRIMARY SJÖGREN'S SYNDROME
Academic Dissertation to be presented with the assent ofthe Faculty of Medicine, University of Oulu, for publicdiscussion in the Auditorium 1 of Oulu UniversityHospital, on February 27th, 2004, at 12 noon.
OULUN YLIOPISTO, OULU 2004

Copyright © 2004University of Oulu, 2004
Supervised byDocent Markku HakalaProfessor Ilkka SuramoDocent Juhani Airaksinen
Reviewed byProfessor Yrjö KonttinenDocent Irma Soini
ISBN 951-42-7274-9 (nid.)ISBN 951-42-7275-7 (PDF) http://herkules.oulu.fi/isbn9514272757/
ISSN 0355-3221 http://herkules.oulu.fi/issn03553221/
OULU UNIVERSITY PRESSOULU 2004

Niemelä, Raija, Imaging of salivary glands and assessment of autonomic nervoussystem function in primary Sjögren's syndrome Department of Internal Medicine, Department of Diagnostic Radiology, University of Oulu,P.O.Box 5000, FIN-90014 University of Oulu, Finland 2004Oulu, Finland
AbstractThe purpose of the present study was to find reliable non-invasive methods for imaging salivaryglands and diagnosing primary Sjögren's syndrome (SS) and to evaluate autonomic function andcentral nervous system (CNS) disorders in patients with primary SS. The patient population consistedof consecutive patients with primary SS, who fulfilled the International classification criteria forprimary SS, from the Division of Rheumatology, Department of Internal Medicine in Oulu UniversityHospital.
Magnetic resonance (MR) imaging and MR sialography of parotid glands were performed on 27patients and 7 healthy controls and ultrasonography (US) of major salivary glands on 27 patients, 27healthy controls, and 27 symptomatic controls with sicca symptoms or salivary gland swellingswithout SS. MR imaging and US showed heterogeneous parenchyma or adipose degeneration of thegland in 81% and 78% of patients, respectively. MR sialography showed ductal system changes,narrowings and dilatations, or cavities in 96% of patients. One healthy control and 2 symptomaticcontrols had abnormal findings of parotid or submandibular glands on US. Other controls had normalfindings. The diagnostic specificity of US was 94%. Parenchymal structural changes on MR imagingand US were associated with anti-Ro/SSA positivity and weakly with the focus score index, but notwith salivary or tear secretion, age, disease duration, or features of systemic activity of the disease,such as hypergammaglobulinemia or systemic complications.
A comprehensive package of cardiovascular tests, including 24-hour heart rate variability,baroreflex sensitivity test with phenylephrine, Valsalva manoeuvre, deep breathing tests, and activeorthostatic test, were conducted on 30 patients and 30 healthy, age and sex-matched, randomlyselected population-based controls. No signs of autonomic dysfunction were found in patientscompared to controls in any of the tests. The test results were not associated with saliva or tearsecretion, age, disease duration, or clinical features of systemic activity of the disease.
A case of severe inflammatory CNS disease associated with primary SS was described, and aninvestigation of the relevant literature was made. Though inflammatory CNS disease is a possiblecomplication of primary SS, there is no consensus regarding its prevalence or significance in theliterature. Diagnostics and treatment are empiric.
In conclusion, MR imaging, MR sialography, and US yield such a definitive picture of theglandular changes in primary SS that they are promising alternatives for invasive examinations in thediagnostics of primary SS. Comprehensive cardiovascular tests revealed no signs of autonomicdysfunction in patients with primary SS compared to general population.
Keywords: central nervous system diseases, heart rate variability, Magnetic resonance imaging, sialography, ultrasonography


Acknowledgements
This work was carried out at the Departments of Internal Medicine and Diagnostic Radiology, University of Oulu, during the years 1999-2003.
I wish to express my sincere gratitude to Professor Antero Kesäniemi, M.D., Ph.D., Head of the Department, for his interest and support during the study. I owe to my warmest thanks to my doctoral supervisor, Docent Markku Hakala, M.D., Ph.D., for suggesting this topic to me and for his invaluable guidance and constant encouragement throughout these years. I am also indebted to my other supervisors, Professor Ilkka Suramo, M.D., Ph.D. and Docent Juhani Airaksinen, M.D., Ph.D., for their excellent guidance. Their expertise and contribution made this work possible.
I owe my sincere thanks to Professor Yrjö Konttinen, M.D., Ph.D., and Docent Irma Soini, M.D., Ph.D., for their valuable criticism and discussions during the preparation of this manuscript.
I am most grateful to my co-authors, Dr. Raija Takalo, M.D., Docent Eija Pääkkö, M.D., Ph.D., Dr. Sirkku Pikkujämsä, M.D., Ph.D., Professor Tuula Salo, D.Ds., Ph.D., Professor Heikki Huikuri, M.D., Ph.D., and Docent Markku Päivänsalo, M.D., Ph.D., for their skilful work, invaluable contribution and good collaboration during the study.
I would like to thank Ms. Pirkko Huikuri, R.N., and Ms. Päivi Karjalainen, R.N., for their technical assistance and Mr. Risto Bloigu, Ph.D., for his expert help with the statistical analyses. I express my gratitude to Ms. Sirkka-Liisa Leinonen, Phil.Lic., for revising the English language of this manuscript and the original papers. My thanks are also due to Ms. Anne Salovaara for her invaluable help and constant positive attitude in all kinds of issues.
I am thankful to the personnel of the rheumatological ward and outpatient clinic for their valuable help during this study and for the warm and favorable atmosphere in both research and clinical work. My thanks are also due to the personnel of the Department of Diagnostic Radiology for their interest and help.
I owe my special thanks to the patients who participated in the study for their enthusiastic co-operation, which made this work possible and rewarding.
I am grateful to all my friends and colleagues for support and joyful times at work and in free time.

Finally, I owe my warmest thanks to my family for all the joy, love and support during my life.
This work has been supported financially by grants of the Medical Research Fund, Oulu University Hospital and the Fund of University Pharmacy.
Oulu, December 2003 Raija Niemelä

Abbreviations
CNS central nervous system CT computed tomography HRV heart rate variability MR magnetic resonance PIH parenchymal inhomogeneity R-R interval R-peak-to-R-peak interval SS Sjögren's syndrome US ultrasonography


List of original publications
This thesis is based on the following original publications, which are referred to in the text by their Roman numerals: I Niemelä RK, Pääkkö E, Suramo I, Takalo R, Hakala M (2001) Magnetic resonance
imaging and magnetic resonance sialography of parotid glands in primary Sjögren's syndrome. Arthritis Rheum (Arthritis Care Res) 45:512-518.
II Niemelä RK, Takalo R, Pääkkö E, Suramo I, Päivänsalo M, Salo T, Hakala M (2003) Ultrasonography of salivary glands in primary Sjögren's syndrome. A comparison to parotid magnetic resonance imaging and magnetic resonance sialography. Submitted for publication.
III Niemelä RK, Pikkujämsä SM, Hakala M, Huikuri HV, Airaksinen KEJ (2000) No signs of autonomic nervous system dysfunction in primary Sjögren's syndrome evaluated by 24-hour heart rate variability. J Rheumatol 27: 2605-2610.
IV Niemelä RK, Hakala M, Huikuri HV, Airaksinen KEJ (2003) Comprehensive study of autonomic function in a population with primary Sjögren's syndrome. No evidence of autonomic involvement. J Rheumatol 30:74-79.
V Niemelä RK, Hakala M (1999) Primary Sjögren's syndrome with severe central nervous system disease. Semin Arthritis Rheum 29: 4-13.


Contents
Abstract Acknowledgements Abreviations List of original articles Contents 1 Introduction ...................................................................................................................13 2 Review of the literature .................................................................................................15
2.1 Salivary glands and production of saliva................................................................15 2.2 Diseases of salivary glands.....................................................................................17 2.3 Histopathology of salivary glands in Sjögren's syndrome (SS)..............................17 2.4 Development of classification criteria for SS .........................................................18 2.5 Methods to assess the structure of salivary glands in the diagnostics of SS...........20
2.5.1 Minor salivary gland biopsy ............................................................................21 2.5.2 Major salivary gland biopsy ............................................................................22 2.5.3 X-ray sialography ............................................................................................22 2.5.4 Scintigraphy.....................................................................................................23 2.5.5 Computed tomography (CT) ...........................................................................24 2.5.6 Ultrasonography (US)......................................................................................24 2.5.7 Magnetic resonance (MR) imaging .................................................................27 2.5.8 MR sialography ...............................................................................................29
2.6 Autonomic nervous system dysfunction .................................................................30 2.7 Assessment of autonomic function .........................................................................31
2.7.1 General ............................................................................................................31 2.7.2 Cardiovascular reflex tests...............................................................................31
2.7.2.1 Valsalva maneuver...............................................................................32 2.7.2.2 Deep breathing test..............................................................................32 2.7.2.3 Orthostatic test ....................................................................................33 2.7.2.4 Baroreflex sensitivity test with phenylephrine ....................................33
2.7.3 Heart rate variability (HRV) ............................................................................33 2.8 Autonomic nervous system manifestations in primary SS......................................35
2.8.1 Clinical picture of autonomic disorders...........................................................35

2.8.2 Autonomic function in tests .............................................................................36 2.9 Central nervous system (CNS) disorders in primary SS.........................................37
2.9.1 Prevalence .......................................................................................................37 2.9.2 Symptoms........................................................................................................39 2.9.3 Diagnosis .........................................................................................................40 2.9.4 Pathophysiology ..............................................................................................41 2.9.5 Treatment.........................................................................................................42
3 Aims of the study...........................................................................................................43 4 Subjects and Methods....................................................................................................44
4.1 Subjects ..................................................................................................................44 4.2 Methods ..................................................................................................................47
4.2.1 Clinical examination........................................................................................47 4.2.2 Standard laboratory tests and minor salivary gland biopsy .............................47 4.2.3 MR imaging.....................................................................................................47 4.2.4 MR sialography ...............................................................................................48 4.2.5 US....................................................................................................................48 4.2.6 Cardiovascular reflex tests...............................................................................49
4.2.6.1 Conventional cardiovascular reflex tests.............................................49 4.2.6.2 Baroreflex sensitivity test with phenylephrine ....................................50
4.2.7 24-hour HRV ...................................................................................................50 4.2.8 Investigation of the literature on CNS disorders in primary SS ......................51 4.2.9 Statistical methods...........................................................................................51 4.2.10 Ethical considerations....................................................................................51
5 Results ...........................................................................................................................52 5.1 MR imaging and MR sialography of parotid glands (I)..........................................52 5.2 US of salivary glands (II) .......................................................................................54 5.3 Comparison of US and MR findings (I,II)..............................................................55 5.4 Clinical associations of US and MR findings (I,II) ................................................55 5.5 Autonomic examinations (III,IV) ...........................................................................56 5.6 Clinical associations of autonomic test findings (III,IV)........................................58 5.7 CNS disorders in primary SS: A case and an analysis of the literature...................58
6 Discussion .....................................................................................................................60 6.1 Selection of patients and controls (I-V)..................................................................60 6.2 MR imaging, MR sialography, and US of salivary glands (I,II).............................61
6.2.1 Imaging findings and their classification.........................................................61 6.2.2 Clinical associations ........................................................................................62 6.2.3 Comparison to previous studies.......................................................................63 6.2.4 Roles of US, MR imaging, and MR sialography in the diagnosis of SS .........64
6.3 Autonomic nervous system function in primary SS ...............................................65 6.3.1 Cardiovascular autonomic function and clinical associations .........................65 6.3.2 Selection of tests..............................................................................................65 6.3.3 Aspects of the discrepancy in autonomic studies.............................................66
6.4 CNS involvement in primary SS: Unsolved entity .................................................67 7 Conclusions ...................................................................................................................69 References Original articles

1 Introduction
Sjögren's syndrome (SS) is a chronic autoimmune exocrinopathy characterized by dryness of the eyes and mouth and mononuclear cell infiltration of exocrine glands. About one third of patients may also have various systemic (fatigue, joint and muscle pain, Raynaud’s phenomenon) and visceral manifestations (hypothyreosis, chronic atrophic gastritis, renal tubular acidosis, etc.) and complications of the disease, such as an increased risk of lymphoma (1,2,3). The course of the disease is usually stable with a good prognosis and mild progression of sicca symptoms, but some patients may be affected by severe life-threatening complications (4-7). Most commonly, SS affects middle-aged women in their fifth or sixth decade. About 90% of the patients are female. SS can be divided into primary and secondary forms. Primary SS is a separate disease entity, while secondary SS is concurrent with another rheumatic disease. The prevalence of primary SS is estimated to be 0.6-4.0% of the world's population (8,9,10). It is generally under-diagnosed.
The diagnosis of primary SS is based on a combination of subjective and objective signs of the involvement of lacrimal and salivary glands and serological findings. Minor salivary gland biopsy and x-ray sialography are conventionally regarded the "corner stones" of diagnosis (11,12). However, they are both invasive examinations that cause inconvenience and a risk of complications to the patient, which is why new reliable, non-invasive methods, such as ultrasonography (US), magnetic resonance (MR) imaging, and MR sialography, for the detection of diagnostic glandular changes have been searched. The rapid technical development has increased the reliability and availability of these methods during the past few years.
The pathophysiology of sicca symptoms in SS is only partially known. The progression of lymphocyte infiltration and the destruction of salivary glands correlate poorly with the diminishing saliva secretion (13,14). As the autonomic nervous system modulates the function of exocrine glands in normal physiological situations (15), and antibodies to parasympathetic cholinergic muscarinic M3 receptors have been found in SS patients' sera (16), the role of the autonomic system in the pathogenesis of SS has become a matter of interest. Autonomic dysfunction might also have an impact on the prognosis of SS patients, since it is known to be associated with increased mortality (17). Autonomic symptoms have been described in connection with primary SS in case reports,

14
but their prevalence is unknown. The results of the few small controlled studies have been contradictory.
In addition to the autonomic nervous system, other parts of the neurological apparatus may also be affected by primary SS. Peripheral nervous system symptoms are well documented, while central nervous system (CNS) involvement is a controversial issue with regard to its frequency, significance, and cause (18,19).
This study focuses on the imaging of salivary glands by US, MR imaging, and MR sialography in order to find new non-invasive diagnostic methods for primary SS. The other aims are to examine autonomic function and to assess CNS involvement in primary SS.

2 Review of the literature
2.1 Salivary glands and production of saliva
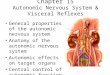
Stimulated saliva is produced by 3 pairs of major salivary glands: parotid, submandibular, and sublingual glands, whereas resting saliva is produced by minor salivary glands distributed throughout the mucosa of the oral cavity (Figure 1.). Salivary glands are exocrine glands composed of secretory units containing acinar and ductal regions. Acinar cells secrete fluid derived from the vascular bed around the acini and about 85% of the proteins, including glycoproteins, or mucins, in the saliva (20,21). During the passage of the secreted fluid through the ductal region, which is water-impermeable, some electrolyte flux occurs: sodium and chloride are reabsorbed, while potassium, bicarbonate, and some proteins are secreted (20,21,22). The acinar cells are either serous or mucinous. The parotid glands are serous glands, while the submandibular and sublingual glands are mixed, or serous-mucinous, glands, depending on the type of their acinar cells (22).
Salivary glands normally produce 600 to 1000 ml of saliva per 24 hours (22,23). If the amount of unstimulated and stimulated saliva is less than 0.1 ml/min and 0.7 ml/min, respectively, hypofunction of salivary glands is considered to be present (22). Many factors stimulate the secretion process, including mechanical, thermal, chemical, psychic, or olfactory stimuli, and the circadian rhythm modulates the secretion at the back ground (22). The basal flow, mostly secreted by minor salivary glands, is constant and necessary for the maintenance of oral health. When a stimulus such as a piece of food enters the mouth, the flow rate increases dramatically, and the composition of saliva changes. Major salivary glands are the main source of reflector secretion (21,22). The stimulus is mediated via the autonomic nerves (15,22). Parasympathetic and sympathetic activity regulate salivary secretion together. Activation of the parasympathetic nerves stimulates acinar cells, mainly via the muscarinic M3 receptors, to secrete watery fluid. The electrolyte and protein concentration of saliva is also modulated by the parasympathetic nerves. The role of sympathetic activation is more complex, but it seems to modulate the consistency, viscosity, and quantity of secreted saliva together with the parasympathetic system. (15,22)

16
Fig. 1. Localization of major salivary glands. The parotid gland, the largest salivary gland, has superficial and deep lobes, which are separated by the facial nerve. The parotid gland lies in front of the ear on the ramus of the mandible. The submandibular gland is situated below the mandible and the sublingual gland under the tongue. (Figure 102 from Palva T (ed) Korva-, nenä- ja kurkkutaudit. Helsingin yliopiston kirjapaino, Korvatieto 1982)
Saliva has many important functions for human well-being. It starts the digestion of food and protects mucosal membranes and teeth with its lubricant, buffering, and antibacterial properties. The pH and composition of saliva, especially the calcium and phosphate it contains and its buffering capacity, help to neutralize the acid attack and to remineralize the enamel that has been demineralized by the acid attack. At the same time, the high calcium and phosphate concentrations play an important role in the conversion of dental plaque to dental calculus. This is important for the health of dental support tissues, because dental calculus predisposes the support tissues to gingivitis and parodontitis. Saliva also helps the person to taste the food by dissolving the taste compounds and contributes to the regulation of water balance. (22,23) Hypofunction of salivary glands may cause various symptoms and complications. Patients with xerostomia complain of dryness of the mouth and lips, burning and smarting sensation, difficulties in speaking, chewing, and swallowing food as well as changed taste sensations. They may also have atypical caries, swellings of parotid glands, coughing episodes, and even changes in nutritional status and show an increased risk of aspiration pneumonia. Further, saliva contains growth factors that may have an influence on the generation and progression of gastrointestinal diseases, such as atrophic gastritis. (2,22,23,24,25)

17
2.2 Diseases of salivary glands
The most common diseases of salivary glands are acute and chronic sialadenitis, sialolithiasis, sialosis, and tumors (26). Acute sialadenitis may be caused by viruses or bacteria. The gland is enlarged and may be hypoechoic on US examination (27). Purulent parotitis is a possible complication of sialolithiasis, ductal stenosis, or trauma. The affected gland is swollen and tender, and abscesses may be found. Monoglandular chronic sialadenitis may be nonspecific or associated with sialolithiasis. In multiglandular cases, autoimmune origin, mainly SS, must be suspected. The cause of chronic sialadenitis, although not definitively determined, is probably multifactorial and includes decrease of salivation, stasis, and ascending retrograde ductal infection. Recurrent tenderness and swelling of the gland is a common symptom. (28) Chronic sialadenitis usually leads to a sausage-like sialographic pattern, with ductal dilatations and strictures, and sialectasies may also be seen (29). In US examination, hypoechoic inhomogeneous parenchyma is a common finding (27). Marked infiltration of chronic inflammatory cells, acinar loss, fibrosis and periductal lymphocytosis may be seen in histology (29). Sialosis involves bilateral enlargement of salivary glands, often related to diabetes mellitus, alcohol abuse, medication, or malnutrition. No inflammatory changes or focal lesions are seen in salivary glands. (26) Parotid tumors are usually benign, while tumors in the other salivary glands may be malignant as well. Pseudotumors may also occur. Multinodular or cystic lesions in salivary glands may be caused by chronic sialadenitis, sarcoidosis, HIV infection, and sometimes by tumors or lymphoma. (26,27)
2.3 Histopathology of salivary glands in Sjögren's syndrome (SS)
Macroscopic findings of major salivary glands. During the course of SS, normal salivary gland tissue is gradually replaced by lymphocyte infiltration. Macroscopically, salivary glands are either diffusely or focally affected by the disease process. The involved portion appears nodular in contrast to the adjacent normal tissue. The gland retains its normal lobular pattern and the general configuration of a salivary gland, though marked enlargement of individual lobes and cystic structures may be seen. (1,30,31)
Microscopic findings of major salivary glands. In the microscopic examination, the main findings are gradual mononuclear cell infiltration and ductal cell proliferation, which finally lead to the formation of epimyoepithelial cell islands (1,2,30). The mononuclear cell infiltration consists mainly of mature CD 4 T cells, while a minority, i.e. about 20%, are B cells, and plasma cells and macrophages may also be seen (2,24,32-37). The first signs of infiltration are frequently seen adjacent to ducts and blood vessels (2,30). Proliferation continues within the lobule, with subsequent atrophy and loss of acinar tissue, until complete replacement of glandular parenchyma by lymphoid tissue, with the exception of the ducts, may occur. Adipose degeneration with acinar atrophy may be found with both gross and mild lymphocyte infiltration (2,31).
The earliest findings in the ductal walls are minor changes of structure and organization accompanied by metaplastic changes of epithelial and myoepithelial cells.

18
Gradually, typical intraductal proliferation, narrowing of the duct, migration of lymphoid cells, and formation of a compact epimyoepithelial cell island occurs. Finally, depositions of hyaline-like substance can be seen. The hyaline-like mass may even completely replace the altered duct structures. (2,30) Epimyoepithelial islands have been described in 5.2% to 94% of parotid gland biopsies in SS patients in various series (1,2,30,38,39,40). Intralobular and interlobular ducts may show the kind of epithelial changes and proliferation that are seen in smaller ducts. Larger ducts may be dilated and form cysts (30,31). The lacrimal gland changes are similar to those in salivary glands (30,41).
Minor salivary glands. The characteristic pathological changes of minor salivary glands in SS were first described in the 1960s (42,43). Mononuclear cell infiltration resembles that of major salivary glands with focal, gradually increasing lymphocyte infiltration (24,34,44), but epimyoepithelial cell islands are rarely seen (24,33). Ductal changes, i.e. dilatations, ductal wall thickening, thinning, and oncocytic changes, have also been described (24,33,34,44). The ductal and parenchymal changes do not necessarily correlate with each other (33,34). Acinar atrophy, periductal fibrosis, and fatty infiltration may also be seen along with lymphocyte infiltration (24,34).
2.4 Development of classification criteria for SS
The diagnostics of SS has developed parallel to the increasing knowledge and understanding of the disease. In 1888, Hadden reported a patient with dry mouth and deficient lacrimal secretion, and in the same year, Mikulicz described a patient with symmetric swellings of the salivary and lacrimal glands due to lymphoid infiltration (2,30). Forty years later, Sjögren reported detailed clinical and histological findings of 19 patients with keratoconjunctivitis sicca and xerostomia, including 13 patients with chronic arthritis (1). The term 'Sjögren's syndrome' was introduced by Morgan in 1954 (45). He pointed out the histological similarity between Mikulicz's disease and Sjögren's syndrome. In 1956, Bloch and coworkers discovered that SS patients with and without connective tissue disease differed clinically and serologically from each other (2). The separate entities of primary and secondary SS were finally suggested by Moutsopoulos and colleagues in 1979 (46).
For decades, the diagnosis of SS was based on a triad of symptoms. The patients were required to have at least 2 of the 3 major components of the disease: keratoconjunctivitis sicca, xerostomia, and connective tissue disease (1). The impact of labial gland biopsy in the diagnostics began to increase in the 1970s, after the grading system of biopsy findings had been developed (33,34,44). It was not until 1980s that a number of more detailed empirical diagnostic criteria were introduced (47-50). The corner-stone of all these criteria is the focus score (the number of lymphocyte accumulations per unit of area) in minor salivary gland biopsy. Each of them also includes objective signs of keratoconjunctivitis sicca and decreased flow of either parotid, whole, stimulated, or unstimulated saliva. Serology (47), x-ray sialography (50), scintigraphy (48), exclusion criteria (47), and subjective symptoms of dry eyes and mouth (49,50) are included in

19
some of them. The sensitivity and specificity of these criteria vary. In general, they are considered to have high specificity, but low sensitivity.
In order to define criteria that would be universally accepted and applicable in both scientific communication and clinical work, the European study group introduced the preliminary European Community classification criteria for SS based on a multi-center validation procedure (51). A revision of the criteria to increase their specificity was proposed in 1996 (52). The European criteria have been broadly accepted since then, but other classification criteria are also still in use.
To establish even more widely accepted criteria, especially for research purposes, an international group of experts introduced the American-European (International) classification criteria for SS in 2002 (Table 1.)(53). These criteria are based on the European criteria with some specifications: to have primary SS, the patient must have either positive anti-Ro/SSA or anti-La/SSB antibodies (item VI) or focus score 1 ≥ in labial gland biopsy (item IV), lymphocyte foci must occur adjacent to normal-appearing acini, Schirmer's I test should be performed without anesthesia, other ocular dyes can be used instead of Rose Bengal, and hepatitis C and past head or neck radiation treatment are included in the exclusion criteria (53).

20
Table 1. International classification criteria for Sjögren's syndrome. (53)
Criteria Definition I Ocular symptoms: a positive response to at least one of the three selected questions:
Have you had daily, persistent, troublesome dry eyes for more than 3 months? Do you have a recurrent sensation of sand or gravel in the eyes? Do you use tear substitutes more than three times a day?
II Oral symptoms: a positive response to at least one of the three selected questions: Have you had a daily feeling of dry mouth for more than 3 months? Have you had recurrently or persistently swollen salivary glands as an adult? Do you frequently drink liquids to aid swallowing dry food?
III Ocular signs: objective evidence of ocular involvement defined as a positive result in at least one of the following two tests:
Schirmer’s I test, performed without anaesthesia (< 5 mm in 5 minutes) Rose Bengal score or other ocular dye score (> 4 according to van Bijsterveld’s scoring system)
IV Histopathology: In minor salivary glands (obtained through normal-appearing mucosa) focal lymphocytic sialadenitis, evaluated by an expert histopathologist, with a focus score > 1, defined as a number of lymphocytic foci (which are adjacent to normal-appearing mucous acini and contain more than 50 lymphocytes) per 4 mm2 of glandular tissue
V Salivary gland involvement: objective evidence of salivary gland involvement defined as a positive result in at least one of the following three diagnostic tests:
Unstimulated salivary flow (< 1.5 ml in 15 minutes) Salivary scintigraphy showing delayed uptake, reduced concentration and/or delayed excretion of tracer Parotid sialography showing the presence of diffuse sialectasias without evidence of obstruction in the major ducts
VI Autoantibodies: presence in the serum of the following autoantibodies: Antibodies to Ro(SS-A) or La(SS-B) antigens, or both
Rules for classification: For primary SS: In patients without any potentially associated disease, primary SS may be defined as follows: A/ The presence of any 4 of the 6 items is indicative for primary SS, as long as either item IV or VI is positive. B/ The presence of any 3 of the 4 objective criteria items (that is, items III,IV,V,VI). For secondary SS: In patients with a potentially associated disease (for instance, another well defined connective tissue disease), the presence of item I or item II plus any two from among items III, IV, and V may be considered as indicative of secondary SS. Exclusion criteria: Past head and neck radiation treatment, hepatitis C infection, pre-existing lymphoma, acquired immunodeficiency disease (AIDS), sarcoidosis, graft versus host disease, use of anticholinergic drugs (since a time shorter than 4-fold the half life of the drug).
2.5 Methods to assess the structure of salivary glands in the diagnostics of SS
The involvement of salivary glands is emphasized in the European and International classification criteria by including it into 2 separate objective items of the criteria: A

21
focus score ≥ 1 in minor salivary gland biopsy is a separate item (item IV), and the disease process of salivary glands can also be indicated by either unstimulated whole sialometry or by x-ray sialography or scintigraphy (item V). However, the involvement and structure of major salivary glands can also be demonstrated by biopsy or by modern non-invasive radiological methods, such as US, MR imaging, MR sialography, and computed tomography (CT). During the past 3 decades, major salivary gland biopsy has been replaced almost completely by minor salivary gland biopsy for fear of complications associated with the former. The role of modern non-invasive radiological methods in the diagnostics of SS is still open, though their availability and capability to visualize glandular structure have increased significantly in the past few years. The comparison of the diagnostic value of various methods is difficult, because of the rapidly improving technique and equipment and the different gold standards and classification criteria used in various studies.
2.5.1 Minor salivary gland biopsy
Focus score. The grading of labial salivary gland findings for the diagnostics of SS was developed in the 1960s and 1970s (33,34,41,44). It is based on lymphocyte infiltration of the gland. Mild diffuse infiltration is considered quite a nonspecific and focal accumulations of large groups of mononuclear cells a more specific finding. An aggregate of at least 50 mononuclear cells is a focus (41), and focus score is the number of foci per 4 mm2 (44). Focus score is considered the most accurate finding for SS in minor salivary gland biopsy (24,53,54), though it is somewhat unspecific and unsensitive. Lymphocytic foci can be found in up to 15% of healthy controls' salivary glands, and their incidence increases with advancing age (55,56,57), and foci have also been described in other diseases, such as myasthenia gravis (58). Further, foci may not be found in all labial glands of SS patients because of the focal nature of the disease, which is a problem especially with small biopsies and in the early stages of the disease (34,56). Tobacco smoking may also cause false negative finding (59). However, in another study with healthy subjects, smoking did not correlate with the focus score (57). When assessed in connection with the validation process of the European classification criteria, the sensitivity and specificity of focus score ≥ 1 were 82% and 86%, respectively (60).
Other findings. There is no consensus of opinions on the significance of other salivary gland findings. Acinar atrophy, periductal fibrosis, and fatty degeneration, usually combined with lymphocyte infiltration, have been considered nonspecific findings (24,34,55,61,62), although such a finding with focal sialadenitis has also been suggested to be a sign of advanced disease (2,30,33,63,64), and acinar atrophy to be a consequence of lymphocyte infiltration (2,30). According to the International criteria, to be diagnostic, the foci must be located adjacent to normal-appearing acini (53). Daniels & Witcher also suggested in 1994 that the lobules with lymphocyte infiltration should show no ductal dilatation or fibrosis (54).
Ductal findings, such as dilatations, ductal wall thickening, thinning, and oncocytic changes, have been suggested to be unspecific, since they can be found without heavy

22
lymphoid cell infiltration (24,33,34) and in healthy controls (55). On the other hand, ductal changes have been described as one of the main findings of the exocrine glands in SS with good diagnostic value and as a preliminary stage leading to the formation of typical epimyoepithelial cell islands and cystic structures (2,24,30,33,65).
The different histological appearances in salivary gland biopsies have been proposed to represent either different stages of the evolution of the same pathological process or discrete pathological entities leading to a common sicca syndrome (2).
Associations. Minor salivary gland changes have been shown to be associated with the presence of anti-Ro/SSA and anti-La/SSB antibodies (38,66-69), hypergamma-globulinemia (70), and saliva secretion (12,24,34), though the latter association has not been confirmed in a few more recent studies (14,70,71,72).
Complications. Labial gland biopsy is an invasive operation with inconvenience and a risk for complications to the patient. Local sensory loss has been described in up to 4 % of labial biopsies, and mild inconvenience is common for a few days after the operation, including local soreness, pain, swelling, or cutaneous echymoses at the biopsy site (24,39). The number of complications has decreased with the newer, less traumatic techniques (73).
2.5.2 Major salivary gland biopsy
Minor salivary gland biopsy has almost completely replaced major salivary gland biopsy in the diagnosis of SS, since it is considered reliable (24) and does not include the risks possibly associated with major salivary gland biopsies, such as scarring, fistula formation, or facial nerve damage (34). Goh and colleagues (74) described complications in 4.3% of patients with submandibular biopsies, but no complications have been described in several other studies with 4 to 105 patients per study (38,39,40,65,71,75).
When comparing major and minor salivary gland biopsies in the diagnostics of SS, parotid and sublingual biopsies seem more sensitive than labial biopsies (39,65,75,76), although an opposite report also exists (38). More abundant lymphocyte infiltration has been noted in submandibular (77) and lacrimal glands (71) compared with labial glands. There are no studies comparing the specificity of biopsies of different glands, but lymphocyte foci have been described in healthy controls' labial glands (56,57) and also in lacrimal and submadibular glands post mortem (78).
2.5.3 X-ray sialography
The first imaging method considered useful in the evaluation of the structure of salivary glands in SS was X-ray sialography, which can demonstrate sialectasies and the contour of the ductal system (11). The findings in SS patients' parotid glands have been traditionally classified according to the combination of the size of the sialectasies and the ductal system changes, though their correlation with each other is quite poor (11,79,80).

23
The classification in the filling phase is as follows: 1. Punctate: punctate ectasies less than 1 mm in diameter, normal main duct, decrease in the number and narrowing of the intraglandular ducts; 2. Globular: globules of contrast material 1 to 2 mm in diameter, main duct normal, intraglandular duct division invisible; 3. Cavitary: coalescence of the globules, which become irregular in size and distribution, and decrease in number; 4. Destructive: destruction of the gland parenchyma, marked dilatation of the main duct (11).
The diagnostic sensitivity of sialography has ranged from 66% to 87% in patients with suspected SS (80,81,82), while sialectasies or ductal dilatations have been reported in up to 30% to 40% of symptomatic controls (82,83). These findings have been proposed to reflect complications of secondary inflammation rather than the specific pathology of SS (79,84). However, the observer's experience may also be crucial to the results. In 2002, Kalk and coworkers (82) showed the sensitivity and specificity of sialography to be 95% and 33%, respectively, for trainees, while the results of experts were 87% and 84%, respectively, on the same images. In the validation process of the European classification criteria, the sensitivity and specificity of x-ray sialography were 72% and 92%, respectively (52).
The association of sialographic stages with histopathologic findings has been a matter of controversy. Though sialographic findings of parotid glands have not always been found to be related to the histopathology of the same gland (2) or labial gland findings (31), contradictory evidence also exists (85). Sialographic stages have been found to be related to labial biopsy findings (85), anti-Ro/SSA antibodies (81), and the duration of oral symptoms (82).
Complications. X-ray sialography can be performed with either water- or oil-soluble contrast media. Oil-soluble contrast medium is considered more reliable, but it may also cause more complications (11,80,82). Especially, if overfilling and retention of contrast medium occurs, the possible complications include pain, inflammation, pathological changes, and obliteration of the ducts. Foreign body reaction and focal necrosis are also possible as well as failure of cannulation, infection, and contrast medium reaction (11,80,86,87,88). Contrast medium has also been shown to penetrate into the glandular tissue through ductal walls and acini in diseased glands (31,79,84). Moreover, acute inflammation is a contraindication for x-ray sialography. On the other hand, a recent study on 100 parotid x-ray sialograms did not report any complications (82).
2.5.4 Scintigraphy
Scintigraphy performed with intravenous 99mTechnetium sodium pertechnetate has been used to examine salivary glands since the 1970s (89). The uptake, concentration, and secretion phases in salivary glands can be analyzed either qualitatively or quantitatively. The estimations of the sensitivity of scintigraphy vary from 73% to 85% (89,90,91) in patients with clinical diagnosis of SS, while specificity has been poor in a large number of studies (89,90,92-95). De Jager and co-workers (1984) concluded that scintigraphy is not able to differentiate between patients and controls (96). There is some evidence that

24
changes in submandibular glands may be better able to differentiate SS patients from controls than changes in parotid glands (94,97). In the validation process of the European classification criteria, the sensitivity and specificity of scintigraphy were 82% and 62%, respectively (52). Scintigraphy findings have been shown to be related to parotid and lacrimal flow rates (89,94,95,97), sialography (89,95), and focus score (95,97).
2.5.5 Computed tomography (CT)
As CT has low contrast resolution in soft tissues, it has not been considered the first choice in the examination of salivary glands (26). There is little experience of CT in the examination of SS patients. Heterogeneous parenchyma of salivary glands has been described (92,98), and in 1988, de Clerck and colleagues concluded that plain CT failed to differentiate patients from controls (83). Good results have been obtained in imaging salivary glands by newer CT methods (99), but there are no studies on patients with SS.
2.5.6 Ultrasonography (US)
US findings of salivary glands in SS were first described in the late 1980s (83,100). Since that time, several controlled studies assessing parotid and submandibular glands in SS have been conducted. The equipment applied in these studies has markedly improved, providing better resolution during the years.
Findings in SS. Normal salivary gland parenchyma has homogeneous appearance and is hyperechoic relative to the surrounding muscles. Sometimes, small normal hypoechoic lymph nodes can be demonstrated (83,101,102). The most typical finding of salivary glands in SS is parenchymal inhomogeneity (PIH) (100,102-109), which can be graded as mild (hypoechoic areas < 2 mm), evident (hypoechoic areas 2-6 mm), or gross PIH (hypoechoic areas > 6 mm in diameter) (104).
Other characteristics that have been observed, but have not been comparable to PIH with regard to their diagnostic value, are qualitatively or quantitatively assessed echogenicity of the parenchyma (83,110,111), the size of the gland (101-104,107), the visibility of the posterior border of the submandibular gland (104,107), hyperechoic bands (105,107,111), dilated main duct (101), presence of lymph nodes (104), and hypoechoic septa (112). In addition to parotid glands, submandibular glands have also been examined with contradictory results on diagnostic accuracy compared to parotids (83,103,104,107).
Correlation with histopathology. Based on a comparison of US findings with the histological appearance of the same gland, mild PIH with small hypoechoic areas on US seems to correspond to focal periductal lymphocyte aggregations and intraglandular dilated ducts, while larger hypoechoic or anechoic areas, cysts and cavities, may represent enlarged parotid lobules, where normal glandular tissue is replaced by lymphocyte infiltration, epimyoepithelial islands, or dilated ducts surrounded by dense

25
lymphocyte infiltration (100,101). Hyperechoic bands seem to correspond to interlobular fibrous tissue (101,102).
Diagnostic accuracy. The diagnostic sensitivity and specificity of US findings have been examined in several studies by comparing SS patients with both healthy and symptomatic controls with sicca symptoms or salivary gland swellings, or with controls who have a disease other than SS that may affect salivary glands. Several different classification criteria and variable gold standards have been used in these studies (Table 2). In the earlier studies, the sensitivity of US to detect changes suggestive of SS varied from 47% to 89% (103,104,105), and specificity from 82% to 85% (104,105), but mild PIH was regarded an unspecific finding in these studies. In more recent studies with newer equipment and patients selected by the European classification criteria, sensitivity has ranged from 76% to 87% (107,108,109), and specificity from 83% to 84% (107,109). Makula and colleagues reported 8% false positive findings (108). Some of the studies have concluded that chronic non-specific sialadenitis is difficult or impossible to differentiate from SS by US (102,104,105,111).
Table 2. Summary of studies on ultrasonography of salivary glands in Sjögren's syndrome.
Reference Patients and controls Registered findings
Results and conclusions
Bradus et al 1988 (100)
6 SS 1 Cystic structures in the glandular parenchyma
Cystic changes may be the rule in uncomplicated SS
de Clerck et al 1988 (83)
15 pSS, 4 sSS 2 33 controls 3
Decreased glandular echogenicity
US can be useful in investigation of sicca symptoms
Kawamura et al 1990 (103)
15 pSS, 9 sSS 4 23 5, 7 6 controls
Heterogenous pattern of parenchyma, echo intensity
Sensitivity 88% May be useful in diagnostics of SS
Corthouts et al 1991 (110)
16 SS 2 33 controls 6
Decreased echogenicity
Good correlation, better specificity, and poorer sensitivity compared to x-ray sialography Can be useful in the diagnostics of SS
de Vita et al 1992 (104)
27 pSS, 13 sSS 7 64 5, 26 3,6 controls
PIH grades (mild, evident, and gross)
Sensitivity 89%, specificity 85% Mild PIH unspecific
Takashima et al 1992 (101)
17 pSS, 13 sSS 4 10 controls 5
PIH grades, hypoechoic areas
Poor correlation with x-ray sialography Cannot discriminate SS from chronic sialadenitis Useful in follow-up

26
Table 2. Continued. Reference Patients and controls Registered
findings Results and conclusions
Makula et al 1996 (102)
53 pSS, 9 probable pSS 8 19 5, 44 6, 6 9 controls
PIH grades Good correlation with x-ray sialography, scintigraphy and focus score Sensitivity 91%, specificity 94% Evident and gross PIH diagnostic, mild PIH suggestive of SS
Ariji et al 1996 (111)
25 pSS, 19 probable pSS 1 83 5, 17 6 controls
Quantitative analysis of echolevels, hypoechoic foci
Good correlation with x-ray sialography Diagnostic accuracy 97% Useful in diagnostics, but does not discriminate SS from chronic sialadenitis
Youshiura et al 1997 (105)
24 pSS 4 22 5, 19 6 controls
Heterogenous hypoechogenicity, echo intensity
Poorer diagnostic accuracy compared to x-ray sialography Sensitivity 47%, specificity 82%, accuracy 63% Useful in diagnostics in advanced stages
Salaffi et al 2000 (107)
30 pSS 8 30 controls 3,6
PIH grades, size of the gland, posterior border of submandibular gland
Good correlation with focus score Sensitivity 77%, specificity 83% Can replace other methods in diagnostics of SS
Makula et al 2000 (108)
44 pSS 8 14 5, 11 3, 27 6 controls
PIH grades Sensitivity 87%, false positive 8% Mild PIH unspecific Useful first-line method when assessing salivary glands in SS
Yonetsu et al 2002 (109)
171 pSS 8 123 3 controls
PIH grades Sensitivity 76%, specificity 94%, diagnostic accuracy 84% As good as x-ray sialography in diagnostics of SS
Abbreviations: SS = Sjögren's syndrome, pSS = primary Sjögren's syndrome, sSS = secondary Sjögren's syndrome, US = ultrasonography, PIH = parenchymal inhomogeneity 1Clinical diagnosis, no common classification criteria used 2Classification criteria proposed by Fox (47) 3Symptomatic controls (sicca symptoms or salivary gland swellings without SS) 4Japanese classification criteria (50) 5Healthy controls 6Controls having a disease other than SS possibly affecting salivary glands 7Copenhagen classification criteria (48) 8European classification criteria (51) 8Controls with a disease probably not affecting salivary glands
Associations with other diagnostic methods. When US is compared with other diagnostic methods, the results are contradictory. No association has been found between US findings and salivary flow (107), but US results have been shown to correlate with x-ray sialography and labial gland biopsy findings (83,102), anti-Ro/SSA and anti-La/SSB positivity, and hypergammaglobulinemia (102,108), although there is also evidence suggesting a lack of correlation between US and sialographic findings (101). X-ray sialography seems to have better diagnostic accuracy compared to US (101,103,105,109), but there are no comparisons with newer US equipment.

27
2.5.7 Magnetic resonance (MR) imaging
MR imaging has high-contrast resolution of soft tissues, and it is thus a good choice for the examination of salivary glands (26). Since the beginning of the 1990s, a few reports with a small number of patients have been published on MR imaging in the evaluation of salivary glands in primary SS. Salivary glands have been studied with T1- and T2-weighted images, of which T2 has been shown to have better accuracy (114,115). Intravenous contrast media have also been used, but with no further information (13,63). The examinations have been carried out with 0.5 to 1.5 Tesla MR imagers and with head or neck coils. Parotid gland is the most commonly examined salivary gland, with one report of each of the following: submandibular (64), sublingual (116), and lacrimal gland (117). Since the first studies in SS patients, the capability of MR imaging to yield more definitive data of the glandular morphological changes in salivary glands has markedly increased due to the rapid technical development, which yields better resolution.
Findings in SS. Normal salivary gland appears homogeneous an has higher signal intensity compared to skeletal muscle (114). The most characteristic finding in SS is the heterogeneous parenchyma of glands (13,63,108,115). Parenchymal changes have been graded based on the nodularity of the parenchyma as normal, fine reticular, small nodular, medium nodular, and coarse nodular (13). Some patients have a characteristic glandular pattern with gross fat degeneration and hardly any parenchyma left in their glands. This fibroadipose degeneration has been suggested either to be nonspecific or to form a stage of its own (63,64,118). The quantitative assessment of the signal intensity of parenchymal tissue and its ratio to skeletal muscle have also been shown to differentiate between patients and controls (64,118). The other findings, which have been without diagnostic significance, are the differences in the size of the gland and lymph nodes (13). Abnormalities analogous to parotids have been found in submandibular and sublingual glands (64,116). Sublingual glands seem less severely affected compared to parotid and submandibular glands (116).
Correlation with histopathology. The nodular appearance with hypo- and hyperintense foci is proposed to reflect focal lymphocyte aggregates with increased interlobular fibrosis, fat, and dilated intralobular ducts, while greater nodules may represent enlarged lobules where parenchymal tissue is replaced by lymphocytic infiltrates and dilated ducts, but there is not much data on the histologic correspondence (31,114,118).
Diagnostic accuracy. The diagnostic accuracy of MR imaging has been evaluated in studies comparing SS patients with both healthy and symptomatic controls. Several classification criteria have been used in these studies (Table 3.). The first study that reported the sensitivity of MR imaging in SS revealed abnormalities in 71% of SS patients (63). A more recent study reported sensitivities of 82% or 100%, depending on the grade of the finding regarded as a sign of SS (108). Specificity has varied between 88% and 100% (13,63,108,115), although a diffuse unhomogeneous, or a fine reticular, finding has been considered nonspecific in some of the studies (13,108,114).
MR imaging is considered the method of choice if a salivary gland tumor is suspected in SS because of its capability to depict the full extent of the tumor and to demonstrate relationships with the adjacent anatomic compartments (26,31,119). Salivary gland lymphoma in SS has been described to be homogeneous, hypointense in T1- and

28
hyperintense in T2-weighted images, and with well-defined margins (119). Though MR images may not distinguish between benign lymphatic lesions and malignant lymphoma, they show the preferable site for biopsy (26,119).
Table 3. Summary of studies on magnetic resonance (MR) imaging and MR sialography of salivary glands in Sjögren's syndrome.
Reference Patients and controls Registered findings Results and conclusions Takashima et al 1991(114) (MR imaging)
5 pSS, 8 sSS 1 10 controls 2
Heterogeneous parenchyma with hypo- and hyperintense foci, intensity ratio
Poor sensitivity Suggestive for diagnosis of SS
Späth et al 1991 (13) (MR imaging)
24 pSS, 6 sSS, 6 susp. SS 1 40 2, 40 3 controls
PIH grades (fine reticular, small nodular, medium nodular, and coarse nodular)
Poor correlation with saliva excretion and focus score Specificity 100%, sensitivity better than in other imaging methods Accurate method for assessing salivary glands in SS
Valesini et al 1994 (63) (MR imaging)
15 pSS, 2 sSS, 6 susp. SS 1
10 controls 4
PIH grades, fibroadipose degeneration
Poor correlation with focus score Specificity 100%, sensitivity 71%, PPV 100%, NPV 55% Useful in diagnostics
Vogl et al 1996 (115) (MR imaging)
24 pSS, 6 sSS, 3 susp. SS 5 25 controls 4
PIH grades, fibroadipose degeneration, signal intensity
True positive 86%, false positive 7%, false negative 3% Could replace invasive examinations in the diagnostics of SS
Izumi et al 1996 (118) (MR imaging)
16 pSS, 12 sSS, 12 probable SS 5 30 2, 10 3 controls
Parenchymal heterogenicity, signal intensity
Good correlation with x-ray sialography and focus score Could replace classical methods in the diagnostics of SS
Makula et al 2000 (108) (MR imaging)
44 pSS 6 14 2, 27 3, 11 7 controls
PIH grades Focus score as gold standard, all grades of PIH regarded as positive: sensitivity 100%, specificity 40%; grades 2-3 regarded as positive: sensitivity 82%, specificity 100% MR imaging and US are useful and equally good in the diagnostics of SS

29
Table 3. Continued. Reference Patients and
controls Registered findings Results and conclusions
Tonami et al 1998 (122) (MR sialography)
43 pSS, 8 sSS 8 5 controls 2
Stages as in conventional x-ray sialography staging by Rubin & Holt (11)
High correlation with x-ray sialography and focus score Could replace x-ray sialography
Ohbayashi 1998 (123) (MR sialography)
35 SS 1 -"- X-ray sialography used as gold standard: specificity 100%, sensitivity 100% Highly useful in the diagnostics of salivary gland disease in SS
Tonami et al 2001 (124) (MR sialography)
80 pSS, 130 susp. SS 9
-"- Better diagnostic accuracy (83%) compared to scintigraphy (72%), PPV 100%, NPV 69% MR sialography is the most preferable method for the diagnostics of SS
Abbreviations: pSS = primary Sjögren's syndrome, sSS = secondary Sjögren's syndrome, PIH = parenchymal inhomogeneity, susp. SS = clinically suspected SS (sicca symptoms or salivary gland swellings, but diagnosis of SS or any other reason for the symptoms could not be confirmed), PPV = positive predictive value, NPV = negative predictive value, US = ultrasonography 1Clinical diagnosis, no common classification criteria used 2Healthy controls 3Controls having a disease other than SS possibly affecting salivary glands 4Controls with a disease probably not affecting salivary glands 5Classification criteria proposed by Fox (47) 6European classification criteria (51) 7Symptomatic controls (sicca symptoms or salivary gland swellings without SS) 8Japanese classification criteria (50) 9Diagnosis based on the histological appearance of minor salivary gland biopsy
Associations with other diagnostic methods. The MR imaging findings of SS patients have been found to be related to the presence of anti-Ro/SSA antibodies and hypergammaglobulinemia (13,108,115) as well as to pathology on US (108) and x-ray sialography (118) findings. Makula and co-workers (108) reported equal accuracy between US and MR imaging in the diagnostics of SS. The relationship between MR imaging and focus score has been a matter of controversy (13,63,118), and there is some evidence that MR imaging findings are not associated with saliva secretion (13). Adipose degeneration of the gland has been associated with higher grades of sialography and focus scores, and decreased saliva secretion (63,64,118), but it is also associated with increasing age (64) and hyperlipidemia (120,121).
2.5.8 MR sialography
MR sialography is a modification of MR imaging, in which the patient's own saliva functions as contrast medium in the ductal system. The main duct and the primary branches can be well visualized by MR sialography with modern equipment, but the more peripheral branches are usually less visible in MR sialography than in x-ray sialography (122,123,125,126,127). MR sialography reveals the ductal system in its physiological

30
state without artificial enlargement or extravasation caused by the contrast medium injection, and it also enables visualization of the peripheral portion of the ductal system in cases of obstruction and incomplete filling with external contrast medium (84,128).
The first preliminary reports of MR sialography in examining the salivary glands of SS patients were published in late 1990s (Table 3.). The findings on MR sialography were graded according to the conventional staging system of x-ray sialography (11) in these studies. In one report, MR sialography was shown to have a strong relationship with x-ray sialography, the agreement between the stages being 83%, and both sensitivity and specificity being 100%, when x-ray sialography was considered the gold standard (123). Compared with scintigraphy, MR sialography has had better specificity (100% vs. 50%), but poorer sensitivity (73% vs. 83%)(124), and an association has been found between MR sialography and focus score (122), with one report of each finding.
2.6 Autonomic nervous system dysfunction
Autonomic nervous system supplies and influences virtually every organ in the body. Its effective component consists of two major divisions, the sympathetic and the parasympathetic, which are regulated by a network of central autonomic nuclei and negative feedback regulation. Both divisions are tonically active and operate in conjunction with each other and the somatic motor system. The balance of activity between these two divisions helps to maintain homeostasis in the body exposed to changing external conditions. The autonomic reflex arc consists of sensory afferent nerves, coordinating central nuclei in the hypothalamus, midbrain and brainstem, and efferent pre- and post-ganglionic nerves leading to the target organ receptors. The sympathetic and parasympathetic divisions innervate cardiac muscle, smooth muscle, and glandular tissue and mediate a variety of visceral reflexes modulating the physical function of the main organ systems and exocrine glands. (15,129)
Autonomic disorders can be either localized or widespread, primary of unknown etiology or secondary to a variety of factors, such as diabetes mellitus, inflammatory and infectious conditions, connective tissue diseases, including rheumatoid arthritis, systemic lupus erythematosus, and systemic sclerosis, and several drugs (129,130,131). Clinical manifestations vary considerably, depending on the primary disorder. They may be derived from cardiovascular, sudomotor, gastrointestinal, ocular, respiratory, or urogenital systems and may include cerebellar or pyramidal features. Signs of several organ systems are frequently found to co-occur (132-135). The possible symptoms are postural hypotension, anhidrosis, heat intolerance, constipation, diarrhea, oropharyngeal dysphagia, anisocoria, Horner's syndrome, stridor, inspiratory gasps, apneic episodes, erectile or ejaculatory failure in male, nocturia, retention, or incontinence (129,131). Decreased saliva and tear secretions may also be detected (136). Autonomic dysfunction has been shown to be associated with increased all-cause mortality and, more closely, with cardiovascular and cerebrovascular mortality in various populations, including patients with diabetes (17,137,138) and myocardial infarction (139,140), the elderly (141), and the general population (142).

31
2.7 Assessment of autonomic function
2.7.1 General
Symptoms of autonomic nervous system dysfunction are nonspecific and start insidiously. Diagnosis is difficult or impossible on the basis of symptoms only. Examination of the autonomic nervous system is based on the evaluation of autonomic reflexes. Most of the data are derived from research on diabetic autonomic neuropathy (17,143,144). There are numerous non-invasive and invasive tests to assess autonomic functions. Indirect methods are normally used, and there are many factors confounding the interpretation of a test. Inter-individual as well as intra-individual variation in the results is marked and most of the tests are poorly standardized (145-148). Further, tests are nonspecific and unable to recognize the exact site of the dysfunction in the reflex arc or at the target organ response mediated by the receptor, post-receptional signaling, and the cell response. Many tests are also complicated, time-consuming, and unsuitable for routine use (131,145,148).
Clinically, cardiovascular tests are the most widely used and accepted indicators of autonomic neuropathy (149,150,151). Cardiovascular autonomic function can be examined with conventional reflex tests, such as the Valsalva maneuver, deep breathing test, orthostatic test, and sustained hand grip, or baroreflex sensitivity test with vasoactive agents and measurement of heart rate variability (HRV) (150,152,153). Other widely used methods, which are included in the recommendation of feasible tests for the screening of diabetic autonomic function, combined with cardiovascular tests, are tests of pupillary responses and sudomotor control, including thermally or chemically induced sweating or a quantitative sudomotor axon reflex test (149,154). There are also several other methods with variable standardization, such as, biochemical tests measuring plasma and urine catecholamines and metabolites, intra-neural recording of sympathetic activity, and passage examinations and manometry of the gastrointestinal canal (131).
2.7.2 Cardiovascular reflex tests
Cardiovascular reflex tests were developed for clinical use in the 1970s to diagnose diabetic autonomic neuropathy (152,155,156). Cardiovascular reflex tests assess mainly the function of the baroreflex system maintaining cardiovascular homeostasis during short-term alterations in blood pressure by measuring the changes of blood pressure and heart rate in response to physical stimuli (153). Today, blood pressure can be accurately measured non-invasively with Finapres finger cuff measurement based on the volume clamp method with infrared photoplethysmography, which provides beat-to-beat changes for computerized analysis (157). Usually, the tests are repeated and a mean value is considered as the result of the test. A battery of three to five tests should be used, because

32
the interpretation of a single test is difficult due to inadequate sensitivity and specificity (144,145,158).
Despite rigorous standardization, there are many confounding factors modifying the test results. The subject's response to a stimulus in a test depends upon a large number of individual factors, including age, gender, body mass index, race, pregnancy, consumption of tobacco and alcohol, and food intake prior to the test, excitement, stress, familiarity with the test, and motivation (144,145,159,160). The diagnostic accuracy of the conventional reflex tests decreases with increasing age (146,147,161). Some of the tests are not feasible in patients older than 50 years in spite of the age-related reference values (158). Centers have been recommended to create their own reference values, in order to minimize the confounding effects of local circumstances: equipment, testing and recording protocols followed, computer facilities, and special laboratory facilities, such as room temperature, during the tests (131,145,158).
2.7.2.1 Valsalva maneuver
To perform the Valsalva maneuver, the subject blows against a resistance for 10 to 15 seconds (152,162). Normally, with a rise of intra-thoracic pressure, venous return falls along with blood pressure, leading to reflex tachycardia due to vagal withdrawal and sympathetic activity. After the release of intra-thoracic pressure, a rebound overshoot blood pressure rise occurs because of persistent sympathetic outflow. The following baroreflex activation then results in a secondary fall in heart rate. (143,145,162) The changes of blood pressure and heart rate are measured. The result is usually expressed as a Valsalva ratio, which is the ratio of the longest R-R interval after the blow to the shortest R-R interval during the blow (162). The Valsalva ratio expresses mainly the parasympathetic function, though sympathetic activity co-stimulates the heart rate rise during the blow (145,147).
2.7.2.2 Deep breathing test
In the deep breathing test, the subject takes maximal breaths at a stable rate, usually 6 breaths per minute, in order to induce maximal heart rate changes between inspirations and expirations (137,155). The mean difference and ratio between the shortest and longest R-R intervals during each respiratory cycle is calculated. The heart rate change in the deep breathing test can be prevented by atropine, and the test is considered to measure parasympathetic function (137,143). The heart rate response to deep breathing is regarded as the single most sensitive and reproducible test among the traditional cardiovascular reflex tests (137).

33
2.7.2.3 Orthostatic test
The subject first lies down to stabilize his/her blood pressure before postural change, which is induced either actively by making the subject stand up or passively using a tilt table (163). After standing up, the blood pressure tends to fall, and sympathetic activity and vagal withdrawal lead to a rise in heart rate and blood pressure. The following vagal reflex overshoot leads to relative bradycardia. (143,145) The heart rate changes during standing can be assessed against the 30/15 ratio. On standing, the normal rise in heart rate is usually maximal at about the 15th beat, followed by slowing, which is most obvious at about the 30th beat (143). The blood pressure response to standing up is taken to be the difference between the measurements made while lying down and after one minute of standing up (143). The relative overshoot bradycardia response is mediated by the vagus nerve, and the blood pressure response by sympathetic nerves, with orthostatic hypotension reflecting the sympathetic impairment (143,145).
2.7.2.4 Baroreflex sensitivity test with phenylephrine
In addition to conventional, physically provoked reflex tests, baroreflexes can be assessed with the help of vasoactive agents (153), such as phenylephrine, which is an alpha adrenergic agonist that does not affect heart rate directly (164). Baroreflex sensitivity can be calculated by measuring the changes in R-R intervals (in ms) against the concomitant changes in blood pressure (in mmHg) achieved with phenylephrine (164). After a period of rest, with a stable heart rate and blood pressure, a bolus of phenylephrine is injected into a peripheral vein. Vasoconstriction induces a blood pressure rise, which is followed by reflex-mediated bradycardia. The changes in heart rate and blood pressure are recorded and a regression line calculated. The slope of the regression line represents baroreflex sensitivity, which is considered to reflect vagal reactivity. (138,153,164) However, sympathetic activity has also been related to baroreflex sensitivity (153,165).
The baroreflex sensitivity test with phenylephrine has been considered the gold standard among reflex tests because of its good prognostic value in heart disease patients, better specificity, and more reliable standardization compared to conventional tests (138,145,166,167). Baroreflex sensitivity measurement with phenylephrine is an invasive examination, which restricts its use in large populations, although it is considered safe based on the experience from large studies with heart disease patients (138,166). About 95% of subjects may have minor side-effects, such as transient headache and circumoral or facial paresthesia (138).
2.7.3 Heart rate variability (HRV)
Basis of the measurement of HRV. Heart rate variance in a healthy heart is caused by many factors, such as exercise and physical and mental stress. In addition, each cardiac

34
cycle, i.e. interval between sinus beats, varies periodically because of respiration, blood pressure regulation, thermoregulation, actions of the renin-angiotensin system, circadian rhythms, and other unknown factors. Such periodic rhythms are the predominant source of HRV. By using Holter recordings, these rhythms can be analyzed to provide a sensitive non-invasive measurement of autonomic input to the heart. (150,168)
HRV analysis began to replace conventional reflex tests in cardiological research in the 1980s. In recent years, it has also been adopted into the investigation of other diseases because of its better sensitivity (149,169,170) and reproducibility (171,172) compared to reflex tests. HRV can be analyzed either on short-term (1- to 2-hour) or on 24-hour Holter recordings. Short HRV recordings have been shown to correlate with reflex tests (173,174), but the correlation has been poorer for 24-hour variables (175,176). This can be explained by the nature of these tests. While reflex tests reveal the function of the autonomic system in provoked situations, 24-h HRV represents mainly the tonic balance of autonomic modulation (150). Measures of 24-hour HRV have been shown to have better sensitivity, reproducibility, and prognostic value compared to measures from short-term recordings (150,177). Further, 24-hour HRV is not dependent on the patient's co-operation and does not involve any placebo effect on the results. It also allows better quantitative and qualitative evaluation of the components of the sympathovagal modulation of cardiovascular function compared to conventional tests (150,168,169,177,178).
24-hour HRV has been shown to carry prognostic information in various populations, including patients with diabetes (174), myocardial infarction (138,139,140,166), and heart failure (179), and the elderly (141). Further, 2-hour HRV has also had prognostic value in a general population (142). HRV is influenced by many diseases and drugs. Coronary heart disease and hypertension may reduce HRV (180,181), while beta-blockers and angiotensin-converting enzyme antagonists may increase it (140,168,182). Gender also seems to have an effect on HRV, though the data on the effect have been somewhat conflicting (183,184).
HRV measures. There are three approaches to quantify HRV: the time domain, frequency domain, and non-linear approaches, which are based on the analysis of inter-beat intervals of normal beats determined from electrocardiography.
The results of time domain analysis, such as the mean and standard deviation of all R-R intervals, reveal the total amount of variability in heart rate, including fast and slow changes modulated by both the sympathetic and the parasympathetic nervous systems. (150,168,177)
Frequency domain analysis yields quantitative information about the overall variance in heart rate resulting from periodic heart rate oscillations at various frequencies (frequency-specific oscillations). Four frequency bands can be considered: high (0.15 – 0.4 Hz) frequency: 9 to 24 cycles per minute; low (0.04 – 0.15 Hz) frequency: 2.4 to 9 cycles per minute; very-low (0.003 – 0.04 Hz) and ultra-low (< 0.003Hz) frequency: less than 2.4 cycles per minute. The high-frequency component is mainly parasympathetically mediated and represents primarily respiratory variation. The low-frequency power is modulated by both the sympathetic and the parasympathetic nervous systems and affected by the oscillatory rhythm of the baroreceptor system (178). The physiological correlates of the very-low and ultra-low-frequency components are still unknown, but they are thought to represent the influence of the thermoregulatory, peripheral vasomotor,

35
circadian, and renin-angiotensin systems and may be mediated mainly by vagal outflow. (150,168)
The newer, less standardized, non-linear dynamic measures are based on the chaos theory and reflect the complex interactions of the multiple mechanisms in complicated real-life situations, such as hemodynamic, electrophysiological, humoral, autonomic, and CNS regulation that control heart beat. Approximate entropy (ApEn) and a short-term scaling exponent (α1) are the most often used non-linear measures. The former is a quantitative measure of the regularity, or complexity, of R-R interval data in the time series, and the latter represents the slope of the line, which relates fluctuation to window size or indicates the fractal-like behavior, or roughness, of the time series (150,185).
2.8 Autonomic nervous system manifestations in primary SS
2.8.1 Clinical picture of autonomic disorders
The prevalence of autonomic impairment in primary SS is unknown, although symptoms have been described in connection with peripheral sensory neuropathy (132,186-194), and there is one report of patients with autonomic symptoms only (195). About 20 to 30 % of SS patients with peripheral polyneuropathy have been found to have autonomic symptoms (132,192), and up to 87% of them have abnormalities in autonomic function tests in some series (194). However, Barendregt and co-workers (196) found no difference in autonomic tests between primary SS patients with or without sensory peripheral polyneuropathy. Patients with peripheral polyneuropathy and isolated sicca symptoms without systemic SS or anti-Ro/SSA or anti-La/SSB antibodies seem to have a higher incidence of autonomic dysfunction compared to those with systemic disease and anti-Ro/SSA positivity (186,194,197,198).
The clinical symptoms that have been most frequently described in SS patients are orthostatic hypotension, tonic Adie's pupil, and hypo- or anhidrosis (132,186-194). There are also descriptions of esophageal dysfunction and urinary retention (191), fixed tachycardia (132), and obstipation (195) coexisting with the symptoms mentioned above. Usually, the symptoms have been quite severe and progressive (132,191,192,193,195). Glucocorticosteroids have relieved the symptoms in most patients, but objective test results may not have improved (193,195). A case of pandysautonomia was treated with intravenous immunoglobulin therapy with good results (199).
Inflammatory process and vasculitis have been suggested as potential etiologies for autonomic impairment in SS. This is based on indirect data on the coexistence of vasculitic changes and autonomic symptoms with peripheral neuropathy in SS. Sural and cutaneous nerve biopsies of SS patients with peripheral neuropathy have revealed a loss of nerve fibers accompanied by vascular or perivascular mononuclear cell infiltration of endoneural or epineural small blood vessels (132,187,189,190), including 3 cases of necrotizing vasculitis (192,194). Also, a loss of nerve fibers with mononuclear cell infiltration has been demonstrated in dorsal root ganglia in some of these patients

36
(132,194). Inflammatory changes have also been found in autonomic ganglia and around nerve fibers in diabetic patients with autonomic disturbances (200).
2.8.2 Autonomic function in tests
Autonomic function in primary SS has been studied with conventional cardiovascular reflex tests (201-204), sudomotor (204,205) and pupillary (203) tests, and short-term HRV (206) with contradictory results: either parasympathetic dysfunction (201,203), both sympathetic and parasympathetic dysfunction (202,204), increased parasympathetic control (206), or no differences between patients and controls (203,207) have been reported. There are marked variations in the selection of patient and control groups, also various tests and different reference values have been used in these studies (Table 4).
None of the studies have reported any relationship between the test results and the salivary or tear flow of the patients, and no association has been found between autonomic tests and scintigraphy (201) or disease duration (205).

37
Table 4. Summary of studies on the autonomic function of patients with primary Sjögren's syndrome compared to healthy controls.
Reference Patients and controls Autonomic tests Results of patients Mandl et al 1997 (201) 19 patients1
56 age-matched controls Deep breathing test Tilt test
Parasympathetic dysfunction
Andonopoulos et al 1998 (202)
32 patients1 22 age and sex-matched controls
Valsalva maneuver Deep breathing test Standing up test Sustained hand grip test
Parasympathetic and sympathetic dysfunction in 88% of patients and 13 % of controls 2
Barendregt et al 1999 (203)
41 patients1 33 age-matched controls3
Valsalva maneuver Deep breathing test Tilt test Pupillography
Parasympathetic dysfunction 2 No differences between patients and controls by pupillography
Tumiati et al 2000 (206) 16 patients1 30 age-matched controls
1-hour HRV (time and frequency domain measures)
Parasympathetic control increased
Kovacs et al 2000 (205) 22 patients1 12 age and sex-matched controls
Skin blood flow response to carbachol stimulus
Lower response due to dysfunction at receptor or post-receptor level
Mandl et al 2001 (204) 30 patients 1,4 80 age-matched controls
Deep breathing test Tilt test Finger skin blood flow response to cold stimulus
Parasympathetic and sympathetic dysfunction
Barendregt et al 2002 (207)
43 patients1 30 sex-matched controls5
Tilt test6
(power spectral analysis of results)
No unequivocal differences between patients and controls
Abbreviations: HRV = heart rate variability 1European classification criteria (51) 2Not age-adjusted reference values 3Only pupillography was performed on controls 4Copenhagen classification criteria (48) 5From among the hospital and university staff 6Patients' blood pressure was measured invasively and controls' blood pressure with Finapress finger cuff
2.9 Central nervous system (CNS) disorders in primary SS
2.9.1 Prevalence
The reported prevalence rates of CNS manifestations connected with primary SS show wide variation. While clinical CNS disease was reported in up to 28% of SS patients in a clinic of internal medicine (208), some investigators have not detected clinical CNS disease in their rheumatological and neurological patients at all (209). There are no

38
controlled studies, and some patient series have been selected on the basis of having a neurological or an inflammatory vascular disease (Table 5.). Several different criteria for diagnosing primary SS and defining neurological involvement have been used in these studies. Further, studies have been conducted in different units, including rheumatological, neurological, or internal medicine clinics, or in centers particularly interested in neurological complications of autoimmune diseases (212,213).
Table 5. Summary of studies on the prevalence of central nervous system involvement in primary Sjögren's syndrome.
References Number of patients
CNS1 symptoms
Psychiatric symptoms
Cognitive symptoms
Additional information of patient characteristics and study clinic
Stolze et al 1960 (210) 139 2 1,4 % 20 % 93% pSS, 7% sSS, Rheumatol. clinic
Kaltreider et al 1969 (211) 109 2 1 % pSS and sSS patients, Rheumatol. clinic
Malinov et al 1985 (212) 40 2 40 % 20 % Patients with neuropsychiatric symptoms, Rheumatol. clinic3
Molina et al 1985 (213) 50 2 48 % 52 % 24 %4 Patients with peripheral inflammatory vascular disease, Rheumatol. clinic 3
Binder et al 1988 (214) 50 2 6 % 52 %4 Rheumatol. clinic Drosos et al 1989 (209) 52 2 0 % Rheumatol., neurol., psych. clinic Mellgren et al 1989 (192) 33 2 6 % Patients with peripheral nervous
system symptoms, Rheumatol., neurol. clinic
Andonopoulos et al 1990 (215) 63 2 1,5 % 77 %4 Rheumatol., neurol. clinic Hietaharju et al 1990 (216) 48 5 22 % 13 % Rheumatol., neurol. clinic Markusse et al 1992 (217) 50 5 6% 3% Rheumatol. clinic Manthorpe et al 1992 (218) 12 6 0% 50% Rheumatol. clinic Moll et al 1993 (219) 45 7 9% Rheumatol. clinic Moutsopoulos 1993 (19) 300 2 0.3 % 82 %8 Rheumatol., neurol. clinic Alexander 1993 (18) NR 2 20 - 25 % Patients since 1981, Rheumatol.
clinic 3 Spezialetti et al 1993 (220) 125 2 59 % 69 %4 91 pSS and 34 sSS patients with
CNS or inflammatory vascular disease, Rheumatol. clinic 3

39
Table 5. Continued. References Number
of patients CNS1
symptoms Psychiatric symptoms
Cognitive symptoms
Additional information of patient characteristics and study clinic
Mauch et al 1994 (221) 20 2 30 % Neurol. clinic Escudero et al 1995 (222) 48 5 23 % 29 % Neurol. clinic Tajima et al 1997 (193) 21 5 14% Rheumatol. clinic Govoni et al 1999 (223) 87 7 8 % Rheumatol., neurol. clinic Coates et al 1999 (224) 30 7 7% 20% Neurol. clinic Lafitte et al 2001 (208) 25 7 28 % Int. Med. clinic
Abbreviations: CNS = central nervous system, pSS = primary Sjögren's syndrome, sSS = secondary Sjögren's syndrome, Rheumatol. = rheumatological, neurol. = neurological, psych. = psychiatric , NR = not reported, Int. Med. = internal medicine 1Focal and/or diffuse central nervous system symptoms 2Clinical diagnosis, no specific classification criteria used 3 Tertiary center, including rheumatological, neurological, dermatological, psychiatric and clinical immunology departments 4Abnormality in neuropsychiatric or cognitive test 5Classification criteria proposed by Fox (47) 6Copenhagen classification criteria (48) 7European classification criteria (51) 8Neuropsychiatric and/or cognitive symptoms
2.9.2 Symptoms
The CNS manifestations described in primary SS are diverse and include focal and diffuse involvement of the brain and the spinal cord. Most frequently, the neurological complications are characterized by insidious onset, recurrent course, and often spontaneous recovery, but symptoms may also occur acutely or become chronic and cumulatively progressive (18,209,226,227). The focal symptoms may include motor and/or sensory disorders, aphasia, dysarthria, seizure disorders, visual loss, movement disorders, a brain stem syndrome, and a cerebellar syndrome, while the diffuse non-focal symptoms that have been described include acute or subacute encephalopathy, aseptic meningitis, cognitive dysfunction, dementia, and neuropsychiatric abnormalities (192,210-214,216,218,220,223,228,229). Spinal cord involvement may result in transverse myelitis, chronic progressive myelitis, a Brown-Sequard syndrome, neurogenic bladder, or lower motoneuron disease (18,212,213,221,227,228). Clinical neuropsychiatric symptoms and/or cognitive dysfunction have been described in 3% to 20% of the patients (210,213,217,222), while abnormalities in specific tests have been observed in 20% - 60% of patients in various populations (212,213,216,220). The most common psychiatric symptoms are depression, anxiety, hypochondriasis, and hysteria, often connected with neurological dysfunction (210,213-216,222,230). The most frequently seen signs of cognitive dysfunction are concentration deficits, memory impairment, and attention deficits (212,221). Migraine has been reported in 15% to 52% of patients (219,222,231). Though the cognitive and psychiatric symptoms are usually clinically mild, they may have a strong influence on the quality of the patient's life and lead to impairment of daily living tasks and work ability (230).

40
2.9.3 Diagnosis
The diagnosis of CNS disease in SS can be reliably set only after careful examinations to exclude other differential diagnostic diseases. The most commonly used examinations, such as brain MR imaging, cerebral angiography, electroencephalogram, or cerebral fluid analysis, are not specific or sensitive alone.
Brain MR imaging scans made in cases with CNS symptoms in primary SS have most frequently shown small regions of increased signal intensity predominantly in subcortical and periventricular white matter in the frontal and parietal lobes and less commonly in deep white matter or in deep and cortical gray matter on T2-weighted images (218,222,223,232,233). In some patients, one or more larger (> 1 cm in diameter) lesions may also be seen (222,223,234). Such lesions are typically seen in primary CNS angiitis
(235,236), but they are not specific and do not always have clinical relevance (218,224). These lesions are consistent with infarction, ischemia, edema, demyelination, periventricular gliosis, dilated perivascular spaces, atrophy, or no histopathological lesion in cerebral biopsy (18,237).
The incidence of these lesions with increased signal intensity increases with age in the general population, but they are considered to be rare in healthy individuals less than 50 years of age (18,237). Hyperintense lesions have been found in approximately 80% of SS patients with focal progressive neurologic dysfunction and in about 50% of patients with diffuse disease (18). Escudero and colleagues (222) found small hyperintense subcortical lesions in 51% of 48 primary SS patients with neurological symptoms and in 37% of age- and sex-matched controls from neurological or neuropsychiatric clinics. These findings are significantly more common in asymptomatic unselected primary SS patients than in healthy controls (224,238). Brain imaging may also show larger infarcts and cortical or cerebellar atrophy (18,233).
High signal intensity areas and cord swelling on T2-weighted images have also been demonstrated in the cervical, thoracal, and lumbar spine as well as on the conus medullaris and cauda equina (239,240,241). Spinal abnormalities have been shown to have a good correlation with the extent and distribution of symptoms (240).
CT. A brain CT scan is less sensitive than a MR imaging scan, though it may show larger infarcts and hemorrhages (18,222,242). Further, contrast enhancement of leptomeninges, non-enhancing lucencies, and cortical atrophy have been found in less than 20% of SS patients with CNS symptoms on CT scans (226,228).
Cerebral angiography. In highly selected cases of CNS involvement in SS, angiography has revealed abnormalities in small and medium-sized cerebral arteries, such as narrowing, dilatation, or occlusion of the vessels, delayed emptying, or anastomotic channels, in approximately 20% of patients (18,243). These changes are consistent with, but not diagnostic of angiitis. In patients with pathologically defined CNS angiitis, the sensitivity of angiography has been 60% to 85% (235,236) and specificity 26% (236). Normal brain MRI and angiography do not exclude active CNS disease in SS (18,229).
SPECT. There are some preliminary experiences of single-photon emission computed tomography (SPECT) in the examination of CNS disease in SS. It has shown cortical and basal areas of hypoperfusion localized predominantly in the frontal and parietal regions both in symptomatic and asymptomatic patients (223,244,245). In one report these areas

41
did not coincide with the areas affected on MR images (223), but in another they correlated with the abnormalities seen in neuropsychiatric tests (241).
Cerebrospinal fluid analysis. Cerebrospinal fluid analysis of SS patients with CNS disorder reflects involvement of the leptomeninges. The value for total protein is usually normal or mildly elevated, though it may occasionally be significantly elevated
(212,216,226,227,229). One or more immunoglobulin G oligoclonal bands can be detected in electrophoresis (18,212,223,229). The IgG index, which is indicative of intrathecal synthesis of IgG, is elevated in approximately 20% to 50% of patients with active focal disease (18,212,216,222,227,229). Mild mononuclear pleocytosis occurs in a subset of patients, and the leukocyte count may occasionally be notably high
(212,216,223,228). Electroencephalography is abnormal in about one to two thirds of SS patients with
active CNS disease showing nonspecific findings, such as focal slow-wave activity, spikes, seizure discharges, or general slowing (18,212,216,223,228,229). Electroencephalography may also show subclinical disease: Hietaharju and co-workers
(216) described abnormal findings in 48% of asymptomatic primary SS patients compared to 15% of controls.
Neuropsychiatric and cognitive tests. A wide range of neuropsychiatric and cognitive tests can be used. Some of these tests are standardized, but the experience of single tests in SS is limited (212,216,221,245). However, cognitive tests are proposed to be the most sensitive tests to detect mild subclinical CNS disease in SS (245).
2.9.4 Pathophysiology
The pathophysiology of CNS manifestations in primary SS is a matter of debate. There are only a few case reports of patients with CNS symptoms studied histologically so far. The brain or spinal biopsies of these patients have revealed unambigious vasculitis in a few cases (211,212,228), but a more typical finding has been mononuclear “vasculopathy”, i.e. perivascular mononuclear infiltration, which may extend into the surrounding brain parenchyma (18,229,233). Microinfarcts and microhemorrhages have also been described, and endothelial cells may be hypertrophied or damaged (18,132,233,242). Further, changes compatible with vasculitis have been detected in cerebral angiography in some SS patients with CNS disease (243). There is also indirect data suggesting vasculitis or an inflammatory etiology for CNS symptoms in SS. Peripheral vascular inflammatory disease has been associated with the presence of central and peripheral nervous system involvement in several studies (18,211,228), though this has not been confirmed in others (214,215,223).
While the presence of anti-Ro/SSA antibodies may be related to the most severe CNS symptoms (225), it is not associated with the occurrence of nervous system manifestations in SS (18,214,215,223,245). Other antibodies implicated in the pathogenesis of CNS symptoms in other autoimmune diseases, such as antiribosomal P, antineuronal, anticardiolipin, and antineutrophilic cytoplasmic antibodies occur very rarely in primary SS (18,219,220).

42
Still, there is no consensus of opinion concerning the pathogenesis of CNS disease in SS, and many investigators are of the opinion that CNS disease in SS patients is likely to be rare and most frequently secondary to the other concurrent diseases, such as diabetes or hypertension, rather than due to a rheumatic process (19,214,221).
2.9.5 Treatment
There are no controlled studies on the treatment of neurological complications in primary SS, and the medication is thus empiric. The knowledge is based on case reports of patients with variable clinical symptoms, usually a mixture of peripheral and CNS symptoms. The evaluation of the clinical response to medication is difficult because of the recurrent course of the disease with spontaneous remissions. It may not be assumed that the exact immunomechanism and the optimal treatment are identical in all patients (246). Finally, publication bias may select the cases with successful results.
Treatment is based on the assumption that the pathological process causing neurological symptoms is inflammation. Treatment is usually started with high-dose oral or intravenous corticosteroids, which are effective in some patients, while others do not respond (211,228,229,234,243,247). In cases of poor efficacy of corticosteroids, chlorambucillin (239) or cyclophosphamide has been added to the treatment (18,213,242,248). In cases with persistent insufficient efficacy or side-effects, plasmapheresis or intravenous immunoglobulin have been added, with a few reports of good responses (242,248). In acute transversal myelitis, high-dose corticosteroids combined with plasmapheresis (227) or pulse cyclophosphamide have been used successfully (18,241). Finally, anti-platelet therapy with low-dose acetylsalicylic acid has also been used to improve microcirculation and to prevent cerebrovascular accidents in these patients (246).
Because treatment with high-dose corticosteroids and cytotoxic agents may be potentially harmful, careful evaluation and observation of SS patients with signs of stable CNS disease is recommended. If the diagnosis is solid and the neurologic symptoms are progressive, leading to neurologic impairment, therapeutic intervention is indicated. Regimens similar to the treatment protocols of severe vasculitis have been recommended for the treatment of severe nervous system disorders in primary SS. (18,208,241,246).

3 Aims of the study
The purpose of the present work was to search for practical non-invasive diagnostic methods and to assess autonomic function and CNS involvement in primary Sjögren's syndrome. More specifically, the aims were to 1. Study MR imaging, MR sialography, and US findings of major salivary glands in
primary SS, compare the methods with each other, and evaluate their diagnostic value. (I,II)
2. Compare imaging findings with the patients' clinical features in order to search for prognostic factors. (I,II)
3. Study cardiovascular autonomic function in primary SS compared to a healthy population by conventional cardiovascular reflex tests, baroreflex sensitivity test with phenylephrine, and 24-hour HRV, and examine whether the results are dependent on the method used. (III,IV)
4. Search for associations between the cardiovascular autonomic test results and the clinical features of the patients. (III,IV)
5. Evaluate CNS involvement in primary SS by describing a case and investigating the relevant literature. (V)

4 Subjects and Methods
4.1 Subjects
A total of 65 consecutive patients with suspected or previously diagnosed primary SS, who visited the Rheumatological Division in the Department of Internal Medicine in Oulu University Hospital during 1997-1999, were evaluated in the present study. Thirty-eight of them were diagnosed to have primary SS. The diagnosis was based on the European classification criteria for primary SS (51). All patients were also required to have either positive anti-Ro/SSA or anti-La/SSB antibodies or a focus score ≥ 1 in minor salivary gland biopsy to confirm the diagnosis. The patients were invited separately into each study (I-IV) from among the patients who had been evaluated and found eligible by the time of the initiation of a study. Pregnant patients were excluded. Patients (n=27) with sicca symptoms or salivary gland swellings who did not fulfil the inclusion criteria for the patient group composed the symptomatic control group in study II. Their diagnoses included sarcoidosis (n=2), Kartagener's triad (n=1), idiopathic chronic sialadenitis (n=1), fibromyalgia (n=8), and anxiety or depression (n=4), and 6 of them had medication known to induce sicca symptoms. Three of the 29 and one of the 28 patients invited to participate in the studies I and II, respectively, refused. Only women were invited to participate in studies III and IV. All invited women agreed.
The 27 healthy age and sex-matched control subjects in the studies I and II were volunteers mainly from among the hospital staff. The control groups in the studies III (n=28) and IV (n=30) consisted of age and sex-matched healthy individuals recruited from among a population sample selected randomly from the register of general population of Oulu by their social security number. The demographics and other characteristics of the patients and controls are shown in Table 6.

Tabl
e 6.
Cha
ract
eris
tics o
f pat
ient
s with
pri
mar
y Sj
ögre
n's s
yndr
ome
and
heal
thy
and
sym
ptom
atic
con
trols
in st
udie
s I-I
V.
Stud
y I
Stud
y II
St
udy
III
Stud
y IV
M
RI a
nd M
RS
of p
arot
id
glan
ds
US
of m
ajor
saliv
ary
glan
ds
24-h
our H
RV
24
-hou
r HR
V, B
RS
test
, co
nven
tiona
l ref
lex
test
s
Cha
ract
eris
tics
SS p
atie
nts
Hea
lthy
cont
rols
SS
pat
ient
s Sy
mpt
om.
cont
rols
H
ealth
y co
ntro
ls
SS p
atie
nts
Hea
lthy
cont
rols
SS
pat
ient
s H
ealth
y co
ntro
ls
N
26
7 27
27
27
28
28
30
30
Fe
mal
es/m
ales
25
/1
6/1
26/1
27
/0
25/2
28
/0
28/0
30
/0
30/0
A
ge (y
ears
) 51
± 1
2 (2
2 - 6
7)
48 ±
12
(27
- 63)
50
± 1
4 (1
8 - 6
7)
45 ±
6
(29
- 56)
50
± 1
0 (2
8 - 6
7)
48
(26
- 67)
48
(2
7 - 6
2)
52 ±
11
(28
- 68)
52
± 1
1 (2
6 - 6
8)
Dis
ease
dur
atio
n (y
ears
)1 12
(1
- 30
)
12 ±
8
(1 -
30)
5 ±
4 (1
- 15
)
11
(1 -
36)
12
± 7
(1
- 31
)
Sicc
a sy
mpt
om o
f eye
s
27
22
0
Sicc
a sy
mpt
om o
f mou
th
27
24
0
Sc
hirm
er's
I tes
t
4.
6 ±
5.7
(0 -
22)
2.52
13 ±
11
(0 -
40)
7.52
15 ±
9
(5.5
-35)
11
2
USW
SF
0.9
± 0.
7 (0
- 3.
8)
4.1
± 4.
2 (0
.3 -
21)
4.4
± 3
(1.6
- 14
)
Ant
i-SSA
or a
nti-S
SB a
ntib
odie
s 19
20
1 0
20
22
Focu
s sco
re
2.5
± 1.
2
2.
3± 1
.63
(0.8
- 5.
0)
0.7±
1.3
3 (0
- 5.
0)
2.
9 ±
1.6
2.
3 ±
1.2
Extra
glan
dula
r man
ifest
atio
ns4
22
21
24

Tabl
e 6.
Con
tinue
d.
Stud
y I
Stud
y II
St
udy
III
Stud
y IV
M
RI
and
MR
S of
pa
rotid
gl
ands
U
S of
maj
or sa
livar
y gl
ands
24
-hou
r HR
V
24-h
our
HR
V,
BR
S te
st,
conv
entio
nal r
efle
x te
sts
Cha
ract
eris
tics
SS p
atie
nts
Hea
lthy
cont
rols
SS
pat
ient
s Sy
mpt
om.
cont
rols
H
ealth
y co
ntro
ls
SS p
atie
nts
Hea
lthy
cont
rols
SS
pat
ient
s H
ealth
y co
ntro
ls
Neu
rolo
gica
l sym
ptom
s5
13
12
Hyp
erga
mm
aglo
bulin
emia
17
18
17
C
ortic
oste
roid
trea
tmen
t 6
6
7
Hyp
erte
nsio
n/ C
AD
5 / 2
4 / 2
Bet
a/ C
a bl
ocke
r/ A
CE
inhi
bito
r
3 / 2
/ 2
3
/ 0 /
4
Res
ults
are
giv
en a
s m
ean
± st
anda
rd d
evia
tion
and
min
imum
to m
axim
um r
ange
()
or n
umbe
r of
sub
ject
s. A
bbre
viat
ions
: MR
I =
mag
netic
res
onan
ce im
agin
g, M
RS
=mag
netic
res
onan
ce s
ialo
grap
hy, U
S =
ultra
sono
grap
hy, H
RV
= h
eart
rate
var
iabi
lity,
BR
S =
baro
refle
x se
nsiti
vity
tes
t w
ith p
heny
leph
rine,
SS
= pr
imar
y Sj
ögre
n's
synd
rom
e, s
ympt
om. =
sym
ptom
atic
, USW
SF =
uns
timul
ated
who
le s
aliv
a flo
w p
er 1
5 m
inut
es, C
AD
= c
oron
ary
arte
ry d
isea
se, C
a bl
ocke
r = c
alci
um c
hann
el b
lock
er,
AC
E =
angi
oten
sin-
conv
ertin
g en
zym
e 1 T
ime
elap
sed
sinc
e th
e fir
st s
ympt
om: s
icca
sym
ptom
or s
aliv
ary
glan
d sw
ellin
g 2 M
edia
n 3 F
ocus
sco
res
of re
cent
ly (≤
1 y
ear)
ta
ken
biop
sies
. 4 Num
ber
of p
atie
nts
havi
ng o
ne o
r m
ore
extra
glan
dula
r m
anife
stat
ions
, whi
ch i
nclu
ded
thyr
oidi
tis,
myo
sitis
, cut
aneo
us v
ascu
litis
, lym
phad
enop
athy
, id
iopa
thic
thro
mbo
cyto
peni
c pu
rpur
a, p
arap
rote
inem
ia, l
arge
gra
nula
r lym
phoc
yte
lym
phoc
ytos
is, e
soph
agiti
s, at
roph
ic g
astri
tis, m
icro
scop
ic c
oliti
s, pa
ncre
atiti
s, pr
imar
y bi
liary
cirr
hosi
s, ce
liac
dise
ase,
leuc
open
ia, p
leur
itis,
or n
euro
logi
cal s
ympt
oms.5 N
umbe
r of p
atie
nts
havi
ng o
ne o
r mor
e ne
urol
ogic
al s
ympt
oms,
whi
ch in
clud
ed c
arpa
l tu
nnel
synd
rom
e, tr
igem
inal
neu
ralg
y, se
nsor
y po
lyne
urop
athy
, epi
leps
y, M
orto
n's m
etat
arsa
lgia
, mye
lopa
thy,
or c
ogni
tive
mem
ory
defic
its.

4.2 Methods
4.2.1 Clinical examination
Careful clinical examinations and interviews were conducted on all patients and controls, and their case histories were reviewed. Previous and concomitant diseases, medications, and symptoms were asked. Special emphasis was put on the symptoms and signs of possible glandular and extraglandular features of primary SS. Especially symptoms of eyes, mouth, and salivary glands were inquired about. Sicca symptoms were defined in accordance with the recommendations of the European classification criteria and lymphadenopathy as lymph node enlargement indicating biopsy. The data of previous and concomitant diseases were based on conventional clinical judgement. Schirmer's I test and 15 minutes' unstimulated whole sialometry were performed and sera were collected from all patients and the controls who participated in the studies I and II. Twelve-lead electrocardiography and cardiac echography had been performed earlier on all controls participating in the studies III and IV by a cardiologist.
4.2.2 Standard laboratory tests and minor salivary gland biopsy
The laboratory measurements were performed with standard methods in the Central Laboratory of Oulu University Hospital and in the Microbiological Laboratory of Oulu University. The laboratory tests included serum erythrocyte sedimentation rate, c-reactive protein, blood cell count, liver enzymes, serum and urine amylase, serum creatinine, immunoglobulin G, A, and M, thyroid-stimulating hormone, and a test of urinary sediment. Antinuclear antibodies were analyzed as well as antibodies to extractable nuclear antibodies, including anti-Ro/SSA and anti-La/SSB. Sera were also tested for antibodies to hepatitis C and human immunodeficiency virus. Minor salivary gland biopsies were taken only for diagnostic purposes. All biopsies, including the previously taken specimens, were microscopically re-evaluated by an experienced oral pathologists blinded to the clinical data. The focus score was determined on all biopsies.
4.2.3 MR imaging
MR imaging was performed by using a 1.5 T scanner (Signa, EchoSpeed, General Electric). A dual circular surface coil was positioned over both parotid glands. Fast-spin echo T1- (TR 500, TE 20, ETL 2, 512x192, 3 excitations) and fat-suppressed T2-

48
weighted (TR 3000, TE 100, ETL 16, 256x192, 2 excitations) oblique sagittal images were obtained parallel to the parotid glands. A field of view (FOV) of 10 cm with a slice thickness of 3.5 mm and a gap of 0.5 mm was used.
The structure of glandular parenchyma on T1- and T2-weighted MR images was categorized into 5 stages. Stage 0 = normal, stage 1= fine nodular, stage 2 = medium nodular, stage 3 = coarse nodular, and stage 4 = dendritic, or fibroadipose degeneration. The other findings registered were cavities and duct dilatations, the number of lymph nodes, and the appearance of the margin of the gland (smooth, globular, or diffuse). The size of the glands was assessed as square millimeters measured on hard copies. Two radiologists blinded to the clinical data analyzed all images separately, negotiating for consensus in cases of discrepancy.
4.2.4 MR sialography
MR sialography was performed using the single-shot fast-spin echo technique (TE 1000). 10-mm-thick single sagittal overlapping sections were obtained through the parotid glands with a FOV of 12 cm and a 256x256 matrix. MR sialography was repeated after stimulation by 2 ml of lemon juice concentrate.
On MR sialography, the duct system (internal and external main duct and primary branches) and the cavities were analyzed separately. The main duct was classified as normal (stage 0), showing an irregular wall contour or narrowed (stage 1), or dilated at >1mm in diameter (stage 2), and the primary branches as normal (stage 0), shortened, decreased in number, or not visible (stage 1), or dilated at > 1 mm in diameter (stage 2). In the final analysis, the stages of the main duct and the branches were combined. The cavities were classified with regard to their number: < 5, 5 to 20, or > 20, and size: < 1 mm, 1 to 2 mm, or > 2 mm in diameter. In the final analysis, a classification based on the size of the cavities was used. Two radiologists blinded to the clinical data analyzed all the images separately, negotiating for consensus in cases of discrepancy.
4.2.5 US
High-resolution US examination was performed on all patients and controls in study II by an experienced radiologist using a GE LOGIQ 500 MR3 (GE Medical Systems, Milwaukee, Wi, USA) real-time scanner with an 11 MHz linear transducer. The deep lobe of the parotid gland was also examined with a 9.6 MHz linear transducer. The length of the contact surface of the transducer was 38 mm, and resolution was 0.3 mm to an axial depth of 0-4 cm.
All patients and controls were examined in a supine position with the neck hyperextended, with a pillow under the shoulders, and with the skin covered by acoustic gel. All salivary glands were examined in the transverse and longitudinal planes. The height, width, and thickness of the submandibular and sublingual glands and the height

49
and width of the superficial lobe of the parotid glands were measured on the scanner display using electronic caliber. Any focal irregularities distinguishable in the homogeneous gland parenchyma were assessed for echogenicity compared with normal salivary gland tissue and measured with the electronic caliber. The sonographic data were recorded on the data sheet during the real-time imaging and documented on a film by a laser printer (3M 969 HQ Laser Imager, Minnesota, USA).
US images were analyzed independently by 2 radiologists blinded to the clinical diagnosis and the MR results. In cases of discrepancy, consensus was negotiated. The parenchymal structure of the glands was categorized into 5 stages. Stages 0-3 were defined as described earlier (102,104): stage 0 = normal, stage 1 = mild PIH (hypoechoic areas < 2 mm), stage 2 = evident PIH (hypoechoic areas of 2 to 6 mm), and stage 3 = gross PIH (hypoechoic areas > 6 mm). Stage 4 was defined as adipose degeneration of the gland (adipose tissue echogenicity and parenchymal atrophy). The other features that were registered were hyperechoic bands, the size of the gland, separate cysts (visible as hypoechoic or anechoic lesions), and ducts.
4.2.6 Cardiovascular reflex tests
Cardiovascular reflex tests were performed in the cardiological laboratory of Oulu University Hospital in standard conditions (143,147). The tests were performed between 0900 and 1200 a.m., the room temperature was kept stable at 20 to 22° C, a light breakfast was allowed more than 2 hours before the tests and coffee, tea, tobacco, and alcohol were not allowed for 12 hours before the measurements. During the tests, non-invasive arterial blood pressure was measured on a beat-to-beat basis by using the Finapres finger cuff method. The R-R intervals were obtained from surface electrocardiography and passed into an analog-to-digital converter. All data acquisitions and analyses were accomplished with a menu-driven software package (CAFTS, Medikro OY, Finland), and all data editing was checked manually.
4.2.6.1 Conventional cardiovascular reflex tests
Valsalva maneuver was performed in a sitting position by blowing into a rubber tube connected to an anaeroid manometer and maintaining a pressure of 40 mmHg for 15 seconds (152,155). The test was repeated 3 times. The result was expressed as a Valsalva ratio.
Deep breathing test. Six cycles of maximal inspiration and expiration at a rate of 6 breaths per minute were performed in a sitting position (137,155). The difference (DBD) and ratio (E/I index) between the shortest and longest R-R intervals during each respiration cycle were measured, and the mean values were calculated.
Active orthostatic test. The subjects stood up quickly from a lying position without any help (145,163). The shortest R-R interval at approximately the 15th beat after standing up

50
and the longest R-R interval at approximately the 30th beat after standing up were determined to obtain the heart rate response to standing (the 30/15 index). The postural change in blood pressure was measured separately for systolic and diastolic pressures as the difference between the pressures in lying and standing positions at one minute after standing up.
Reference values. Since the results of all heart rate-based reflex tests are strongly age-dependent, population-based, age-related reference values were used (147). Thus, the lower normal limit for the deep breathing difference ranged from 2 to 17, that for the 30/15 index from 0.99 to 1.39, and that for the Valsalva ratio from 1.10 to 1.45, depending on the subject's age. Postural blood pressure changes of more than 30 mmHg of systolic or 10 mmHg of diastolic pressure were considered abnormal (147).
4.2.6.2 Baroreflex sensitivity test with phenylephrine
The test was performed as follows: After a period of rest, with a stable heart rate and blood pressure, a bolus of phenylephrine was injected into a peripheral vein. The initial dose was 100 micrograms. The dose was increased in order to obtain at least 2 acceptable tests with an adequate (over 15 mmHg) rise in systolic blood pressure. The analysis window included the time from the beat that started the sustained rise in systolic blood pressure to the beat following the peak. Only regression lines with a correlation co-efficient greater than 0.8 and with a blood pressure rise > 15 mmHg were accepted for analysis. (153,164) Baroreflex sensitivity of less than 3.0 ms/mmHg was regarded as abnormal (166).
4.2.7 24-hour HRV
A 24-hour ambulatory electrocardiography recording was performed during the normal everyday activities out of hospital. The digitized data were transferred from the Delmar Avionics scanner into a microcomputer for an analysis of HRV. The measures of R-R interval dynamics were calculated for the entire 24-hour recording (III,IV) and also separately for the time representing the night hours (0-6 am) (III). The data were edited automatically and manually, eliminating carefully any premature beats and artefacts. All subjects had at least 18 hours of electrocardiography data, with at least 85% consisting of normal sinus beats. (150)
The mean and the standard deviation of all R-R intervals were used as time domain measures. Values less than 70 ms for the standard deviation of consecutive R-R intervals were defined as abnormal (140). The power spectrum densities were estimated using the fast Fourier method. Three frequency bands were considered in frequency domain analysis: very-low (0.003 – 0.04 Hz), low (0.04 – 0.15 Hz), and high (0.15 – 0.4 Hz) frequency. As non-linear measures, approximate entropy (ApEn) and a short-term scaling exponent (α1) were analyzed (150,185).

51
4.2.8 Investigation of the literature on CNS disorders in primary SS
Using PUBMED, a systematic search on English literature was performed for publications on CNS disorders in primary SS. At first, a combination of primary SS and CNS manifestations, disease, symptoms, or disorders were searched. Special attention was focused on the information of prevalence, pathophysiology, diagnostics, clinical picture, and treatment, which were separately searched in combination with CNS disease and primary SS. Reviews and original publications, including articles, letters, and case reports were accepted for preliminary screening, and the references in these articles were screened for other studies on the subject. Original publications were used in analysis.
4.2.9 Statistical methods
Statistical Package of Social Sciences (SPSS) 6.5 - 9.0 for Windows (Chicago, IL, USA) was used for statistical analyses as statistical software. The results of continuous variables are given as means + standard deviation and with 95% confidence intervals (III, IV) and as medians and minimum to maximum range when appropriate (II,IV). Variables with skewed distribution of absolute values were statistically analyzed after natural logarithmic transformation (III,IV). Independent samples t-test or Mann-Whitney U-test was used for group comparisons when appropriate with regard to the normal or skewed distribution of the variable, respectively. The associations between continuous variables and between continuous and ordinal variables were analyzed by Spearman's rank correlation (I,II,IV) or Pearson's bivariate correlation (III), and those between ordinal variables by linear-by-linear association and Fisher's exact test (I) or by Spearman's rank correlation (II). Cohen's kappa test was used for the analysis of inter-observer variation (II). Sensitivity, specificity, accuracy, and positive and negative predictive values were calculated as follows: sensitivity = true positive results / (true positive + false negative results); specificity = true negative results / (true negative + false positive results); accuracy = (true positive + true negative results) / total number of results; positive predictive value = true positive results / (true positive + false positive results); negative predictive value = true negative results / (true negative + false negative results) (II). P values < 0.05 were considered as statistically significant (I-IV).
4.2.10 Ethical considerations
All patients and controls gave their informed consent. The study protocols were approved by the Ethical Committee of the University of Oulu. The research was conducted according to the provisions of the Declaration of Helsinki.

5 Results
5.1 MR imaging and MR sialography of parotid glands (I)
Twenty-two (85%) of the 26 patients had abnormalities: parenchymal changes, i.e. nodularity or adipose degeneration, (n=21) (Table 7.), ductal dilatations (n=6), or cavities (n=5) in their parotid glands on MR images. One patient with ductal dilatation visible on MR images had normal glandular parenchyma. The MR imaging findings were equal bilaterally in 25 patients, while in 1 patient the parenchymal classification differed by 1 stage (2 vs. 3) between the contralateral glands. The findings based on the T1- and T2-weighted images differed in 5 patients, who were graded as stage 1 on T1 images and stage 2 on T2 images. The T1 and T2 stages were combined by choosing the higher stage available (T2) for further analysis.
On MR sialography, 25 (96%) patients had ductal system changes and 16 (62%) cavitary abnormalities (Table 7.). In 2 patients the cavitary classification differed by 2 stages (0 vs. 2) between the contralateral glands. The oral application of lemon juice had no impact on the sialography results.
One patient and 7 controls had normal findings in both MR imaging and MR sialography examinations.
Imaging correlates. The structural appearance of the parenchyma on MR images had a linear association with the ductal system stages (p < 0.05), but no correlation with the cavitary stages on MR sialography (Table 8.). The ductal changes in the external and internal main duct and the branches on MR sialography were associated significantly with each other (p < 0.001), as were the number and size of the cavities (p < 0.001), but the ductal changes did not correlate with the cavitary abnormalities (Table 9.). The margin of the gland correlated significantly with the structural classification (p < 0.001), but the size of the glands or the presence or number of lymph nodes were not associated with the other imaging findings. The cavities and ductal dilatations were visible on MR images if the cavity was > 3 mm and ductal dilatation > 1.5 mm in diameter on MR sialography.

53
Table 7. Magnetic resonance (MR) imaging and MR sialography classifications in patients with primary Sjögren's syndrome.
MR classifications Patients ( N = 26) MR imaging
Stage 0 = normal Stage 1 = fine nodular Stage 2 = medium nodular Stage 3 = coarse nodular Stage 4 = dendritic
5 2
10 2 7
MR sialography, ductal system Stage 0 = normal Stage 1 = narrowed, shortened, fewer in number Stage 2 = dilated > 1 mm
1
17 8
MR sialography, cavitary system Stage 0 = cavities not found Stage 1 = cavities < 1 mm in diameter (punctate) Stage 2 = cavities 1-2 mm in diameter (globular) Stage 3 = cavities > 2 mm in diameter (cavitary)
10 2 8 6
Table 8. Relationship between magnetic resonance (MR) imaging and MR sialography findings in patients with primary Sjögren's syndrome.
MR imaging classification MR sialography classifications 0 1 2 3 4
Total
Ductal stages1 0 1 1 1 3 2 7 2 3 17 2 1 3 4 8 Cavitary stages 2 0 3 2 3 2 10 1 1 1 2 2 2 3 3 8 3 4 1 1 6 Total 5 2 10 2 7 1 p < 0.05, 2 NS (non-significant)
Table 9. Relationship between ductal and cavitary findings on magnetic resonance sialography in patients with primary Sjögren's syndrome.
Cavitary stages Ductal stages1 0 1 2 3
Total
0 1 1 1 6 2 5 4 17 2 3 3 2 8 Total 10 2 8 6 26 1 NS (non-significant)

54
5.2 US of salivary glands (II)
Structure of parenchyma. Twenty-one (78%) patients had abnormal structure of glandular parenchyma on US examination. Eighteen (67%) patients had PIH or adipose degeneration of parotid glands, 18 (67%) PIH of submandibular glands (Table 10.), and 8 (30%) mild PIH (stage 1) of sublingual glands. Seventeen patients had abnormalities in both parotid and submandibular glands. The findings were bilateral in all patients. One healthy control had adipose degeneration (stage 4) in her parotid glands, and 2 symptomatic controls had evident PIH (stage 2) in their parotid glands and mild PIH (stage 1) in their submandibular glands. Other controls had normal findings.
Table 10. Relationship between structural classifications of parotid and submandibular glands by ultrasonography in patients with primary Sjögren's sydnrome.
Structure of submandibular gland 1 Structure of parotid gland Normal Mild PIH Evident PIH Gross PIH Total
Normal 8 1 9 Mild PIH 2 2 4 Evident PIH 1 1 3 5 Gross PIH 1 1 2 Adipose degeneration 2 4 1 7 Total 9 7 10 1 27 Abbreviations: PIH = parenchymal inhomogeneity 1 r = 0.73, p < 0.0001
Other findings. Hyperechoic bands were seen with all grades of parenchymal changes (0-4) in parotid glands (n=10) and with stages 1-2 in submandibular glands (n=8). Separate cysts and dilated ducts were only seen in parotid glands, in 11 and 2 patients, respectively. The size of the gland did not correlate with the parenchymal finding in any of the glands.
Comparison between glands. The parenchymal structural scores of parotid and submandibular glands were associated with each other (r = 0.73, p < 0.0001), the total agreement between stages being 48% (Table 10.), while there was no relationship between the parenchymal stages of sublingual and parotid or sublingual and submandibular glands. There were 3 patients with normal parotids, but with stage 1 changes in either sublingual (2 patients) or submandibular (1 patient) glands.
Diagnostic accuracy. The sensitivity of US was 78%, specificity 94%, accuracy 85%, positive predictive value 88%, and negative predictive value 88%, if PIH and adipose degeneration (stages 1-4) were considered as a sign of primary SS. Kappa test for inter-observer variation was very good, 0.83. The other salivary gland findings: hyperechoic bands, separate cysts or ducts, and the size of the gland did not yield any additional information for the diagnostics.

55
5.3 Comparison of US and MR findings (I,II)
The parenchymal scores of parotid glands on US and MR images were closely related to each other (r = 0.76, p < 0.0001), the total agreement between stages being 48% (Table 11.).
In a comparison of the US and MR methods, MR sialography was the most sensitive method (96%), followed by MR imaging (81%) and US (78%), to detect findings suggestive of SS (I,II). The specificity of US was 94% (II). The definite specificity of MR methods was not assessed, because MR examinations were only performed on 7 healthy controls, although all controls had normal findings (I).
Table 11. Relationship between structural classifications of parotid glands by ultrasonography and magnetic resonance imaging in patients with primary Sjögren's syndrome.
Structure on magnetic resonance imaging1 Structure on ultrasonography Normal Fine nodular Medium
nodular Coarse nodular
Dendritic Total
Normal 5 1 3 9 Mild PIH 4 4 Evident PIH 2 1 2 5 Gross PIH 1 1 2 Adipose degeneration 1 5 7 Total 5 1 10 3 7 27 Abbreviations: PIH = parenchymal inhomogeneity 1 r = 0.76, p < 0.0001
5.4 Clinical associations of US and MR findings (I,II)
The presence of anti-Ro/SSA antibodies was associated with the parenchymal findings on parotid MR imaging (p < 0.001)(I), MR sialography (p < 0.01)(I), and US (p < 0.05)(II), but not with submandibular or sublingual US (II). Anti-La/SSB positivity correlated with MR imaging (p < 0.05) (I). The focus scores of the 15 SS patients with recently taken minor salivary gland biopsies were related to the parotid changes on MR imaging (r = 0.6, p < 0.05), but the association with US findings was not significant (I,II). The ductal stages on MR sialography were associated marginally with the history of repeated parotid swellings (p < 0.05) (I). The results of neither US nor MR examinations were related to tear or saliva secretion, age, disease duration, the presence or number of disease complications, or hypergammaglobulinemia in the patients.
The patients with stage 4 changes (adipose degeneration) on MR imaging or US were all anti-Ro/SSA-positive and had manifestations of advanced glandular disease. Their focus score levels were higher (3.8 ± 1.7 vs. 2 ± 1), disease duration longer (8 ± 4.5 vs. 3 ± 2.8), and salivary flow rate lower (0.5 ± 0.6 vs. 1.2 ± 0.9), while they were younger (43 ± 10 vs. 50 ± 14) than the other patients (I,II). Ductal dilatations or cavities > 2 mm

56
in diameter on MR examinations were only found in patients with anti-Ro/SSA and age > 45 years, of whom 73% had these changes (I). The frequency of antibodies was equal in patients younger and older than 45 years. The only patient with normal MR images and sialography was Ro/SSA antibody-negative (I).
The healthy control subject with adipose degeneration of parotid glands on US had no history of sicca symptoms or other symptoms or diseases of parotid glands, and her tear and saliva secretion and submandibular and sublingual US findings were normal. One of the symptomatic controls with abnormal findings on US had Kartagener's triad with parotid swellings and a focus score of 5 in labial gland biopsy, but no other signs of SS, and the other had sarcoidosis, confirmed by parotid biopsy, with sicca symptoms and findings as well as parotid swellings. The other symptomatic control with sarcoidosis had sicca symptoms with normal saliva secretion and US of salivary glands. MR examinations were not performed on these controls. One symptomatic control developed persistent (> 4 years) local sensory loss as a complication of labial gland biopsy (II).
5.5 Autonomic examinations (III,IV)
There were no significant differences between the patients and the controls in any of the measures of 24-hour HRV or in HRV during the night-time hours (III). The result was repeated in study IV, in which no differences were found in patients compared to controls in 24-hour HRV, in conventional cardiovascular reflex tests, or in baroreflex sensitivity test with phenylephrine (Table 12, Figure 2.). One patient and 2 controls had abnormal results in a deep breathing test and 1 patient and 1 control in an orthostatic test, in which their 30/15 index values were low, but blood pressure responses were normal (III). There were no other abnormal test results.
When the patients on corticosteroid treatment [n=6 (III), n=7 (IV)] or with cardiovascular disease [n=6 (III), n=7 (IV)] and medication [n=7 (III,IV)] were excluded separately, there were still no differences between the groups, and when analyzed by subgroups, no differences emerged compared to the other patients or controls (III,IV).

57
Fig. 2. Individual values (•) and 95% confidence intervals for the means (•-•) of the frequency domain measures of 24-hour HRV, BRS, Valsalva ratio, E/I index and 30/15 index. For abbreviations see Table 12.
0.9
1.0
1.1
1.2
1.3
1.4
1.5
1.6
1.7
patientscontrols
30/1
5 in
dex
3
4
5
6
7
8
9
patientscontrols
LN
HF
(mse
c2)
5,0
5,5
6,0
6,5
7,0
7,5
8,0
patientscontrols
LNLF
(mse
c2)
0
5
10
15
20
25
30
35
40
45
patientscontrols
BRS
1,0
1,2
1,4
1,6
1,8
2,0
2,2
2,4
2,6
2,8
patientscontrols
Vals
alva
ratio
1,0
1,2
1,4
1,6
1,8
2,0
patientscontrols
E/I i
ndex

58
Table 12. Measures of 24-hour heart rate variability and autonomic reflex tests in patients with primary Sjögren's syndrome and in controls.
Controls Patients Variable Mean SD Median Mean SD Median
P
24-hour HRV R-R interval (ms) 836 91.6 810 844 106 833 NS SDNN (ms) 142 37.0 144 150 34.5 150 NS Ln(HF) (ms2) 5.54 0.80 5.56 5.57 0.85 5.37 NS Ln(LF) (ms2) 6.40 0.73 6.37 6.24 0.67 6.11 NS Ln(VLF) (ms2) 7.12 0.44 7.05 7.04 0.43 7.03 NS ApEn 1.06 0.18 1.09 1.04 0.14 1.06 NS α1 1.20 0.11 1.20 1.14 0.15 1.13 NS
Reflex tests Valsalva ratio 1.69 0.27 1.67 1.72 0.37 1.65 NS E/I index 1.25 0.12 1.24 1.25 0.17 1.20 NS DBD 15.8 6.53 15.0 15.9 9.25 15.0 NS 30/15 index 1.21 0.14 1.20 1.20 0.17 1.16 NS SBP change 12.2 10.9 12 13.2 11.3 10 NS DBP change 19.3 10.5 18 18.9 9.78 18 NS BRS 11.0 7.71 8.75 12.0 7.50 8.90 NS
The probability values are from Mann-Whitney 2-sample tests between the controls and patients. Abbreviations: SD = standard deviation; HRV = heart rate variability; SDNN = standard deviation of R-R intervals; Ln = natural logarithm; HF = high frequency; LF = low frequency; VLF = very-low frequency; ApEn = approximate entropy; α1 = short-term scaling exponent; DBD = deep breathing difference; SBP = systolic blood pressure; DBP = diastolic blood pressure; BRS = baroreflex sensitivity; NS = non-significant. ApEn and α1 results are from study III, the other results are from study IV.
5.6 Clinical associations of autonomic test findings (III,IV)
The spectral measures of 24-hour HRV correlated with age in both groups (r ranging from 0.64 to 0.69, p < 0.001) (III). None of the HRV parameters or reflex test results correlated with tear or saliva secretions, disease duration, sedimentation rate, focus score, occurrence of antibodies to anti-Ro/SSA or anti-La/SSB, or extraglandular disease manifestations (r ranging from 0.02 to 0.24) (III,IV).
5.7 CNS disorders in primary SS: A case and an analysis of the literature
A 24-year-old woman with primary SS and a five-month history of benign lymphadenopathy and myositis developed severe CNS symptoms: seizures and decreased

59
level of consciousness, with concomitant vasculitic lesions in her hands and a neurogenic bladder with urinary incontinence as a probable manifestation of spinal cord involvement. The diagnosis of CNS disease associated with primary SS was based on the clinical picture, the results of a brain MR imaging scan (multiple bilateral lesions of increased signal intensity in deep white and gray matter and in periventricular white matter), electroencephalography (mild general bilateral slowing), and cerebrospinal fluid analysis (positive IgG index, mild pleocytosis, high protein level), exclusion of other diseases, and response to immunosuppressive therapy (high-dose methylprednisolon and intravenous pulse cyclophosphamide). The diagnosis of primary SS had been made 5 years earlier. She fulfilled all 6 items of the European classification criteria, and she had the typical symptoms of SS: sicca symptoms, rapidly progressing dental caries, and Raynaud's phenomenon. She also had had recurrent joint swellings without radiological changes for two years at the early stages of the disease.
In the investigation of the literature, original articles, letters, and case reports from clinics of rheumatology, neurology, and internal medicine in Europe, United States, and Japan were found and analyzed. There were no controlled studies on the prevalence or treatment of CNS manifestations in primary SS. No follow-up studies on the prognosis were found, either. The diagnosis of primary SS was based on clinical judgement in most studies, and several different classification criteria were used in the others. Further, the methods of grading and diagnosing CNS disorders varied between the studies. Finally, even if all these factors are taken into account, there still is wide controversy about the etiology, significance, and prevalence of CNS disease associated with primary SS in the literature.

6 Discussion
6.1 Selection of patients and controls (I-V)
Selection of patients. The patients recruited into the present study were consecutive patients with diagnosed or suspected primary SS, who visited the Division of Rheumatology, Department of Internal Medicine in Oulu University Hospital, a referral center for 400 000 inhabitants, where most of the diagnoses of primary SS in the catchment area are confirmed. Thus, the patients represented the SS population of the area.
All patients recruited into the present study were required to fulfil the European classification criteria for primary SS (51) and to have either antibodies to anti-Ro/SSA or anti-La/SSB or a focus score ≥ 1 in minor salivary gland biopsy to confirm the diagnosis. The criteria that were used correspond to the International classification criteria (53), which are more specific, but less sensitive, than the original European criteria. As the main goals of the present study were to examine the imaging findings of salivary glands and to assess autonomic function in a population of primary SS patients, all consecutive patients, both previously (45% of the patients) and newly diagnosed (55% of the patients) ones, were included. This may have an effect on the diagnostic sensitivity of the present imaging studies (I,II). Earlier studies on the diagnostics of SS have included patients with either a previous or a new diagnosis, or both.
About 70% of the patients were anti-Ro/SSA-positive, which is quite a high proportion, but similar numbers have also been reported in several other series (4,5,209,217,249). Since minor salivary gland biopsies were taken in this study only for diagnostic purposes, only 55% of the patients had a new biopsy. There were 6 patients with previously diagnosed primary SS, of whom biopsy had not been taken. All of the 6 patients fulfilled the inclusion criteria, and either typical changes on x-ray sialography or epimyoepithelial cell islands in parotid biopsy had been found earlier. Thus, their diagnoses were considered solid.
Selection of controls. The selection of classification criteria also modifies the composition of the control group. This is important especially in the examination of the diagnostic methods. The symptomatic control group in study II consisted of subjects who

61
had sicca symptoms and/or salivary gland swellings and a suspicion of SS, but did not fulfil the inclusion criteria. The symptomatic control group was heterogeneous, representing the clinical real-life situation and differential diagnostic problems.
The healthy controls in the imaging studies of salivary glands (I,II) were age and sex-matched volunteers recruited mainly from among the hospital staff. It was assumed that the morphology of their salivary glands represented well that of the general population, although recruitment of volunteers in this way may result in inclusion of subjects with minor symptoms and health problems.
In the examination of autonomic functions, the selection of controls must be performed carefully to match them with patients as well as possible, since there are many confounding factors affecting the results, such as familiarity with the test and the testing environment (145,159). Also, matching for age and sex is important (147,183). Randomly selected population-based age and sex-matched controls were recruited into the autonomic studies (III,IV).
6.2 MR imaging, MR sialography, and US of salivary glands (I,II)
US, MR imaging, and MR sialography have been shown to be able to detect morphological changes of salivary glands in primary SS, but their role in diagnostics is open. In the present study, salivary glands were examined by modern high-resolution scanners. MR imaging showed abnormalities suggestive of SS in 85%, MR sialography in 96%, and US in 78% of patients, and the specificity of US was 94% when the clinical diagnosis of primary SS based on the European criteria with above mentioned specifications, corresponding to the International criteria, was used as gold standard. The definitive specificity of the MR methods could not be assessed reliably, because examinations were performed only on 7 healthy controls, although all controls had normal findings.
6.2.1 Imaging findings and their classification
Parenchymal findings. The most characteristic finding of SS patients' salivary glands on both US and MR imaging was inhomogeneous, or nodular, parenchyma (I,II). Because of the better spatial resolution of parenchyma achieved with the newer equipment, the old staging system (13) could not be used for MR imaging in the present study. The better resolution allowed many small nodules to be seen instead of a single large one, which is why a new parenchymal grading for MR imaging was created (I). US stages 0 to 3, i.e. normal to gross PIH, were defined according to the scoring system by de Vita and co-workers (104). Some patients, however, showed a characteristic glandular picture with abundant fat degeneration and hardly any glandular parenchyma left in their glands. As this finding differed significantly from the stages of PIH and could not be graded by the

62
same criteria, these glands were discretionarily graded separately into the stage 4 in both MR and US scoring (I,II).
The significance of the finding of adipose degeneration is a matter of controversy. There are some previous data to show that the amount of fat tissue increases in salivary glands with age (22,55,64) and in some diseases, such as serum hyperlipidemia (120,121). Therefore, it has been considered quite an unspecific finding. On the other hand, it has also been associated with SS (64,118), higher grades of x-ray sialography and focus scores, and decreased saliva secretion (63,64,118). Although one healthy control had adipose degeneration of parotid glands on US (MR examinations were not performed on her), the SS patients with a similar finding on US or MR imaging clearly showed features of advanced glandular disease, suggesting that, although this finding is somewhat unspecific, it may be associated with a more severe form of the glandular disease (I,II).
The other features registered, such as the size of the gland, lymph nodes, or hyperechoic bands, did not give any further diagnostic information (I,II).
Ductal system and cavities. The peripheral branches of the ductal system are less visible on MR sialography with the present equipment than on x-ray sialography (125,129) because of the poorer spatial resolution. The manual injection of contrast medium into the salivary ducts used in x-ray sialography also influences the results, as it may cause artificial dilatation of the ductal system, and contrast medium also penetrates into the glandular parenchyma through ductal walls and acini (31,79,84). Despite these differences, MR sialography has been shown to have a high correlation with conventional x-ray sialography (126). In the present study, the conventional staging system based on x-ray sialography could not be applied to MR sialography, because of the differences in visualization between the methods and the poor correlation between ductal and cavitary changes. Therefore, a new classification system was created and the ducts and cavities were graded separately. (I)
Associations between findings. The parenchymal classifications of MR imaging and US had a poor association with the ductal and cavitary changes on MR sialography (I,II). Only a marginal linear association between MR imaging and ductal changes could be seen (I). There is also some previous evidence suggesting that parenchymal and ductal changes do not develop simultaneously and parallel to each other (34,79), which suggests that separate pathological mechanisms may lead to parenchymal and ductal system changes in SS patients' salivary glands.
6.2.2 Clinical associations
The abnormal findings on parotid MR imaging, MR sialography, and US were associated with the presence of antibodies to anti-Ro/SSA (I,II). MR imaging also correlated with the focus scores of the recently taken minor salivary gland biopsies, and the ductal changes on MR sialography correlated with the history of parotid swellings, but otherwise the results did not correlate significantly with any other clinical features reflecting the severity of the disease, including salivary flow rate, disease duration,

63
presence of extraglandular manifestations, hypergammaglobulinemia, or age (I,II). These findings are in accordance with some previous data (13,14,24,63,108) and with a recent hypothesis suggesting that the inflammatory and destructive changes in salivary glands in primary SS may lead to antigen exposure and generation of anti-SSA antibodies, while other pathological processes, such as local interference of cytokines into the function of glandular tissue, including interleukine IL-6, tumor necrosis factor alpha, antibodies against muscarinic M3 receptors, and disturbances of the nitric oxide synthase system, may cause the defect in saliva and tear secretion (250). The correlation between MR sialographic findings and recurrent glandular swellings suggests that these findings may be caused by recurrent sialadenitis possibly secondary to reduced saliva secretion. Although no comparative studies have been conducted by MR sialography, it has been shown that chronic non-specific sialadenitis, typically characterized by recurrent glandular swellings during inflammations, may cause similar findings in x-ray sialography as SS (28). Clinically, however, these diseases can usually be differentiated from each other by their clinical features. While SS is usually a multi-glandular and systemic disease, non-specific sialadenitis is a mono-glandular disease without systemic manifestations (28).
Since imaging findings have a poor correlation with the clinical signs of disease, it seems that the clinical progression of systemic primary SS cannot be predicted by the imaging findings of salivary glands. The value of these methods in predicting the progression of glandular disease and in evaluating the effectiveness of treatment remains to be determined with longitudinal studies (251).
6.2.3 Comparison to previous studies
There is a wide variety of methods used in the examination of glandular changes in the diagnostics of primary SS. Also, the technology used in US and MR imaging studies has markedly improved during the past few years. In addition, wide variation in the selection of both classification criteria and gold standards for the definition of the diagnostic value of the findings makes any direct comparison between studies difficult or impossible.
The methodology used in the present study offered some advantages and disadvantages compared to previous studies with US, MR imaging, or conventional methods, including x-ray sialography, scintigraphy, and labial gland biopsy. In the present study, MR imaging, MR sialography, and US were performed with modern equipment, i.e. a special surface coil and a high-intensity magnetic field were used in MR examinations and an 11 MHz transducer in US, which yielded better spatial resolution compared to the older technology. Further, this was the first study reported in the English literature to combine MR imaging and MR sialography in the examination of SS patients (I). These methods give information on different aspects of glandular pathology. Since MR sialography takes only about 5 minutes to perform in connection with MR imaging, both should be performed to obtain complementary information. MR sialography with ductal system changes seems to be the most sensitive method to show early disease, while conventional parenchymal imaging gives a better picture of the glandular

64
parenchymal changes and the destruction of the gland (I). The ability of US, even with an 11 MHz transducer and modern equipment, to detect ductal system changes seems limited (II). Finally, this was the first study in the literature to examine all major salivary glands by US at the same time (II), which made it possible to compare the findings of separate glands with each other and gave the best sensitivity of US without decreasing specificity.
Though direct comparison between the results of the present and previous studies is impossible, it seems that US, MR imaging, and MR sialography are promising alternatives or supplementary methods to conventional diagnostic examinations. Multi-center studies comparing these methods with conventional examinations should be conducted to assess their accuracy in the diagnostics of SS.
6.2.4 Roles of US, MR imaging, and MR sialography in the diagnosis of SS
US, MR imaging, and MR sialography are continuously developing non-invasive methods which provide welcome alternatives to the conventional invasive examinations. Their use is likely to increase both in scientific research and in clinical practise in the near future. They all visualize the gland in its physiological state without artefacts caused by intraductal contrast medium or biopsy procedures, not to mention the lack of inconvenience and the risk of complications to the patient. With modern equipment, they can yield such a definitive picture of the glandular structural changes in primary SS that they can already be considered for clinical use in the diagnostics of primary SS, although they are not officially recognized in any classification criteria at the present. Comparative multi-center studies must be conducted to confirm their diagnostic value and cost-effectiveness in SS, before they can be widely accepted and included into the classification criteria for SS.
According to the present data, US seems to be a good candidate as the first-line radiological examination in the diagnosis of SS, because it is much cheaper and more widely available than the MR technique and gives an opportunity to evaluate all salivary glands easily at the same time. As MR sialography and MR imaging, especially in combination, seem to have better sensitivity and specificity compared to US, they could also be considered as the first choice methods, if available.
However, it has to be noted that the improving ability of US, MR imaging, and MR sialography to visualize the glandular structure in more detail does not necessarily increase their accuracy in the diagnostics of SS much further, since some of the glandular changes are not specific to SS, but may also be found in other diseases, such as sarcoidosis or chronic non-specific sialadenitis. Further, SS populations selected with the present criteria are heterogeneous, probably containing patients with variable pathological processes in their salivary glands leading to sicca syndrome. The diagnosis of primary SS will thus be based on a combination of clinical, laboratory, and imaging findings even in the future.

65
6.3 Autonomic nervous system function in primary SS
6.3.1 Cardiovascular autonomic function and clinical associations
Symptoms of autonomic dysfunction have been described in connection with primary SS (211), but their prevalence is unknown. The results of controlled studies have been contradictory showing either sympathetic, parasympathetic, or no autonomic dysfunction in SS patients (201,202,203,206,207). In the present study, the cardiovascular autonomic function of primary SS patients was compared to population-based healthy age and sex-matched controls from the same area by comprehensive cardiovascular methods. No signs of cardiovascular autonomic dysfunction were found in the patients compared to the general population (III,IV). The results were confirmed by all of the tests that were conducted, including conventional reflex tests, baroreflex sensitivity test with phenylephrine, and 24-hour HRV.
The spectral measures of 24-hour HRV correlated with age in both study groups (III), which was expected (150), but none of the results were related to tear or salivary flow (IV) or any other clinical features of the patients, such as disease duration, focus score, occurrence of anti-Ro/SSA or extraglandular manifestations, or the level of sedimentation rate (III). Thus, cardiovascular autonomic dysfunction does not seem to be associated with the symptoms or the progression of primary SS. However, it has to be noted that even comprehensive cardiovascular tests can not rule out or demonstrate local dysfunction in other sections of the autonomic system, including exocrine glands (16,250,252). The present results with no signs of cardiovascular autonomic dysfunction are in accordance with some previous data showing that the prognosis of mortality in primary SS is comparable to that in the general population (4,5,7).
6.3.2 Selection of tests
The investigation of the autonomic nervous system is complicated. The results of autonomic studies of SS as well as other diseases have frequently been variable, reflecting the numerous difficulties in the standardization and interpretation of these tests. (147,148)
Cardiovascular autonomic tests are most widely used and accepted as indicators of autonomic neuropathy (150,151). They are also better standardized than the other autonomic tests. Further, signs of cardiovascular autonomic dysfunction can be found to occur together with signs of other sections of the autonomic system, such as pupillary and sudomotor systems, in SS as well as in other diseases (132-135), although the correlation between individual test results may be poor (133). Orthostatic hypotension is the most commonly described autonomic symptom in primary SS. It has frequently been found to exist together with hypohidrosis and Adie's tonic pupil (186-195). The first controlled studies on autonomic function in primary Sjögren's syndrome, which were performed

66
with conventional cardiovascular reflex tests, found either sympathetic or parasympathetic dysfunction in SS patients (201,202). Later on, studies with short-term HRV and pupillary and sudomotor tests have been conducted, but the results have still been variable (203-207). There are no standardized tests to examine the autonomic regulation of exocrine lacrimal and salivary glands.
Due to the difficulties in the investigation of the autonomic nervous system and the discrepancies reported in the previous studies, several different cardiovascular tests assessing both autonomic reflexes in provoked situations and tonic autonomic balance were selected for the present study. In addition to conventional reflex tests (Valsalva maneuver, deep breathing test, orthostatic test), the examination package included a baroreflex sensitivity test with phenylephrine and 24-hour HRV, which have better specificity and sensitivity and are better standardized and more reproducible than conventional reflex tests (138,145,146,166,167,169,171,172). It was hoped that this would help to resolve some of the discrepancies reported in the earlier studies, although despite careful standardization of these tests locally, the direct comparison between studies conducted in different laboratories is difficult. It was also assumed that cardiovascular autonomic function reflects the general status of the autonomic nervous system of the patients, although it does not reveal possible local dysfunction in other sections of the autonomic system. Therefore, no direct conclusions on the eventual state of the autonomic system regulating the function of exocrine lacrimal and salivary glands cannot be drawn based on the present results.
6.3.3 Aspects of the discrepancy in autonomic studies
Apart from methodological variations, the possible explanations for the discrepancy in the results of autonomic function studies in SS include differences in the selection of patient populations and control groups. Unlike in the earlier studies, we recruited all the screened patients who fulfilled the primary SS criteria in order to keep the sample representative of all of our patients with primary SS, although this does not exclude the possible selection bias based on the referral system. When patients with cardiovascular disease and medication were excluded from the analyses, there still were no significant differences between the patients and controls. Since corticosteroid treatment may also influence autonomic function by improving small vessel vasculitis affecting vasa nervosum or decreasing the production of autoantibodies against neurotransmitter receptors, the patients on corticosteroids were also analyzed as a subgroup. Their results were similar to those of the other patients and controls. The average age and disease duration of the patients in the present study did not differ significantly from the other studies. Most of the patients also had immunologically active disease and extraglandular manifestations suggesting an active systemic disease.
Autonomic symptoms in primary SS have been described frequently in connection with peripheral sensory polyneuropathy (132,192) and sicca symptoms without systemic disease or anti-Ro/SSA (194,239). There were no patients with a clinical picture of this kind in the present series, only one patient had sensory polyneuropathy, and up to 70%

67
were anti-Ro/SSA-positive. This might to an extent explain the discrepancy between this and some of the earlier studies.
The healthy control group of the present study was derived from a random sample of the local general population matched for both age and sex with the patients. Neither the control subjects nor the patients were familiar with the reflex tests in advance. The comparability of the study groups in these respects is important because all these factors have a significant effect on the results of autonomic tests (147,180,183). On the other hand, because neither the patients nor the controls were familiar with the test procedure, inadvertent variation in the conventional reflex test results caused by confounding factors, such as fear or anxiety, might have influenced the results. This must be taken into consideration in the evaluation of the conventional reflex test results, particularly because no calculations were performed on the power of the present experimental setting, which makes type II beta error possible. However, the effect of confounding factors is much more limited on the baroreflex sensitivity tests with phenylephrine and especially on 24-hour HRV.
The variable results of the autonomic studies make the evaluation of systemic cardiovascular autonomic dysfunction associated with primary SS difficult. This, in combination with the wide inter-individual variation in the autonomic function test results of healthy subjects (138,147) and publication bias prone to favor studies with "positive" results, may lead to different results in small studies performed with relatively unspecific, insensitive, and poorly standardized methods.
6.4 CNS involvement in primary SS: Unsolved entity
Cases of definitive active inflammatory CNS disease have been described in patients with primary SS in the literature. However, there are no controlled follow-up studies to confirm a causal association between CNS disease and primary SS (253). The reports of the prevalence vary widely: While some authors report CNS disease in 22% to 28% of patients (208,216), others find it very rarely or never (19,209).
There are several confounding factors that may explain the controversy in the reports. First of all, diagnoses of both primary SS and CNS disorders are complicated due to the lack of specific methods. In addition, the wide range of clinical symptoms and the variable course of the disease with spontaneous remissions make the diagnosis of CNS symptoms in autoimmune diseases difficult. Also, the clinic where the study is conducted may have an impact on the results. In other words, studies conducted in rheumatological, neurological, or general internal medicine clinics, or in centers especially focused on the CNS involvement of autoimmune diseases may yield different results. Finally, genetic and environmental factors may predispose some patient populations to CNS disorders.
The patient in the present report (V) had the typical symptoms of primary SS. She did not fulfil the criteria of any other connective tissue disease, and all of the 6 items of the European classification criteria for primary SS were present. She had antibodies to anti-RNP, which are typical of mixed connective tissue disease, but they are also seen in 6% of primary SS patients (4). The diagnosis of rheumatic CNS disease associated with

68
primary SS was based on the clinical picture, the results of a brain MR scan, an electroencephalogram, cerebrospinal fluid analysis, the exclusion of other diseases, and the good response to immunosuppressive therapy.
The increasing interest in the topic, the development of more accurate and widely available diagnostic methods for the detection of CNS disease, and the widely accepted classification criteria for primary SS will provide chances for better focused research and yield more information about the nature of CNS disease in primary SS in the future.

7 Conclusions
1. US and MR imaging of salivary glands in primary SS show heterogeneous, or nodular, glandular parenchyma, or adipose degeneration of the gland. MR sialography depicts the contour of the ductal system: narrowings and dilatations of the main duct and primary branches, and peripheral cystic changes, or cavities. Parenchymal findings have a poor association with ductal system changes. The findings of parotid and submandibular glands on US have a good correlation with each other, though adipose degeneration is only seen in parotid glands. Sublingual glands are less severely affected. Among the methods tested in the present study, the best diagnostic sensitivity is achieved with MR sialography, followed by MR imaging and US. Examination of all major salivary glands yields the best sensitivity of US without decreasing specificity.
2. US, MR imaging, and MR sialography conducted with the modern technology yield such a definitive picture of glandular structural changes in primary SS that they are promising alternatives to the conventional invasive examinations in the diagnostics of primary SS. To be widely accepted and included into the classification criteria of SS their diagnostic value and cost-effectiveness must be confirmed in comparative multi-center studies.
3. Morphological changes of major salivary glands on US, MR imaging, and MR sialography are associated with anti-Ro/SSA-positivity, but they are not associated with saliva secretion or with the parameters that reflect the systemic activity of primary SS, such as hypergammaglobulinemia, disease duration, or systemic complications. MR imaging is also associated with the focus score index in minor salivary gland biopsy.
4. There are no signs of cardiovascular autonomic nervous system dysfunction in primary SS compared to the general population evaluated by comprehensive cardiovascular tests: conventional reflex tests, baroreflex sensitivity test with phenylephrine, and 24-hour HRV.

70
5. The results of cardiovascular autonomic tests are not associated with tear or saliva secretion, or other clinical features of the patients, including disease duration, sedimentation rate, systemic complications, or anti-Ro/SSA-antibodies.
6. Severe inflammatory CNS disease is a possible complication of primary SS, though its prevalence is a matter of controversy.

References
1. Sjögren H (1933) Zur Kenntnis der Keratoconjunctivitis sicca (Keratitis filiformis bei hypofunction der Tränendrüsen). Acta Ophtalmol Suppl 11:1-151.
2. Bloch KJ, Buchanan WW, Wohl MJ & Bunim JJ (1965) Sjögren's syndrome. A clinical, pathological, and serological study of sixty-two cases. Medicine 44: 187-231.
3. Talal N & Bunim JJ (1964) Development of malignant lymphoma in the course of Sjögren's syndrome. Am J Med 36: 529-540.
4. Kelly CA, Foster H, Pal B, Gardiner P, Malcolm AJ, Charles P, Blair GS, Howe J, Dick WC & Griffiths ID (1991) Primary Sjögren's syndrome in North East England - A longitudinal study. Br J Rheumatol 30: 437-442.
5. Kruize AA, Hené RJ, van der Heide A, Bodeutsch C, de Wilde PCM, van Bijsterveld OP, de Jong J, Feltkamp TEW, Kater L & Bijlsma JWJ (1996) Long-term followup of patients with Sjögren's syndrome. Arthritis Rheum 39: 297-303.
6. Davidson BKS, Kelly CA & Griffiths ID (1999) Primary Sjögren's syndrome in the North East of England: a long-term follow-up study. Rheumatology 38: 245-253.
7. Martens PB, Pillemer SR, Jacobsson LTH, O'Fallon WM & Matteson EL (1999) Survivorship in a population based cohort of patients with Sjögren's syndrome, 1976-1992. J Rheumatol 26: 1296-1300.
8. Jacobsson LTH, Axell TE, Hansen BU, Henricsson VJ, Larsson Å, Lieberkind K, Lilja B & Manthorpe R (1989) Dry eyes or mouth-an epidemiological study in Swedish adults, with special reference to primary Sjögren's syndrome. J Autoimmun 2: 521-527.
9. Dafni UG, Tzioufas AG, Staikos P, Skopouli FN & Moutsopoulos HM (1997) Prevalence of Sjögren's syndrome in a closed rural community. Ann Rheum Dis 56: 521-525.
10. Thomas E, Hay EM, Hajeer A & Silman AJ (1998) Sjögren's syndrome: A community-based study of prevalence and impact. Br J Rheumatol 37: 1069-1076.
11. Rubin P & Holt JF (1957) Secretory sialography in diseases of the major salivary glands. Am J Roentgenol 77: 575-598.
12. Daniels TE, Silverman S, Michalski JP, Greenspan JS, Path MRC, Sylvester RA & Talal N (1975) The oral component of Sjögren's syndrome. Oral Surg 39: 875-885.
13. Späth M, Kruger K, Dresel S, Grevers G, Vogl T & Schattenkirchner M (1991) Magnetic resonance imaging of the parotid gland in patients with Sjögren's syndrome. J Rheumatol 18:1372-1378.
14. Jonsson R, Kroneld U, Bäckman K, Magnusson B & Tarkowski A (1993) Progression of sialadenitis in Sjögren's syndrome. Br J Rheumatol 32: 578-581.
15. Garrett JR (1987) The proper role of nerves in salivary secretion: A review. J Dent Res 66: 387-397.

7216. Bacman S, Sterin-Borda L, Camusso J, Arana R, Hubscher O & Borda E (1996) Circulating
antibodies against rat parotid gland M3 muscarinic receptors in primary Sjögren’s syndrome.Clin Exp Immunol 104: 454-459.
17. Ewing DJ, Cambell IW & Clarke BF (1976) Mortality in diabetic autonomic neuropathy. Lancet 1(7960): 601-603.
18. Alexander EL (1993) Neurologic disease in Sjögren’s syndrome: Mononuclear inflammatory vasculopathy affecting central/peripheral nervous system and muscle. Rheum Dis Clin North Am 19: 869-908.
19. Moutsopoulos HM, Sarmas JH & Tala N (1993) Is central nervous system involvement a systemic manifestation of primary Sjögren’s syndrome? Rheum Dis Clin North Am 19: 909-912.
20. Tischler M, Yaron I, Shirazi I & Yaron M (1997) Saliva: an additional diagnostic tool in Sjögren's syndrome. Semin Arthritis Rheum 27: 173-179.
21. Turner RJ (1993) Mechanisms of fluid secretion by salivary glands. ANN NY Acad Sci 694: 24-35.
22. Tenovuo J & Lagerlöf F (1994) Saliva. In: Fejerskov O & Thylstrup A (eds) Textbook of clinical cariology. Munksgaard, Copenhagen, 17-43.
23. Petersen JK (1986) Xerostomia. Scand J Rheumatol Suppl 61: 185-189. 24. Daniels TE (1984) Labial salivary gland biopsy in Sjögren's syndrome. Arthritis Rheum 27:
147-156. 25. Soto-Rojas AE, Villa AR, Sifuentes-Osornio J, Alarcón-Segovia D & Kraus A (1998) Oral
manifestations in patients with Sjögren's syndrome. J Rheumatol 25: 906-910. 26. Yousem DM, Kraut MA & Chalian AA (2000) Major salivary gland imaging. Radiology
216: 19-29. 27. Gritzmann N, Rettenbacher T, Hollerweger A, Macheiner P & Hübner E (2003) Sonography
of the salivary glands. Eur Radiol 13: 964-975. 28. Mandel L & Witek EL (2001) Chronic parotitis. Diagnosis and treatment. J Am Dent Assoc
132: 1707-1711. 29. Marchal F, Kurt A-M, Dulguerov P, Becker M, Oedman M & Lehmann W (2001)
Histopathology of submandibular glands removed for sialolithiasis. Ann Otol Rhinol Laryngol 110: 464-469.
30. Morgan WS & Castleman B (1953) A clinocopathologic study of "Mikulicz's disease". Am J Path 29: 471-503.
31. Takashima S, Nagareda T, Noguchi Y, Takeuchi N, Tomiyama N, Johkoh T, Ikezoe J & Kozuka T (1992) CT and MR appearances of parotid pseudotumors in Sjögren's syndrome. J Comput Assist Tomogr 16: 376-383.
32. Talal N, Sylvester RA, Daniels TE, Greenspan JS & Williams RC (1974) T and B lymphocytes in peripheral blood and tissue lesions in Sjögren's syndrome. J Clin Invest 53: 180-189.
33. Tarpley TM, Anderson LG & White CL (1974) Minor salivary gland involvement in Sjögren's syndrome. Oral Surg Oral Med Oral Pathol 37: 64-74.
34. Greenspan JS, Path MRC, Daniels TE, Talal N & Sylvester RA (1974) The histopathology of Sjögren's syndrome in labial gland biopsies. Oral Surg 37: 217-219.
35. Konttinen YT (1981) In situ characterization of the cellular infiltrate in labial and palatine glands in Sjogren's syndrome. Scand J Rheumatol 10: 321-330.
36. Fox RI, Adamson III TC, Fong S, Robinson CA, Morgan EL, Robb JA & Howell FV (1983) Lymphocyte phenotype and function in pseudolymphoma associated with Sjögren's syndrome. J Clin Invest 72: 52-62.
37. Dalavanga YA, Drosos AA & Moutsopoulos HM (1986) Labial salivary gland immunopathology in Sjögren's syndrome. Scand J Rheumatol Suppl 61: 67-70.
38. Wise CM, Agudelo CA, Semble EL, Stump TE & Woodruff RD (1988) Comparison of parotid and minor salivary gland biopsy specimens in the diagnosis of Sjögren's syndrome. Arthritis Rheum 31: 662-666.

7339. Marx RE, Hartman KS & Rethman KV (1988) A prospective study comparing incisional
labial to incisional parotid biopsies in the detection and confirmation of sarcoidosis, Sjögren's syndrome, sialosis and lymphoma. J Rheumatol 15: 621-629.
40. Biasi D, Mocella S, Caramaschi P, Carletto A, Baracchino F, Colletti V & Bambara LM (1996) Utility and safety of parotid gland biopsy in Sjögren's syndrome. Acta Otolaryngol (Stockh) 116: 896-899.
41. Waterhouse JP (1963) Focal adenitis in salivary and lacrimal glands. Proc Roy Soc Med 56: 911-918.
42. Cifarelli PS, Bennett MJ & Zaino EC (1966) Sjogren's syndrome. A case report with an additional diagnostic aid. Arch Intern Med 117: 429-431.
43. Calman HI & Reifman S (1966) Sjögren's syndrome. Report of a case. Oral Surg 21: 158-162.
44. Chisholm DM & Mason DK (1968) Labial salivary gland biopsy in Sjögren's disease. J Clin Pathol 21: 656-660.
45. Morgan WS (1954) The probable systemic nature of Mikulicz's disease and its relation to Sjögren's syndrome. N Engl J Med 251: 1-5.
46. Moutsopoulos HM, Webber BL, Vlagopoulos TP, Chused TM & Decker JL (1979) Differences in the clinical manifestations of sicca syndrome in the presence and absence of rheumatoid arthritis. Am J Med 66: 733-736.
47. Fox RI, Robinson CA, Curd JG, Kozin F & Howell FV (1986) Sjögren's syndrome. Proposed criteria for classification. Arthritis Rheum 29: 577-585.
48. Manthorpe R, Oxholm P, Prause JU & Schiodt M (1986) The Copenhagen criteria for Sjögren's syndrome. Scand J Rheumatol Suppl 61: 19-21.
49. Skopouli FN, Drosos AA, Papaioannou T & Moutsopoulos HM (1986) Preliminary diagnostic criteria for Sjögren's syndrome. Scand J Rheumatol Suppl 61: 22-25.
50. Homma M, Tojo T, Akizuki M & Yamagata H (1986) Criteria for Sjögren's syndrome in Japan. Scand J Rheumatol Suppl 61: 26-27.
51. Vitali C, Bombardieri S, Moutsopoulos HM, Balestrieri G, Bencivelli W, Bernstein RM, Bjerrum KB, Braga S, Coll J, de Vita S, Drosos AA, Ehrenfeld M, Hatron PY, Hay EM, Isenberg DA, Janin A, Kalden JR, Kater L, Konttinen YT, Maddison PJ, Maini RN, Mathorpe R, Meyer O, Ostuni P, Pennec Y, Prause JU, Richards A, Sauvezie B, Schiodt M, Sciuto M, Scully C, Shoenfeld Y, Skopouli FN, Smolen JS, Snaith ML, Tishler M, Todesco S, Valesini G, Venables PJW, Wattiaux MJ & Youinou P (1993) Preliminary criteria for the classification of Sjögren's syndrome. Results of a prospective concerted action supported by the European Community. Arthritis Rheum 36: 340-347.
52. Vitali C, Bombardieri S, Moutsopoulos HM, Coll J, Gerli R, Hatron PY, Kater L, Konttinen YT, Mathorpe R, Meyer O, Mosca M, Ostuni P, Pellerito RA, Pennec Y, Porter SR, Richards A, Sauvezie B, Schiodt M, Sciuto M, Shoenfeld Y, Skopouli FN, Smolen JS, Soromenho F, Tishler M, Tomsic M, van de Merwe JP, Yeoman CM & Wattiaux MJ (The European study group on diagnostic criteria for Sjögren's syndrome) (1996) Assessment of the European classification criteria for Sjögren's syndrome in a series of clinically defined cases: results of a prospective multicentre study. Ann Rheum Dis 55: 116-121.
53. Vitali C, Bombardieri S, Jonsson R, Moutsopoulos HM, Alexander EL, Carsons SE, Daniels TE, Fox PC, Fox RI, Kassan SS, Pillemer SR, Talal N, Weisman MH & the European study group on classification criteria for Sjögren's syndrome (2002) Classification criteria for Sjögren's syndrome: a revised version of the European criteria proposed by the American-European Consensus group. Ann Rheum Dis 61: 554-558.
54. Daniels TE & Whitcher JP (1994) Association of patterns of labial salivary gland inflammation with keratoconjunctivitis sicca. Analysis of 618 patients with suspected Sjögren's syndrome. Arthritis Rheum 37: 869-877.
55. Syrjänen S (1984) Age-related changes in structure of labial minor salivary glands. Age Ageing 13: 159-165.
56. Segerberg-Konttinen M, Konttinen YT & Bergroth V (1986) Focus score in the diagnosis of Sjögren's syndrome. Scand J Rheumatol Suppl 61: 47-51.

7457. Radfar L, Kleiner DE, Fox PC & Pillemer SR (2002) Prevalence and clinical significance of
lymphocytic foci in minor salivary glands of healthy volunteers. Arthritis Rheum (Arthritis Care Res) 47: 520-524.
58. Lindahl G & Hedfors E (1986) Focal lymphocytic infiltrates of salivary glands are not confined to Sjögren's syndrome. Scand J Rheumatol Suppl 61: 52-55.
59. Manthorpe R, Benoni C, Jacobsson L, Kirtava Z, Larsson Å, Liedholm R, Nyhagen C, Tabery H & Theander E (2000) Lower frequency of focal lip sialadenitis (focus score) in smoking patients. Can tobacco diminish the salivary gland involvement as judged by histological examination and anti-SSA/Ro and anti-SSB/La antibodies in Sjögren's syndrome? Ann Rheum Dis 59: 54-60.
60. Vitali C, Moutsopoulos HM, Bombardieri S & the European community study group on diagnostic criteria for Sjögren's syndrome (1994) The European community study group on diagnostic criteria for Sjögren's syndrome. Sensitivity and specificity of tests for ocular and oral involvement in Sjögren's syndrome. Ann Rheum Dis 53: 637-647.
61. Drosos AA, Andonopoulos AP, Costopoulos JS, Papadimitriou CS & Moutsopoulos HM (1988) Prevalence of primary Sjögren's syndrome in an elderly population. Br J Rheumatol 27: 123-127.
62. Vivino FB, Gala I & Hermann GA (2002) Change in final diagnosis on second evaluation of labial minor salivary gland biopsies. J Rheumatol 29: 938-944.
63. Valesini G, Gualdi GF, Priori R, DiBiasi C, Polettini E, Trasimeni G, Filippi A, Pezzi P & Balsano F (1994) Magnetic resonance imaging of the parotid glands and lip biopsy in the evaluation of xerostomia in Sjögren's syndrome. Scand J Rheumatol 23:103-6.
64. Izumi M, Eguchi K, Nakamura H, Nagataki S & Nakamura T (1997) Premature fat deposition in the salivary glands associated with Sjögren's syndrome: MR and CT evidence. Am J Neuroradiol 18:951-958.
65. LeRoy JP, Pennec YL, Jouquan J, Lelong A & Youinou (1989) Relations of the histopathology of sublingual and labial salivary glands to the clinical presentation in primary Sjögren's syndrome. Clin Exp Rheum 7: 171-174.
66. Shah F, Rapini RP, Arnett FC, Warner NB & Smith CA (1990) Association of labial salivary gland histopathology with clinical and serologic features of connective tissue diseases. Arthritis Rheum 33: 1682-1686.
67. Wise CM & Woodruff RD (1993) Minor salivary gland biopsies in patients investigated for primary Sjögren's syndrome. A review of 187 patients. J Rheumatol 20: 1515-1518.
68. Gerli R, Muscat C, Giansanti M, Danieli MG, Sciuto M, Gabrielli A, Fiandra E & Vitali C (1997) Quantitative assessment of salivary gland inflammatory infiltration in primary Sjögren's syndrome: Its relationship to different demographic, clinical and serological features of the disorder. Br J Rheumatol 36: 969-975.
69. Lee M, Rutka JA, Slomovic AR, McComb J, Bailey DJ & Bookman AAM (1998) Establishing guidelines for the role of minor salivary gland biopsy in clinical practice for Sjögren's syndrome. J Rheumatol 25: 247-253.
70. Brennan MT, Sankar V, Leakan RA, Kleiner D, Atkinson JC, Wilkinson WE, Baum BJ & Pillemer SR (2002) Risk factors for positive minor salivary gland biopsy findings in Sjögren's syndrome and dry mouth patients. Arthritis Rheum (Arthritis Care Res) 47: 189-195.
71. Xu K-P, Katagiri S, Takeuchi T & Tsubota K (1996) Biopsy of labial salivary glands and lacrimal glands in the diagnosis of Sjögren's syndrome. J Rheumatol 23: 76-82.
72. Haga H-J (2002) Clinical and immunological factors associated with low lacrimal and salivary flow rate in patients with primary Sjögren's syndrome. J Rheumatol 29: 305-308.
73. Friedman JA, Miller EB & Huszar M (2002) A simple technique for minor salivary gland biopsy appropriate for use by rheumatologists in an outpatient setting. Clin Rheumatol 21: 349-350.
74. Goh YH & Sethi DS (1998) Submandibular gland excision: a five-year review. J Laryngol Otol 112: 269-273.
75. McGuirt WFJr, Whang C & Moreland W (2002) The role of parotid biopsy in the diagnosis of pediatric Sjögren syndrome. Arch Otolaryngol Head Neck Surg 128: 1279-1281.

7576. Pennec YL, LeRoy JP, Jouquan J, Lelong A, Katsikis P & Youinou P (1990) Comparison of
labial and sublingual salivary gland biopsies in the diagnosis of Sjögren's syndrome. Ann Rheum Dis 49: 37-39.
77. Chisholm DM, Waterhouse JP & Mason DK (1970) Lymphocytic sialadenitis in the major and minor glands: a correlation in postmortem subjects. J Clin Pathol 23: 690-694.
78. Segerberg-Konttinen M (1988) Focal adenitis in lacrimal and salivary glands. Scand J Rheumatol 17: 379-385.
79. Dijkstra PF (1980) Classification and differential diagnosis of sialographic characteristics in Sjögren's syndrome. Semin Arthritis Rheum 10: 10-17.
80. Markusse HM, van Putten WI, Breedveld FC & Oudkerk M (1993) Digital subtraction sialography of the parotid glands in primary Sjögren's syndrome. J Rheumatol 20: 279-283.
81. Vitali C, Tavoni A, Simi U, Marchetti G, Vigorito P, d'Ascanio A, Neri R, Cristofani R & Bombardieri S (1988) Parotid sialography and minor salivary gland biopsy in the diagnosis of Sjögren's syndrome. A comparative study of 84 patients. J Rheumatol 15: 262-267.
82. Kalk WWI, Vissink A, Spijkervet FKL, Bootsma H, Kalleberg CGM & Roodenburg JLN (2002) Parotid sialography for diagnosing Sjögren's syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 94: 131-137.
83. De Clerck LS, Corthouts R, Francx L, Brussaard C, De Schepper A, Vercruysse HA & Stevens WJ (1988) Ultrasonography and computed tomography of the salivary glands in the evaluation of Sjögren's syndrome. Comparison with Parotid sialography. J Rheumatol 15:1777-1781.
84. Som PM, Shugar JMA, Train JS & Biller HF (1981) Manifestations of parotid gland enlargement: radiographic, pathologic, and clinical correlations. Radiology 141: 415-419.
85. Vitali C, Monti P, Giuggioli C, Tavoni A, Neri R, Genovesi-Ebert F, Marchetti G, Gabriele M & Bombardieri S (1989) Parotid sialography and lip biopsy in the evaluation of oral component in Sjögren's syndrome. Clin Exp Rheumatol 7: 131-135.
86. Adolph H (1966) Komplikation nach sialographie der glandula parotis. Dtsch Stomat 16:175-180.
87. Ansell G (1968) A national survey of radiological complications: interim report. Clin Radiol 19: 175-191.
88. Cockrell DJ & Rout PGJ (1993) Case report. An adverse reaction following sialography. Dentomaxillofac Radiol 22: 41-42.
89. Schall HL, Anderson LG, Wolf RO, Herdt JR, Tarpley TM, Cummings NA, Zeiger LS & Talal N (1971) Xerostomia in Sjögren's syndrome. Evaluation of sequential salivary scintigraphy. JAMA 216: 2109-2116.
90. Markusse HM, Pillay M & Breedveld FC (1993) The diagnostic value of salivary gland scintigraphy in patients suspected of primary Sjögren's syndrome. Br J Rheumatol 32: 231-235.
91. Tensing EK, Nordstrom DC, Solovieva S, Schauman KO, Sippo-Tujunen I, Helve T, Natah S, Ma J, Li TF & Konttinen YT (2003) Salivary gland scintigraphy in Sjogren's syndrome and patients with sicca symptoms but without Sjogren's syndrome: the psychological profiles and predictors for salivary gland dysfunction. Ann Rheum Dis 62: 964-968.
92. Lindvall AM & Jonsson R (1986) The salivary gland component of Sjögren's syndrome: An evaluation of diagnostic methods. Oral Surg Oral Med Oral Pathol 62: 32-42.
93. Arrago JP, Rain JD, Brocheriou C & Rocher F (1987) Scintigraphy of the salivary glands in Sjögren's syndrome. J Clin Pathol 40: 1463-1467.
94. Håkansson U, Jacobsson L, Lilja B, Manthorpe R & Henriksson V (1994) Salivary gland scintigraphy in subjects with and without symptoms of dry mouth and/or eyes, and in patients with primary Sjögren's syndrome. Scand J Rheumatol 23: 326-333.
95. Saito T, Fukuda H, Horikawa M, Ohmori K, Shindoh M & Amemiya A (1997) Salivary gland scintigraphy with 99mTc-pertechnetate in Sjögren's syndrome: relationship to clinicopathologic features of salivary and lacrimal glands. J Oral Pathol Med 26: 46-50.
96. de Jager JP, Choy D & Fleming A (1984) Salivary scanning in rheumatoid arthritis with sicca syndrome. Ann Rheum Dis 43: 610-612.

7697. Daniels TE, Powell MR, Sylvester RA & Talal N (1979) An evaluation of salivary
scintigraphy in Sjögren's syndrome. Arthritis Rheum 22: 809-814. 98. March DE, Rao VM & Zwillenberg D (1989) Computed tomography of salivary glands in
Sjögren's syndrome. Arch Otolaryngol Head Neck Surg 115: 105-106. 99. Szolar DH, Groell R, Braun H, Preidler K, Stiskal M, Kern R, Kainz J, Moelleken S &
Stammberger H (1996) Ultrafast computed tomography and three-dimensional image processing of CT sialography in patients with parotid masses poorly defined by magnetic resonance imaging. Acta Otolaryngol (Stockh) 116: 112-118.
100. Bradus RJ, Hybarger P & Gooding GAW (1988) Parotid gland: US findings in Sjögren's syndrome. Radiology 169:749-751.
101. Takashima S, Morimoto S, Tomiyama N, Takeuchi N, Ikezoe J & Kozuka T (1992) Sjogren syndrome: Comparison of sialography and ultrasonography. J Clin Ultrasound 20: 99-109.
102. Makula E, Pokorny G, Rajtar M, Kiss I, Kovacs A & Kovacs L (1996) Parotid gland ultrasonography as a diagnostic tool in primary Sjögren's syndrome. Br J Rheumatol 35: 972-977.
103. Kawamura H, Taniguchi N, Itoh K & Kano S (1990) Salivary gland echography in patients with Sjögren's syndrome. Arthritis Rheum 33: 505-510.
104. De Vita S, Lorenzon G, Rossi G, Sabella M & Fossaluzza V (1992) Salivary gland echography in primary and secondary Sjögren's syndrome. Clin Exp Rheumatol 10: 351-356.
105. Yoshiura K, Yuasa K, Tabata O, Araki K, Yonetsu K, Nakayama E, Kanda S, Shinohara M & Higuchi Y (1997) Reliability of ultrasonography and sialography in the diagnosis of Sjögren's syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 83: 400-407.
106. Mandel L & Orchowski YS (1998) Using ultrasonography to diagnose Sjögren's syndrome. J Am Dent Assoc 129: 1129-1133.
107. Salaffi F, Argalia G, Carotti M, Giannini FB & Palombi C (2000) Salivary gland ultrasonography in the evaluation of primary Sjögren's syndrome. Comparison with minor salivary gland biopsy. J Rheumatol 27: 1229-1236.
108. Makula E, Pokorny G, Kiss M, Vörös E, Kovacs L, Kovacs A, Csernay L & Palkó A (2000) The place of magnetic resonance and ultrasonographic examinations of the parotid gland in the diagnosis and follow-up of primary Sjögren's syndrome. Rheumatology 39: 97-104.
109. Yonetsu K, Takagi Y, Sumi M & Nakamura T (2002) Sonography as a replacement for sialography for the diagnosis of salivary glands affected by Sjögren's syndrome (letter). Ann Rheum Dis 61: 276-286.
110. Corthouts B, De Clerck LS, Francx L, De Schepper A, Vercruysse HA & Stevens WJ (1991) Ultrasonography of the salivary glands in the evaluation of Sjögren's syndrome. Comparison with sialography. J Belge Radiol 74: 189-192.
111. Ariji Y, Ohki M, Eguchi K, Izumi M, Ariji E, Mizokami A, Nagataki S & Nakamura T (1996) Texture analysis of sonographic features of the parotid gland in Sjögren's syndrome. Am J Roentgenol 166: 935-941.
112. Ahuja AT & Metreweli C (1996) Ultrasound features of Sjögren's syndrome. Australas Radiol 40: 10-14.
113. Rinast E, Gmelin E & Hollands-Thorn B (1989) Digital subtraction sialography, conventional sialography, high-resolution ultrasonography and computed tomography in the diagnosis of salivary gland disease. Eur J Radiol 9: 224-230.
114. Takashima S, Takeuchi N, Morimoto S, Tomiyama N, Ikezoe J, Shogen K, Kozuka T & Okumura T (1991) MR imaging of Sjögren's syndrome: Correlation with sialography and pathology. J Comput Assist Tomogr 15: 393-400.
115. Vogl TJ, Dresel SHJ, Grevers G, Späth M, Bergman C, Balzer J & Lissner J (1996) Sjoegren's syndrome: MR imaging of the parotid gland. Eur Radiol 6: 46-51.
116. Sumi M, Izumi M, Yonetsu K & Nakamura T (1999) Sublingual gland: MR features of normal and disease states. Am J Roentgenol 172: 717-722.
117. Izumi M, Eguchi K, Uetani M, Nakamura H, Takagi Y, Hayashi Y & Nakamura T (1998) MR features of the lacrimal gland in Sjögren's syndrome. Am J Roentgenol 170: 1661-1666.

77118. Izumi M, Eguchi K, Ohki M, Uetani M, Hayashi K, Kita M, Nagataki S & Nakamura T
(1996) MR imaging of the parotid gland in Sjögren's syndrome: A proposal for new diagnostic criteria. Am J Roentgenol 166: 1483-1487.
119. Grevers G, Ihrler S, Vogl TJ & Weiss M (1994) A comparison of clinical, pathological and radiological findings with magnetic resonance imaging studies of lymphomas in patients with Sjögren's syndrome. Eur Arch Otorhinolaryngol 251: 214-217.
120. Sheikh JS, Sharma M, Kunath A, Fritz DA, Glueck CJ & Hess EV (1996) Reversible parotid enlargement and pseudo-Sjögren's syndrome secondary to hypertriglyceridemia. J Rheumatol 23: 1288-1291.
121. Izumi M, Hida A, Takagi Y, Kawabe Y, Eguchi K & Nakamura T (2000) MR imaging of the salivary glands in sicca syndrome: Comparison of lipid profiles and imaging in patients with hyperlipidemia and patients with Sjögren's syndrome. Am J Roentgenol 175:82-834.
122. Tonami H, Ogawa Y, Matoba M, Kuginuki Y, Yokota H, Higashi K, Okimura T, Yamamoto I & Sugai S (1998) MR sialography in patients with Sjögren's syndrome. Am J Neuroradiol 19: 1199-1203.
123. Ohbayashi N, Yamada I, Yoshino N & Sasaki T (1998) Sjögren's syndrome: Comparison of assessments with MR sialography and conventional sialography. Radiology 209: 683-688.
124. Tonami H, Higashi K, Matoba M, Yokota H, Yamamoto I & Sugai S (2001) A comparative study between MR sialography and salivary gland scintigrapy in the diagnosis of Sjögren's syndrome. J Comput Assist Tomogr 25: 262-268.
125. Lomas DJ, Carrol NR, Johnson G, Antoun NM & Freer CEL (1996) MR sialography. Radiology 200: 129-133.
126. Fischbach R, Kugel H, Ernst S, Schröder U, Brochhagen H-G, Jungehulsing M & Heindel W (1997) MR sialography: Initial experience using a T2-weighted fast SE sequence. J Comput Assist Tomogr 21: 826-830.
127. Sartoletti-Schefer S, Kollias S, Wichmann W & Valavanis A (1999) 3D T2-weighted fast spin-echo MRI sialography of the parotid gland. Neuroradiology 41: 46-51.
128. Becker M, Marchal F, Becker CD, Dulguerov P, Georgakopoulos G, Lehmann W & Terrier F (2000) Sialolithiasis and salivary ductal stenosis: Diagnostic accuracy of MR sialography with a three-dimensional extended-phase conjugate-symmetry rapid spin-echo sequence. Radiology 217: 347-358.
129. Mathias CJ (2000) Disorders of the autonomic nervous system. In: Bradley WG, Daroff RB, Fenichel GM & Marsden CD (eds) Neurology in Clinical Practice. Third Edition. Butterworth-Heinemann, Boston, 2131-2158.
130. Bennett PH & Scott JT (1965) Autonomic neuropathy in rheumatoid arthritis. Ann Rheum Dis 24: 161-168.
131. Binnie CD, Cooper R, Fowler CJ, Mauguière F & Prior PF (1996) Assessment of autonomic function. In: Osselton JW (ed) Clinical Neurophysiology. First Edition. Butteworth-Heineman, The University Press, Cambridge, 218-232.
132. Griffin JW, Cornblath DR, Alexander E, Campbell J, Low PA, Bird S & Feldman EI (1990) Ataxic sensory neuropathy and dorsal root ganglionitis associated with Sjögren’s syndrome. Ann Neurol 27: 304-315.
133. Levy DM, Rowley DA & Abraham RR (1992) Portable infrared pupillometry using Pupilscan: relation to somatic and autonomic nerve function in diabetes mellitus. Clin Auton Res 2: 335-341.
134. Miralles R, Espadaler JM, Navarro X & Rubies-Prat J (1995) Autonomic neuropathy in chronic alcoholism: evaluation of cardiovascular, pupillary and sympathetic skin responses. Eur Neurol 35: 287-292.
135. Trudgill NJ, Hussain FN, Smith LF & Riley SA (1999) Studies of autonomic function in patients with achalasia and nutcracker oesophagus. Eur J Gastroenterol Hepatol 11:1349-1354.
136. Ramos-Remus C, Suarez-Almazor M & Russell AS (1994) Low tear production in patients with diabetes mellitus is not due to Sjögren's sydnrome. Clin Exp Rheumatol 12: 375-380.
137. Watkins PJ & Mackay JD (1980) Cardiac denervation in diabetic neuropathy. Ann Intern Med 92: 304-407.

78138. Farrell TG, Odemuyiwa O, Bashir Y, Cripps TR, Malik M, Ward DE & Camm AJ (1992)
Prognostic value of baroreflex sensitivity testing after acute myocardial infarction. Br Heart J 67: 129-137.
139. Bigger JT, Fleiss JL, Steinman RC, Rolnitzky LM, Kleiger RE & Rottman JN (1992) Frequency domain measures of heart period variability and mortality after myocardial infarction. Circulation 85: 164-171.
140. Kleiger RE, Miller JP, Bigger JT Jr, Moss AJ & the Multicenter Post-Infarction Research Group (1987) Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am J Cardiol 59: 256-262.
141. Huikuri HV, Mäkikallio TH, Airaksinen KEJ, Seppänen T, Puukka P, Räihä IJ & Sourander LB (1998) Power-law relationship of heart rate variability as a predictor of mortality in the elderly. Circulation 97: 2031-2036.
142. Tsuji H, Larson MG, Venditti FJ, Manders ES, Evans JC, Feldman CL & Levy D (1996) Impact of reduced heart rate variability on risk for cardiac events. The Framingham heart study. Circulation 94: 2850-2855.
143. Ewing DJ & Clarke BF (1982) Diagnosis and management of diabetic autonomic neuropathy. Br Med J 285: 916-918.
144. Ewing DJ, Martyn CN, Young RJ & Clarke BF (1985) The value of cardiovascular autonomic function tests: 10 years experience in diabetes. Diabetes Care 8:491-498.
145. Ekberg DL (1980) Parasympathetic cardiovascular control in human disease: a critical review of methods and results. Am J Physiol 239: H581-H593.
146. Smith SE & Smith SA (1981) Heart rate variability in healthy subjects measured with a bedside computer-based technique. Clin Sci 61: 379-383.
147. Piha SJ (1991) Cardiovascular autonomic reflex tests: normal responses and age-related reference values. Clin Physiol 11: 277-290.
148. Ravitz JM (1997) AAEM minimonograph # 48: autonomic nervous system testing. Muscle Nerve 20: 919-937.
149. Consensus statement. Report and recommendations of the San Antonio conference on diabetic neuropathy (1988) Diabetes 37: 1000-1004.
150. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology (1996) Heart rate variability: standards of measurement, physiological interpretation and clinical use. Circulation 93: 1043-1065.
151. Kempler P, Tesfaye S, Chaturvedi N, Stevens LK, Webb DJ, Eaton S, Kerenyi Z, Tamas G, Ward JD, Fuller JH & EURODIAB IDDM complications study group (2002) Autonomic neuropathy is associated with increased cardiovascular risk factors: the EURODIAB IDDM complications study. Diabet Med 19: 900-909.
152. Sharpey-Schafer EP & Taylor PJ (1969) Absent circulatory reflexes in diabetic neuritis. Lancet 1(7124):559-562.
153. Smyth HS, Sleight P & Pickering GW (1969) Reflex regulation of arterial pressure during sleep in man: a quantitative method of assessing baroreflex sensitivity. Circ Res 24: 109-121.
154. Proceedings of a consensus development conference on standardized measures in diabetic neuropathy. Autonomic nervous system testing (1992) Muscle Nerve 15: 1158-1166.
155. Wheeler T & Watkins PJ (1973) Cardiac denervation in diabetes. Br Med J 4: 584-586. 156. Bennett T, Farquhar IK, Hosking DJ & Hampton J (1978) Assessment of methods for
estimating autonomic nervous control of the heart in patients with diabetes mellitus. Diabetes 27: 1167-1174.
157. Imholz BP, van Montfrans GA, Settels JJ, van der Hoeven GM, Karemaker JM & Wieling W (1988) Continuous non-invasive blood pressure monitoring: reliability of Finapres device during the Valsalva manoeuvre. Cardiovasc Res 22: 390-397.
158. Piha SJ (1993) Age-related diminution of the cardiovascular autonomic responses: diagnostic problems in the elderly. Clin Physiol 13: 507-517.
159. Jones DH, Hamilton CA & Reid JL (1978) Plasma noradrenaline, age and blood pressure: a population study. Clin Sci Mol Med 55 Suppl 4: 73s-75s.

79160. Airaksinen KEJ, Salmela PI, Ikäheimo MJ, Kirkinen P, Linnaluoto MK & Takkunen JT
(1987) Effect of pregnancy on autonomic nervous function and heart rate in diabetic and nondiabetic women. Diabetes Care 10: 748-751.
161. Bergström B, Lilja B, Rosberg K& Sundkvist G (1986) Autonomic nerve function tests. Reference values in healthy subjects. Clin Physiol 6: 523-528.
162. Levin AB (1966) A simple test of cardiac function based upon the heart rate changes induced by the Valsalva maneuver. Am J Cardiol 18: 90-99.
163. Page MMcB & Watkins PJ (1977) The heart in diabetes: autonomic neuropathy and cardiomyopathy. Clin Endocrinol Metab 6: 377-388.
164. Eckberg DL, Drabinsky M & Braunwald E (1971) Defective cardiac parasympathetic control in patients with heart disease. N Engl J Med 285: 877-883.
165. Hartikainen J, Fyhrquist F, Tahvanainen K, Länsimies E & Pyörälä K (1995) Baroreflex sensitivity and neurohormonal activation in patients with acute myocardial infarction. Br Heart J 74: 21-26.
166. La Rovene MT, Bigger JT Jr, Marcus FI, Mortara A & Schwartz PJ (1998) Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes after Myocardial Infarction) Investigators. Lancet 351: 478-484.
167. Pitzalis MV, Mastropasqua F, Passantino A, Massari F, Ligurgo L, Forleo C, Balducci C, Lombardi F & Rizzon P (1998) Comparison between noninvasive indices of baroreceptor sensitivity and the phenylephrine method in post-myocardial infarction patients. Circulation 97: 1362-1367.
168. Stein PK, Bosner MS, Kleiger RE & Conger BM (1994) Heart rate variability: A measure of cardiac autonomic tone. Am Heart J 127: 1376-1381.
169. Ewing DJ, Neilson JM & Travis P (1984) New method for assessing cardiac parasympathetic activity using 24 hour electrocardiograms. Br Heart J 52: 396-402.
170. Ziegler D, Dannehl K, Mühlen H, Spüler M & Gries FA (1992) Prevalence of cardiovascular autonomic dysfunction assessed by spectral analysis, vector analysis, and standard tests of heart rate variation and blood pressure responses at various stages of diabetic neuropathy. Diabetic Med 9: 806-814.
171. Huikuri HV, Kessler KM, Terracall E, Castellanos A, Linnaluoto MK & Myerburg RJ (1990) Reproducibility and circadian rhythm of heart rate variability in healthy subjects. Am J Cardiol 65: 391-393.
172. Lord SW, Clayton RH, Hall MCS, Gray JC, Murray A, McComb JM & Kenny RA (1998) Reproducibility of three different methods of measuring baroreflex sensitivity on normal subjects. Clin Sci 95: 575-581.
173. Šega S, Jager F & Kiauta T (1993) A comparison of cardiovascular reflex tests and spectral analysis of heart rate variability in healthy subjects. Clin Auton Res 3: 175-182.
174. Ducher M, Cerutti C, Gustin MP, Abou-Amara S, Thivolet C, Laville M, Paultre CZ & Fauvel JP (1999) Noninvasive exploration of cardiac autonomic neuropathy. Diabetes Care 22: 388-393.
175. Spallone V, Bernardi L, Maiello MR, Cicconetti E, Ricordi L, Fratino P & Menzinger G (1996) Twenty-four-hour pattern of blood pressure and spectral analysis of heart rate variability in diabetic patients with various degrees of autonomic neuropathy. Comparison to standard cardiovascular tests. Clin Sci Suppl 91: 105-107.
176. Hoffmann J, Grimm W, Menz V, Müller H-H & Maisch B (2000) Heart rate variability and baroreflex sensitivity in idiopathic dilated cardiomyopathy. Heart 83: 531-536.
177. Kleiger RE, Stein PK, Bosner MS & Rottman JN (1992) Time domain measurements of heart rate variability. Cardiol Clin 10: 487-498.
178. Akselrod S, Gordon D, Ubel FA, Shannon DC, Barger AC & Cohen RJ (1981) Power spectrum analysis of heart rate fluctuation: a quantitative probe of beat-to-beat cardiovascular control. Science 213:220-222.
179. Brouwer J, van Veldhuisen DJ, Man in't Veld AJ, Haaksma J, Dijk WA, Visser KR, Boomsma F, Dunselman PHJM & Lie KI for the Dutch Ibopamine multicenter trial study

80group (1996) Prognostic value of heart rate variability during long-term follow-up in patients with mild to moderate heart failure. J Am Coll Cardiol 28: 1183-1189.
180. Huikuri HV, Ylitalo A, Pikkujämsä SM, Ikäheimo MJ, Airaksinen KEJ, Rantala AO, Lilja M & Kesäniemi YA (1996) Heart rate variability in systemic hypertension. Am J Cardiol 77: 1073-1077.
181. Pikkujämsä SM, Huikuri HV, Airaksinen KEJ, Rantala AO, Kauma H, Lilja M, Savolainen MJ & Kesäniemi YA (1998) Heart rate variability and baroreflex sensitivity in hypertensive subjects with and without metabolic features of insulin resistance syndrome. Am J Hypertens 11: 523-531.
182. Niemelä MJ, Airaksinen KEJ & Huikuri HV (1994) Effect of beta-blockade on heart rate variability in patients with coronary artery disease. J Am Coll Cardiol 23: 1370-1377.
183. Huikuri HV, Pikkujämsä SM, Airaksinen KEJ, Ikäheimo MJ, Rantala AO, Kauma H, Lilja M & Kesäniemi YA (1996) Sex-related differences in autonomic modulation of heart rate in middle-aged subjects. Circulation 94: 122-125.
184. Umetani K, Singer DH, McCraty R & Atkinson M (1998) Twenty-four hour time domain heart rate variability and heart rate: relations to age and gender over nine decades. J Am Coll Cardiol 31: 593-601.
185. Huikuri HV, Mäkikallio T, Airaksinen KEJ, Mitrani R, Castellanos A & Myerburg RJ (1999) Measurement of heart rate variability: A clinical tool or a research toy? J Am Coll Cardiol 34: 1878-1883.
186. Kennett RP & Harding AE (1986) Peripheral neuropathy associated with the sicca syndrome. J Neurol Neurosurg Psychiatry 49: 90-92.
187. Gemignani F, Manganelli P, Pavesi G & Marbini A (1988) Polyneuropathy in Sjögren’s syndrome. A case of prevalently autonomic neuropathy with tonic pupil and hypohidrosis. Funct Neurol 3: 337-348.
188. Low PA, Mertz LE, Auger RG, Dillon AM, Fealey RD, Jaradeh SS, Younge BR, Litchy WJ & Dyck PJ (1988) The autonomic neuropathies of Sjögren’s syndrome [abstract]. Neurology 38 Suppl 1: 104.
189. Kumazawa K, Sobue G, Yamamoto K & Mitsuma T (1993) Segmental anhidrosis in the spinal dermatomes in Sjögren’s syndrome – associated neuropathy. Neurology 43: 1820-1823.
190. Denislic M, Meh D, Popovic M & Kos-Golja M (1995) Small nerve fibre dysfunction in a patient with Sjögren’s syndrome. Scand J Rheumatol 24: 257-259.
191. Sorajja P, Poirier MK, Bundrick JB & Matteson EL (1999) Autonomic failure and proximal skeletal myopathy in a patient with primary Sjögren’s syndrome. Mayo Clin Proc 74: 695-697.
192. Mellgren SI, Conn DL, Stevens JC & Dyck PJ (1989) Peripheral neuropathy in primary Sjögren’s syndrome. Neurology 39: 390-394.
193. Tajima Y, Mito Y, Owada Y, Tsukishima E, Moriwaka F & Tashiro K (1997) Neurological manifestations of primary Sjögren’s syndrome in Japanese patients. Intern Med 36: 690-693.
194. Grant IA, Hunder GG, Homburger HA & Dyck PJ (1997) Peripheral neuropathy associated with sicca complex. Neurology 48: 855-862.
195. Andonopoulos AP & Ballas C (1995) Autonomic cardiovascular neuropathy in primary Sjögren’s syndrome. Rheumatol Int 15: 127-129.
196. Barendregt PJ, van den Bent MJ, van Raaij-van den Aarssen VJM, van den Meiracker AH, Vecht CJ, van der Heijde GL & Markusse HM (2001) Involvement of the peripheral nervous system in primary Sjögren's syndrome. Ann Rheum Dis 60: 876-881.
197. Wright RA, Grant IA & Low PA (1999) Autonomic neuropathy associated with sicca complex. J Auton Nerv Syst 75: 70-6.
198. Katz JS, Houroupian D & Ross MA (1999) Multisystem neuronal involvement and sicca complex: broadening the spectrum of complications. Muscle Nerve 22: 404-407.
199. Dupond J-L, Gil H & de Wazieres B (1999) Five-year efficacy of intravenous gammaglobulin to treat dysautonomia in Sjögren's syndrome (letter). Am J Med 106: 125.
200. Duchen LW, Anjorin A, Watkins PJ & Mackay JD (1980) Pathology of autonomic neuropathy in diabetes mellitus. Ann Intern Med 92: 301-303.

81201. Mandl T, Jacobsson L, Lilja B, Sundkvist G & Manthorpe R (1997) Disturbances of
autonomic nervous function in primary Sjögren’s syndrome. Scand J Rheumatol 26: 401-406.
202. Andonopoulos AP, Christodoulou J, Ballas C, Bounas A & Alexopoulos D (1998) Autonomic cardiovascular neuropathy in Sjögren’s syndrome. A controlled study. J Rheumatol 25: 2385-2388.
203. Barendregt PJ, van den Meiracker AH, Markusse HM, Tulen JHM, Boomsma F, van der Heijde GL & Man in't Veld AJ (1999) Parasympathetic failure does not contribute to ocular dryness in primary Sjögren's syndrome. Ann Rheum Dis 58: 746-750.
204. Mandl T, Bornmyr SV, Castenfors J, Jacobsson LTH, Manthorpe R & Wollmer P (2001) Sympathetic dysfunction in patients with primary Sjögren's syndrome. J Rheumatol 28: 296-301.
205. Kovács L, Török T, Bari F, Kéri Z, Kovács A, Makula É & Pokorny G (2000) Impaired microvascular response to cholinergic stimuli in primary Sjögren's syndrome. Ann Rheum Dis 59: 48-53.
206. Tumiati B, Perazzoli F, Negro A, Pantaleoni M & Regolisti G (2000) Heart rate variability in patients with Sjögren's syndrome. Clin Rheumatol 19: 477-480.
207. Barendregt PJ, Tulen JHM, van den Meiracker AH & Markusse HM (2002) Spectral analysis of heart rate and blood pressure variability in primary Sjögren's syndrome. Ann Rheum Dis 61: 232-236.
208. Lafitte C, Amoura Z, Cacoub P, Pradat-Diehl P, Picq C, Salachas F, Léger JM, Piette JC & Delattre JY (2001) Neurological complications of primary Sjögren's syndrome. J Neurol 248: 577-548.
209. Drosos AA, Andonopoulos AP, Lagos G, Angelopoulos NV & Moutsopoulos HM (1989) Neuropsychiatric abnormalities in primary Sjögren’s syndrome. Clin Exp Rheumatol 7: 207-209.
210. Stoltze CA, Hanlon DG, Pease GL & Henderson JW (1960) Keratoconjunctivitis sicca and Sjögren’s syndrome. Arch Intern Med 106: 513-522.
211. Kaltreider HB & Talal N (1969) The neuropathy of Sjögren’s syndrome. Ann Intern Med 70: 751-762.
212. Malinow KL, Molina R, Gordon B, Selnes OA, Provost TT & Alexander EL (1985) Neuropsychiatric dysfunction in primary Sjögren’s syndrome. Ann Intern Med 103: 344-349.
213. Molina R, Provost TT & Alexander EL (1985) Peripheral inflammatory vascular disease in Sjögren’s syndrome. Arthritis Rheum 28: 1341-1347.
214. Binder A, Snaith ML & Isenberg D (1988) Sjögren’s syndrome: A study of its neurological complications. Br J Rheumatol 27: 275-280.
215. Andonopuolos AP, Lagos G, Drosos AA & Moutsopoulos HM (1990) The spectrum of neurological involvement in Sjögren’s syndrome. Br J Rheumatol 29: 21-23.
216. Hietaharju A, Yli-Kerttula U, Häkkinen V & Frey H (1990) Nervous system manifestations in Sjögren’s syndrome. Acta Neurol Scand 81: 144-152.
217. Markusse HM, Oudkerk M, Vroom ThM, Breedveld FC (1992) Primary Sjögren's syndrome: clinical spectrum and mode of presentation based on an analysis of 50 patients selected from a department of rheumatology. Neth J Med 40:125-134.
218. Manthorpe R, Manthorpe T & Sjöberg S (1992) Magnetic resonance imaging of the brain in patients with primary Sjögren’s syndrome. Scand J Rheumatol 21: 148-149.
219. Moll JWB, Markusse HM, Pijnenburg JJJM, Vecht ChJ & Henzen-Logmans SC (1993) Antineuronal antibodies in patients with neurologic complications of primary Sjögren's syndrome. Neurology 43: 2574-2581.
220. Spezialetti R, Bluestein HG, Peter JB & Alexander EL (1993) Neuropsychiatric disease in Sjögren’s syndrome: Anti-ribosomal P and anti-neuronal antibodies. Am J Med 95: 153-160.
221. Mauch E, Volk C, Kratzsch G, Krapf H, Kornhuber HH, Laufen H & Hummel KJ (1994) Neurological and neuropsychiatric dysfunction in primary Sjögren’s syndrome. Acta Neurol Scand 89: 31-35.

82222. Escudero D, Latorre P, Codina M, Coll-Canti J & Coll J (1995) Central nervous system
disease in Sjögren’s syndrome. Ann Med Interne 146: 239-242. 223. Govoni M, Bajocchi G, Rizzo N, Tola MR, Caniatti L, Tugnoli V, Colamussi P & Trotta F
(1999) Neurological involvement in primary Sjögren's syndrome: Clinical and instrumental evaluation in a cohort of Italian patients. Clin Rheumatol 18: 299-303.
224. Coates T, Slavotinek JP, Rischmueller M, Schultz D, Anderson G, Dellamelva M, Sage MR & Gordon TP (1999) Cerebral white matter lesions in primary Sjögren's syndrome: A controlled study. J Rheumatol 26: 1301-1305.
225. Alexander EL, Arnett FC, Provost TT & Stevens MB (1983) Sjögren’s syndrome: Association of anti-Ro(SS-A) antibodies with vasculitis, hematologic abnormalities, and serologic hyperreactivity. Ann Intern Med 98: 155-159.
226. Alexander EL, Malinow K, Lejewski JE, Jerdan MS, Provost TT & Alexander GE (1986) Primary Sjögren’s syndrome with central nervous system disease mimicking multiple sclerosis. Ann Intern Med 104: 323-330.
227. Konttinen YT, Kinnunen E, von Bonsdorff M, Lillqvist P, Immonen I, Bergroth V, Segerberg-Konttinen M & Friman C (1987) Acute transverse myelopathy succesfully treated with plasmapheresis and prednisolone in a patient with primary Sjögren’s syndrome. Arthritis Rheum 30: 339-344.
228. Alexander GE, Provost TT, Stevens MB & Alexander EL (1981) Sjögren’s syndrome: Central nervous system manifestations. Neurology 31: 1391-1396.
229. Caselli RJ, Scheithauer BW, Bowles CA, Trenerry MR, Meyer FB, Smigielski JS & Rodriguez M (1991) The treatable dementia of Sjögren’s syndrome. Ann Neurol 30: 98-101.
230. Valtýsdóttir ST, Gudbjörnsson B, Lindqvist U, Hällgren R & Hetta J (2000) Anxiety and depression in patients with primary Sjögren's syndrome. J Rheumatol 27: 165-169.
231. Pal B, Gibson C, Passmore J, Griffiths ID & Dick WC (1989) A study of headaches and migraine in Sjögren's syndrome and other rheumatic disorders. Ann Rheum Dis 48: 312-316.
232. Alexander EL, Beall SS, Gordon B, Selnes OA, Yannakakis GD, Patronas N, Provost TT & McFarland HF (1988) Magnetic resonance imaging of cerebral lesions in patients with the Sjögren's syndrome. Ann Intern Med 108: 815-823.
233. Ranzenbach M, Kumar A, Rosenbaum A, Patronas N, Harley J, Reichlin M & Alexander EL (1992) Anti-Ro(SS-A) autoantibodies (A-RoAb) in the immunopathogenesis of serious focal CNS disease in Sjögren’s syndrome (CNS-SS) (abstract). Arthritis Rheum 35: Suppl: 114.
234. Gottfried JA, Finkel TH, Hunter JV, Carpentieri DF & Finkel RS (2001) Central nervous system Sjögren's syndrome in a child: case report and review of the literature. J Child Neurol 16: 683-685.
235. Greenan TJ, Grossman RI & Goldberg HI (1992) Cerebral vasculitis: MR imaging and angiographic correlation. Radiology 182: 65-72.
236. Calabrese LH, Duna GF & Lie JT (1997) Vasculitis in the central nervous system. Arthritis Rheum 40: 1189-1201.
237. Kozachuk WE, DeCarli C, Schapiro MB, Wagner EE, Rapoport SI & Horwitz B (1990) White matter hyperintensities in dementia of the Alzheimer’s type and in healthy subjects without cerebrovascular risk factors. A magnetic resonance imaging study. Arch Neurol 47: 1306-1310.
238. Pierot L, Sauve C, Leger J-M, Martin N, Koeger AC, Wechsler B & Chiras J (1993) Asymptomatic cerebral involvement in Sjögren's syndrome: MRI findings of 15 cases. Neuroradiology 35: 378-380.
239. Wright RA, O'Duffy JD & Rodriquez M (1999) Involvement of myelopathy in Sjögren's syndrome with chlorambucil and prednisolone therapy. Neurology 52: 386-388.
240. Mori K, Koike H, Misu K, Hattori N, Ichimura M & Sobue G (2001) Spinal cord magnetic resonance imaging demonstrates sensory neuronal involvement and clinical severity in neuropathy associated with Sjögren's syndrome. J Neurol Neurosurg Psychiatry 71: 488-492.

83241. Williams CCS, Butler E & Román GC (2001) Treatment of myelopathy in Sjögren's
syndrome with a combination of prednisolone and cyclophosphamide. Arch Neurol 58: 815-819.
242. Gerraty RP, McKelvie PA & Byrne E (1993) Aseptic meningoencephalitis in primary Sjögren's syndrome. Response to plasmapheresis and absence of CNS vasculitis at autopsy. Acta Neurol Scand 88: 309-311.
243. Ferreiro JE, Robalino BD & Saldana MJ (1987) Primary Sjögren's syndrome with diffuse cerebral vasculitis and lymphocytic interstitial pneumonitis. Am J Med 82: 1227-1232.
244. Kao C-H, Lan J-L, ChangLai S-P & Chieng P-U (1998) Technetium-99m-HMPAO brain SPECT in Sjögren's syndrome. J Nucl Med 39: 773-777.
245. Belin C, Moroni C, Caillat-Vigneron N, Debray M, Baudin M, Dumas J-L, Moretti J-L, Delaporte P & Guillevin L (1999) Central nervous system involvement in Sjögren's syndrome: evidence from neuropsychological testing and HMPAO-SPECT. Ann Intern Med 150: 598-604.
246. Govoni M, Padovan M, Rizzo N & Trotta F (2001) CNS involvement in primary Sjögren's syndrome. Prevalence, clinical aspects, diagnostic assessment and therapeutic approach. CNS Drugs 15: 597-607.
247. Tsai K-Y, Tsai C-P & Liao N (2001) Sjögren's syndrome with central nervous system involvement presenting as multiple sclerosis with failure response to beta-interferon. Eur Neurol 45: 59-60.
248. Canháo H, Fonseca JE & Rosa Á (2000) Intravenous gammaglobulin in the treatment of central nervous system vasculitis associated with Sjögren's syndrome (letter). J Rheumatol 27: 1102-1103.
249. Pertovaara M, Korpela M, Kouri T & Pasternack A (1999) The occurrence of renal involvement in primary Sjögren’s syndrome: a study of 78 patients. Rheumatology 38: 1113-1120.
250. Fox RI, Konttinen YT & Fischer A (2001) Short analytical review. Use of muscarinic agonists in the treatment of Sjögren's syndrome. Clin Immunol 101: 249-263.
251. Fox RI (2001) The value of non-invasive studies of parotid glands in primary Sjögren's syndrome (editorial). Arthritis Rheum (Arthritis Care Res) 45:473-474.
252. Hakala M, Niemelä RK (2000) Does autonomic nervous impairment have a role in pathophysiology of Sjögren's syndrome (commentary). Lancet 355: 1032-1033.
253. Ioannidis JP, Moutsopoulos HM (1999) Sjögren' syndrome: Too many associations, too limited evidence. The enigmatic example of CNS involvement (editorial). Semin Arthritis Rheum 29:1-3.