Embed Size (px)
Citation preview

IMAGING OF AN
ASCENDING AORTIC ANEURYSM
Adamantios Tsangaris,
National and Kapodistrian University of Athens
Diana Litmanovich, MD
MAY 2012

1 Adamantios Tsangaris
Diana Litmanovich, MD
Outline
•Definition and epidemiology of ascending aortic aneurysm
•Anatomy of the thoracic aorta and classification
•Etiology and pathogenesis of ascending aortic aneurysm
•Clinical presentation and complications of ascending aortic aneurysm
•Different modalities for the diagnosis and evaluation of ascending aortic aneurysm
•Companion Patient #1 : CXRs
•DDx of prominent aorta or aortic arch
•Index Patient : History and findings
•Companion Patient #2 : on transthoracic echocardiography
•Transthoracic echocardiography and transesophageal echocardiography imaging of
ascending aortic aneurysm
•Index Patient : MRA Imaging
•Index Patient : CTA Imaging
•Comparison between different modalities
•Treatment
•References
•Acknowledgements

2
Definition and epidemiology of ascending
aortic aneurysm
Localized dilatation of the aorta
50% over the normal diameter
Includes all three layers of the vessel (intima, media, adventitia)
Ascending aortic aneurysms arise anywhere from the aortic
valve to the innominate artery
Incidence 3.6-6 cases per 100.000 pt. years
Males - 2x-4x more commonly than females
Adamantios Tsangaris
Diana Litmanovich, MD Woo Y Joseph., Mohler R. Emile, (Jan 29,2009).Clinical features and diagnosis of thoracic aortic aneurysm. Uptodate.
Retrieved May 11, 2012, from http://www.uptodate.com/contents/clinical-features-and-diagnosis-of-thoracic-aortic

3
Anatomy of the thoracic aorta and
classification
Massachusetts General Hospital Thoracic Aortic Center
60%
10%
10%
40%
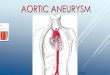
Aneurysm of the thoracic
aorta can be classified
into four anatomical
categories
• Ascending aortic
• Aortic arch
• Descending aortic
• Thoracoabdominal
Drawing of the thoracic aorta
anatomy. The arrows show the
percentage of the thoracic
aneurysm that involves each
anatomical segment.
Aneurysms can be:
Fusiform or
Saccular
Adamantios Tsangaris
Diana Litmanovich, MD

4
Pathophysiology:
Cystic medial degeneration
Risk factors are:
•Aging
•Hypertension
•Atherosclerosis (infrequent cause).
•Smoking
•Bicuspid valve
•Inflammatory/infectious disorders (eg. giant cell arthritis, syphilitic
aortitis)
•When occurs in young patients, think:
Marfan syndrome
Ehlers- Danlos syndrome
Other familiar (eg. mutation in TGF beta receptor 2 gene)
Takayasu arthritis : Young females/males
Etiology and Pathogenesis of ascending aortic
aneurysm
Isselbacher Eric M. Thoracic and Abdominal Aortic Aneurysms. Circulation 2005, 111:816-828. Adamantios Tsangaris
Diana Litmanovich, MD

5
Clinical presentation and complications of
ascending aortic aneurysm.
Most often asymptomatic
Heart failure due to aortic regurgitation
Myocardial ischemia or MI
Rare presentations due to mass effect:
•Hoarseness, hemidiaphragmatic paralysis
•Wheezing, cough , hemoptysis, dyspnea pneumonitis
•Dysphagia
•SVC syndrome
•Chest or back pain due to bone compression
•Thromboembolic episodes
Complications:
Dissection, leakage, rupture, acute aortic regurgitation Woo Y Joseph., Mohler R. Emile, (Jan 29,2009).Clinical features and diagnosis of thoracic aortic aneurysm. Uptodate.
Retrieved May 11, 2012, from http://www.uptodate.com/contents/clinical-features-and-diagnosis-of-thoracic-aortic
Adamantios Tsangaris
Diana Litmanovich, MD

6
Different modalities for the diagnosis and
evaluation of the ascending aortic aneurysm
• Chest X-ray
• Echocardiography
• CTA
• MRA
• Conventional angiography – seldom used our
days
Adamantios Tsangaris
Diana Litmanovich, MD

7
Companion patient #1 : CXR (PA view)
Possible findings on a CXR
suggesting an ascending
aortic aneurysm can be:
1. Widening of the
mediastinum as a result of
the prominence of the
ascending aorta.
2. Mass effect (e.g.
deviation of the trachea)
can be an indicator of an
ascending aortic aneurysm.
There is no such finding in
this companion patients
CXR.
PACS, BIDMC
Adamantios Tsangaris
Diana Litmanovich, MD

8
Companion patient #1: CXR (Lateral view)
PACS, BIDMC
This is the companion patient
(#1) lateral chest X-ray. Our
findings are:
Normal aortic arch
Normal distal ascending
aorta
Dilated proximal ascending
aorta
Adamantios Tsangaris
Diana Litmanovich, MD

9
DDx of prominent ascending aorta or aortic
arch Congenital
• Aortic arch anomaly (e.g., double aortic arch, right aortic arch
• PDA
• Tetralogy Fallot
• Coarctation of aorta; pseudocoarctation
Acquired
• Aneurysm of aorta
• Aortic regurgitation
• Aortic valve stenosis
• Aortitis (eg, syphilitic, giant cell, rheumatoid, Takayasu’s)
• Atherosclerosis (tortuosity, elongation, unfolding, and/or
dilatation of aorta)
• Hypertensive heart disease
• Medial degeneration of aorta (eg, Marfan S., Ehlers-Danlos S.)
• Mediastinal mass simulating large aorta (eg, lymphoma)
Reeder M. M., Bradley G. W., Jr. (1993). Reeder and Felson’s Gamuts in Radiology. (3rd edition). New York: Springer-Verlag
Adamantios Tsangaris
Diana Litmanovich, MD

10
Index Patient: History and findings
PMH: No
Findings: Hypertensive (SP 150 mmHg)
Transthoracic Echocardiography was performed to evaluate for
hypertrophic left ventricle.
Findings: bicuspid valve and ascending aortic aneurysm.
25 year old male presenting to the student clinic for a check up.
Adamantios Tsangaris
Diana Litmanovich, MD

11
This is a parasternal long-axis view in a
companion patient (#2) showing a dilated
aortic root and ascending aorta (white
arrows).
Ilenia Foffa, Pier Luigi Festa, Lamia Ait-Ali3, Annamaria Mazzone, Stefano
Bevilacqua and Maria Grazia Andreassi
http://www.cardiovascularultrasound.com/content/7/1/34
Companion patient #2 : on
transthoracic echocardiography
Adamantios Tsangaris
Diana Litmanovich, MD

2003 ACC/AHA guidelines : Echocardiography for the diagnosis
2006 ACC/AHA guidelines : CT or MRI for quantification of dilatation
TTE Preferred procedure. Effective for imaging the aortic root
(eg. In patients with Marfan syndrome), generally not be used for sizing
thoracic aortic aneurysms.
TEE Can visualize the entire thoracic aorta well, semi-invasive
not favored for routine imaging .
Aortic root or ascending aortic diameter > 4 cm and bicuspid aortic
valve further evaluation (size morphology of root and ascending
aorta) by echo, CT or MR yearly. So our index patient needs further CT
or MR evaluation.
Transthoracic Echocardiography (TTE) and
Transesophageal Echocardiography (TEE) imaging of
ascending aortic aneurysm
12 Woo Y Joseph., Mohler R. Emile, (Jan 29,2009).Clinical features and diagnosis of thoracic aortic aneurysm. Uptodate.
Adamantios Tsangaris
Diana Litmanovich, MD

13
Index Patient: MRA imaging (levels of sinus
of Valsalva and main pulmonary artery Multiplanar T1 and T2 weighted MR images were acquired in
order to evaluate the aortic root and ascending aorta dilatation. Axial view , C+, thoracic MRA
Level of the sinuses of Valsalva
Axial view, C+, thoracic MRA
Level of the main pulmonary artery
PACS, BIDMC PACS, BIDMC Aortic diameters Adamantios Tsangaris
Diana Litmanovich, MD

14
Index Patient: MRA imaging (levels of right
pulmonary artery and aortic arch)
Axial view , C+, thoracic MRA
Level of the aortic arch
PACS, BIDMC PACS, BIDMC Aortic diameters
Axial view , C+, thoracic MRA
Level of the right pulmonary artery
Adamantios Tsangaris
Diana Litmanovich, MD

15
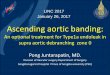
Index Patient: MRA imaging (Sagittal view)
3D MR reformation of the aorta
demonstrating a dilated ascending
aorta.
Measurement of the ascending
aorta was taken at the level of the
left pulmonary artery (42,9 mm).
Another measurement was taken
at the level of the aortic arch
(23,8 mm).
Findings: The aortic root and ascending thoracic aorta are dilated.
PACS, BIDMC
Sagittal view , C+,thoracic MRA
Adamantios Tsangaris
Diana Litmanovich, MD

16
3D reformation, C+, Thoracic CTA
CTA images were then acquired to evaluate the aortic valve for
calcification and the ascending aneurysm dimensions.
Aortic valve has a bicuspid morphology with a tiny calcific speck.
Index Patient: CTA imaging
Axial view, C+, Thoracic CTA
PACS, BIDMC PACS, BIDMC Adamantios Tsangaris
Diana Litmanovich, MD

17
Index Patient : CTA imaging
3D Reformations, Axial, Oblique
views, C+, CTA
Aortic valve level
PACS, BIDMC Adamantios Tsangaris
Diana Litmanovich, MD
At the aortic valve level, a
maximum diameter of 27,7
mm is measured in the
oblique view (bottom right
corner).

18
Index Patient : CTA imaging imaging
PACS, BIDMC
3D Reformations, Axial, Oblique
views, C+, CTA
Sinus of Valsalva level
Adamantios Tsangaris
Diana Litmanovich, MD
At the Sinus of Valsalva
level, a maximum diameter
of 52,3 mm is measured in
the oblique view (bottom
right corner).

19
Index Patient :CTA imaging
Maximum aortic
diameter (Valsalva l.)
Bicuspid Valve
Left Ventricle
Outflow Track
Left Atrium
Descending aorta
PACS, BIDMC
Axial view, C+, CTA
Sinus of Valsalva level
Adamantios Tsangaris
Diana Litmanovich, MD
At the Sinus of Valsalva
level, a maximum diameter
of 48.33 mm is measured in
the axial view.

20
Index Patient : CTA imaging
PACS, BIDMC
3D Reformations, Axial, Oblique
views, C+, CTA
Aortic root level
Adamantios Tsangaris
Diana Litmanovich, MD
At the aortic root level, a
maximum diameter of 40,6
mm is measured in the
oblique view (bottom right
corner).

21
Index Patient : CTA imaging
PACS, BIDMC
3D Reformations, Axial, Oblique
views, C+, CTA
Ascending aorta; level of right
pulmonary artery
Adamantios Tsangaris
Diana Litmanovich, MD
At the right pulmonary
artery level, a maximum
diameter of 39,4 mm is
measured in the oblique view
(bottom right corner).

22
Bicuspid aortic valve with fusiform dilatation of the ascending aorta with
a maximum changes appreciated in the sinus of Valsalva.
MRA and CTA findings
Maximum Diameter measurements in CTA and MRA (in mm). The upper normal limit of Intra-luminal AAOD, is 35.6 for males in age group 20 to 40.*
Level of Aorta CTA MRA
Sinus of Valsalva 52.3 51
Aortic root 40,6 42
(Asc.) Right pulmonary
artery
39.4 43
Aortic arch - 24
(Des.) Right main
pulmonary artery
23 -
*Song Shou Mao, MD, Nasir Ahmadi, MPH, Birju Shah, M.B.B.S, Daniel Beckmann, BS, Annie Chen, BS, Luan
Ngo, BS, Ferdinand R Flores, BS, Yan lin Gao, MD, and Matthew J Budoff, M.D.
Adamantios Tsangaris
Diana Litmanovich, MD

23
Comparison between different modalities
TTE TEE CXR CTA MRA
1st choice - - Suitable for
emergency
Time consuming
(x2 CTA)
No contrast,
no radiation
exp.
No contrast,
no radiation
exp.
No contrast,
exposure to
radiation
Contrast, exposure to
radiation
(renal failure?)
Contrast, no
radiation exp.
Non invasive Semi-
invasive, low
risk
Non invasive Non invasive Non invasive
Low cost Low cost Low cost Expensive Most expensive
Only images
aortic root and
ascending
aorta
Provides
additional
info TTE
Not diagnostic
(64% sensitivity
of wid . Med.
Sign. thoracic
dis.)
Good in diagnosing
and detecting
dimensions (92%
accuracy for all
th.abs.)
Good in diagnosing
and detecting
dimensions
- - - Images thrombus and
calcification better
Images aortic root
better
Adamantios Tsangaris
Diana Litmanovich, MD

24
Treatment
Lavall Daniel, Schäfers Hans-Joachim, Böhm Michael, Laufs Ulrich
http://www.aerzteblatt.de/int/archive/article?id=124325
Surgical: Index patient has a dilation of 51mm, one risk
factor and a bicuspid valve, thus recommended for surgery
Medical Beta blocker
Laplace law (T=p*r/2*t) T: Aortic wall tension
P: Intraluminal (blood) pressure
r: radius of aorta
t: aortic wall thickness
A decrease in blood
pressure (b-blocker)
decreases the aortic wall
tension thus decreasing
the aneurysms rate of
growth (the vessel does
not compensate by
increasing its radius) and
thus the possibility of
dissection.
Adamantios Tsangaris
Diana Litmanovich, MD

25
References
• Reeder M. M., Bradley G. W., Jr. (1993). Reeder and Felson’s Gamuts in Radiology. (3rd edition). New
York: Springer-Verlag.
• Isselbacher Eric M. Thoracic and Abdominal Aortic Aneurysms. Circulation 2005, 111:816-828.
• Guo D, Hasham S, Kuang S-Q, Vaughan CJ, Boerwinkle E, Chen H, Abuelo D, Dietz HC,
Basson CT, Shete SS, Milewicz DM. Familial thoracic aortic aneurysms and dissections.
Circulation. 2001;103: 2461–2468.
• Woo Y Joseph., Mohler R. Emile, (Jan 29,2009).Clinical features and diagnosis of thoracic aortic
aneurysm. Uptodate. Retrieved May 11, 2012, from http://www.uptodate.com/contents/clinical-
features-and-diagnosis-of-thoracic-aortic
aneurysm?source=search_result&search=aortic+aneurysm&selectedTitle=2%7E150
• Miller, WT. Thoracic Aortic Aneurysms: Plain Film Findings. Seminars in Roentgenology 2001 Oct;
36(4): 288-294.
• Song Shou Mao, MD, Nasir Ahmadi, MPH, Birju Shah, M.B.B.S, Daniel Beckmann, BS, Annie
Chen, BS, Luan Ngo, BS, Ferdinand R Flores, BS, Yan lin Gao, MD, and Matthew J Budoff, M.D.
Normal Thoracic Aorta Diameter on Cardiac Computed Tomography in Healthy Asymptomatic
Adult; Impact of Age and Gender. Acad Radiol. 2008 July ; 15(7): 827–834
• Lavall Daniel, Schäfers Hans-Joachim, Böhm Michael, Laufs Ulrich. Aneurysms of the Ascending
Aorta Dtsch Arztebl Int. 2012 March; 109(13): 227–233
Adamantios Tsangaris
Diana Litmanovich, MD

26
Acknowledgements
• Gillian Lieberman, MD
• Diana Litmanovich, MD
• Emmanouel Grigoriou
• Guangzu Gao
• Gagandeep Singh
• Ashton Lehmann
• Hailu Tilahun
• Claire Odom
Adamantios Tsangaris
Diana Litmanovich, MD