Embed Size (px)
Citation preview

Thorax, 1977, 32, 743-748
Delayed non-mycotic false aneurysm ofascending aortic cannulation siteA. S. SOORAE, J. CLELAND, AND H. O'KANE
From the Cardiac Surgical Unit, Royal Victoria Hospital, Grosvenor Road, Belfast BT12 6BA,Northern Ireland
Soorae, A. S., Cleland, J., and O'Kane, H. (1977). Thorax, 32, 743-748. Delayed non-mycoticfalse aneurysm of ascending aortic cannulation site. Two cases of delayed non-mycotic falseaneurysm arising from the ascending aortic cannulation site, presenting one-and-a-half yearsand seven years after cardiopulmonary bypass, are described. These two cases represent anincidence of 0O12% of this complication. Repair using profound hypothermia and circulatoryarrest with femoral artery and femoral vein cannulation for cardiopulmonary bypass isrecommended. The advantages and complications of aortic cannulation are discussed andrecommendations to minimise the complications of cannulation are made. The clinicalpresentation and diagnosis of non-mycotic false aneurysms arising from the aortic cannulationsite are described. In addition one delayed and two early cases of non-mycotic cannulation sitefalse aneurysms previously published are analysed. Surgeons should be alert to the possibility ofthis complication in all patients who have had aortic cannulation for cardiopulmonary bypasseven in ithe distant past. Unexpected symptoms such as constant anterior chest pain, dysphagia,hoarseness, and increasing widening of the superior mediastinum on the chest radiographwarrant prompt investigation.
Delayed non-mycotic false aneurysm arising fromthe ascending aortic cannulation site is a rare com-plication of this technique for arterial return incardiopulmonary bypass, and only one case hasbeen reported previously (Williams et al., 1976).We report a further two patients who presentedone-and-a-half years and seven years after theoriginal operation.A total of over 1600 aortic cannulations have
been carried out in our unit and the two casesreported here represent an incidence of 0-12% ofthis complication.
Case reports
CASE 1A 44-year-old man with a history of rheumaticfever at the age of 9 years had the mitral valvereplaced with a size 4 Starr-Edwards cloth-coveredprosthesis for mitral stenosis in October 1969 (seeTable). Cannulation and decannulation werecarried out uneventfully and the sternotomywound healed satisfactorily. The postoperative
progress was uncomplicated and he was dischargedfrom hospital two weeks after the operation.He was seen regularly in the outpatient depart-
ment and within six months he was working a12-hour day on his farm. However, he remainedin atrial fibrillation and 10 months later he under-went an unsuccessful attempt at DC cardioversion.During this procedure a small burn was producedover one of the sternal suture wires at the level ofthe manubriosternal junction, possibly due to in-appropriate contact with the electrode. This ulti-mately resulted in a sinus in which the sternal wirecould be easily palpated. This sinus was excisedand the sternal wire removed. Histological exam-ination showed a foreign-body reaction withchronic inflammatory cells but culture from thearea was sterile.The patient was readmitted to hospital in Feb-
ruary 1971 with a fluctuant swelling in the upperthird of the sternotomy scar at the site of the pre-vious sinus. This produced serosanguinous fluidwhen incised, but no organisms were culturedfrom the fluid. As he had a low-grade pyrexia,
743

A. S. Soorae, J. Cleland, and H. O'Kane
Table Details of cases of non-mycotic false aneurysm from ascending aortic cannulation site
Time betweenAge/sex operation and
Author ofpatient Original operation diagnosis Clinical presentation Re-operation Comment
Flick et al. (1971) 7 years Repair of 5 weeks Pulsatile mass in Successful repair by -Male membranous suprasternal notch. means of peripheral
subvalvular Chest radiograph- cannulation,aortic stenosis widening of profound
superior hypothermia, andmediastinum circulatory arrest
Branchini et al. (1976) 54 years Mitral valve 6 weeks Pulsatile mass in Repair under limited Patient died 40 hMale replacement upper third of cardiopulmonary later. Necropsy-
sternotomy scar. bypass and posterior myocardialChest radiograph- hypothermic infarction due tonon-contributory circulatory arrest right coronary artery
injury at operation.Subarachnoidhaemorrhage
Williams et al. (1976) 42 years Double aorta to 3 years Pulsatile swelling Successful repairMale coronary artery lower neck, with hypothermia
bypass grafts progressive and circulatorydysphagia, and arreststridor. Chestradiograph-densityin upper andanterior mediastinum
This studyCase 1 44 years Mitral valve 1 years Intermittent sinus Successful repair Aneurysm ruptured
Male replacement and haemorrhage without the aid of in anaesthetic room.from sternotomy cardiopulmonary Repair withoutscar. Chest bypass bypass was possibleradiograph- because of narrowwidening of neck (Fig. I) assuperior mediastinum bleeding could be
controlled withfinger tip
Case 2 62 years Mitral valve 7 years Pulsatile swelling in Repair using Patient died 27 daysFemale replacement anterior chest wall, peripheral postoperatively from
sternal pain, and cannulation, progressivesensation of cardiopulmonary respiratory andhoarseness. Chest bypass, hypothermia, hepatic failureradiograph- and circulatorycalcification and arrestwidening ofsuperior mediastinum
blood cultures were made, but no organisms weregrown. Intermittent bleeding and serosanguinousdischarge from the area slowly diminished, andthe patient was allowed to go home. He was read-mitted in March 1971 after a large haemorrhagefrom the same region. He was found to be clinic-ally anaemic, apyrexial, and in atrial fibrillation at76 per minute and his blood pressure was 110/70mmHg. Normal prosthetic valve sounds wereheard. A chest radiograph showed cardiomegalywith some widening of the superior mediastinumwhen compared with previous chest radiographs.Tomograms of the sternum suggested osteomye-litis. Exploration of the sinus was carried out andthe osteoporotic bone was nibbled away, revealinga pulsatile swelling behind the sternum. At thisstage the procedure was terminated. An aortogramperformed on the following day showed a falseaneurysm arising from the ascending aorta about2 cm proximal to the origin of the innominate
artery and lying between the aorta and the pos-terior surface of the sternum (Fig. 1).He was taken to the operating theatre the next
day for repair of the aneurysm. During inductionof anaesthesia the aneurysm ruptured, resulting intorrential haemorrhage. The sternum was partiallyopened without sterile precautions and control ofthe haemorrhage was obtained by inserting a fingerthrough the neck of the aneurysm, which wasabout 1 cm in diameter and situated at the pre-vious cannulation site. The sternal splitting wasformally completed while the finger effectivelycontrolled the bleeding. To close the orifice of theaneurysm, sutures buttressed with Teflon stripswere passed under the finger and tied, thus con-trolling the haemorrhage. The sac of the aneurysmwas then sutured over the front of the aorta.No organisms were cultured from the aneurysm
after three weeks of incubation and blood culturesbefore and after operation were all negative.
744

Delayed non-mycotic false aneurysm of ascending aortic cannulation site
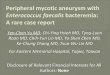
Fig. I Case 1. Aortogram, lateral view, showing falseaneurysm situated between the posterior surface of thesternum and ascending aorta; note the narrow neck.
His recovery following this near disaster was
uneventful, and he is alive and well six years afterthis episode.
Case 2
A 55-year-old woman with a history of rheumaticfever at the age of 26 years and a closed mitralvalvotomy at 41 years of age was admitted fortreatment of re-stenosis of the mitral valve and tri-cuspid incompetence (see Table). At operationin September 1969 the mitral valve was replacedby a size 3 Xtarr-Edwards cloth-covered prosthesis.The tricuspid incompetence, which was moder-ately severe, was thought to be functional and wasnot corrected. There was no difficulty with can-nulation or decannulation of the ascending aorta,nor was there excessive bleeding in the immediatepostoperative period, and the sternotomy woundhealed by first intention.The patient's exercise tolerance improved but in
the following year she had to be readmitted tohospital on three occasions with congestive heartfailure from tricuspid incompetence. The pros-thetic valve was functioning normally, but shecontinued to have signs of marked tricuspid in-competence with an enlarged liver and grosscardiomegaly.
In 1973 cholelithiasis was diagnosed but she wastreated conservatively because she was thought tobe too ill for surgery. She was readmitted tohospital in August 1976, now aged 62 years, witha year's history of sternal pain, made worse bycoughing and movement, and a sensation ofhoarseness for two or three months. A week be-fore admission she had noticed a swelling in thefront of the chest which was painful and increas-ing in size. There was no history of dysphagia.On examination she was in slow atrial fibrilla-
tion with equal pulses in both arms and a bloodpressure of 135/75 mmHg. The jugular venouspressure was raised with a large 'v' wave. Theliver was enlarged, and there was clinical evidenceof right and left ventricular hypertrophy. Normalprosthetic valve sounds were heard. A pulsatileswelling 6-5X60 cm over the upper third andslightly to the right of the sternotomy scar wasvisible. A systolic thrill was felt over it and asystolic murmur was heard. The chest radiographshowed gross cardiomegaly with widening andfaint calcification in the right side of the superiormediastinum. Cardiac catheterisation showed poorleft ventricular function and tricuspid incom-petence. An aortogram revealed a jet 2 cm proxi-mal to the origin of the innominate artery fillinga saccular cavity lying anterior and to the rightof the ascending aorta. (Fig. 2).
Because of the risk of rupture it was decided torepair the aneurysm despite her poor haemo-dynamic condition. In September 1976 bypass was
745

A. S. Soorae, J. Cleland, and H. O'Kane
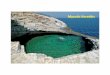
Fig. 2 Case 2. Aortogram, lateral view, showinganeurysm between the sternum and ascending aorta;note the wide neck.
instituted with right femoral artery and vein can-
nulation and cooling to 22°C. The artery was
cannulated with a size 20 arterial cannulal andthe venous cannula was introduced approximatelyas far as the right atrium. The aneurysm, which
IUSCI, Division ofCR Bard Inc, Ballerica, Massachusetts 01 821, USA
was partially calcified, ruptured when the sternumwas opened. Bleeding at this stage was controlledby reducing the pump flow and inserting a fingerin the neck of the aneurysm, which was dissectedfree and found to be arising from the previouscannulation site.The circulation was arrested and repair was
carried out by direct suture over pledgets of Teflonthrough the neck of the aneurysm. It was noticedat this stage that a tear had been produced at thejunction of the superior vena cava and the in-nominate vein as a result of retraction of thesternum before adequate freeing of adhesions.This allowed air to enter the venous system. Cir-culatory arrest was continued for longer thananticipated while the tear was being repaired.After re-warming the heart started to beat spon-taneously but it needed considerable inotropicsupport before cardiopulmonary bypass could beterminated. After the operation the patient soonwoke up and the following morning all inotropicdrugs were discontinued.Her early progress was satisfactory but she
developed a Klebsiella chest infection and respira-tory failure followed. A tracheostomy wasperformed and prolonged artificial ventilation con-tinued. She subsequently developed hepatic failure,no doubt as a result of long-standing tricuspid in-competence, and there was a gradual deteriorationin her condition until she died 27 days after theoperation. Permission for necropsy was refused.
Technique of cannulation of ascending aorta
The technique of cannulation to be described herehas been used in all cases of ascending aortic can-nulation for cardiopulmonary bypass in our unit.A 3-0 Ethiflex suture mounted on a 17 mm
half-circle needle is inserted as a superficial purse-string into the adventitia and outer media on theanterior surface of the ascending aorta proximalto the origin of the innominate artery. The diam-eter of the purse-string is slightly greater thanthat of the cannula to be used. A second, similarpurse-string is inserted immediately outside thefirst, and the ends of both sutures are threadedthrough separate 6-8 cm long thin tubing 'snares'.
In adults, a size 6, 60 cm long, Portex2 atrialcannula, with a 450 bevel at the end and withoutside holes, is used for cannulation. A double Mer-silene suture is applied on the cannula 2-3 cm fromthe tip to act as a marker. A polished stainless steelconnector is attached to the outer end of thecannula.A lateral occlusion clamp is applied longitudin-
'Portex Limited, Hythe, Kent, UK
<I
/NI-
\ V~~
r = 7w |~t I i ss-w
746

Delayed non-mycotic false aneurysm of ascending aortic cannulation site
ally enclosing the area of the purse-strings and alongitudinal incision slightly smaller than thediameter of the cannula is made with a No. 11
Bard Parker scalpel blade. The aortotomy is in-spected to ensure that the incision has not dis-sected into the wall and the edges are gently heldapart with Potts-Smith diamond jaw forceps: asthe cannula, held near its tip, is quickly guidedalong the forceps into the aortic lumen the clampis released. The cannula is inserted as far as themarker suture, the purse-strings are tightened, andthe snares are tied to the cannula thus securing itin position. We think that this technique, in whichthe cannula is introduced under direct vision andguided into the aortic lumen along the forcepsholding the edges of the aorta, prevents the tip ofthe cannula dissecting into the wall of the aorta.At the conclusion of perfusion a lateral occlu-
sion clamp is re-applied and the cannula is re-moved simultaneously. The aortotomy is closedwith a continuous 4-0 Prolene stitch in two layersand the purse-strings are tied without tension.
Discussion
The use of direct cannulation of the ascendingaorta for cardiopulmonary bypass has been gener-
ally accepted after early reports by Niunez andBailey (1959) and DeWall and Levy (1963).The reported complications of direct cannula-
tion of the ascending aorta include acute aorticdissection (Salama and Blesovsky, 1970; Reinkeet al., 1974; Williams et al., 1974), excessivehaemorrhage from the cannulation site necessitat-ing re-operation (Gerbode et al., 1968), and carotidhyperperfusion causing fatal brain damage (Kul-karni, 1968; Krous et al., 1973). Some postperfusiondeaths, especially in children, may be due to inade-quate aortic arch perfusion, as suggested by Parker(1969). Mycotic false aneurysms arising from theaortic cannulation site, secondary to mediastinalinfection, have been described (Lillehei et al.,1969; Salama and Blesovsky, 1970), but falseaneurysms from this site in the absence of infec-tion are extremely rare and only three reportedcases could be found. Two of these three cases
presented in the early postoperative period and thethird one presented late, as in our two cases re-
ported here (Table). Cannulation site aneurysm
can present either in the early postoperative period(Flick et al., 1971; Branchini et al., 1976) or may
be delayed for years, as reported by Williams et
al. (1976) and as occurred in our two cases.
The diagnosis of non-mycotic aneurysms fromthe ascending aortic cannulation site should besuspected if there is a pulsatile mass in the anterior
chest wall or lower neck and increasing wideningof the superior mediastinum on a chest radio-graph. Four out of the five cases reviewed herehad these features in common. Other less commonfeatures included symptoms caused by pressure ofthe aneurysm on surrounding structures, such assternal pain, sternal erosion, progressive stridor,and dysphagia (Table). The bony changes due topressure on the posterior surface of the sternumled to the mistaken diagnosis of osteomyelitis incase 1. To confirm the diagnosis of a suspectedfalse aneurysm a biplane aortogram is mandatory.There is no satisfactory explanation of the cause
of this complication in our two cases. There wereno difficulties with cannulation or decannulationat the original operation, no excessive postopera-tive bleeding, no mediastinal or wound infection,and the patients were not hypertensive in the im-mediate or late postoperative period. At the timeof re-operation there was no obvious infection inthe mediastinum and no organisms could be cul-tured from the aneurysms. There is, however, aremote possibility that the electrical burn overthe sternal suture wire in case 1, which occurredat the time of cardioversion, also selectively causeda burn over the aorta with resulting aortic wallnecrosis and aneurysmal formation. Neither cana satisfactory explanation be given for the pre-viously published cases with the possible exceptionof the patient of Branchini et al. (1976) in whomdifficulty with haemostasis from the cannulationsite necessitated the use of extra pledgets ofTeflon.
In order to minimise the complications of can-nulation we recommend that the aortotomy shouldbe slightly smaller than the diameter of the can-nula and in the longitudinal axis of the aorta. Theaortotomy should be made inside a superficiallyplaced double purse-string. The cannula shouldnot be inserted for more than 2-3 cm into theaortic lumen and it should lie free within theaorta, as indicated by adequate arterial line andperipheral arterial pressures. Through-and-throughstitches should be used to close the aortotomy,buttressed by Teflon pledgets if necessary, and thepurse-strings should not be tied under tension. Ifthe aorta is markedly atheromatous, repeatedclamping and unclamping should be avoided. Ifthe aorta is grossly calcified or aneurysmal femoralartery cannulation should be used. Severe hyper-tension in the immediate postoperative periodshould be controlled and the systolic blood pres-sure should not be allowed to exceed 150 mmHg.We consider that repair using femoral artery
and femoral vein cannulation, cardiopulmonarybypass, profound hypothermia, and circulatory
747

A. S. Soorae, J. Cleland, and H. O'Kane
arrest is the best way of treating these aneurysms(Lillehei et al., 1969; Salama and Blesovsky, 1970).The aneurysm in case 1 ruptured in unusual cir-cumstances and no planned procedure could becarried out. It had a narrow neck (Fig. 1), thebleeding could be controlled with a finger, and itwas possible to repair it without the aid of bypass.The actual extent of the aneurysm and the size ofthe neck at operation do not always correlate wellwith the aortographic appearances, as in ourcase 2.The aneurysm frequently ruptures when the
sternum is opened (Lillehei et al., 1969; Branchiniet al., 1976) and hence adequate cooling shouldprecede sternotomy so that the circulation can bearrested. The patient's blood is drained into theoxygenator, and thus a bloodless operative field isachieved. Injudicious spreading of the sternum isbest avoided if damage to the heart and underlyingvessels is to be prevented (Lillehei et al., 1969;Branchini et al., 1976). The tear at the junction ofthe superior vena cava and innominate artery inour case 2 could thus have been avoided. There isa great danger of air being sucked into the aorta,causing fatal air embolism, when the circulationis arrested and the aneurysm is opened. The per-fusion pump should be kept turning very slowlyin order to maintain a positive pressure in theaorta; this can be combined with a Trendelenburgtilt of the table of about 300. Direct suction intothe aorta should of course be avoided.
Cannulation of the ascending aorta has provedto be a safe and simple technique with an ac-ceptably low incidence of complications, varyingfrom 0 11% (Flick et al., 1971) to 05% (Gerbodeet al., 1968). It avoids some of the complicationsassociated with femoral artery cannulation, whichhave been reported to vary from 1 2% (Roe andKelly, 1969) to 5 4% (Gerbode et al., 1968), thatis, much higher than in aortic cannulation. Aorticcannulation allows larger cannulae to be used,which can be of great importance in children(Nuinez and Bailey, 1959), and avoids a secondoperative field of questionable sterility. The arterialperfusion site is under direct vision all the timeand hence early detection and correction of anycomplication from it is possible.
References
Branchini, B., Zingone, B., and Vaccari, M. (1976).Ascending aortic false aneurysm following cannula-tion for perfusion. Thorax, 31, 234-237.
DeWall, R. A., and Levy, M. J. (1963). Direct can-nulation of the ascending aorta for open-heartsurgery. Journal of Thoracic and CardiovascularSurgery, 45, 496-499.
Flick, W. F., Hallermann, F. J., Feldt, R. H., andDanielson, G. K. (1971). Aneurysm of aortic can-nulation site: successful repair by means of per-ipheral cannulation, profound hypothermia, andcirculatory arrest. Journal of Thoracic andCardiovascular Surgery, 61, 419-423.
Gerbode, F., Kerth, W. J., Kovacs, G., Sanchez, P. A.,and Hill J. D. (1968). Cannulation of the ascendingaorta for perfusion during cardiopulmonary bypass.Journal of Cardiovascular Surgery, 9, 293-296.
Krous, H. F., Mansfield, P. B., and Sauvage, L. R.(1973). Carotid artery hyperperfusion during open-heart surgery: Report of a case. Journal of Thoracicand Cardiovascular Surgery, 66, 118-121.
Kulkarni, M. G. (1968). A complication of aortic can-nulation. Journal of Cardiovascular Surgery, 9, 207-208.
Lillehei, C. W., Todd, D. B., Jr., Levey, M. J., andEllis, R. J. (1969). Partial cardiopulmonary bypass,hypothermia, and total circulatory arrest. A lifesaving technique for ruptured mycotic aorticaneurysms, ruptured left ventricle and other com-plicated cardiac pathology. Journal of Thoracic andCardiovascular Surgery, 58, 530-544.
Nunez, L. E., and Bailey, C. P. (1959). New methodfor systemic arterial perfusion in extracorporeal cir-culation. Journal of Thoracic Surgery, 37, 707-710.
Parker, R. (1969). Aortic cannulation. Thorax, 24,742-745.
Reinke, R. T., Harris, R. D., Klein, A. J., and Daily,P. 0. (1974). Aortoiliac dissection due to aorticcannulation. Annals of Thoracic Surgery, 18, 295-299.
Roe, B. B., and Kelly, P. B. (1969). Perfusion throughthe ascending aorta: experience with 410 cases.Annals of Thoracic Surgery, 7, 238-241.
Salama, F. D., and Blesovsky, A. (1970). Complica-tions of cannulation of the ascending aorta for openheart surgery. Thorax, 25, 604-607.
Williams, C. D., Suwansirikul, S., and Engelman,R. M. (1974). Thoracic aortic dissection followingcannulation for perfusion. Annals of Thoracic Sur-gery, 18, 300-304.
Williams, G. D., Zimmerman, G. J., Osam, P. N., andDaniel, M. S. (1976). False aneurysm of aortic can-
nulation site occurring three years postoperatively:successful repair with hypothermia and circulatoryarrest. Journal of Cardiovascular Surgery, 17, 266-269.
Requests for reprints to: H. O'Kane, BSc, FRCS,MCh, Cardiac Surgical Unit, Royal Victoria Hospital,Belfast BT12 6BA. Northern Ireland.
748