Embed Size (px)
Citation preview

Imaging Findings in the Injuries to the Neck Muscles – Examples with
Review of Anatomy
E. Scortegagna Jr., MD
K. de Macedo Rodrigues, MD
A. Abayazeed, MD
S. K. Dundamadappa, MD
D. Takhtani, MD
University of Massachusetts Medical School – UMASSWorcester – MA - USA
eEdE-87

Disclosures
The authors have no actual or potential conflict of interest in relation to this electronic exhibit

Objectives
• To review the anatomic aspects of the neck muscles
• To review the imaging findings in the injuries to the muscles of the neck

Introduction• Most studies on trauma to the cervical spine have focused on
the injuries to the ligament, disc, bone, and the spinal cord. There is hardly any report in the literature on the imaging findings in the injuries to the muscles of the neck.
• The osseoligamentous system contributes 20% to the mechanical stability of the cervical spine, while the remaining 80% is provided by the surrounding neck musculature.
• With increasing use of MRI in the patients with neck trauma, we come across several examples of injury to the neck muscles with or without fractures and ligament injuries.

Cervical spine/neck muscles anatomy review
In the following slides, we present a focused review of numerous muscles of the cervical region with examples of injuries to some of them

Anatomy – anterior vertebral musclesMuscle Origin Insertion
Function
Longus Colli Three parts Superior oblique
Inferior oblique
Vertical
Ant. Surface of vertebral column
3/4/5th ant. Transv. Processes
First 2 or 3 ant vert. bodies
Front of upper 3 thoracic bodies
Anterior arch of the atlas
Anterior 5/6th cervical vertebrae
2/3/4th cervical vertebrae
Flexes and rotates the cervical portion of the vertebral column
Longus Capitis Anterior tubercles of anterior transverse processes of the 3/4/5/6th cervical vertebrae
Inferior surface of the basilar part of the occipital bone
Antagonist of the muscles at the back. Restores the head to its natural position after drawn backward. Also flexes the head and rotate it.
Rectus capitis anterior
Located post. to the longus colliAnterior surface of lateral mass of the atlas
Inferior surface of the jugular process of the occipital bone
Similar to Longus Capitis.
Rectus capitis lateralis
Upper surface of the transverse process of the atlas
Under surface of the jugular process of the occipital bone
Bends the head laterally.
Gray’s anatomy of the human body: Twentieth edition, Revised by Warren H. Lewis, New york: Bartleby.com, 2000

Anatomy – posterior vertebral muscles
Muscle Origin Insertion Function
Splenius capitis Lower half of ligamentum nuchae, from spinous process of 7th and upper 3 or 4 cervical vertebrae
Mastoid process of the temporal and occipital bones
Draw the head backward, assisting the trapezius and semispinalis capitis. Acting separately they can draw the back to one side and slightly rotate
Splenius Cervicis Spinous processes from 3rd to 6th thoracic vertebrae
Posterior tubercle of the transverse processes of the 2 or 3 cervical vertebrae
Same as spleinus capitis
Semispinalis capitis
Transverse processes of the upper 6 or 7 thoracic and 7th cervical vertebrae, and articular process of 3 cervical vertebrae above
Between superior and inferior nuchal lines of the occipital bone
Head extension, lateral flexion and rotation of the cervical spine
Multifidus Articular processes of the lower 4 cervical vertebrae
Into the spinous process of the vertebrae above
Stabilization and rotation of the spine
Gray’s anatomy of the human body: Twentieth edition, Revised by Warren H. Lewis, New york: Bartleby.com, 2000

Anatomy – posterior vertebral muscles (cont.)
Muscle Origin Insertion Function
Longissimus cervicis
Transverse processes of the 4 or 5 thoracic vertebrae
Posterior tubercles of the transverse processes from 2nd to 6th cervical vertebrae
Bilaterally extends the cervical spine. Unilaterally produces extension of the neck to the same side
Longissimus capitis
Transverse processes of the 4 o 5 thoracic vertebrae and articular processes of lower 3 or 4 cervical vertebrae
Posterior margin of the mastoid process
Bilaterally extends and hyperextends the head. Unilaterally flexes and rotates the head to the same side.
Gray’s anatomy of the human body: Twentieth edition, Revised by Warren H. Lewis, New york: Bartleby.com, 2000

Anatomy – lateral vertebral muscles
Muscle Origin Insertion Function
Scalenus anterior Anterior tubercles of anterior processes of 3/4/5/6th vertebrae
Inner board and upper surface of the 1st rib
Elevate the first and second ribs, acting as inspiratory muscle
Scalenus medius Largest and longest of the three. Arises from post. Tubercles of transverse processes of lower 6 vertebrae
Upper surface of the first rib Similar to scalenus anterior
Scalenus posterior Posterior tubercles of transverse processes of lower 2 or 3 cervical vertebrae
Outer surface of the 2nd rib, behind the serratus anterior
Similar to scalenus anterior
Gray’s anatomy of the human body: Twentieth edition, Revised by Warren H. Lewis, New york: Bartleby.com, 2000

Anatomy – lateral cervical muscles
Muscle Origin Insertion Function
Sternocleidomastoideus Sternum and clavicle (2 heads)Sternum – medial head -Anterior manubrium sterniClavicle – lateral head - Medial third of clavicle
Both heads are inserted into the lateral surface of the mastoid process and superior nuchal line of the occipital bone
Bilaterally it flexes and extends the head. Unilaterally rotates to the opposite side and flexes to the same side.
Trapezius External occipital protuberance and medial third of superior nuchal line of the occipital bone, ligamentum nuchae, spinous process of the 7th cervical, and spinous processes of all thoracic vertebrae
Superior fibers are inserted into the posterior border of the lateral third clavicle. Middle fibers into the medial margin of the acromion and superior lip of posterior border of spine and scapula. Inferior fibers converge near the scapula and end in an aponeurosis to be inserted into a tubercle at the apex of this smooth triangular surface
Main function is to stabilizes and move the scapulae.
Gray’s anatomy of the human body: Twentieth edition, Revised by Warren H. Lewis, New york: Bartleby.com, 2000

Anatomy – superficial muscle
Muscle Origin Insertion Function
Platysma Fascia covering the upper parts of the Pectoralis major and Deltoideus, extend superiorly along the side of the neck
Some fibers insert in the mandible, others into the skin and subcutaneous of the lower face. Fibers can insert partially in the zygomaticus or orbicularis oculi
Wrinkles the skin of the neck. Also serves to draw down the lower lip and angle the mouth in expression of melancholy.
Gray’s anatomy of the human body: Twentieth edition, Revised by Warren H. Lewis, New york: Bartleby.com, 2000

Image based anatomy
Rectus capitis posterior major
Longus capitis
Sternocleidomastoid
Splenius capitis
Semispinalis capitis
Trapezius
Obliquus capitis inferior
Medial pterygoid
Digastric – posterior belly

Image based anatomy
Longus colli
Longus capitis
Semispinalis cervicis
Multifidus
Trapezius
Levator scapulae
Sternocleidomastoid
Splenius capitis
Splenius cervicis

Image based anatomy
Trapezius
Longus colli
Longus capitis
Scalenus anterior
Scalenus medius
Levator scapulae
Splenius capitis
Rhomboid minor
Multifidus
Semispinalis cervicis
Semispinalis capitis
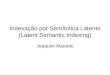
Image based anatomy
Trapezius
Rhomboid minor
Splenus capitis
Multifidus
Semispinalis cervicis
Levator scapulae
Longus colli
Scalenus medius
Scalenus posterior
Methods
• We have reviewed MRI scans of patients with traumatic injuries to the neck over the past eight years to look for injuries to the neck muscles.
• Routine MRI of the cervical spine for trauma in our institution includes: Spin Echo T1 sagittal, Fast Spin Echo T2 sagittal, Short Tau Inversion Recovery sagittal, Fast Spin Echo T2 axial and Gradient T2 axial sequences.

Patient #1
19-year-old female involved in a motor vehicle accident with loss of consciousness

a b
c dFigure 1: a,b: Axial STIR images demonstrate hyperintensity within the bilateral sternocleidomastoid muscles (arrows) and bilateral scalene muscles (b: circles). c: Coronal STIR image demonstrating the extensive injury of the scalene muscles (brackets) and d: Sagittal T2 sequence showing the extension of the left sternocleidomastoid injury (arrows).

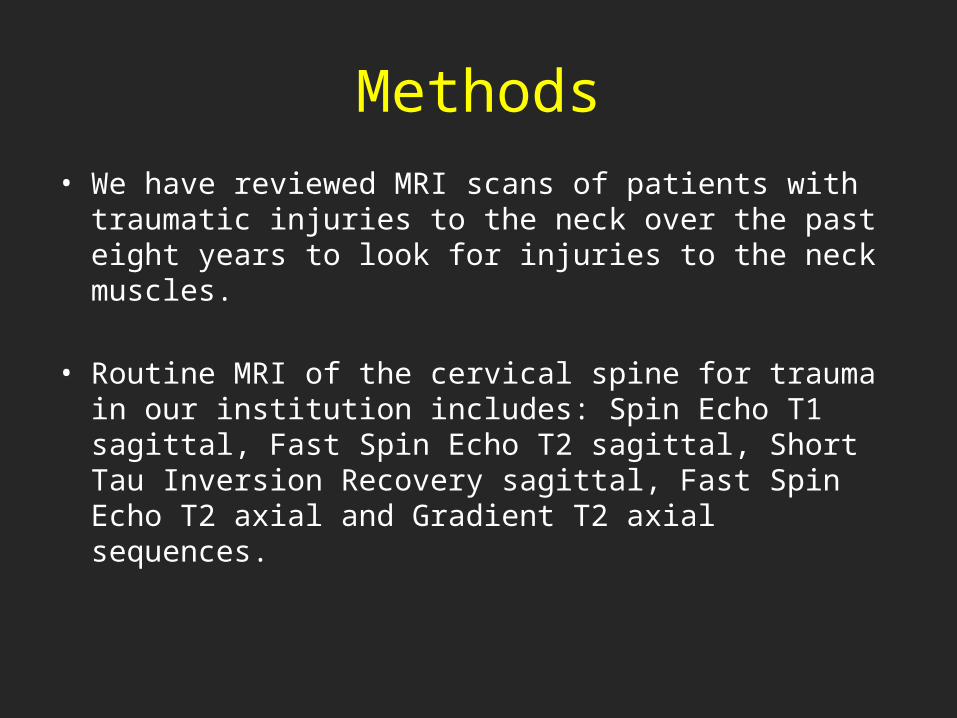
Patient #2
55-year-old female with history of fall at home and loss of consciousness
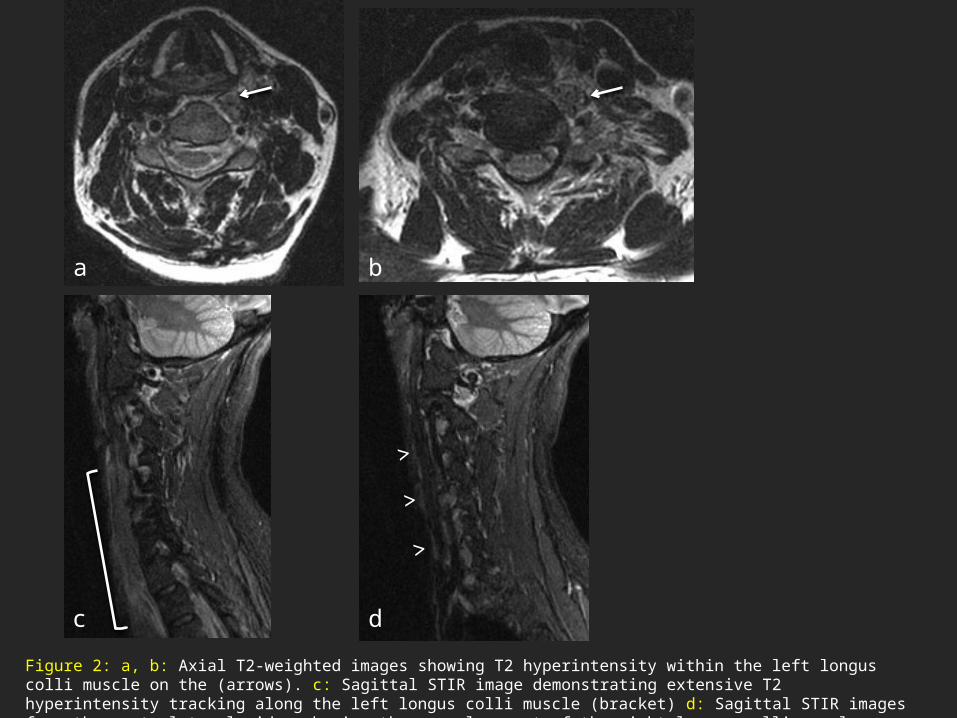
Figure 2: a, b: Axial T2-weighted images showing T2 hyperintensity within the left longus colli muscle on the (arrows). c: Sagittal STIR image demonstrating extensive T2 hyperintensity tracking along the left longus colli muscle (bracket) d: Sagittal STIR images from the contralateral side, showing the normal aspect of the right longus colli muscle (arrowheads).
a b
c d
>
>
>
Patient #3
45 year-old male involved in a motor vehicle accident as a pedestrian, with associated loss of consciousness
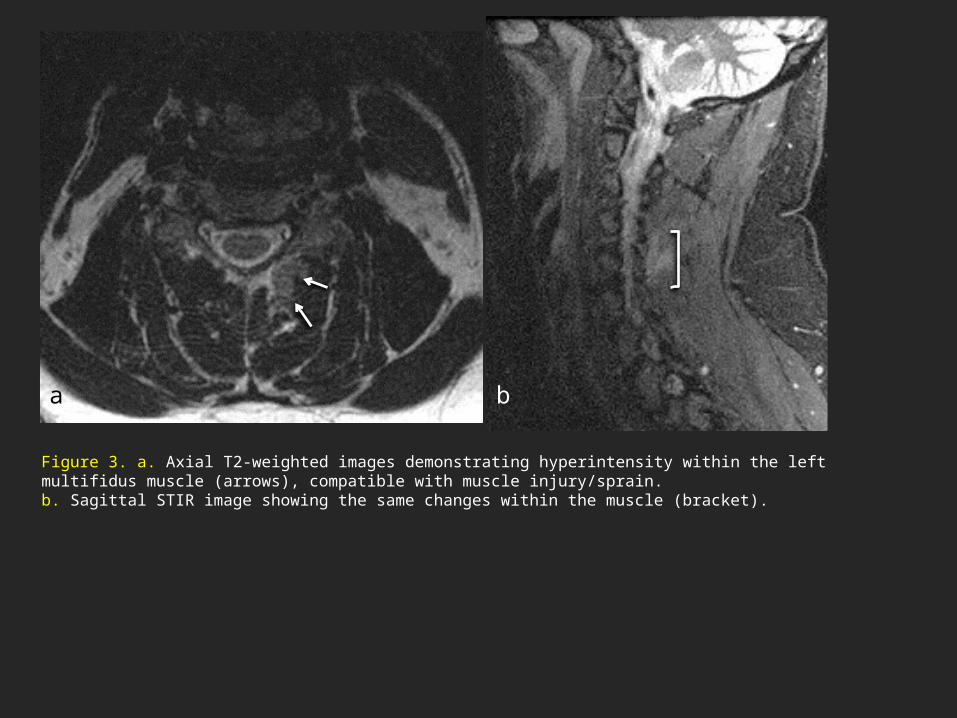
Figure 3. a. Axial T2-weighted images demonstrating hyperintensity within the left multifidus muscle (arrows), compatible with muscle injury/sprain. b. Sagittal STIR image showing the same changes within the muscle (bracket).
a b
Patient #4
34-year-old found unresponsive at home and with persistent left arm deficit
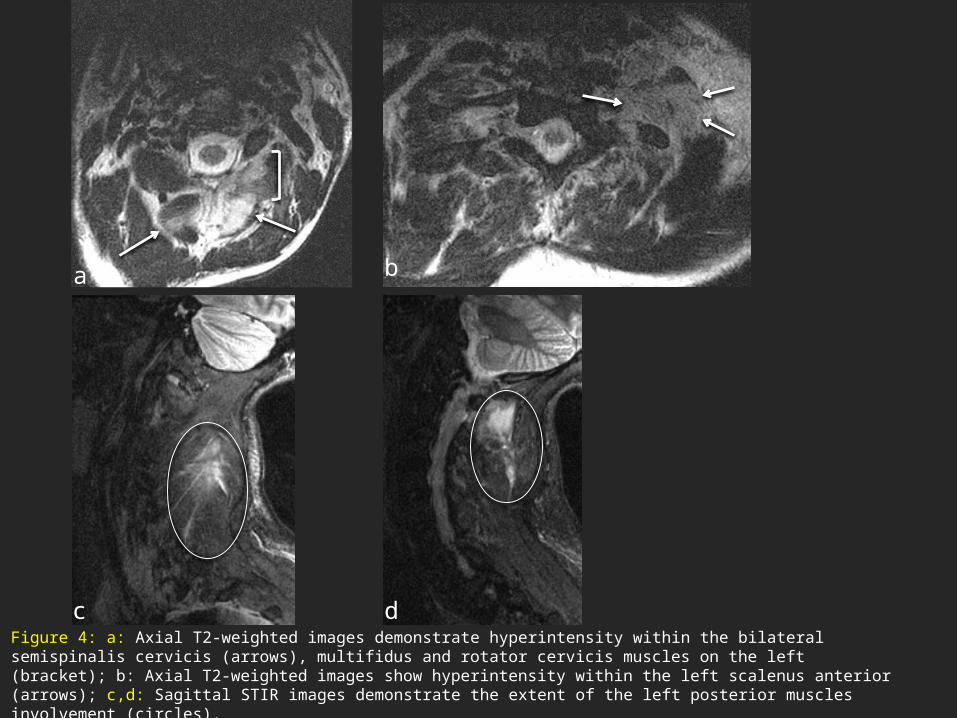
Figure 4: a: Axial T2-weighted images demonstrate hyperintensity within the bilateral semispinalis cervicis (arrows), multifidus and rotator cervicis muscles on the left (bracket); b: Axial T2-weighted images show hyperintensity within the left scalenus anterior (arrows); c,d: Sagittal STIR images demonstrate the extent of the left posterior muscles involvement (circles).
a b
c d

Patient #5
10-year-old injured while performing gymnastics

Figure 5: a,b: Axial T2-weighted images demonstrate hyperintensity within the bilateral semispinalis cervicis muscles, left greater then right (arrows); c: Sagittal STIR images demonstrates the extent of the injury (circle).
a b
c

Patient #6
64-year-old with history of helmeted motorcycle crash with multiple facial fractures
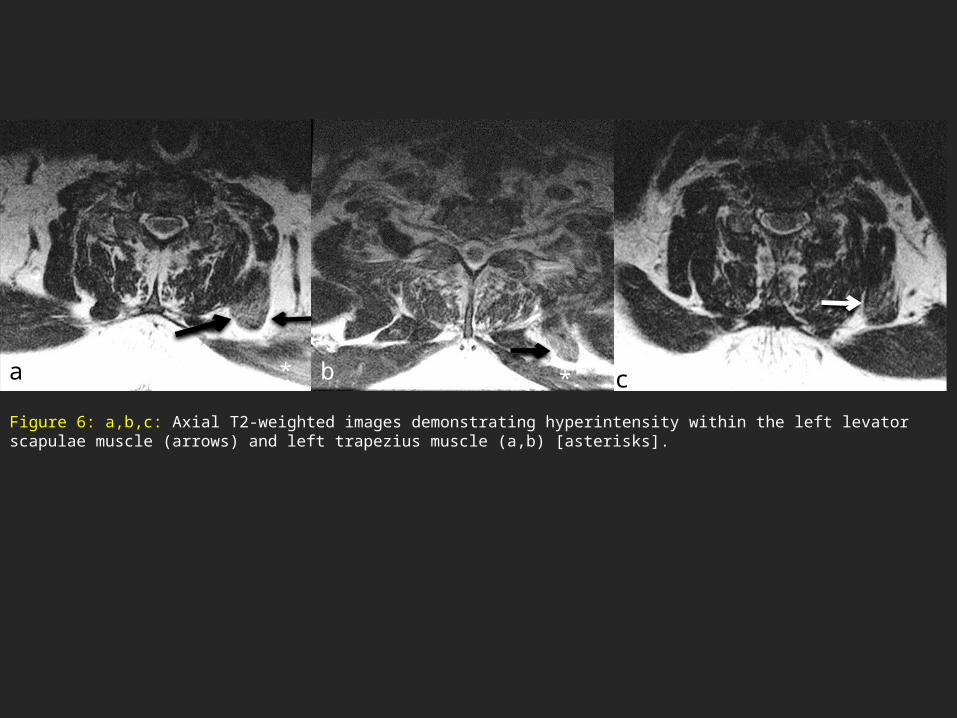
Figure 6: a,b,c: Axial T2-weighted images demonstrating hyperintensity within the left levator scapulae muscle (arrows) and left trapezius muscle (a,b) [asterisks].
a b c* *

Patient #7
71-year-old male found down in pulseless electrical activity

Figure 7: axial T2-weighted image demonstrating hyperintensity within the right anterior scalene muscle (arrows)
Patient #8
68-year-old female who fell down 15 stairs.

Figure 8: a,b: axial T2-weighted images demonstrating hyperintensity within the right longus colli muscle (arrow). There is also hyperintensity within the left semispinalis cervicis on the left side (a) [circle]. c: Sagittal STIR images demonstrating hyperintensity within the left semispinalis cervicis muscle (circle). d: Sagittal STIR demonstrate the extent of the injury to the right longus colli muscle shown on the axial images (arrows).
a b c
d

Patient #9
22-year-old male with history of motor vehicle accident

Figure 9: a, b: Axial CT images showing contusions within the right semispinalis muscle (arrow), splenius capitis (asterisk) . c, d: Coronal and Sagittal CT images demonstrate the contusions described in the axial planes (arrows). Edema can also be seen tracking along the fascial planes, better seen on the axial images.
*
*
a
b
c
d

Discussion• Plain films have a limited role in the injury to the neck. A subset of patients
with neck injury will even have normal CT. In one large meta-analysis
involving 464 patients, MRI showed additional findings in nearly 20% of
patients that were not seen in the plain films with or without CT [2].
• In another large series of 174 patients who underwent MRI for occult
injuries of the cervical spine after their plain X-rays were normal, 36% (62)
patients had evidence of soft tissue injury. Both these studies concluded
that negative MRI should be a confirmation of cleared spine [3].
• American college of Radiology also advocates use of MRI in case of
suspected soft tissue injury.

Discussion• The injury to the soft tissues of the neck can involve the flexor or extensor
muscles depending on the nature of injury.
• The flexion injuries cause sprain of the extensors whereas the whiplash
injuries damage the flexor group. There are also cases of direct injury to the
muscles causing contusion.
• On MR imaging, the most common findings of muscle injury are swelling of
the muscle and edema (high T2 signal). In addition to this, patients can
present with rupture of muscle fibers, intramuscular hematoma and bleeding,
or reactive fluid in the adjacent soft tissues. These changes are best seen on
the short tau inversion recovery (STIR) and FSET2 sequences.

Conclusion
Injuries to the neck muscles can be an important finding on MRI, which in our opinion is often overlooked. Patient with pain following neck trauma can greatly benefit from correctly identifying various components of neck injury, which can guide appropriate management and follow-up.

References
1. Panjabi MM, Cholewichi J, Nibu K, Grauer J, Babat LB,Dvorak J. Critical load of the human cervical spine: an in vitro experimental study. Clin Biomech (Bristol, Avon). 1998 Jan;13(1):11-17. 2. Muchow RD, Resnick DK, Abdel MP, Munoz A, Anderson PA. Magnetic resonance imaging (MRI) in the clearance of the cervical spine in blunt trauma: A meta-analysis. J Trauma. 2008;64(1):179-189. 3. Benzel EC, Hart BL, Ball PA, Baldwin NG, Orrison WW, Espinosa MC. Magnetic resonance imaging for the evaluation of patients with occult cervical spine injury. J Neurosurg. 1996;85(5):824-829. 4. Branstetter BF 4th, Weissman JL. Normal anatomy of the neck with CT and MR imaging correlation. Radiol Clin North Am. 2000 Sep;38(5):925-40, ix.
5. Gray’s anatomy of the human body: Twentieth edition, Revised by Warren H. Lewis, New york: Bartleby.com, 2000