Embed Size (px)
Citation preview

Imaging degenerative disk Imaging degenerative disk disease in the lumbar disease in the lumbar
spinespine
Elaine Besancon MS IIIDr. Gillian Lieberman

Learning ObjectivesLearning Objectives
Anatomy reviewAnatomy review
Pathophysiology of degenerative disc Pathophysiology of degenerative disc diseasedisease
Common Common sequelaesequelae of disk diseaseof disk disease–– HerniationHerniation–– StenosisStenosis–– InstabilityInstability
Imaging modalitiesImaging modalities
Clinical OutcomesClinical Outcomes

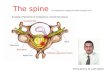
Anatomy of the three Anatomy of the three joint complexjoint complex
Degenerative disk disease is a poorly defined term.Degenerative disk disease is a poorly defined term.Often misused, but generally agreed to refer to pathology associOften misused, but generally agreed to refer to pathology associated with ated with repetitive traumatic injury to the repetitive traumatic injury to the ““threethree--jointjoint--complexcomplex”” of the spineof the spine
EndplateEndplate--discdisc--endplateendplate2 facet joints2 facet joints
Image courtesy of Dr. Rafael Rojas

Anatomy of the three Anatomy of the three joint complexjoint complex
Degenerative disk disease is a poorly defined term.Degenerative disk disease is a poorly defined term.Often misused, but generally agreed to refer to pathology associOften misused, but generally agreed to refer to pathology associated with ated with repetitive traumatic injury to the repetitive traumatic injury to the ““threethree--jointjoint--complexcomplex”” of the spineof the spine
EndplateEndplate--discdisc--endplateendplate2 facet joints2 facet joints
Image courtesy of Dr. Rafael Rojas

Pathophysiology of disk Pathophysiology of disk injuryinjury
Failure of disks most Failure of disks most common in regions with common in regions with highest mechanical stress, highest mechanical stress, especially lower lumbar especially lower lumbar region.region.
Disc nutrition dependent on Disc nutrition dependent on diffusion from marrow of diffusion from marrow of bone or from blood vessels bone or from blood vessels through annulusthrough annulus
Whether primary pathology Whether primary pathology is usually metabolic or is usually metabolic or mechanical is not known.mechanical is not known.
Image courtesy of Dr. Rafael Rojas

Pathophysiology of disk Pathophysiology of disk injury continuedinjury continued
•Deformation of endplate and loss of water in the nucleus can lead to abnormal forces on annulus
•Small contribution from various environmental factors like exercise, trauma.
•Twin studies suggest large role for genetic predisposition.
•Collagen•Cytokines (IL-2)
Image courtesy of Dr. Rafael Rojas

Common featuresCommon features
Common Common sequelaesequelae of disk disease of disk disease –– HerniationHerniation–– StenosisStenosis–– InstabilityInstability

Common featuresCommon features
Common Common sequelaesequelae of disk disease of disk disease –– HerniationHerniation–– StenosisStenosis–– InstabilityInstability

Index Patient: Low back Index Patient: Low back painpain
49 year-old woman presents for evaluation of low back pain that radiates down to her lower legs.
Do you image her?

When to image for low When to image for low back painback pain
85% of people with LBP are never given a precise 85% of people with LBP are never given a precise pathoanatomicalpathoanatomical diagnosis, diagnosis, even with imagingeven with imaging
Imaging findings and symptoms do not correlate precisely Imaging findings and symptoms do not correlate precisely
Indications of a more complicated status, often termed "red flagIndications of a more complicated status, often termed "red flags," include s," include the following:the following:
–– Recent significant trauma, or milder trauma, age >50 Recent significant trauma, or milder trauma, age >50 –– Unexplained weight loss Unexplained weight loss –– Unexplained fever Unexplained fever –– ImmunosuppressionImmunosuppression–– History of cancer History of cancer –– Intravenous (IV) drug use Intravenous (IV) drug use –– Prolonged use of corticosteroids, osteoporosis Prolonged use of corticosteroids, osteoporosis –– Age >70 Age >70 –– Focal neurologic deficit with progressive or disabling symptoms Focal neurologic deficit with progressive or disabling symptoms –– Duration longer than 6 weeksDuration longer than 6 weeks

Index Patient: Persistent Index Patient: Persistent low back painlow back pain
49 year-old woman presents for evaluation of low back pain that radiates down to her lower legs.
Do you image her?
Initially, no.
However, she returns with continuing pain after 6 weeks.

Imaging ModalitiesImaging Modalities
Plain filmPlain film
MRI MRI – Most accurate modality for assessing
intervertebral disk disease.
CTCT–– CT CT myelogrammyelogram

Imaging Modalities: Plain Imaging Modalities: Plain FilmFilm
Plain filmPlain film–– ProsPros
FastFast
Low CostLow Cost
Good for bony abnormalitiesGood for bony abnormalities
–– ConsCons
Poor visualization of disksPoor visualization of disks
Radiation exposureRadiation exposure
Most abnormalities seen on xMost abnormalities seen on x--ray can be better ray can be better characterized on CT or MRI.characterized on CT or MRI.

Imaging Modalities: MRIImaging Modalities: MRI
MRI MRI –– Pros:Pros:
Most accurate modality for assessing intervertebral disk disease.
Excellent for soft tissue abnormalities
No radiation exposure– Cons
Less useful for bony abnormalities
Higher costHigher cost
Contraindicated in patients with ferromagnetic objects in Contraindicated in patients with ferromagnetic objects in their bodies, or patients with implanted electronic devices. their bodies, or patients with implanted electronic devices.
Claustrophobia or inability to hold still for long periods of Claustrophobia or inability to hold still for long periods of time may prevent patients from completing the MRI.time may prevent patients from completing the MRI.

Imaging Modalities: CTImaging Modalities: CT
CTCT–– Only indicated for imaging of disk disease in patients who Only indicated for imaging of disk disease in patients who
have contraindications to MRI.have contraindications to MRI.–– Pros:Pros:
Faster than MRIFaster than MRI
Good for abnormalities of bony cortexGood for abnormalities of bony cortex–– ConsCons
Radiation exposureRadiation exposure
Poor soft tissue differentiationPoor soft tissue differentiation–– CT CT myelogrammyelogram
CT plus injection of CT plus injection of intrathecalintrathecal contrastcontrast
Pros:Pros:–– Much better imaging of disk pathologyMuch better imaging of disk pathology
Cons:Cons:–– InvasiveInvasive–– Many contraindications, including all contraindications for lumbMany contraindications, including all contraindications for lumbar ar
puncture and those for IV contrast.puncture and those for IV contrast.

Index Patient: Disk Index Patient: Disk HerniationHerniation on MRIon MRI
49 year-old woman presents for evaluation of low back pain that radiates down to her lower legs.
Disc bulges seen at all lumbar levels.
Classic history is pain that increases with flexion.
Pain with straight leg raise seen on exam.

Index Patient MRI and Index Patient MRI and Normal ComparisonNormal Comparison

Index Patient: Index Patient: OsteophytesOsteophytes and Marrow Changes on and Marrow Changes on
MRIMRI

Companion Patient: Companion Patient: Annular Tear on MRIAnnular Tear on MRI
35 yo male with history of LBP and R sided radiculopathy and groin pain.
Image courtesy of Dr. Rafael Rojas
Radial annular tear seen as hyperintensity at L5/S1

Companion Patient: Disk Companion Patient: Disk Disease on Plain FilmDisease on Plain Film
76-year-old female with a longstanding history of low back pain, and a more recent history of radiating left leg pain provoked by walking.
•Note signs of disk disease:
•Decreased intervertebral height
•Endplate sclerosis
•Osteophyte formation

Common featuresCommon features
Common Common sequelaesequelae of disk disease of disk disease –– HerniationHerniation–– StenosisStenosis–– InstabilityInstability

Index Patient: Spinal Index Patient: Spinal stenosisstenosis on MRIon MRI
•Constriction of canal and foramina commonly caused by:
•Anteriorly•herniated disks
•Posteriorly•enlarged ligamentum flavum•Facet hypertrophy
•Symptoms improve with flexion and worsen with activity (“neurogenic claudication”).
Spinal stenosis:

Index Patient: Spinal Index Patient: Spinal stenosisstenosis on MRI with normal on MRI with normal
comparisoncomparison

Common featuresCommon features
Common Common sequelaesequelae of disk disease of disk disease –– HerniationHerniation–– StenosisStenosis–– InstabilityInstability

Companion Patient: Companion Patient: spondylolysisspondylolysis on plain filmon plain film

Companion Patient: the Scotty Companion Patient: the Scotty dog sign on plain filmdog sign on plain film

Companion Patient: Companion Patient: SpondylolisthesisSpondylolisthesis on Plain Filmon Plain Film
•• SubtypesSubtypes•• DegenerativeDegenerative
•• SubluxationSubluxation at facet at facet jointsjoints
•• Normal or narrow Normal or narrow canalcanal
•• IsthmicIsthmic•• Due to Due to spondylolysisspondylolysis
(seen in (seen in 6% of adults6% of adults
•• Widened canalWidened canal

Companion Patient: Companion Patient: SpondylolisthesisSpondylolisthesis on CTon CT
Reasons to order CT:Reasons to order CT:–– Better for bony cortexBetter for bony cortex–– OsteophytesOsteophytes–– TraumaTrauma–– MRI contraindicationsMRI contraindications
68 year old man with LBP after a fall
Anterior displacement of L5 on S1

Index Patient: Instability on Index Patient: Instability on plain filmplain film
•Leftward listhesis
•Disk space narrowing
•Due to ligament laxity and degenerative joint disease

Clinical OutcomesClinical Outcomes
So you see degenerative disk disease on imagingSo you see degenerative disk disease on imaging……now now what?what?
–– Studies have found 25Studies have found 25--64% of asymptomatic patients 64% of asymptomatic patients have disk have disk herniationsherniations
–– 2/3 of patients with symptomatic disc 2/3 of patients with symptomatic disc herniationherniation have have significant resolution of symptoms at 6 months.significant resolution of symptoms at 6 months.
–– Radiologic findings do not correlate well with surgical Radiologic findings do not correlate well with surgical outcomesoutcomes
–– Surgery may be useful in symptomatic patients with Surgery may be useful in symptomatic patients with signs of nerve root compression or severe canal signs of nerve root compression or severe canal narrowing if conservative therapy has failednarrowing if conservative therapy has failed

Take Home PointsTake Home Points
Imaging not indicated for LBP unless more than 6 weeks have Imaging not indicated for LBP unless more than 6 weeks have past or a past or a red flagred flag is present in the historyis present in the history
Imaging of choice for DDD is Imaging of choice for DDD is nonnon--contrast MRIcontrast MRI
Common complications of DDD include disk Common complications of DDD include disk herniationherniation, spinal , spinal stenosisstenosis, and joint instability, and joint instability
Imaging findings do Imaging findings do notnot correlate well with symptom severity correlate well with symptom severity or surgical outcomeor surgical outcome
In the majority of cases, conservative management will lead to In the majority of cases, conservative management will lead to significant resolution of symptomssignificant resolution of symptoms

ReferencesReferences
Davis PC, Davis PC, WippoldWippold
FJ II, FJ II, BrunbergBrunberg
JA, Cornelius RS, De La Paz RL, JA, Cornelius RS, De La Paz RL, DormontDormont
D, Gray L, Jordan JE, D, Gray L, Jordan JE,
MukherjiMukherji
SK, SK, SeidenwurmSeidenwurm
DJ, DJ, TurskiTurski
PA, Zimmerman RD, Sloan MA, Expert Panel on Neurologic PA, Zimmerman RD, Sloan MA, Expert Panel on Neurologic
Imaging. ACR Appropriateness CriteriaImaging. ACR Appropriateness Criteria®®
low back pain. [online publication]. Reston (VA): low back pain. [online publication]. Reston (VA):
American College of Radiology (ACR); 2008. 7 p.American College of Radiology (ACR); 2008. 7 p.
Fontaine S, Lee D, Maloney W, Fontaine S, Lee D, Maloney W, GrosmanGrosman
H, Wallace C. CAR Standards and Guidelines for H, Wallace C. CAR Standards and Guidelines for
MyelographyMyelography. [Online Publication]. . [Online Publication]. Ottawa(OntarioOttawa(Ontario): Canadian Association of ): Canadian Association of
Radiologists (CAR); 2002. 7p. Radiologists (CAR); 2002. 7p.
DeyoDeyo
RA and Weinstein JN.RA and Weinstein JN.
Low Back Pain. N Low Back Pain. N EnglEngl
J Med 2001 Feb 1;344(5):363J Med 2001 Feb 1;344(5):363‐‐70.70.
Freund, M and Sartor, K. Degenerative Spine Disorders in the ConFreund, M and Sartor, K. Degenerative Spine Disorders in the Context of Clinical Findings. European text of Clinical Findings. European
Journal of Radiology 2006 Apr; 58(1):15Journal of Radiology 2006 Apr; 58(1):15‐‐26.26.
Ginsberg Lawrence E, "Chapter 13. Imaging of the Spine" (ChapterGinsberg Lawrence E, "Chapter 13. Imaging of the Spine" (Chapter). Chen MYM, Pope TL, Jr., ). Chen MYM, Pope TL, Jr., OttOtt DJ: Basic Radiology: http://www.accessmedicine.com.ezpDJ: Basic Radiology: http://www.accessmedicine.com.ezp-- prod1.hul.harvard.edu/content.aspx?aID=2271105. prod1.hul.harvard.edu/content.aspx?aID=2271105.
ModicModic, MT and Ross, JS. Lumbar Degenerative Disk Disease. Radiology 2, MT and Ross, JS. Lumbar Degenerative Disk Disease. Radiology 2007 Oct;245(1):43007 Oct;245(1):43‐‐57.57.

AcknowledgmentsAcknowledgments
Dr. Gillian LiebermanDr. Gillian Lieberman
Maria Maria LevantakisLevantakis
Dr. Rafael RojasDr. Rafael Rojas
Dr. Jay Dr. Jay PahadePahade