Embed Size (px)
Citation preview

Original Research Article
Indian Journal of Orthopaedics Surgery 2016;2(1):52-63 52
Evaluation of Degenerative Lumbar Disc Surgeries
Anubhav Sharma1, Pradeep K Singh2, Sohael M Khan3,*,
Shounak Taywade4, Ankit Chintawar5, Sparsh Naik6
1,4,5,6Junior Resident, 2Professor and Head, 3Assistant Professor, Dept. of Orthopaedics,
Jawaharlal Nehru Medical College, Wardha, Maharashtra, India
*Corresponding Author: E-mail: [email protected]
Abstract Background: Back pain has been known since the start of written history, probably the first report of back pain and sciatica can
be found in an ancient text, the so-called Edwin Smith Surgical Papyrus presumably written around 1550 B.C.1 Although
backache (with or without sciatica) is a benign often self -limiting condition (Macnab). 2 The cost of both time lost from work
(with loss of productivity) and medical care, as well as the cost of litigation and disability claims, make back pain an industry
unto itself.
Purpose: The main purpose of this study was to evaluate the clinical, radiological outcome of the lumbar disc patients managed
surgically and to compare the results of different surgeries performed.
Methods: This study was prospective, non-randomized, cohort study it was carried out in the Department of Orthopaedics,
Acharya Vinoba Bhave Rural Hospital, Wardha, between August 2013 – 2015. Patients with more than 18 years were included
with persistent bothersome sciatic pain, despite conservative management for a period of 6-12 weeks. All the patients with
progressive neurological involvement during a period of conservative treatment. All the patients with cauda equina syndrome or
impending cauda equina syndrome.
Results: Out of total 67 patients the mean age was 49.85±8.75 years ranging from 40 to 72 years. Male gender was
predominantly forming 66% of the sample size whereas 34% of females. All the patients had radicular pain, 26 out of 67 patients
had left sided radiculopathy and right-sided radiculopathy was observed in 21 patients whereas 20 patients had bilateral
radiculopathy. After MRI 34 patients had extrusion of disc, whereas 17 patients showed sequestrated disc, protrusion of disc was
observed in 12 patients, whereas disc bulge was observed in 4 patients. 42% of patients were operated by laminectomy, 33 %
patients were operated by microscopic discectomy and minimum 25% of patients were operated with microendoscopic
discectomy. L4-L5 level was the most common level to get involved. Mean Pre-operative VAS score for male patients was 6.64
and female patients was 6.78, which was reduced to 3.14 and 3.48 respectively after 6 months of operative management. Mean
Pre-operative Oswestery score for male patients was observed to be 44.05 and female patients was 44.87, which was reduced to 24.95
and 27.83 respectively after 6 months of operative management. Complications in all three surgeries were observed.
Conclusion: Minimally invasive techniques in all areas of surgery have gained momentum in recent years. Spinal surgery has
been no exception. Unfortunately, minimally invasive techniques have often been equated with minimally effective procedures.
We understand that the micro endoscopic discectomy and microscopic discectomy techniques are superior to the standard
discectomy technique for the treatment of single level lumbar disc herniation’s with regard to pain relief, clinical outcome and
functional outcome, volume of blood loss, systemic repercussions, and duration of hospital stay. However, technical expertise
and learning curve of the technique could be the limitation. Minimally invasive surgeries are cost-effective treatment for lumbar
herniated discs. Results and complications were comparable with those associated with standard discectomy techniques. Patient
satisfaction was high, and a cost savings was realized.
Keywords: Degenerative, Lumbar Spine, Disc Surgeries, Microscopic Discectomy, Laminectomy, Decompression
Access this article online
Quick
Response Code:
Website:
www.innovativepublication.c
om
DOI: 10.5958/2395-1362.2016.00009.8
Introduction
The first published report of lumbar disc herniation
with radiculopathy was written by Mixter and Barr in
1934. Surgical treatment was not widespread until the
1950s. Today, lumbar discectomy is one of the most
commonly performed elective operations. Lumbar disc
disease accounts for a large amount of lost productivity
in the workforce in the Indian population. Although
most people experience back pain during their lifetime,
only a fraction experience lumbar radiculopathy or
sciatica as a consequence of root compression or
irritation. Almost 5% of males and 2.5% of females
experience sciatica at some time in their lifetime.
In the industrialized countries, back pain today is
the second most common reason for seeking medical
care.3 Everybody belonging to this group of
‘BACKPAIN’ wants an answer to their sufferings and
in process the Governments health care budget’s share
for backache goes up to billions per year and increasing
year after year. The economic burden of spinal
disorders includes:
1) Direct - concern medical expenditure

Anubhav Sharma et al. Evaluation of Degenerative Lumbar Disc Surgeries
Indian Journal of Orthopaedics Surgery 2016;2(1):52-63 53
2) Indirect - consist of lost work output attributable
to a reduced capacity for activity, and result from
lost productivity.
3) Intangible costs are the most difficult to estimate.
Intangible costs include psychosocial burdens
resulting in reduced quality of life, such as job
stress, economic stress, family stress, and
suffering. The direct and indirect costs are
considerable and their management utilizes a
significant part of the gross national product of
many countries. However, back pain has a severe
impact on the individual, families, and society. 4
When a fragment of nucleus herniates, it irritates
and/or compresses the adjacent nerve root. This can
cause the pain syndrome known as sciatica and, in
severe cases, dysfunction of the nerve.
Most lumbar disc herniation’s (lumbar disc
diseases) are preceded by bouts of varying degrees and
duration of back pain. In many cases, an inciting event
cannot be identified. Pain eventually radiates into the
leg. It may be characterized as achy, burning, or similar
to an electrical shock and is often described as a
shooting or stabbing pain. The distribution of the leg
pain is somewhat dependent on the level of nerve root
irritation.
On examination, patients may be neurologically
normal, may have a profound radiculopathy, or may
even demonstrate a cauda-equina syndrome. A positive
straight-leg raising sign is almost always present.
However, a crossed straight-leg raising sign may be
even more predictive of a lumbar disc herniation
(lumbar disc disease). A disc herniation (lumbar disc
disease) most frequently irritates the displaced nerve
root.
Aim & Objective The aim of the study was to evaluate clinical,
functional and radiological outcome of lumbar disc
surgeries and to compare the results of different
surgeries performed for lumbar disc.
Method and Material The present study was carried out in the
Department of Orthopaedics, Acharya Vinoba Bhave
Rural Hospital, Wardha, between August 2013 – 2015.
The study design was prospective, non-randomized,
cohort study.
Patients with more than 18 years were included
with persistent bothersome sciatic pain, despite
conservative management for a period of 6-12 weeks.
All the patients with progressive neurological
involvement during a period of conservative treatment.
All the patients with cauda equina syndrome or
impending cauda equina syndrome.
Patients with disc prolapse at more than one level,
operated earlier for the disc pathology, who required
spinal fusion surgeries and patients with associated
vertebral fracture, infective, or neoplastic disease of the
spine were excluded
Observation & Results Out of total 67 patients the mean age was
49.85±8.75 years ranging from 40 to 72 years. The
distribution curve was bell shaped with rounded peak at
fourth decade and tapering ends at extremes of age.
Maximum patients were from fourth decade of life. The
proportion of patients in different age group was
analyzed using chi-square test. Male gender was
predominantly forming 66% of the sample size whereas
34% of females.
The mean age for male patients was found to be
49.84±8.58 years, which was nearly same for the
female patients, mean age 49.87±9.25 years. Minimum
age for female was 40 years and maximum 70 years and
minimum age for male was 40 and maximum 72 years.
All the patients had radicular pain, 26 out of 67 patients
had left sided radiculopathy and right-sided
radiculopathy was observed in 21 patients whereas 20
patients had bilateral radiculopathy.
MRI findings of the patients in the study were
observed, 34 patients had extrusion of disc, whereas 17
patients showed sequestrated disc, protrusion of disc
was observed in 12 patients, whereas disc bulge was
observed in 4 patients. Changes in MRI of the patients
were observed, 39 patients had ligamentum flavum
hypertrophy, whereas 38 patients had facetal
hypertrophy, modic changes were observed in 25
patients and 9 patients showed pars defect without
listhesis.
Maximum 42% of patients were operated by
laminectomy, 33% patients were operated by
microscopic discectomy and minimum 25% of patients
were operated with microendoscopic discectomy. The
Proportion of number of surgeries to type of surgery
was found to be significant.(Chi-square test p=0.001
<0.05).
Most of the surgeries were done in the patients of
age group of fourth decade. 50% of all type of surgeries
was done in fourth decade. Microscopic group had
patients with minimum age of 40 and maximum age of
70. Whereas, microendoscopicscopic group had
youngest patient of age 40 years and eldest 61years.
However the distribution of number of surgeries in
different age group was statistically significant. (chi
square test p=0.0001(p<0.05).
Laminectomy group patients had higher mean age
54.25±9.656 years as compared to microscopic and
micro endoscopic surgery group 46.5±6.940 and
46.95±6.088 years respectively. The mean age of three
groups was compared and the difference was found to
be statistically significant.(Analysis of variance
p=0.01(p<0.05).
When comparison between time period of
symptoms and type of surgery was done it was found
that the patients who had undergone microendoscopic

Anubhav Sharma et al. Evaluation of Degenerative Lumbar Disc Surgeries
Indian Journal of Orthopaedics Surgery 2016;2(1):52-63 54
discectomy had less time between onset of symptoms
and surgery which was 13.94±6.28 months as compared
to microscopic discectomy which was 19.36±12.11
months and for standard laminectomy it was
24.14±12.80 months. The difference was found to be
significant. (one way ANOVA test p=0.016 p<0.05).
L4-L5 level was the most common level to get
involved and accounted for 72% of total single level
surgeries. L5-S1 accounted for 25% of total surgeries
whereas L3-L4 level surgeries accounted for only 3%
of total patients. However, the distribution was found to
be significant. (chi- square test p=0.025; p<0.05).
The mean VAS scores of pre-operative, post-
operative and 6 months follow up VAS scores were
compared, there was significant reduction in the
postoperative VAS scores in all three surgeries and the
reduction in mean VAS score was maximum in
microendoscopic discectomy by 4.18, followed by
microscopic discectomy by 3.37 and laminectomy by
3.04. However, the difference was found significant.
(One way ANOVA test p=0.0001(p<0.05).
The mean oswestery scores for pre-operative, post-
operative and 6 months follow up were compared.
Maximum reduction in mean Oswestery score was
found in microendoscopic discectomy by 22.71, for
microscopic discectomy score reduced by 17.45 and
minimum reduction in mean Oswestery score was
found in standard laminectomy by 16.50. However, the
difference was found significant in all the thre
surgeries. (one way ANOVA p=0.0001 p<0.05).
The mean hospital stay for microendoscopic
discectomy was 1.82±0.72 days, for laminectomy group
patients was 6.46±2.15 days, whereas for microscopic
discectomy hospital stay was 4.23±0.75 days. The mean
hospital stay in all three surgeries was compared. The
difference was statistically significant (one way
ANOVA test p=0.016 (p<0.05).
A Complications in all three surgeries were
observed, laminectomy had maximum number of
complications, 6 patients did not had pain relief, dural
tear was observed in 3 patients, however 3 patients had
superficial surgical site infections, discitis was observed
in 2 patients, however 1 patient had reherniation.
Whereas, only 2 patients did not have pain relief after
microscopic surgery, superficial infection was observed
in 1 patient, however 1 patient had discitis and
reherniation was observed in 1 patient. However, only 1
patient did not relieve of pain after microendoscopic
discectomy.
Table 1: Age description
Statistics
Age
Number of patients 67
Mean 49.85
Std. Error of Mean 1.069
Std. Deviation 8.751
Variance 76.583
Range 32
Minimum 40
Maximum 72
Graph 1: shows distribution of age

Anubhav Sharma et al. Evaluation of Degenerative Lumbar Disc Surgeries
Indian Journal of Orthopaedics Surgery 2016;2(1):52-63 55
Table 2: Shows Gender Wise Distribution According to Mean Age
Group Statistics p value
Gender Number of
patients Mean
Std.
Deviation
Std. Error
Mean
.990
(p>0.05) Age Male 44 49.84 8.586 1.294
Female 23 49.87 9.255 1.930
Graph 2: Shows Distribution of Radicular Symptoms
Table 3: Distribution of patients according to stages of herniated disc
Herniated Disc
Frequency Percent
Disc Bulge 4 6
Protrusion of Disc 12 18
Extrusion of Disc 34 51
Sequestrated Disc 17 25
Total 67 100
Graph 3: Changes in MRI
BILATERAL30%
LEFT39%
RIGHT31%
0
5
10
15
20
25
30
35
40
Ligamentum
Flavum
Hypertrophy
Facetal
Hypertrophy
Modic Changes Pars Defect
39 38
25
9

Anubhav Sharma et al. Evaluation of Degenerative Lumbar Disc Surgeries
Indian Journal of Orthopaedics Surgery 2016;2(1):52-63 56
Table 4: Distribution of patients according to types of surgeries
Type of Surgery Number of patients Percentage
Laminectomy 28 42
Microendoscopic discectomy 17 25
Microscopic discectomy 22 33
Total 67 100
Table 5: Correlation between different age group with type of surgeries
Age
group Laminectomy
Microendoscopic
discectomy
Microscopic
Discectomy Total p value
31-40 1 3 3 7
0.0001
41-50 14 9 16 39
51-60 5 4 2 11
61-70 7 1 1 9
71-80 1 0 0 1
Total 28 17 22 67
Graph 4: shows correlation between type of surgery and mean age
Table 5: Distribution of Level of operation among total number of patients
Level of operation Number of patients Percentage
L3-L4 2 3
L4-L5 48 72
L5-S1 17 25
Total 67 100
42
44
46
48
50
52
54
56
Laminectomy Microendoscopic
discectomy
Microscopic
discectomy
54.25
46.94 46.5
Age(mean)

Anubhav Sharma et al. Evaluation of Degenerative Lumbar Disc Surgeries
Indian Journal of Orthopaedics Surgery 2016;2(1):52-63 57
Table 6: Correlation between type of surgery and pre-operative,
post-operative and 6 months follow up VAS Score
Descriptives Number of
patients Mean
Std.
Deviation p value
Pre-operative
VAS
Laminectomy 28 7.36 .678 .000
Microendoscopic discectomy 17 6.18 .728 .000
Microscopic discectomy 22 6.23 .612 .000
Post-operative
VAS
Laminectomy 28 6.57 .959 .000
Microendoscopic discectomy 17 4.65 1.272 .000
Microscopic discectomy 22 5.18 .795 .000
6 months follow
up VAS
Laminectomy 28 4.32 1.090 .000
Microendoscopic discectomy 17 2.00 1.173 .000
Microscopic discectomy 22 2.86 1.082 .000
Graph 5: shows correlation between type of surgery and mean pre-operative,
post-operative and 6 months follow up VAS Scores
Table 7: Correlation between type of surgery and pre-operative,
post-operative and 6 months Oswestery Score Score
Number of
patients Mean
Std.
Deviation p value
pre operative
oswestery score
Laminectomy 28 48.29 4.545 0.0001
Microendoscopic discectomy 17 39.18 4.004 0.0001
Microscopic discectomy 22 43.27 3.120 0.0001
post operative
oswestery score
Laminectomy 28 47.93 10.059 0.0001
Microendoscopic discectomy 17 33.65 5.623 0.0001
Microscopic discectomy 22 38.55 3.912 0.0001
6 months
oswestery score
Laminectomy 28 31.79 11.396 0.0001
Microendoscopic discectomy 17 16.47 7.922 0.0001
Microscopic discectomy 22 25.82 7.195 0.0001
7.36
6.57
4.32
6.18
4.65
2
6.23
5.18
2.86
0
1
2
3
4
5
6
7
8
Pre-Op VAS Score Post-Op VAS Score 6 months VAS Score
Laminectomy Microendoscopic discectomy Microscopic discectomy

Anubhav Sharma et al. Evaluation of Degenerative Lumbar Disc Surgeries
Indian Journal of Orthopaedics Surgery 2016;2(1):52-63 58
Graph 6: Shows correlation between type of surgery and pre-operative,
post-operative and 6 months mean Oswestery Score
Graph 7: Shows correlation between type of surgery and mean of hospital stay
Graph 8: Shows correlation between mean pre-operative and mean 6 months values of VAS and Oswestery
scores
48.29 47.93
31.79
39.18
33.65
16.47
43.2738.55
25.82
0
10
20
30
40
50
60
Pre-Op Oswestery Score Post-Op Oswestery Score 6 months Oswestery Score
Laminectomy Microendoscopic discectomy Microscopic discectomy
0
2
4
6
8
Laminectomy Microendoscopicdiscectomy
Microscopicdiscectomy
6.46
1.82
4.23
Hospital stay(Days)
0
20
40
60
80
100
120
VAS Score Oswestery score FIM Score
6.69
44.33
92.76
3.25
25.94
113.57
Pre-Op Scores 6 Months Scores

Anubhav Sharma et al. Evaluation of Degenerative Lumbar Disc Surgeries
Indian Journal of Orthopaedics Surgery 2016;2(1):52-63 59
Table 8: Distribution of complications among three surgeries
Complications
Pain Not
Relieved
Dural
Tear
Superficial
Infection Discitis Reherniation
Laminectomy 6 3 3 2 1
Microscopic Discectomy 2 0 1 1 1
Microendoscopic
Discectomy 1 0 0 0 0
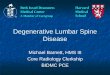
Radiological and Clinical Photograph
CASE 1: Pre-Operative X-ray and MRI
Case 2: Pre Operative X-ray and MRI

Anubhav Sharma et al. Evaluation of Degenerative Lumbar Disc Surgeries
Indian Journal of Orthopaedics Surgery 2016;2(1):52-63 60
Discussion The mean age of our study group was 49.85±8.75
years, which is comparable to other studies. Wang et
al.5, Righesso et al.6 and Mariscalco et al.7 observed
comparable mean age in their study. The explanation to
this can be that, the young- middle age group of
population are the most productive age of the society
and indulge in outdoor activities, which involve heavy
strenuous work.
Age group and gender distribution were correlated
and we observed that male had a mean age of
49.84±8.58 years and female patients had a mean age of
49.87±9.25 years. However the difference was
statistically insignificant.
VAS score is one of the leading indicators for
verifying the effects of interventions. However, low
back pain (LBP) has multiple causes, while sciatica is a
unique symptom of Lumbar disc herniation. So sciatica
could always be relieved after the surgery. Thus,
compared with LBP, the relief of sciatica (leg pain)
would be a more appropriate choice to evaluate the
effects of the surgery.
In present study microendoscopic discectomy
shows maximum reduction of VAS score in comparison
to microscopic and laminectomy surgery which is
comparable to international literature. To support our
study, Ryang et al.8, Tulberg et al.9, had similar findings
for microendoscopic discectomies. Katayama et al.10,
Teli et al.11 observed that patients VAS scores were as
low as normal. Alistair et al.12, Tulberg et al.9 observed
same results from microscopic discectomy. For
laminectomy Alistair et al.14, Fritzell et al.13 observed
comparable results with the present study. Righesso et
al.4 observed zero VAS score value in their both type of
surgical patients.
Turner J A et al.14 performed a study and observed
that success rate in terms of Oswestry Disability Index
of the microendoscopic discectomy was as high as
90%; excellent results were obtained in 80% patients in
microscopic discectomy patients. However, in
laminectomy patients, the success rate was 70% only.
In a historical meta-analysis, the success rate was 64%
only15. Our results in terms of Oswestry Disability
Index were much better as compared with study done
by Iguchi et al16 on traditional open laminectomy, in
which only 56.7% patients obtained good or excellent
results.17
With MED, the bony destruction was limited at the
interlaminar window and most of the facet joints are
preserved. Our study confirmed that MED is a good
surgical option to decompress the herniation while
preserving the intrinsic stability. Ng et al 18 found a
statistically significant increased risk of poor outcome
for Oswestry Disability Index and Low Back Pain
Outcome Score (but not for visual analog scale) if the
duration of sciatica exceeded 12 months prior to
surgery. In our study after 6 months Oswestery score is
16.47 which is comparable to international studies, Ulf
S Nerland et al19, John A et al20.
In the present study the reduction of Oswestry
score was significant for microscopic discectomy too.
Bhavuk Garg et al21 found 6 months follow up
Oswestry score 14.05 which is comparable to our study
25.82±7.19. In microscopic discectomy small incision
and less muscle injury and small fenestration window
accounts for less instability and soft tissue damage with
better healing and early mobilization when compared
with open laminectomy.
Oswestery score for standard laminectomy has
been studied in literature. Sun Zhuoran et al.22 and Ulf
S Nerland et al.23 observed significant reduction in open
Laminectomy, present study shows comparable results
31.79±11.40 with Sun Zhuoran et al.22 and Ulf S
Nerland et al.23, Oswestery score after 6 months.
However, Memduh et al.24 observed after open
laminectomy reduction of oswestery scores was
average. Our results were comparable to Sun Zhuoran
et al 22 and Ulf S Nerland et al23.
In our study 72% of the patients had disc prolapsed
at L4-L5 level which is comparable worldwide with
other studies like Cao Peng et al.9 shows(65%), Bhavuk
Garg et al.21 (75%) found single level pathology at L4-
L5 level. L4-L5 level is most vulnerable for disc
herniation. Pradeep K. Singh et al.25 concludes that the
common level for disc herniation involve L4-L5 of
lumbar spine due to weak inherent property of annulus

Anubhav Sharma et al. Evaluation of Degenerative Lumbar Disc Surgeries
Indian Journal of Orthopaedics Surgery 2016;2(1):52-63 61
fibrosus and posterior longitudinal ligament at L4-L5
level.
As a general rule duration of symptoms was
directly proportional to outcome of surgery. The
patients who had surgery within 12 months of
symptomatology do better. A recent prospective study
by Rihn et al.26 in (Spine Patient Outcomes Research
Trail [SPORT])27 concludes that patient with symptoms
duration of 6 months or less had better outcomes (with
conservative or operative treatment) compared to
patients with symptoms duration of more than 6
months. However, there were significant baseline
differences in the two groups. These differences
included the type of herniation of nucleus pulposus, the
presence of neurological deficit, operative time,
percentage of patients who reported depression,
percentage of patients who perceived that the problem
was getting worse and percentage of patients who had a
preference for surgical treatment. Silverplats et
al.28 found duration of leg pain of <6 months and
duration of sick leave of <2 months was related to
better outcome. Hurme et al.29 found long duration of
preoperative sciatica (more than 2 months) was a
predictor of poor results.
Although there was no randomization but we found
in our present study that the patients who presented
early in 13.94±6.28 months had undergone microscopic
discectomy as compared to microscopic discectomy for
which patients presented in 19.36±12.11 months and
laminectomy for which patients presented in 24.14±
12.80 months.
Duration of hospital stay was primarily dependent
on postoperative mobilization of the patients. We
mobilized our patients as early as 1.82 days (mean) for
the patients who had MED, which was comparable to
many studies whereas for fenestration surgeries and
standard laminectomy it was 4.23 and 6.46 respectively.
Patients were discharged same day after post-op
mobilization.
Data regarding hospital stay were available in eight
studies including Ryang et al8, Tulberg et al.9,
Katayama et al10, Righesso et al6, all reported a
significant difference between the MED and
laminectomy group. The length of hospital stay varies
widely. In different reports the post-operative stay
ranged from 1.1 to 8.5 days30.
In our study we observed that ligamentum flavum
hypertrophy was present in 58% of patients, facetal
hypertrophy in 57%, modic changes in 37% and pars
defect in 13% of patients. Brinjikji W et al.31 concludes
that MR imaging evidence of disc bulge, degeneration,
extrusion, protrusion, Modic changes, and spondy-
lolysis are more prevalent in adults 50 years of age or
younger with back pain compared to asymptomatic
individuals. Takatalo J et al.32 concludes that
herniation’s were most likely in the subjects with recent
onset or persistent (3-yr period) low back symptoms,
when compared in subjects with no symptoms.
This is in keeping with the 1986 statement on the
role of micro discectomy in relation to standard
discectomy in which Hudgins wrote, “My concept of
micro-lumbar discectomy is that it consists of the
ability to do all the surgical maneuvers of standard
partial hemi laminectomy that have stood the test of
time, but through a much smaller incision.” It is
important that the complication rate associated with the
microscopic lumbar discectomy is comparable with that
in standard micro discectomy series. In our current
series there was a 5.9% wound infection rate, a 4.4%
discitis rate, and a 4.4% dural tear rate. These rates
compared favorably with those reported by Williams et
al.33 (0, 0, and 0%, respectively), Ebling et al.34 (3.3,
0.8, and 3.9%, respectively), Caspar, et al35. (0.7, 0.7,
and 6.7%, respectively), and Pappas, et al 36,(7.2, 0.5,
and 1%, respectively).
Our reoperation rate was 3%. This included one
recurrence of disc prolapsed at the same level and same
side, whereas one patient had herniation on
contralateral side of same level and were managed
conservatively. Whereas, one patient developed
refractory backache and required fusion eventually.
The aforementioned authors reported reoperation rates
of 14, 5.5, 5.7, and 3%, respectively.
In our study success rate was very high for all three
surgeries accounting for 92% in total. Whereas,
Williams33, Ebling, et al34, Caspar, et al35, and Findlay
et al37, have reported success rates ranging from 73 to
86%.
SUMMARY
The mean age was 49.85±8.75 years ranging from
40 to 72 years. Maximum patients were from fourth
decade of life. Male gender was predominant. The
mean age for male patients was found to be 49.84±8.58
years. All the patients had radicular pain, 26 out of 67
patients had left sided radiculopathy and right-sided
radiculopathy was observed in 21 patients whereas 20
patients had bilateral radiculopathy. Most of the
surgeries were done in the patients of age group of
fourth decade.
Maximum 42% of patients were operated by
laminectomy, 33 % patients were operated by
microscopic discectomy and minimum 25% of patients
were operated with microendoscopic discectomy.
Laminectomy group patients had higher mean age
54.25±9.656 years as compared to microscopic and
microendoscopic surgery group 46.5±6.940 and
46.95±6.088 years respectively. L4-L5 level was the
most common level to get involved and accounted for
72% of total single level surgeries.
The mean VAS scores of pre-operative, post-
operative and 6 months follow up significantly reduced.
The mean oswestery scores for pre-operative, post-
operative and 6 months follow up were compared and a
significant change was observed. The mean hospital

Anubhav Sharma et al. Evaluation of Degenerative Lumbar Disc Surgeries
Indian Journal of Orthopaedics Surgery 2016;2(1):52-63 62
stay for microendoscopic discectomy was less as
compared to other methods.
Complications in all three surgeries were observed,
laminectomy had maximum number of complications, 6
patients did not had pain relief, dural tear was observed
in 3 patients, however 3 patients had superficial
surgical site infections, discitis was observed in 2
patients, however 1 patient had reherniation. Whereas,
only 2 patients did not have pain relief after
microscopic surgery, superficial infection was observed
in 1 patient, however 1 patient had discitis and 1 patient
had reherniation. However, only 1 patient did not
relieve of pain after micro endoscopic discectomy.
Conclusion Minimally invasive techniques in all areas of
surgery have gained momentum in recent years. Spinal
surgery has been no exception. Unfortunately,
minimally invasive techniques have often been equated
with minimally effective procedures. The procedure
involving tubular instrumentation and technique is an
attempt to allow for a standard familiar microsurgical
discectomy to be performed using standard
microsurgical techniques via a minimally invasive
approach.
We understand that the micro endoscopic
discectomy and microscopic discectomy techniques are
superior to the standard discectomy technique for the
treatment of single level lumbar disc herniation’s with
regard to pain relief, clinical outcome and functional
outcome, volume of blood loss, systemic repercussions,
and duration of hospital stay. However, technical
expertise and learning curve of the technique could be
the limitation.
The advantages of MED over SD include small
incision, better cosmesis, early ambulation, less
postoperative back pain, less blood loss, short hospital
stay, less analgesics, short time to return to work and
thus less cost of treatment.
Conflict of Interest: None
Source of Support: Nil
References: 1. Breasted JH (1930) Edwin Smith Surgical Papyrus, in
Facsimile and Hieroglyphic Transliteration and with
Translation and Commentary, 2 vols. Chicago:
University of Chicago Oriental Publications.
2. Macnab’s Backache fourth edition. (2007)
3. Hoy DG, Bain C, Williams G, March L, Brooks P, Blyth
F, Woolf A, Vos T, Buchbinder R. “A systematic review
of the global prevalence of low back pain.” Arthritis
Rheum. 2012 Jun; 64(6):2028-37.
4. Medline Plus. Back Pain.
http://www.nlm.nih.gov/medlineplus/backpain.html.
Accessed March 11, 2013.
5. Wang HL, Lü FZ, Jiang JY, Ma X, Xia XL, Wang LX
(2011) Minimally invasive lumbar interbody fusion via
MAST quadrant retractor versus open surgery: a
prospective randomized clinical trial. Chin Med J
124:3868–3874.
6. Pool JL. Direct visualization of dorsal nerve roots of the
cauda equine by means of a myeloscope. Arch Neurol
Psychiatr 1938; 39: 1308-1312.
7. Mariscalco MW, Yamashita T, Steinmetz MP,
Krishnaney AA, Lieberman IH, Mroz TE (2011)
Radiation exposure to the surgeon during open lumbar
microdiscectomy and minimally invasive
microdiscectomy: a prospective, controlled trial.Spine
36:255–260.
8. Ryang YM, Oertel MF, Mayfrank L, Gilsbach JM,
Rohde V (2008) Standard open microdiscectomy versus
minimal access trocar microdiscectomy: results of a
prospective randomized study. Neurosurgery 62:174–
181. doi:10.1227/ 01.neu.0000311075.56486.c5,
discussion 181–172.
9. Wang HL, Lü FZ, Jiang JY, Ma X, Xia XL, Wang LX
(2011) Minimally invasive lumbar interbody fusion via
MAST quadrant retractor versus open surgery: a
prospective randomized clinical trial. Chin Med J
124:3868–3874.
10. Brunori A, De Caro GM, Giuffrè R. Ann Ital Chir. 1998
May-Jun;69(3):285-93. PMID:9835099[PubMed -
indexed for MEDLINE]
11. Rawlings CE 3rd, Wilkins RH, Gallis HA, Goldner JL,
Francis R. Postoperative intervertebral disc space
infection. Neurosurgery. 1983; 13(4):371-6.
12. Alistair Daniel Robert Jones • Ahmad Mounir Wafai
Amy Louise Easterbrook Eur Spine J 2014) 23:135–
141 DOI 10.1007/s00586-013-2964-5.
13. Manchikanti L, Singh V, Falco FJE, Cash KA, Pampati
V. Evaluation of the effectiveness of lumbar
interlaminar epidural injections in managing chronic
pain of lumbar disc herniation or radiculitis: A
randomized, double-blind, controlled trial.Pain
Physician 2010; 13:343-355.
14. Turner JA, Ersek M, Herron L, Deyo R (1992) Surgery
forlumbar spinal stenosis. Attempted metaanalysis of the
literature.Spine 17:1–8. doi:10.1097/00007632-
199201000-00001.
15. Turner JA, Ersek M, Herron L, Deyo R (1992) Surgery
forlumbar spinal stenosis. Attempted metaanalysis of the
literature.Spine 17:1–8. doi:10.1097/00007632-
199201000-00001.
16. Iguchi T, Kurihara A, Nakayama J, Sato K, Kurosaka
M,Yamasaki K (2000) Minimum 10-year outcome of
decompressivelaminectomy for degenerative lumbar
spinal stenosis. Spine25:1754–1759.
doi:10.1097/00007632-200007150-00003.
17. Memduh Ka ymaz, Alp Ozgun Borcek, Hakan Emmez,
Emre Durda G, Aydin Pasaoglu Effectiveness of Single
Posterior Decompressive Laminectomy in Symptomatic
Lumbar Spinal Stenosis: A Retrospective StudyGazi
University, Faculty of Medicine, Department of
Neurosurgery, Ankara, Turkey.
18. Ng LC, Predictive value of the duration of sciatica for
lumbar discectomy. A prospective cohort study.Ng LC,
Sell PJ Bone Joint Surg Br. 2004 May; 86(4):546-9.
19. Cao Peng, Chen Zhe, Zheng Yuehuan, Wang Yuren,
Jiang Leisheng, Yang Yaoqi, Zhuang Chengyu
LiangYu,Zheng Tao, Gong Yaocheng, Zhang Xingkai,
Wu Wenjian and Qiu Shijing Comparison of simple
discectomy and instrumented posterior lumbar interbody fusion
for treatment of lumbar disc herniation combined with Modic
endplate changes Chinese Medical Journal 2014;127 (15).
20. John A. Polikandriotis, Elizabeth M. Hudak*, Michael
W. Perry Minimally invasive surgery through

Anubhav Sharma et al. Evaluation of Degenerative Lumbar Disc Surgeries
Indian Journal of Orthopaedics Surgery 2016;2(1):52-63 63
endoscopic laminotomy and foraminotomy for the
treatment of lumbar spinal stenosis. Laser Spine
Institute, 3001 North Rocky Point Drive East, Tampa,
FL 33607, USA.
21. Suk KS, Lee HM, Moon SH, Kim NH (2001) Recurrent
lumbar disc herniation: results of operative
management. Spine 26:672–676.
22. Ulf S Nerland, Asgeir S Jakola, Ole Solheim, Clemens
Weber, Vidar Rao, Greger Lønne, Tore K Solberg,yvind
Salvesen, Sven M Carlsen, ystein P Nygaard, Sasha
Gulati. BMJ 2015;350:h1603 doi:10.1136/bmj.h1603.
23. Cao Peng, Chen Zhe, Zheng Yuehuan, Wang Yuren,
Jiang Leisheng, Yang Yaoqi, Zhuang Chengyu Liang
Yu, Zheng Tao, Gong Yaocheng, Zhang Xingkai, Wu
Wenjian and Qiu Shijing Comparison of simple discectomy
and instrumented posterior lumbar inter body fusion for
treatment of lumbar disc herniation combined with Modic
endplate changes Chinese Medical Journal 2014;127 (15).
24. Memduh Ka ymaz, Alp Ozgun Borcek, Hakan Emmez,
Emre Durda G, Aydin Pasaoglu Effectiveness of Single
Posterior Decompressive Laminectomy in Symptomatic
Lumbar Spinal Stenosis: A Retrospective Study Gazi
University, Faculty of Medicine, Department of
Neurosurgery, Ankara, Turkey.
25. Pradeep K. Singh, Sandeep Shrivastava, Rajesh
Dulani, Pankaj Banode, and Sharad Gupta Dorsal
Herniation of Cauda Equina Due to Sequestrated
Intradural Disc Asian Spine J.2012 Jun;6(2):145–147.
Published online 2012 May
31. doi: 10.4184/asj.2012.6.2.145.
26. Duration of symptoms resulting from lumbar disc
herniation: effect on treatment outcomes: analysis of the
Spine Patient Outcomes Research Trial (SPORT). Rihn
JA, Hilibrand AS, Radcliff K, Kurd M, Lurie J, Blood
E, Albert TJ, Weinstein JNJ Bone Joint Surg Am. 2011
Oct 19; 93(20):1906-14.
27. Duration of symptoms resulting from lumbar disc
herniation: effect on treatment outcomes: analysis of the
Spine Patient Outcomes Research Trial (SPORT). Rihn
JA, Hilibrand AS, Radcliff K, Kurd M, Lurie J, Blood E,
Albert TJ, Weinstein JNJ Bone Joint Surg Am. 2011 Oct
19; 93(20):1906-14.
28. Clinical factors of importance for outcome after lumbar
disc herniation surgery: long-term follow-up. Silverplats
K, Lind B, Zoëga B, Halldin K, Rutberg L, Gellerstedt
M, Brisby H Eur Spine J. 2010.
29. Factors predicting the result of surgery for lumbar
intervertebral disc herniation.Hurme M, Alaranta
HSpine (Phila Pa 1976). 1987 Nov; 12(9):933-8.
30. Xian Chang & Bin Chen & Hai-yin Li & Xiao-bo Han
& Yue Zhou & Chang-qing Li International
Orthopaedics (SICOT) (2014) 38:1225–1234 DOI
10.1007/s00264-014-2331-0.
31. Brinjikji W, Diehn FE, Jarvik JG, Carr CM, Kallmes
DF, Murad MH, Luetmer PH. MRI Findings of Disc
Degeneration are More Prevalent in Adults with Low
Back Pain than in Asymptomatic Controls: A
Systematic Review and Meta-Analysis. AJNR Am J
Neuroradiol. 2015 Sep 10. [Epub ahead of print]
32. Takatalo J, Karppinen J, Niinimäki J, Taimela S,
Mutanen P, Sequeiros RB, Näyhä S, Järvelin
MR,Kyllönen E, Tervonen O. Association of modic
changes, Schmorl's nodes, spondylolytic defects, high-
intensity zone lesions, disc herniations, and radial tears
with low back symptom severity among young Finnish
adults. Spine (Phila Pa 1976). 2012 Jun 15;37(14):1231-
9. doi: 10.1097/BRS.0b013e3182443855.
33. Williams, Koebbe CJ, Maroon JC, Abla A, El-Kadi H,
Bost J Lumbar microdiscectomy: a historical
perspective and current technical considerations.
Neurosurg Focus. 2002 Aug 15;13(2):E3.
34. Saftić R, Grgić M, Ebling B, Splavski B. Case-control
study of risk factors for lumbar intervertebral disc
herniation in Croatian island populations. Croat Med J.
2006 Aug;47(4):593-600.
35. Casper GD, Mullins LL, Hartman VL. Laser-assisted
disc decompression: a clinical trial of the holmium:YAG
laser with side-firing fiber. J Clin Laser Med Surg. 1995
Feb;13(1):27-32.
36. Pappas CT, Harrington T, Sonntag VK. Outcome
analysis in 654 surgically treated lumbar disc
herniations. Neurosurgery. 1992 Jun;30(6):862-6.
37. Chatterjee S, Foy PM, Findlay GF. Report of a
controlled clinical trial comparing automated
percutaneous lumbar discectomy and microdiscectomy
in the treatment of contained lumbar disc herniation.
Spine (Phila Pa 1976). 1995 Mar 15;20(6):734-8.