Embed Size (px)
Citation preview

Original Research
Image Artifacts due to a Time-VaryingContrast Medium Concentrationin 3D Contrast-Enhanced MRA
Jonas Svensson, MSc,1* J. Stefan Petersson, PhD,1 Freddy Ståhlberg, PhD,3
Elna-Marie Larsson, MD, PhD,4 Peter Leander, MD, PhD,2 and Lars E. Olsson, PhD1
The purpose of this work was to study image effects due totime-varying contrast medium concentration in contrast-enhanced three dimensional (3D) magnetic resonance angi-ography (MRA) images. Two different simulation models(1D and 3D) and two different contrast medium variationschemes were used. Phantom measurements were alsoperformed. Experiments were performed for several differ-ent bolus timings. Similar sequence and image objectparameters were used in both simulations and measure-ments (TE/TR 2.1/7.8 mses, flip angle 30°, T1/T2 1200-80/150-40 msec, flow velocity 100 cm/sec). A small variationin bolus timing yielded large variations in the appearanceof the image effects, especially if the center of k-space wassampled in the vicinity of rapid contrast medium concen-tration variation. For a typical bolus injection in a patient,a severe signal loss but only minor ringing and edgeartifacts appeared if the bolus injection was poorly timed.Effects of pulsatile flow were minor. The 3D model provedto be a useful tool in these studies. J. Magn. Reson.Imaging 1999;10:919–928. r 1999 Wiley-Liss, Inc.
Index terms: magnetic resonance; angiography; contrastmedium; artifacts; simulations
THE THREE-DIMENSIONAL (3D) time-of-flight (TOF)MR angiography (MRA) is not readily applicable inimaging of the abdominal and renal vessels. The non-zero acquisition time (TA) leads to ghosting and blurringdue to breathing and peristaltic movement (1). In addi-tion, the 3D volume is often acquired in the coronalview, which leads to blood signal saturation, since thevessels then are oriented ‘‘in-plane’’ (2).
The TOF technique is based on gradient-echo se-quences and the enhancement of signal from inflowingblood to build up vessel contrast. The impact of breath-
ing and peristaltic motion on the images from thesesequences is reduced if the TA is shortened. This isachieved if the TR is shortened, and with the availableMR scanners the TR can be reduced enough to acquire awhole 3D volume in one single breath-hold (3). In thisway, motion artifacts are almost eliminated. Unfortu-nately, the short TR leads to severe blood signal satura-tion, which makes the angiogram unusable. To achievegood vessel contrast even if a short TR is used, aT1-reducing MR contrast medium (CM) can be utilized(4), the so-called contrast-enhanced (CE) MRA tech-nique. The build-up of image contrast using this methodis fundamentally different from that in TOF techniques.The vessel contrast in a CM-enhanced image is basedon T1 effects instead of the inflow effect utilized inTOF (3,5).
The technique, whereby a CM is injected duringimaging with a breath-holding sequence, has beendeveloped over the past few years and is used forimaging of the descending aorta and renal arteries (6–9).
The T1-reducing contrast media on the market todayare made for extracellular use and not for blood pooluse. The CM concentration in the blood thus decreasesrapidly after injection (3,10). Therefore imaging is per-formed during the first pass of the CM bolus in thevolume of interest (10). Furthermore, the CM injectionis timed so that the maximum concentration of CMmatches acquisition of the central lines in k-space(6,7,11). This procedure lead to a varying CM concentra-tion and an undesired MR signal amplitude variationduring acquisition. Such variation may cause aorticsignal loss and artifacts in the phase-encoding directionof the image (8,12–14). Similar signal amplitude modu-lation artifacts appear due to inflow effects from pulsat-ing flow (15,16). T2/T2* decay during acquisition causesthe same effects in turbo spin-echo techniques (17) andechoplanar imaging (18).
Several papers have pointed out the importance ofaccurate injection timing to avoid artifacts (6,7,12,19).However, only a few studies have evaluated the impacton image quality of a time-varying CM concentration(12,13). 1D Simulations of these effects have beenperformed (12). The model used in that work is a strictmathematical model, not related to MR imaging. Simu-
1Department of Radiation Physics, Lund University, Malmo UniversityHospital, SE-205 02 Malmo, Sweden.2Department of Diagnostic Radiology, Lund University, Malmo Univer-sity Hospital, SE-205 02 Malmo, Sweden.3Department of Radiation Physics, Lund University, Lund UniversityHospital, SE-221 85 Lund, Sweden.4Department of Diagnostic Radiology, Lund University, Lund UniversityHospital, SE-221 85 Lund, Sweden.*Address reprint requests to: J.S., Department of Radiation Physics,Lund University, Malmo University Hospital, SE-205 02 Malmo, Swe-den. E-mail: [email protected] August 27, 1998; Accepted July 19, 1999.
JOURNAL OF MAGNETIC RESONANCE IMAGING 10:919–928 (1999)
r 1999 Wiley-Liss, Inc. 919

lations of MR images taking into account effects fromrelaxation, choice of pulse sequence, flow (eg, pulsatil-ity), and 3D acquisition have not been performed. Whenperforming these simulations, it is also important toconsider the signal from surrounding tissue, sincesignal from the vessel might be smeared and sumvectorially with signal from the surroundings. This hasnot been taken into account in previous works. Afurther detailed analysis of the causes of these effectsusing a more sophisticated simulation model wouldyield a more complete understanding of the problem.Since clinical imaging with this technique is performedin 3D, it is of interest to perform simulations in 3D also.The aim of this work was to study the mechanisms ofpossible artifacts appearing in CE 3D MRA images. Inparticular, the effects associated with a time-varyingCM concentration during acquisition are of interest.These artifacts are studied separately as well as incombination with flow-related effects. The usefulness ofa 3D MRI simulation model in performing these studiesis also evaluated.
THEORY
Two different simulation models are used. Model I is onedimensional and is described in this section. A similarmodel was used by Maki et al (12). However, that workdid not take into account signal from vessel surround-ings. Simulations with this model are not related to MRimaging but more to the mathematical aspects of theFourier transform used for image reconstruction.
Model II is a model for simulation of MR images/volumes in 3D using k-space formalism (20,21). MRimages from any general steady-state free precessionsequence can be simulated. Effects of pulsatile through-plane and in-plane flow as well as the effects of adynamic CM distribution are handled. Model II is de-scribed in detail elsewhere (22,23).
3D MR imaging requires two phase-encoding gradi-ents (image and slice). The stepping of these two gradi-ents during acquisition corresponds to two loops in thedesign of the sequence. Each step of the outermost loopis equivalent to a time step (TA divided by the totalnumber of steps in the outermost loop) during imageacquisition.
Assume that we have a coronal 3D image volumecontaining a contrast-enhanced aorta with surround-ing tissue. Let frequency encoding be in the head-feetdirection and the image phase-encoding loop be theoutermost one. The slice phase-encoding loop is theninside the image phase-encoding loop. If the CM concen-tration varies during acquisition, variation during encod-ing of the slice direction will be small compared with thevariation along the image phase direction (due to theloop order and the number of phase-encoding steps).CM variation during readout is negligible since this timeis very short. Thus, the CM concentration variation willonly matter in the image phase-encoding direction (right-left), and the problem of studying CM variation effectscan be reduced to one dimension. The signal matrix, S,(k-space) and the image matrix, M, are a Fourier trans-
form (FT) pair. The FT is a linear operation, and the totalk-space signal is the sum of individual signals fromdifferent tissues (Eq. [1]). Thus, only the signal from theaorta and not from the surrounding tissue has to beconsidered when studying the effects of a CM distribu-tion in k-space:
Maorta 1 Mtissue 5 Mtotal 5 FT 5Stotal6 5 FT 5Saorta 1 Stissue6
5 FT 5Saorta6 1 FT 5Stissue6. (1)
For a spoiled gradient-echo sequence, the steady-statesignal can be calculated using Eq. [2] (24):
S ~(1 2 e2(TR/T1))
1 2 cos (a)e2(TR/T1)sin (a)e2(TE/T2) (2)
where a is the flip angle (FA). From Eq. [2] it is seen thatS is maximal for either a long TR or a short T1. A shortT1 can be achieved by administration of a contrastmedium. Relaxation time reduction and CM concentra-tion are interrelated via Eq. [3a, b] (4).
1
T1after5
1
T1before1 r1 · C
1
T 2after5
1
T 2before1 r2 · C (3a, b)
where r1 and r2 are the relaxivities [mM21 · s21] and C isthe concentration of the CM. The subscripts ‘‘before’’and ‘‘after’’ denote tissue relaxation times before andafter the administration of CM. The current gadolinium(Gd)-based contrast media used in MRA have in vitrorelaxivities of approximately r1/r2 5 4.0/6.0 mM21 · s21
at 1.5 T (10,25). If a CM is distributed during theacquisition, the signal is enhanced according to Eqs. [2]and [3]. The contrast-enhanced line profile is obtainedfrom Eq. [4]:
MaortaCE (x ) 5 FT215SR(t ) · Saorta(kx(t )6 (4)
where SR(t) is the signal ratio between contrast-enhanced and unenhanced blood. Saorta(kx(t )) is ob-tained from an FT of Maorta(x ) (Eq. [1]). Thus, effects of atime-varying CM concentration are easily studied usingEqs. [1] and [4].
MATERIALS AND METHODS
Simulations were performed using models I and II. Theeffects described in the theory section were demon-strated with model I. Model II was used to simulate MRimages with the same effects. Advanced simulationsusing model II and a patient-like model (flow, CMconcentration variation, pulsativity) were performed.Phantom measurements were also performed.
920 Svensson et al.

Simulations
Model I: 1D Simulations
The signal ratio between unenhanced blood and sur-rounding tissue was calculated using Eq. [2] and theparameters T1tissue/T2tissue 300/60 msec (fat), T1aorta/T2aorta 1200/150 msec (unenhanced blood) (26), TE/TR2.1/7.8 msec, flip angle 30°. SR(t) was calculated usingEqs. [2] and [3a, b]. A 3 mM constant concentration ofCM (blood T1/T2 < 80/40 msec) during 10 secondsand zero concentration elsewhere was assumed.
The aorta and tissue signal were stored in two 256-element, 1D vectors, Maorta(x ) and Mtissue(x ). Effects ofCM variation will only affect the aorta vector. The sum ofthe two vectors, M(x ), corresponds to a line profile froman ideal image of an aorta with surrounding fatty tissue.SR(t ) was stored in a separate 256-element vector. M(x )is assumed to come from an image acquired with a 3DMRA sequence, with TA 32 seconds and the outermostphase-encoding loop in the line profile direction. Thus,each vector element in 1D k-space corresponds to a timestep of 32/256 5 0.125 seconds, and the 10 secondbolus will cover 80 elements in SR(t ).
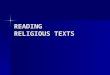
The contrast-enhanced line profile was obtained fromEqs. [1] and [4]. Several different bolus timings weresimulated, but only four of them are presented here(Fig. 1):
a. Centered bolus, starting at element 88 and endingat element 167 in k-space.
b. Bolus arrives in the vessel 4 seconds later than ina, starting at element 120.
c. Bolus arrives 5 seconds later than in a, starting atelement 128. No enhancement of the first half ofk-space.
d. Bolus arrives 6 seconds later than in a, starting atelement 136 in k-space; the central parts of k-space are not covered by this bolus.
The importance of taking into account the surroundingtissue was studied with simulations of a 5.5 second latebolus with and without the fatty tissue.
All model I simulations were performed using IDLsoftware (Research Systems, Boulder, CO) on an Intel-based MS Windows NT 4.0 workstation.
Model II: 3D Simulations
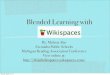
A computer program developed at our department, theMRI Simulator (27), was used to perform simulations in3D. The program simulates MR images from any generalsteady-state free precession sequence. The sequence aswell as the imaging object is constructed within theprogram by the user. A spoiled 3D gradient-echo se-quence, similar to the one used in the phantom measure-ments below (differing only in resolution and number ofslices), was implemented (TE/TR 2.1/7.8 msec, flipangle 30°, matrix size 256 3 256 3 16). The TA for sucha sequence would be 32 seconds. An abdominal objectwas created with a central circular aorta (T1/T2 1200/150 msec, steady flow velocity 1.0 m/sec) surroundedby stationary fatty tissue (T1/T2 300/60 msec). Foursimulations with the same bolus timings and bolusshape as for model I were performed. In these simula-tions, the flow was turned off, to imitate model I. Therest of the simulations were performed using typicalblood and CM dynamics from the descending aorta. Thepulsatile flow velocity function was a positive 0.4 secondlong lobe with a peak velocity of 100 cm/sec. The periodwas 1.2 seconds. The CM concentration data were takenfrom Fritz-Hansen et al (28) and correspond to a 0.1mmol/kg bolus injected in less than 10 seconds. Peakconcentration lasts approximately 7 seconds. Forty-onesimulations with different bolus timings were carriedout. The timing was varied in 1 second steps imitatingpeak CM concentration at times from 20 seconds beforeacquisition of the k-space center to 20 seconds after, forexample (Fig. 2):
a. Peak concentration 13 seconds before k-spacecenter.
b. Peak concentration centered in k-space.c. Peak concentration 13 seconds after k-space cen-
ter.d. Peak concentration 15 seconds after k-space cen-
ter.
A 13 second late bolus starts just before acquisition ofthe k-space center. If the bolus is 15 seconds late, it willstart just after acquisition of the central lines in k-space. The 13 second early bolus was simulated toreveal possible differences between equally displacedearly and late boluses. The images containing the center
Figure 1. Relative signal enhancement, SR(t ), for the fourdifferent bolus timings used in simulations with model I (andmodel II). An ideal 10 second long bolus shape is used.Maximum concentration is 3 mM (yields blood T1/T2 78/40and a ninefold signal enhancement). k-Space center is sampledafter half the acquisition time (sequential technique) with a TAof 32 seconds assumed. a: Bolus centered in k-space. b–d: Bolusarrives 4, 5, and 6 seconds later than in a, respectively.
Image Artifacts in 3D CE MRA 921

of the aorta (no. 8 of 16) were evaluated with line profilesaveraged over column 180–190.
Two simulations were carried out to study the effect ofpulsatile flow. One of them was performed with pulsa-tile flow and one with steady flow. Peak CM concentra-tion was timed to the center of k-space.
An Intel-based MS Windows NT 4.0 workstation wasused for the simulations.
Phantom Measurement
Flow measurements were performed on a MagnetomVision 1.5 T MR system (Siemens, Erlangen, Germany).A flow phantom consisting of two plastic pipes inside aplastic cylinder filled with doped water was used. Thepipe used for the measurements had an inner diameterof 2 cm and soft PVC tubes connected at each end. ThePVC tubes were connected to a flow inlet container anda flow outlet container. The fluid was regular tap waterdoped to blood T1 < 1200 msec using Gd31 (GdCl3).Steady, nonpulsatile flow through the phantom wasestablished with the help of a height difference betweenthe inlet and outlet hoses. Flow velocity was determinedto 105 cm/sec using the flow quantification packageavailable at the scanner.
During every image acquisition a bolus of 45 ml 50mM Gd31 solution was injected manually into the flowsystem (injection time 11 seconds). The CM bolus dy-namics on its way through the phantom was deter-mined using a turbo fast low-angle shot (FLASH) se-quence (tfl_t1_1b488 · ykc, TI/TE/TR 300/1.4/3.3msec). The sequence was able to deliver 60 transversalimages with a temporal resolution of 1 second. Theseimages were evaluated with a circular region of interest(ROI) over the flow area of the image, and the signal
mean was plotted versus image number. The samesequence is used clinically when determining the bolustravel time from injection to volume of interest.
3D CE MRA experiments were performed for twodifferent bolus timings using a 3D spoiled gradient-echosequence (fi3d_2b195.ykc, TE/TR 2.1/7.8 msec, flipangle 30°, field of view (FOV) 30 3 40 cm, matrix192 3 512, 26 slices). TA was 41 seconds, and imageswere obtained in the coronal view with the image phaseencoding in the right-left direction. This sequence isused clinically for breath-hold 3D CE MRA of theabdominal aorta.
RESULTS
Simulations
Ideal Bolus Shape
The results from models I and II simulations of an idealbolus shape agree very well (Fig. 3). Thus model II can beused to simulate MR images containing effects from avarying contrast medium concentration.
Although there is only 1 second in timing differencebetween b, c, and d in Fig. 3, the difference in shapebetween the three line profiles is large. In Fig. 3b, aringing artifact appears. In Fig. 3c, there is no ringing,but edge enhancement and signal loss are seen. Thus,the line profile shapes are highly sensitive even to minortiming variation.
As expected, best aortic enhancement is achievedwhen the bolus is centered (Fig. 3a). A 4 second latebolus also has a high aortic signal, but the vessel shapeis not as well defined. If the bolus misses the center ofk-space completely, there is no enhancement (Fig. 3d).
Ringing and/or edge enhancement artifacts appear inall cases, the effects being more pronounced the moredisplaced the bolus is.
The signal from the ‘‘smeared’’ vessel adds vectoriallywith any signal from the surrounding tissue. If thesurroundings are not taken into account in the calcula-tions, this vector summation does not occur, and theresulting effects can appear totally different (Fig. 4). Inthis example, large ringing artifacts occur if there is aninitial signal in the surroundings. If the same calcula-tions are performed without the surrounding signal,these artifacts are not seen. Thus it is important toconsider signal from the surrounding tissue in thesimulations.
Typical Blood and CM Dynamics
All the line profiles from the simulations of variousbolus timings are plotted consecutively in Fig. 5. Theprofile numbered zero is from the simulation with acentered bolus, and increasing numbers correspond tolater injections. The thick profiles are extracted inFig. 6.
A small difference in timing yields large differences inthe resulting line profiles if the center of k-space issampled during the rapid CM concentration increase(Fig. 6c,d). The signal loss is not symmetrical in thesense that an early bolus does not yield the same effects
Figure 2. Timing of the CM concentration curve, used inpatient-like bolus dynamics simulations with model II; TA of 32seconds. Maximum CM concentration is 2.7 mM (yields bloodT1/T2 86/44) and lasts 7 seconds. a: Peak CM concentrationarrives 13 seconds early (compared with a centered bolus).b: Centered in k-space. c: 13 seconds late. d: 15 seconds late.
922 Svensson et al.

as a late bolus, even if they are equally displaced (Fig.6a,c). This effect is a result of how the CM concentrationvaries during acquisition. Some CM remains in thevessel long after peak concentration (Fig. 2). Eventhough that concentration is low, it will still contribute
to signal enhancement. Therefore contrast enhance-ment is more effective for an early bolus, since it coversmore of k-space than a late bolus.
The artifacts seen in the simulations with an idealbolus are not present here. This is due to the slowerincrease/decrease in CM concentration when a pa-tient’s bolus dynamics are assumed. Thus, the more
Figure 3. Line profiles from simulations using model I (thin lines) and model II (thick dashed lines) in conjunction with an idealbolus (Fig. 1). Thick continuous lines correspond to the unenhanced aorta. a: Bolus centered in k-space. b–d: Bolus arrives 4, 5,and 6 seconds later than in a, respectively.
Figure 4. Simulations showing the importance of taking intoaccount the surrounding tissue. The dashed line shows resultsfrom a simulation without surrounding tissue, and the continu-ous line is the corresponding simulation when the surroundingtissue is considered. The artifacts in the two cases appeartotally different.
Figure 5. Line profiles from simulations with model II plottedconsecutively for different bolus timings. A patient-like concen-tration curve (Fig. 2) has been used. Increasing profile numbercorresponds to later injection. The thick profiles are extractedin Fig. 6.
Image Artifacts in 3D CE MRA 923

rapid the CM concentration variation, the higher therisk for artifacts, especially if this rapid variation occursin the vessel during sampling of the central lines ink-space.
The vessel signal strength reflects the concentrationof CM in the vessel during sampling of the central linesin k-space (Fig. 6b). If maximal vessel signal is to beachieved, the central lines in k-space must be sampledduring peak concentration. With the bolus shape usedin these simulations, peak concentration lasts 7 sec-onds. A displaced bolus yields lower aortic signal (55%,in Fig. 6a, 47% in Fig. 6c, and 29% in Fig. 6d) comparedwith aortic signal with a centered bolus (Fig. 6b). Amodest edge enhancement is also seen in the displacedbolus cases. Some ‘‘ghost vessels’’ are visible in theimage from the simulation with pulsatile flow (Fig. 7a;see also the line profiles in Fig. 6). These artifacts are notpresent when steady flow is used (Fig. 7b). However, theartifacts are only pronounced to the left in the image,where the inflow effects lead to a stronger vessel signal.In a clinical situation these inflow effects (and thus thepronounced pulsatile artifacts) would not be visiblesince the coil excites a volume that is larger than theFOV. Hence the influence of pulsatile flow in CE 3D MRAis only of minor importance.
Measurements
Injection of the CM during the turbo FLASH acquisitionresulted in a bolus shape in the phantom similar to theone used in simulations of an ideal bolus (Fig. 8).Injection was performed with the same rate and CMvolume during the angiographic measurements as well.It is therefore likely that the bolus shape was the samein those measurements. Visual evaluation of the imagesfrom the angiographic measurements confirms the re-sults of the simulations qualitatively. Centering thebolus in k-space yields the best vessel contrast (Fig. 9a).The image acquired with an early bolus contains signalloss and artifacts (Fig. 9b).
DISCUSSION
The breath-hold CE 3D MRA technique has been devel-oped over the past few years; many authors havepointed out the importance of proper bolus timing(6,7,12,19). However, studies investigating the proper-ties of effects due to inaccurate bolus timing (12,13) arerare. The 3D model (model II) used in this work proved tobe valuable in performing such studies. The simulated
Figure 6. Line profiles extracted from Fig. 5. The thick line is the line profile from contrast-enhanced images, and the thinlines are from unenhanced images. a: Peak CM concentration arrives 13 seconds early (compared with a centered bolus). b:Centered in k-space. c: 13 seconds late. d: 15 seconds late. The small artifacts seen in the ‘‘tissue’’ are due to pulsatile flow; seealso Fig. 7.
924 Svensson et al.

sequence and object parameters are easily modified toobtain different criteria of interest.
The results from simulations with an ideal bolususing models I and II agree very well, implying that theartifacts appearing in the two models when simulatingan ideal bolus have the same origin. Model I considersonly signal modulation in Fourier space and has nodirect relation to MRI or blood flow. Model II simulates3D MRI images, taking into account a varying contrastmedium concentration during acquisition. The varying
CM concentration modulates the MR signal. The arti-facts appearing in the 3D model simulations of an idealbolus must therefore have their origin solely in thek-space signal modulation.
Signal loss is present when the patient-like bolus isnot centered in k-space. However, the only artifactspresent (except for some minor edge enhancement) aresome low intensity ‘‘ghost vessels’’ due to pulsatility (seebelow). Thus the risk of image artifacts due to a varyingCM concentration seems to be low, even if the bolusinjection is very poorly timed. However, even if the riskfor artifacts is low, the timing of the bolus is of greatimportance to achieve good vessel contrast.
A previous study has reported the appearance ofartifacts in simulations with CM bolus dynamics similarto the ones used here (12). These results showed severeartifacts when the authors simulated a centric acquisi-tion order. Centric acquisition is more sensitive to bolusdisplacement than sequential acquisition (see below)and means that the sequence starts with acquisition ofthe central k-space lines and continues with the distant(less important) k-space lines (29,30). Previous work didnot take into account surrounding tissue, which maycause the resulting artifacts to appear differently. Theirsimulations also assumed a longer TA (45 seconds), andso their peak CM concentration covers a smaller part ofk-space. Another important parameter to consider ishow rapidly the CM increases to peak concentration. Animmediate enhancement (Fig. 3, ideal bolus) causesmore artifacts than a gradual CM concentration in-crease (Fig. 6, patient bolus). It is possible that Maki etal (12) used CM dynamics with a more rapid initial CMconcentration increase than the one used here.
Acquisition of the center of k-space in the vicinity ofrapid CM increase can result in images with severeartifacts (ideal bolus simulations). The same results
Figure 7. Image no. 8 of 16 in simulations using pulsatile (a) and steady (b) flow. The pulsatile flow generates artifacts. However,they are only pronounced on the left-hand side, where inflow effect gives a stronger vessel signal.
Figure 8. Phantom measurements. Evaluation of images ac-quired using the turbo FLASH sequence. Signal from an ROIwithin the ‘‘vessel’’ is plotted versus image number. Timebetween images equals 1 second. The signal enhancement for11 seconds is seen during passage of the 45-ml Gd bolus.
Image Artifacts in 3D CE MRA 925

have been reported in patient examinations (14). Suchacquisition also makes the line profile shape very sensi-tive to even minor timing variations. The difference intiming between Fig. 3b, c, and d is only 1 second in eachcase but the corresponding line profile shapes varygreatly.
Some CM remains in the vessel long after peakconcentration (Fig. 2) and results in more effectivecontrast enhancement for an early bolus than for a latebolus (Fig. 6). Earlier studies have reached the sameresults (12). The remaining CM concentration after thepeak is rather low, but it still contributes to signalenhancement. For an early bolus, peak concentrationappears before the k-space center and there is CM left inthe vessel throughout the rest of the acquisition. A latebolus leaves the whole first part of k-space withoutcontrast enhancement. The fact that rapid CM concen-tration variation near the k-space center can causeartifacts also makes early injection preferable. Thecentric encoding scheme is even more sensitive to theseeffects (12,29). Furthermore, a late bolus injection willresult in increased venous enhancement, which compli-cates evaluation of the angiogram (7,31).
The blood flow in the aorta is pulsatile, and it is wellknown that a pulsatile blood flow can result in imageartifacts (16). However, earlier studies have not reportedany problems with aortic pulsatile flow in CE tech-niques, and the simulations performed here indicatethat the problems with pulsatility should be of minorimportance. Only low-intensity ghost artifacts are vis-ible even when the vessel is greatly enhanced.
The phantom measurements confirm the bolus dis-placement signal loss seen in the simulations qualita-tively. Furthermore, the images from the experimentwith a displaced bolus contain artifacts, which probablyare a result of rapid CM variation during acquisition of
the k-space center. A further reason for the poor imagequality may be the injection technique used. The CMwas injected approximately 4 m from the imaging vol-ume. Considering the large pipe diameter and the highflow velocity, it is possible that the CM concentrationover a cross section of the pipe in the volume of interestwas not homogeneous.
Even though the 3D simulation model used simulatesMR images of a 3D volume taking into account in-planepulsatile flow, several aspects of breath-hold CE 3DMRA are not considered, for example, incomplete breath-holding and different k-space sampling trajectories.Patients undergoing to breath-hold CE 3D MRA areoften in poor condition and may have trouble holdingtheir breath throughout a whole acquisition (approxi-mately 30 seconds). Maki et al (32) showed that if thepatient breathes during more than 50% of the acquisi-tion, noticeable artifacts may appear in the images. Thisis especially true if the central parts of k-space aresampled during non-breath-hold. In this work a sequen-tial k-space acquisition is assumed. If a centric acquisi-tion technique is used instead, the problems associatedwith partial breath-holding can be reduced (14,32). Theimportant central k-space lines are then sampled at thebeginning of the acquisition and if breathing occurs inthe middle or at the end of the sequence, it will onlyaffect the higher (less important) spatial frequencies.
The methodology of breath-hold 3D CE MRA is con-tinuously being developed, and improvements are beingmade in sequences as well as in bolus timing tech-niques. The main goal of sequence improvement is toshorten the scan time without a decrease in imagequality. A shorter scan time will result in a shorterbreath-holding time for the patient, more uniform CMcoverage of k-space, and a reduced risk of venousenhancement. Thus, a shorter scan time will reduce the
Figure 9. Images from contrast-enhanced 3D MRA phantom experiments. a: Bolus centered in k-space. b: Early bolus.
926 Svensson et al.

risk of image artifacts. One way to achieve this is toreduce the number of phase/slice-encoding steps andfill in the missing k-space data using either zero-filling(33) or calculated (interpolated) data (34). It is alsoimportant to measure the bolus travel time accuratelyfrom injection to arrival in the vessel of interest, to avoidpoor vessel enhancement and artifacts. An accurate buttime-consuming technique for this is to use a small testbolus of CM and a sequence capable of producingimages at a rapid rate (7,9,19). New bolus timing tech-niques instead utilize, eg, automated detection (14,35)or fluoroscopic imaging (30) to measure the arrival ofthe bolus in the imaging volume. These new techniquesseem promising and may be capable of reducing the riskof artifacts and signal loss due to improper timing.
New contrast media, so-called blood pool agents, havea long intravascular half-life and minimal leakage to theextracellular space (3). With such a CM, imaging duringthe first pass of the bolus will no longer be necessary,and the artifacts discussed here will no longer be aproblem. However, the veins and arteries will be equallyenhanced if imaging is performed after vascular CMequilibrium is reached. This may result in new prob-lems, eg, with separation of veins from arteries in theangiograms.
CONCLUSIONS
The timing of the bolus is of great importance, to achievegood vessel contrast. A small variation in bolus timingcan yield large variations in the appearance of the vesselif the center of k-space is sampled during a rapid CMconcentration variation. If the CM concentration varia-tion is extremely rapid, artifacts may arise. However, therisk of image artifacts due to a varying CM concentra-tion in CE 3D MRA seems to be rather low. Effects ofpulsatility do not seem to degrade the image qualityconsiderably. The 3D model used here is capable ofhandling effects of flow, pulsatility, and CM concentra-tion variation simultaneously and is therefore a usefultool for performing such studies.
REFERENCES1. Masaryk TJ, Lewin JS, Laub G. Magnetic resonance angiography.
In: Stark DD, Bradely WG, editors. Magnetic resonance imaging,vol. 1. St Louis, MO: Mosby-Year Book; 1992. p 327.
2. Yano T, Kodama T, Suzuki Y, Watanabe K. Gadolinium-enhanced3D time-of-flight MR angiography. Experimental and clinical evalu-ation. Acta Radiol 1997;38:47–54.
3. Maki JH, Chenevert TL, Prince MR. Three-dimensional contrast-enhanced MR angiography. Top Magn Reson Imaging 1996;8:322–344.
4. Hendrick RE, Haacke EM. Basic physics of MR contrast agents andmaximization of image contrast. J Magn Reson Imaging 1993;3:137–148.
5. Prince MR. Gadolinium-enhanced MR aortography. Radiology 1994;191:155–164.
6. Prince MR, Narasimham DL, Stanley JC, et al. Breath-hold gado-linium-enhanced MR angiography of the abdominal aorta and itsmajor branches. Radiology 1995;197:785–792.
7. Steffens JC, Link J, Grassner J, et al. Contrast-enhanced, k-space-centered, breath-hold MR angiography of the renal arteries and theabdominal aorta. J Magn Reson Imaging 1997;7:617–622.
8. Holland GA, Dougherty L, Carpenter JP, et al. Breath-hold ultrafastthree-dimensional gadolinium-enhanced MR angiography of theaorta and the renal and other visceral abdominal arteries. AJR1996;166:971–981.
9. Grist TM, Sproat IA, Kennel TW, Korosec FR, Swan JS. MR angiogra-phy of the renal arteries during a breath-hold using gadolinium-enhanced 3D TOF with k-space zero-filling and a contrast timingscan. In: Proceedings of the International Society of MagneticResonance in Medicine, 1996.
10. Kouwenhoven M. Contrast-enhanced MR angiography. Methods,limitations and possibilities. Acta Radiol Suppl 1997;412:57–67.
11. Levy RA, Prince MR. Arterial-phase three-dimensional contrast-enhanced MR angiography of the carotid arteries. AJR 1996;167:211–215.
12. Maki JH, Prince MR, Londy FJ, Chenevert TL. The effects of timevarying intravascular signal intensity and k-space acquisitionorder on three-dimensional MR angiography image quality. J MagnReson Imaging 1996;6:642–651.
13. Ito K, Kato J, Okada S, Kumazaki T. k-space filter effect inthree-dimensional contrast MR angiography. Acta Radiol 1997;38:173–175.
14. Prince MR, Chenevert TL, Foo TK, et al. Contrast-enhanced abdomi-nal MR angiography: optimization of imaging delay time by automat-ing the detection of contrast material arrival in the aorta. Radiology1997;203:109–114.
15. Lauzon ML, Holdsworth DW, Frayne R, Rutt BK. Effects of physi-ologic waveform variability in triggered MR imaging: theoreticalanalysis. J Magn Reson Imaging 1994;4:853–867.
16. Frank LR, Buxton RB, Kerber CW. Pulsatile flow artifacts in 3Dmagnetic resonance imaging. Magn Reson Med 1993;30:296–304.
17. Listerud J, Einstein S, Outwater E, Kressel HY. First principles offast spin echo. Magn Reson Q 1992;8:199–244.
18. Fischer H, Ladebeck R. Echo-planar imaging image artifacts. In:Schmitt F, Stehling MK, Turner R, editors. Echo planar imaging—theory, technique and application. Berlin: Springer-Verlag; 1998.pp 192–194.
19. Earls JP, Rofsky NM, DeCorato DR, Krinsky GA, Weinreb JC.Breath-hold single-dose gadolinium-enhanced three-dimensionalMR aortography: usefulness of a timing examination and MR powerinjector. Radiology 1996;201:705–710.
20. Ljunggren S. A simple graphical representation of fourier-based-imaging methods. J Magn Reson 1983;54:338–343.
21. Twieg DB. The k-trajectory formulation of the NMR imaging processwith applications in analysis and synthesis of imaging methods.Med Phys 1983;10:610–621.
22. Petersson JS, Christoffersson JO, Golman K. MRI simulation usingthe k-space formalism. Magn Reson Imaging 1993;11:557–568.
23. Petersson JS, Christoffersson JO. A multidimensional partitionanalysis of SSFP image pulse sequences. Magn Reson Imaging1997;15:451–467.
24. van der Meulen P, Groen JP, Tinus AM, Bruntink G. Fast field echoimaging: an overview and contrast calculations. Magn Reson Imag-ing 1988;6:355–368.
25. Bjornerud A, Myhr G. MR-kontrastmidler-virkningsmekanismer.In: Myhr G, Nordlid K, Bjornerud A, Lihaug EG, editors. Fokus påMRI og bruk av kontrastmidler. Oslo: Nycomed Imaging; 1996. pp44–45.
26. Sattin W, Haacke EM. Fast imaging and vessel contrast. In: PotchenEJ, Haacke EM, Siebert JE, Gottschalk AG, editors. Magneticresonance angiography, concepts and applications. St. Louis, MO:Mosby-Year Book; 1993. p 46.
27. Petersson JS. k-Space models in MRI using the concept of parti-tions, thesis, Malmo, Lund University, 1998.
28. Fritz Hansen T, Rostrup E, Larsson HB, et al. Measurement of thearterial concentration of Gd-DTPA using MRI: a step toward quanti-tative perfusion imaging. Magn Reson Med 1996;36:225–231.
29. Shetty AN, Bis KG, Vrachtolis TG, et al. Contrast-enhanced 3D MRAwith centric ordering in k space: a preliminary clinical experience inimaging the abdominal aorta and renal and peripheral arterialvasculature. J Magn Reson Imaging 1998;8:603–615.
30. Wilman AH, Riederer SJ, King BF, et al. Fluoroscopically triggeredcontrast-enhanced three-dimensional MR angiography with ellipti-cal centric view order: application to the renal arteries. Radiology1997;205:137–146.
Image Artifacts in 3D CE MRA 927

31. Hany TF, McKinnon GC, Leung DA, Pfammatter T, Debatin JF.Optimization of contrast timing for breath-hold three-dimensionalMR angiography. J Magn Reson Imaging 1997;7:551–556.
32. Maki JH, Chenevert TL, Prince MR. The effects of incompletebreath-holding on 3D MR image quality. J Magn Reson Imaging1997;7:1132–1139.
33. Grist TM, Sproat IA, Kennel TW, Korosec FR, Swan JS. MR angiogra-phy of the renal arteries during a breath-hold using gadolinium-enhanced 3D TOF with k-space zero-filling and a contrast timing
scan. In: Proceedings of the ISMRM 4th Annual Meeting, New York,1996.
34. Korosec FR, Frayne R, Grist TM, Mistretta CA. Time-resolvedcontrast-enhanced 3D MR angiography. Magn Reson Med 1996;36:345–351.
35. Foo TK, Saranathan M, Prince MR, Chenevert TL. Automateddetection of bolus arrival and initiation of data acquisition in fast,three-dimensional, gadolinium-enhanced MR angiography. Radiol-ogy 1997;203:275–280.
928 Svensson et al.