Embed Size (px)
Citation preview

Illinois Early Learning Council
February 24, 2020

| 2
Agenda1. Welcome and Introductions2. Universal Newborn Supports
3. Governor’s Early Childhood Priorities4. Governor’s Early Childhood Funding Commission
5. Break6. PDG B-5 Renewal Announcement
7. PN3 Initiative 8. Committee Reports
9. Announcements & Public Comments10. Adjourn

| 3
Universal Newborn Supports
Arden Handler, Nick Wechsler, and Diana Rauner

The Role of Universal Newborn Supports in Promoting Women’s Health in the Postpartum Period, Early Learning and Health, and Community Well-Being Home Visiting Task Force | February 24, 2020

5

Agenda
6
I. Universal Newborn Supports; exploration and implementation experience of Family Connects IllinoisNick Wechsler, Director for Program Development, Ounce of Prevention Fund
II. The Role of Home Visiting in Supporting Women’s Health in the Postpartum PeriodArden Handler, DrPH, Director of the Center of Excellence in Maternal and Child Health, Professor in the Community Health Sciences division of the UIC School of Public Health
III. Next steps & considerations for expanding Universal Newborn Supports Diana Rauner, Gaylord Gieseke, Co-chairs, Home Visiting Task Force

Exploration of Universal Newborn Supports
▫ Robust investment in intensive home visiting ▫ Exploration by Home Visiting Task Force
Subcommittee▫ Funding secured through the Maternal Infant and
Early Childhood Home Visiting program and the Illinois State Board of Education
▫ Selection and launch of Family Connects Illinois pilot sites: Stephenson and Peoria in May-June 2017
7
Launching Family Connects in Illinois

Universal Newborn Support Approach
▫ Model is not duplicative of intensive core home visiting services
▫ 100% voluntary, no cost to participants
▫ Reduces stigma of home visiting targeted toward “at-risk” populations
▫ Given existing focus on family needs in addition to early childhood, expanding focus on women’s health is logical
8
Family Connects Model

Evidence base for Family Connects
▫ 39% reduction in child welfare investigations through 60 months
▫ 50% less infant emergency medical care at 12 months, 37% at 24 months
▫ $3.17 in savings in medical care per $1 on the intervention
▫ 28% reduction in maternal reports of clinical anxiety
▫ Increased positive parenting skills (observer rated and parent reported)
▫ Increased connections to community resources
▫ Safer homes
9
Original RCT and subsequent research from 2009 - 2019

FC IL site updates July 2017 – December 2019
Robust outcomes from Stephenson & Peoria
▫ 3,540 births across two sites offered IHV▫ 1,959 received an integrated home visit▫ 95% bedside acceptance rate in most recent quarter, 76% IHV completion rate
among families agreeing to participate in the program
▫ Parent health, infant health, and household/material supports were most significant risks assessed, 97% need education about infant care
▫ 100% of families eligible for HV receive referrals to longer term intensive services▫ 190 families accepted referrals to longer term HV▫ 2,796 distinct community service referrals provided
10

The Role of Home Visiting in Supporting Women’s Health
in the Postpartum Period
Arden Handler, DrPHPresentation to the Early Learning Council
February 24, 2020

Reproductive and Perinatal Continuum
Improved Maternal Outcomes: Reduced Maternal
Morbidity and Mortality

Postpartum Period Increasingly Viewed as a Critical Time of Intervention
▪ Both mother and infant are in a time of transition and adaptation: risk of death highest for both mother and infant during this time (WHO, 2015)
▪ Women must recover from childbirth, a task made even more challenging if they have had a C-section, while also adapting to multiple physical, social, and psychological changes of their own ▪ Women are at risk of experiencing the “baby blues” or major postpartum depression
(American College of Obstetricians and Gynecologists, 2016)▪ Many women experience a substantial amount of morbidity (e.g., diabetes, hypertension)
during pregnancy, which often continues into the postpartum period (Callaghan, Creanga, & Kuklina, 2012)
▪ Women who have had a recent pregnancy are also at increased risk of unintended pregnancy compared to other women of reproductive age not using contraception (Fagan, Rodman, Sorensen, Landis, & Colvin, 2009)

Postpartum Period Increasingly Viewed as a Critical Time of Intervention
▪ Maternal Death is not only a Pregnancy Phenomenon ▪ In Illinois, of the 36 pregnancy-related deaths in 2015,
14% of deaths occurred during pregnancy, 53% occurred within 42 days PP, and 33% occurred between 43 and 364 days of the most recent pregnancy (IDPH, Maternal Morbidity and Mortality Report, October 2018).
▪ These data demonstrate importance of the PP period as a time for intervention to improve maternal health

▪ In some populations ,particularly among low-income women in the US, fewer than 60% of women receive a PP visit (IDHFS, 2016)
▪ Women who do not receive standard PP visit are at increased risk of unintended pregnancy, short interpregnancy interval, increased or unresolved morbidities, and unresolved postpartum depression
▪ Because 4-6 wk PP visit may be too “late”, new approaches to PP care are being developed
Issues of Concern with the 4-6 Week PP Visit

▪ Changing PP visit schedule and changing insurance reimbursement:
▪ ACOG now recommends postpartum care be an ongoing process, rather than a single encounter:▪ All women to have contact with their OB-GYN or other obstetric care provider within the first 3
weeks postpartum▪ Initial assessment to be followed up with ongoing care as needed, concluding with a
comprehensive postpartum visit no later than 12 weeks after birth
▪ New models in which women receive care or counseling/referral at the Well-Baby Visit of the newborn: ▪ In contrast to the PP visit, the Well-Baby Visit is highly utilized. Because women are more
likely to obtain care for their infants, compared to their own PP care, they are likely to attend multiple WBV visits (up to 9 visits in 18 months after delivery)
▪ Family Practice (Srinivasan et al. 2018) and pediatric models being developed (Caskey et al 2016; Haider et al. 2020)
Beyond the 4-6 Week Postpartum Visit: New Approaches to Providing PP Care

Home Visiting and Case Management Programs as an Opportunity for a Postpartum “Touch” for Women
▪Multiple Home Visiting/Case Management prenatal/postnatal programs: ▪ Includes nurse and non-nurse models (e.g., community health worker, doula)▪ Many focus primarily on infant, not woman
▪ Few efforts in US are universal--most are risk based▪ WHO recommends home visits for all women and infants in the first week
postpartum (WHO 2015) ▪ European nations include home visit as part of PP care (Cheng et al. 2006)
▪Durham Family Connects: universal early postpartum nurse home visiting program

Family Connects Model Developed with Focus on Early Childhood
▪Although Family Connects was developed with focus on early childhood, there has always been a focus on the entire family’s needs
▪Logical to expand the focus of the program to include:▪ women’s health and well-being

Formative Evaluation of Illinois Family Connects (IFC) Elevated FC as a Strategy for Postpartum
Women’s Health
▪ The formative evaluation of IFC was conducted in Winter 2018 in Peoria and Stephenson Counties, the two pilot sites for Illinois Family Connects ▪ UIC-School of Public Health Evaluation Team

Objectives of Early Formative Evaluation of Illinois Family
Connects
The Illinois Family Connects (IFC) early formative evaluation sought to determine: Best practices related to IFC implementation Barriers to and facilitators of IFC implementation Implementation challenges Initial perceived impact on women, infants, and
families, community institutions, and the community service delivery system
20

IFC Formative Evaluation Methods
Qualitative Interviews: Conducted 18 Key Informant interviews (9 in Peoria County, 9 in Stephenson County)
with IFC personnel, IFC associated hospital personnel and other key stakeholders Transcribed interviews, and coded and analyzed interview transcripts utilizing Dedoose
qualitative software Developed key themes and findings from the interview transcripts
Quantitative Information: Reviewed each county’s IFC Quarterly Reports Obtained information on each participating hospital’s birth demographics as well as each
county’s birth demographics (from vital records) and compared to IFC birth information
Triangulated quantitative and qualitative data
21

Consideration of Family Connects as a Woman’s Postpartum Health Program Emerged as a Key
Concept from the IFC Formative Evaluation
Formative Evaluation data were re-analyzed to align with the following questions:
Why is universal nurse home visiting in the early postpartum (PP) period an important part of the health care delivery system
for postpartum women?
Why does universal nurse home visiting appeal to staff, postpartum women, and their families?
What factors affect acceptance and completion of the universal nurse home visit in the postpartum period?
What are community-wide strategies to increase acceptance of and completion of the postpartum nurse home visit by women and families?

Why is Universal Nurse Home Visiting in the Early Postpartum (PP) Period an Important part of the Health
Care Delivery System for PP Women?
The early PP visit reaches women shortly after discharge which allows the identification of medical issues requiring immediate attention or referral:
• …“we’ve caught some serious medical conditions on those home visits and made direct connections immediately for services that have helped families avoid very serious health complications. We had one who had postpartum preeclampsia. It was caught by the nurse, and the nurse made contact with the doctor. The woman was admitted immediately, and they were able to address it before there was anything more serious.”

Why is Universal Nurse Home Visiting in the Early Postpartum (PP) Period an Important part of the
Health Care Delivery System for PP Women?
The early postpartum visit helps to identify and support women with postpartum depression:
• “ Because we’re seeing these women at three weeks postpartum versus six. And I sometimes think (visits) at six weeks …are too far out…..Where if they’re seeing somebody at three weeks and then they’re starting counseling that helps tremendously than waiting and additional month.”

Why does Universal Nurse Home Visiting appeal to Staff, Postpartum Women, and their Families?
Universality reduces Stigma:• “ So this is the biggest benefit that we’ve seen from this
program is that it’s universal, which is amazing because we obviously get, here at the health department, the higher risk, higher need population. But we’ve been able to identify and link families with services that we have and would not have come in contact with before had we not had the universal aspect of the program.”

Why does Universal Nurse Home Visiting appeal to Staff, Postpartum Women, and their Families?
Services Provided by a Nurse --- when home visitors are nurses, they are viewed as having the skills, expertise and authority to reassure women about their health and well-being, and that of the infant:
• “I think just having medical personnel come in. Having a nurse. Usually medical professionals not just nurses are trusted, have a good rapport with most patients….and I think its nice for moms and I think that makes it different from other home visiting programs.”

Chicago Family Connects (CFC)
▪Chicago has high rates of maternal and infant mortality with vast inequities partly due to:• Systems not coordinated; creating duplication and families
slipping through cracks• Many services not evidence-based• Services focus on families pre-determined to be at-risk• Families face barriers to enrolling in needed services• Structural and social determinants play a major role in MCH:
insufficient child care, transportation, housing in the context of residential segregation and racism

Chicago Family Connects
28
Organize referrals around hospitals, where 98% of births take place
Primary sites are hospitals
Select mix of hospitals to reach many populations, provide range of infrastructure and capacity, and offer lessons for scaling
Diversity to maximize learning
Establish CDPH as execution lead, using existing nurses, with potential for additional staffing through hospitals
Leverage existing resources
Reach enough families (est. ~4,000) to ensure a large sample size that can make the case for going to scale
Establish a proof point

More than 4,200 infants and their families will be reached through the first four pilot hospitals, concentrated on the west and
south sides
Rush University St. Bernard Hospital Norwegian American Hospital
Hospital Partners for CFC Pilot
29
Mount Sinai

The Chicago Family Connects Implementation Evaluation
▪ Two evaluation phases: implementation and impact
▪ The implementation evaluation of Chicago Family Connects (CFC) has three main objectives: ▪ To provide feedback on ongoing implementation during the
pilot phase of implementation ▪ To provide information about best practices prior to
expansion of CFC ▪ To inform the development of the impact evaluation

Three Regions to Launch Community Alignment Councils in 2020:
A, B, and D
31

Questions and Contact Information
▪ Arden Handler, DrPH
▪University of Illinois School of Public Health

Leveraging the existing momentum to fulfill PDG B-5 Strategic Plan
Next steps for expanding universal newborn supports
A. Identify and charge an existing workgroup to participate in the action steps and finance mechanisms.
B. Assess availability, access, quality, and equity of a full range of existing newborn supports.
C. Continue to identify community interest and share Family Connects Illinois Readiness Assessment.
D. Source of sustainable funding to supplement, not supplant EBHV funding
E. & F. Plan for alignment and coordination of providers and referral processess across ECE systems
33

To learn more:
▫ Nick Wechsler, Director for Program Development, Ounce of Prevention Fund
▫ Kayla Goldfarb, staffer, Home Visiting Task Force
▫ Family Connects Illinois (FC IL)
▫ https://familyconnectsil.org
34

| 35
Governor’s Early Childhood Priorities
Theresa Hawley

Early Learning Priorities
Early Learning CouncilFebruary 2020

Our Vision
37
We envision Illinois as a place where every young child—regardless of race, ethnicity, income, language, geography, ability, immigration status, or other circumstance—receives the strongest possible start in life so that they grow up safe, healthy, happy, ready to succeed, and eager to learn.

Education Goals for the administration

Themes for Our ECEC Agenda
• Restoring and Expanding Access to High-Quality ECEC
• Refining and Re-designing Standards, Funding Streams, and Infrastructure Supports
• Growing a Highly-Qualified ECEC Workforce
Strategic Plan: Access, Quality/Coordination, Workforce

Restoring & Expanding Access
• What we’ve already done– Raised CCAP eligibility to entry under 200% FPL; exit at
225% FPL– Lowered co-pays to no more than 9% of family income– Expanded PFA, PFAE and PI by a total of over 6,000
children– PDG B-5: Scaling up Home Visiting for DCFS-involved
families

Restoring & Expanding Access
• What we want to do– Bring intensive Home Visiting to “saturation”– Further lower co-pays to no more than 7% of family
income– Expand quality center-based infant-toddler care slots– Fill-in PFA/PFAE/HS “deserts”– Raise quality of preschool in child care centers,
especially for low-income children, so that children of working parents have access to HQ preschool
41

Access Goals for ECEC for this term
• Bring intensive home visiting to scale– Add about 13,000 slots (compared to FY18); needs to be carefully targeted
to avoid oversaturation– Develop potential scalable funding model for universal newborn visits
• Double the number of infants and toddlers in high quality child care
– Add about 5,000 slots of Prevention Initiative-Center Based, Early Head Start-Child care Partnership, or new initiative to create high quality slots
– Implement stronger supports for FFN and licensed Family Child Care• Ensure all low-income preschoolers have access to a high-quality
preschool education– Requires some expansion in schools, in some communities (targeted)– Requires raising to Gold the quality of preschool education in many more
child care centers• Support continued financial viability of child care providers

Refining & Redesigning
• Goal is to create greater coherence and stability for the system, so that it has a solid foundation on which to scale up
• What we’ve already done:– Establish Equitable ECEC Funding Commission– Re-established the Child Care Advisory Committee– Substantially revised the ECBG RFPs to better target
expansion– Raised CCAP reimbursement rate, addressing disparities in
rural counties– Included support for Pyramid Model implementation, K
transitions pilots, and I/ECMH training in PDG B-5 grant– Begun planning for intentional engagement of families in
ELC & system governance

Refining & Redesigning—To Do’s
• Update ExceleRate Illinois– Better support and recognize incremental quality
improvement– Support “ownership” of continuous quality improvement– Facilitate funding for structural quality (the things that cost
more)• Refine CCAP rate structure/contract approach
– Informed by cost modeling – Emphasis on paying for quality– Taking into account other funding streams as appropriate
• Clarify program models/standards– Clarify model(s) for incorporating PFA into FD/FY child care
programs– Clarify PI Center-Based model requirements

Refining & Redesigning—To Do’s, Cont.
• Strengthen our approaches to supporting quality– Pilot new approach to supporting quality improvement with
contracts– Bring I/ECMH consultation supports to scale– Embed Pyramid Model approach throughout EC training
infrastructure– Design & implement expanded supports for FFN and FCC
care
• Design & establish stable funding for accountable local early childhood community systems– Building on successes of AOK Networks, Innovation Zones,
other community collaborations– Focus on system-level planning, coordinated recruitment &
enrollment, comprehensive supports

Refining & Redesigning—To Do’s, Cont.
• Strengthen data systems to support planning and CQI– Longitudinal Data System 2.0: Better approach for
combining existing data to facilitate meaningful data analysis
– “What if?” Design: Explore possibilities for new types of data collection systems (e.g., cross-system attendance database?)

Growing a Highly-Qualified ECEC Workforce
• Areas of emphasis:– Increasing compensation– Strengthening workforce development pathways
• What we’ve already done:– Increase minimum wage– ECGB RFPs, City RFPs require more equitable wages– Pilot child care contracts with emphasis on compensation– Included funding for cohort models in PDG B-5– Included funding for modularization of coursework in
PDG B-5

Workforce, Cont.
• What we’d like to do:– Build stronger pathways for moving from entry all the way
to BA/PEL– Explore innovations for potential to scale
• Credit-bearing CDAs• Credit for prior learning
– Strengthen support for job-embedded professional development
– Develop and implement strategies for recruiting people to the field
• Goal: Produce 6,000 new early childhood teachers– Including current staff who get higher level credentials

Embargoed until 12:00 Noon, Wednesday, February 19, 2020
Fiscal Year 2021 Budget –Rebuilding Illinois - Stronger Each Day
The proposed fiscal year 2021 budget builds on the progress that Illinois has made in the last year.
Restore Economic and Budgetary Stability
Ensure a Responsibly Balanced Budget Through Reserves Dependent on Public Act 101-0008 Taking Effect
Make Illinois the Best State in the Nation to Raise a Family
Strengthen Illinois’ Social Safety Network
Reform the Criminal Justice System and Invest in Public Safety
Rebuild Illinois’ Infrastructure
Keep Illinois a World Leader and Competitive in a Global Economy
49
Overview

Embargoed until 12:00 Noon, Wednesday, February 19, 2020
Birth Through FiveInvesting in Our Children
50
Making Illinois the best state in the nation to raise a family, with record early childhood funding to prepare all Illinois children for kindergarten and beyond.
Increases State Early Childhood Block Grant - $50 million
Strengthens Child Care Assistance Program to provide care to nearly 140,000 children monthly - $100 million increase
Increases Early Intervention Program funding - $7 million
Additional $13.5 million federal funding to improve quality of preschool programs
Increases home visiting services to an additional 500 families to provide coaching and support beginning with pregnancy and continuing through the first few years of the lives of their children - $4.25 million
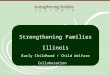
Early Childhood
$394
$444
$494
$544
$594
$250
$300
$350
$400
$450
$500
$550
$600
$650
FY2017Enacted
FY2018Enacted
FY2019Enacted
FY2020Enacted
FY2021Proposed
Early Childhood Block Grant Funding(Dollars in Millions)

| 51
Governor’s Early Childhood Funding Commission
Theresa Hawley

Commission on Equitable Early Childhood Education and Care FundingUpdate for the Early Learning Council
52
February 2020

Commission’s Charge
53
“The Commission shall study and
make recommendations to
establish funding goals and funding
mechanisms to provide equitable
access to high-quality early
childhood education and care
services for all children birth to age
five and advise the Governor in
planning and implementing these
recommendations.”

Commission Deliverable
• We need to know “the number”. There is not enough revenue in the system to support a sufficient, stable supply of providers of high-quality ECEC – how much do we need?
• We need to assess all funding mechanisms and the management and oversight structures of ECEC.– How should we distribute funds?
– Who should distribute and monitor the funds?
• We need to determine how to implement our recommendations– How will we reach our recommended end state, over what period
of time?
54

Commission Timeline
The Commission will deliver its report by January 2021 with consideration to the Governor’s budget address and legislative session timing.
55

Guiding Principles
These Guiding Principles reflect the Commission’s values and beliefs, guide how it operates, and lay a foundation for decision-making
56
•It should be invested in as such as this is critical to our State’s workforce, economy, and welfare of its residents.
High Quality ECEC is a Public Priority
•We will endorse a system that promotes equitable outcomes for children, with intentional focus on race, ethnicity, culture, language, income, children’s individual needs, and geography
Promote Equity
•Everything is on the table, including how funding flows, how funding decisions are made, and who makes them, to better serve all children and families
Embrace Bold System-Level Changes
•We will build upon the successes of Illinois’ past and current system, its commitment to a prenatal to 5 system, the lessons from other states, and the expertise and research in the field
Build Upon the Solid Foundation
•We will prioritize families' perspectives, needs, and choices as we make recommendations to improve the system
Prioritize Family Perspectives, Needs, and Choices
•We recognize our system must provide funding stability for providers, educators, and staff across mixed delivery settings to better serve families
Design for Stability and Sustainability
•We see these as necessary conditions for all stakeholders, funding distributors, and funding recipients for any future ECEC funding structure
Require System Transparency, Efficiency, and Accountability
•We will plan for meaningful change over a multi-year time horizonRecognize Implementation Realities

We will utilize Working Groups to address key questions
57
Working Groups(Focused on key charge questions)
Commission

We established these Working Groups
Funding Adequacy
Funding Mechanisms
Management & Oversight
Inclusion
58

Management & Oversight Working Group Charge
59
Goal: recommend improved ECEC management structures and responsibilities, in alignment with Guiding Principles
Key Questions to Answer:
• Who sets the vision and maintains and updates policies and priorities for the overall ECEC system in Illinois?
• Who allocates funds and distributes them?
• Who holds recipients accountable for what they do with funding?

Funding Mechanism Working Group Charge
60
Goal: recommend improved funding mechanisms to move funding from various sources to recipients, in alignment with Guiding Principles
Key Questions to Answer:• How can funding mechanisms be improved to support
the Commission’s guiding principles?• What funding innovations could increase efficiency of
existing funding?• How will funding move from various sources to
recipients? • How will recipients of funding be determined?• How do funding systems/structures interact with
accountability systems/structures?

What do we mean when we say ”funding mechanisms”?
The process by which money appropriated for ECEC services is distributed to fund ECEC
services.
61

Funding Adequacy Working Group Charge
62
Goal: determine the cost of providing high quality ECEC services and how to fund over time
Key Questions to Answer:• What is the cost of providing high quality ECEC to
all families in Illinois?• What should the state process be for determining
adequate resources across settings for each program type?
• How much of the cost should be covered by the federal government, the state, local funding, and parent contributions?
• What is the recommended timeline to get to the state’s full investment?

Simplistic Formula for System Cost
63
Program Cost
Structure
Program Cost
Structure
Program Cost
Structure
Children served
Children served
Children served
Total System Costs
Prog
ram
1Pr
ogra
m 2
Prog
ram
3
What resources are required to
meet “high quality”
standards?
How many families will opt
into which programs?
What system-level costs must be
added to programmatic costs
(i.e., admin and infrastructure)?
Infra-structure
Costs

Inclusion Charge
64
Goal: Inform the work of other Working Groups and the full Commission as it relates to children receiving special education and early intervention services, in alignment with the Commission's guiding principles
Key Questions to Answer:
• What is the cost for identifying students in need of special services and for serving children in inclusive environments? (Funding Adequacy)
• How should funding sources particular to Special Education / Early Intervention interact with other funding sources? (Funding Mechanism)
• How will funding particular to Special Education/ Early Intervention move from various sources to recipients? (Funding Mechanism)
• How do we ensure funding promotes seamless supports from identification to receiving services? (All three working groups)
• How do we ensure transparency, efficiency, effectiveness, and greater coordination in the system to enable state-level and community-level planning and accountability?

Stakeholder engagement is at the heart of our Commission’s guiding principles; thus:
We will look to the public and stakeholders for advice and innovation in formulating
recommendations and will incorporate public and stakeholder advice into the final
recommendations to the maximum extent possible.
65

Our stakeholder engagement is successful if…
ECEC advocates, providers, and families feel heard, valued, respected, prioritized, and involved in the Commission's work, and
They see their perspectives and recommendations for change reflected in the
Commission's information gathering, deliberations, final recommendations, and
blueprint for change.
66

Commission Meeting Dates for 2020
Tuesday, March 10Tuesday, April 14Monday, May 11Tuesday, June 16Tuesday, July 14
67
Tuesday, August 18Tuesday, September 15Tuesday, October 13Tuesday, November 10Tuesday, December 8

| 68
Break

| 69
PDG B-5 Renewal Announcement
Artiya Nash

2020 Grant AwardPDG B-5
• 20 states and territories were awarded three-year renewal grants
• 6 of the 20 states received highest amount $13,414,500
• Award amounts ranged from $3million - $13 million
• Illinois Awarded $ 13,414,500

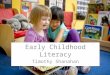
PDG B-5 Activity Budget FY20
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
3,500,000
4,000,000
4,500,000
Activity 1 Activity 2 Activity 3 Activity 4 Activity 5 Activity 6
Needs Assessment Strategic Planning FamilyEngagement
Professional Development
Quality Data

Activity 1
Needs Assessment
• In Renewal Year One, Illinois will focus on addressing data gaps identified through the initial PDG B-5 Statewide Needs Assessment, prioritizing qualitative analysis to better understand how families engage with the ECCE system, what their needs are, and how the ECCE system might better address those needs.

Activity 2
Strategic Plan
• The Strategic Plan is organized into four goal areas: Access, Coordination, Quality, and Workforce Support
• As proposed in the strategic planning and performance measurement cycle, Illinois will conduct an updated statewide needs assessment to incorporate improvements to data accessibility, cleanliness, and integration completed through Activities One and Six. This will inform an annually updated Strategic Plan.

Activity 3Family Engagement
Illinois’ Renewal application reflects a strong emphasis
on family engagement with the goal of delivering ECCE services that are responsive
to family needs.
We will engage families in policymaking through the
Family Advisory Committee of the Early Learning Council
(ELC).
We will also conduct Parent Cafés built upon protective
factors to connect families to services and to each other around topics that reflect
expressed interests

Activity 4Professional Development (sharing best practices )
Provide Provide workforce development supports, including financial assistance, course modularization, and cohorts for completing degrees and credentials
Expand Expand both practice-based coaching and evidence-based programs to support children’s social/emotional development and address trauma.
Deepen In the Renewal, Illinois will deepen alignment across professional development (PD) systems to share best practices.

Activity 5
Quality
• Expansion of high-quality early learning opportunities in child care settings will be supported with PDG B-5 Renewal funds through subgrants to support enhanced rates, increased staff compensation, improved staff-to-child ratios, and support for continuous quality improvement (CQI), with a focus on rural areas and programs serving infants and toddlers.

Activity 6
Data
• Finally, Illinois’ application reflects a commitment to using high-quality data to inform cross-agency decision making. Illinois will standardize ECCE data across systems and construct a platform for replicable, comprehensive analysis; construct a more accurate and comprehensive unduplicated count of children served by publicly-funded systems

Bonus Sections
KDG Transition Pilot
Illinois will implement eight kindergarten transition community partnership pilots designed to support local community context and decision-making that includes all involved in the transition to kindergarten.
Infant Toddler Emphasis
The Illinois Children's Mental Health Partnership is currently working closely with public and private stakeholders to implement a multi-year I/ECMH Initiative with the goal of developing and testing a universal, effective, and sustainable Illinois I/ECMHC Model,
Coordinated Intake Pilot
CI pilot will be developed to link evidence-based HV to partners that already connect families to other services, namely CCR&Rs and HS/EHS.

PDG B-5 FY 20Total Projects
34 Projects

| 80
Prenatal to Three Initiative (PN3)
Karen Berman

| 81
Committee Report:Access Committee
Maria Whelan

| 82
Committee Report:Home Visiting Task Force
Gaylord Gieseke and Diana Rauner

| 83
Committee Report:Integration & Alignment Committee
Shauna Ejeh and Karen Berman

Integration and Alignment full committee updates
• To advance the ELC mixed service delivery recommendations, the Committee is supporting OECD, DHS, ISBE and the Head Start Collaboration Office to develop coordinated budgeting and operationalizing templates for providers to use in applying for program funding. These tools would be used for providers outside of the City of Chicago, where blending and braiding of funding is quite limited. Co-chair, Shauna Ejeh, completed a series of interviews with providers to inform this work.
• The Committee will also be considering the findings from interviews with LEAs and community providers in areas with the greatest 3-5 slot gaps to determine the policies and supports that would best support them in applying for and implementing high quality early childhood programs.
• The Committee continues to inform and analyze how the state’s early childhood funding is designed and allocated to meet the quality improvement and access to services across the state, with particular attention to the families who are most in need of services.
Next IAC Meeting: March 4, 2020, 10:30 am – 1:00 pm

Integration and Alignment subcommittee updates
Health Subcommittee• Partnering with MCOs to identify how partnerships with early childhood program and
attention to the early years can support enrollment in high-quality early child care.• Elevating concerns and identifying strategies to address the increase in uninsured children in
Illinois.
Inclusion Subcommittee• Supporting advancement of the ELC approved recommendation to improve the quality and
supply of inclusive child care for children with disabilities. Updated recommendations are pending approval by the full Child Care Advisory Council.
• Advancing work with OECD and ISBE to ensure that children ages 3-5 with disabilities can receive special education and related services within community-based programs. Work includes developing and promoting financing and staffing models for LEAs and CBOs.
Data, Research and Evaluation Subcommittee• Supporting the needs of OECD and AIR regarding PDG B-5.
Community Systems Development:• Grace Araya, Illinois Action for Children, appointed as co-chair. Providing input and support to
OECD on development of an input and feedback mechanism for community systems to elevate concerns and needs to the Administration.

| 86
Committee Report:Quality Committee
Dan Harris and Teri Talan

PDG B5 Child Care PilotOpportunity to test revised standards
ExceleRate Subcommittee

Goals for standards revision
• Funders support adequate staffing
• Program staff “owns” continuous improvement
• Publicly-funded supports align with standards
• Aggregate data informs policy and funding

Funders support adequate staffing
• Current standards hold programs responsible for staffing patterns and credentials.
• An effective system will fund staffing first, then expect quality (not vice-versa w/ rate add-ons).
• Pilot will fund programs (classrooms) through contracts, as PFA and HS do.

Program staff “owns” continuous improvement• Use program assessment results as baseline
information for staff. No high-stakes “cut scores” with funding ramifications.
• Plan as a team for improvement, on a regular schedule
• Learn as a team through job-embedded professional learning
• Test new approaches: small steps, short cycles

Supports align with standards
• Standards describe continuous improvement practices at Bronze, Silver and Gold levels
• Technical assistance and coaching can be aligned to the standards

Aggregate data informs policy and funding
• Program assessment scores can be aggregated to answer questions of system effectiveness, and as baseline data for system improvement.

| 93
Committee Report:ELC Membership Ad Hoc
Phyllis Glink

| 94
Announcements & Public Comments

| 95
Adjourn