Embed Size (px)
Citation preview

Australian Resuscitation
Council
ILCOR, ARC & NZRC PAEDIATRIC
RESUSCITATION RECOMMENDATIONS
2010
Jim Tibballs
Resuscitation Officer, RCH
Convenor, Paediatric Sub-Committee,
Australian Resuscitation Council (ARC)
ARC Paediatric Representative
International Liaison Committee on Resuscitation (ILCOR)

Australian Resuscitation
Council
CONFLICT of INTEREST
• No financial
• Intellectual
• Member of ARC
• ILCOR delegate
• Co-author of some studies

Australian Resuscitation
Council
• Present some 2010 ILCOR recommendations
• Present rationale of a few changes
• Identify “departures” by ARC & NZRC (&ERC)
from ILCOR recommendations
• Identify some ARC & NZRC recommendations
not considered by ILCOR
Australian Resuscitation
Council 2010 ILCOR • 55 clinical subjects
• 20 new recommendations
• 7 “need to know” recommendations • Medical emergency team
• Starting CPR
• Pulse palpation
• Breaths vs no breaths
• Compression:ventilation ratios
• Infants and children
• Newborns outside delivery room
• Exhaled CO2 monitoring
• DC shock dose
• Oxygen
• Hypothermia

Australian Resuscitation
Council
ILCOR GUIDELINES published Oct-Nov 2010
<www,ilcor.org> Resuscitation 2010; 81: e213-e259 (Oct)
Circulation 2010; 122: S466-S515 (Oct)
Pediatrics 2010: 126(5):e1261-318 (Nov)
www.resus.org.au
paediatric guidelines
summary of changes to guidelines
JT 2011

Australian Resuscitation
Council Medical Emergency/Rapid Response
Team/Early Warning Scores
ILCOR
• Pediatric RRT or MET
systems may be
beneficial to reduce the
risk of respiratory and/or
cardiac arrest in
hospitalized pediatric
patients
ARC and NZRC
• All institutions … should
have a system which
enables staff at the
bedside to quickly
summon expert help to
assist in the management
of serious-illness.
Examples of such
systems are medical
emergency team (MET)
or rapid response team
(RRT) systems

Australian Resuscitation
Council
Chan PS, Jain, R. et. al.(2010) “Rapid Response Teams: a systematic review and meta-analysis.” Arch Intern Med. 170(1):18-26
Control Post Intervention Wt. RR (95% CI )
# pts Dths # Pts Dths
Results: Rate of Cardiopulmonary Arrest (↓ 38%)

Australian Resuscitation
Council Chan PS, Jain, R. et. al.(2010) “Rapid Response Teams: a systematic review and meta-analysis.” Arch Intern Med. 170(1):18-26
Results: Hospital Mortality Rate (↓21%)
Control Post Intervention Wt. RR (95% CI )
# pts Dths # Pts Dths

Australian Resuscitation
Council STARTING CPR
• If the victim is unresponsive and not
breathing normally (ILCOR – and there are
no signs of life)…
• … and if cannot palpate a pulse within 10
seconds with certainty, start CPR

Australian Resuscitation
Council
PULSE PALPATION (Resuscitation 2009; 80: 61. Resuscitation 2010; 81: 671)
• Accuracy 78% - all doctors and nurses
• Sensitivity 86% (diagnose CA correctly – BUT fail to diagnose CA 14%)
• Specificity 64% (exclude CA correctly – BUT diagnose CA incorrectly 36%)
• Average 15 seconds to exclude CA when truly absent
• Average 30 seconds to confirm CA when truly present
Experienced doctors correctly diagnose CA within 10 seconds

Australian Resuscitation
Council INITIAL BREATHS
ILCOR
2-5 (2005)
AHA
start ECC first
ARC & NZRC
Start ECC first
2 breaths first optional
ERC
5 breaths first
JT 2011
ILCOR 2010 Silent

Australian Resuscitation
Council
Shockable Non
Shockable
Shock (4 J/kg)
Return of
Spontaneous
Circulation ?
Post Resuscitation Care
CPR for 2 minutes
During CPR Airway adjuncts (LMA / ETT)
Oxygen
Waveform capnography
IV / IO access
Plan actions before interrupting
compressions
(e.g. charge manual defibrillator to 4
J/kg)
Drugs
Shockable
* Adrenaline 10 mcg/kg after 2nd
shock
(then every 2nd loop)
* Amiodarone 5mg/kg after 3rd shock
Non Shockable
* Adrenaline 10 mcg/kg immediately
(then every 2nd loop)
Consider and Correct Hypoxia
Hypovolaemia
Hyper / hypokalaemia / metabolic disorders
Hypothermia / hyperthermia
Tension pneumothorax
Tamponade
Toxins
Thrombosis (pulmonary / coronary)
Post Resuscitation Care Re-evaluate ABCDE
12 lead ECG
Treat precipitating causes
Re-evaluate oxygenation and ventilation
Temperature control (cool)
Advanced Life Support
for Infants and Children
December 2010
CPR for 2 minutes
Assess
Rhythm
Start CPR 15 compressions : 2 breaths
Minimise Interruptions
Attach Defibrillator / Monitor
Adrenaline 10 mcg/kg (immediately then every 2nd cycle)
JT 2011
Can give 2
breaths first

Australian Resuscitation
Council
COMPRESSION : VENTILATION RATIO
15:2
Why not 30:2 ratio for infants and
children? JT 2011

Australian Resuscitation
Council Why not 30:2 for paediatrics? • No human evidence
• Consensus with adult scientists NOT achieved. (Paediatricians not persuaded by animal cardiac arrest studies, mannekin studies and computer simulations)
• Rationale conjecture:
• Paediatric ventilation requirement greater than adult
• Hypoxic arrest, not sudden arrhythmia arrest, more common in paediatric practice
• In out-of-hospital paediatric cardiac arrest (Kitamura et al., Lancet 2010;
375: 1347)
• Survival from asphyxial cause better (7.2%) with standard CPR (7.2%) vs compression-only CPR (1.6%) vs no CPR (1.5%)
• Survival from cardiac cause same with standard CPR (9.9%) vs compression-only CPR (8.9%) vs no CPR (4.1%)
• 15:2 previously used for children (one-person rescue)
JT 2011

Australian Resuscitation
Council
Compression-ventilation ratios for
infants
JT 2011

Australian Resuscitation
Council Compression : ventilation ratio for infants (Term infants out of delivery area within first month)
At birth – 3:1
ILCOR
• In non-neonatal setting (eg
ED, PICU, prehospital) or with
cardiac aetiology regardless of
location:
• No ETT – prefer 15:2 over 3:1
• ETT – continuous compressions
no pauses for ventilations (15:2)
“ For use of training – use what is
commonly used in your
environment”
ARC & NZRC
• In ED, PICU, wards,
prehospital setting use 15:2
• With exception of newborns,
with cardiac aetiology
regardless of location:
• No ETT - 15:2
• ETT - continuous compressions
no pauses for ventilation 10/min

Australian Resuscitation
Council Ventilations after intubation
ILCOR
“reduce”
AHA 8-10/min (no circ)
12-20/min (circ)
ARC & NZRC 10/min
ERC
10-12/min
JT 2011
2010

Australian Resuscitation
Council
Compression : Ventilation ratio
after intubation
10:1
JT 2011

Australian Resuscitation
Council Compression – Ventilation Cycles
Basic CPR 30:2 (single rescuer)
2010 ILCOR
silent
AHA
5 in 2 min*
ARC & NZRC
5 in 2 min*
ERC
silent
• 75 compressions/minute
• 5 breaths/minute
JT 2011

Australian Resuscitation
Council Compression – Ventilation Cycles
Advanced CPR 15:2 (2 rescuers)
2010 ILCOR
silent
AHA
5 in 1 min* ARC & NZRC
5 in 1 min*
ERC
silent
• 75 compressions/minute
• 10 breaths/minute
JT 2011

Australian Resuscitation
Council
DC shock dose
JT 2011

Australian Resuscitation
Council
Dose of DC Shock
(Single shock strategy)
ILCOR CoSTR
2 - 4 J/kg
AHA
2 - 4 J/kg
ARC & NZRC
4 J/kg
ERC
4 J/kg
JT 2011
Australian Resuscitation
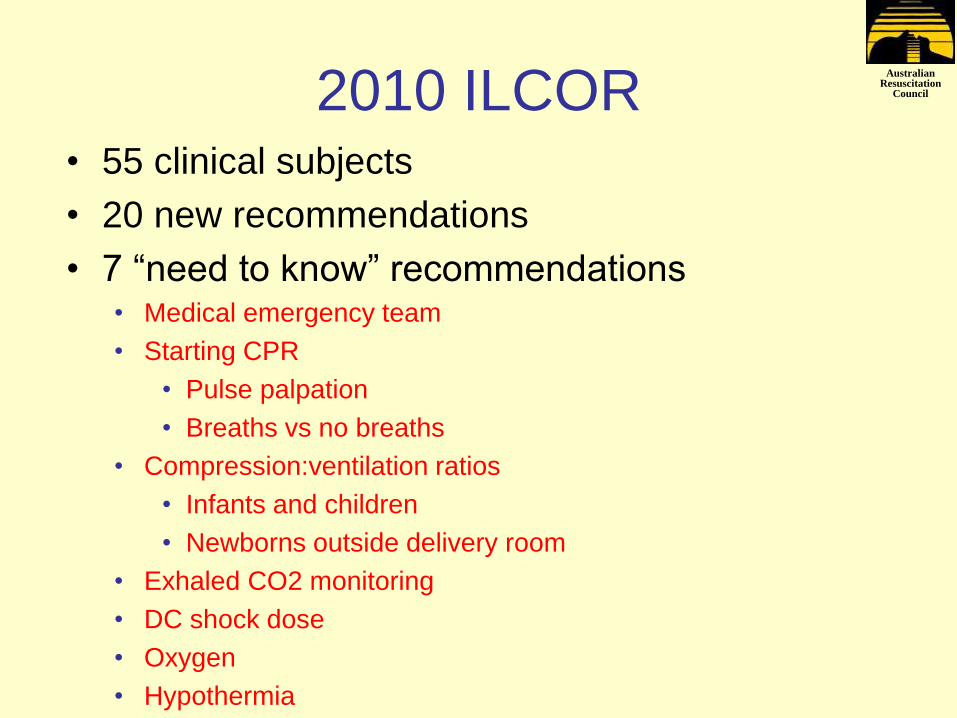
Council Biphasic DC shock for VF and pulseless VT Pediatr Crit Care Med 2011; 12: 14-20
0
20
40
60
80
100
120
140
160
180
200
220
0 10 20 30 40 50 60 70 80 90 100
Body weight (kg)
Jo
ule
s
ROSC
non-ROSC1J/kg
2J/kg
3J/kg4J/kg5J/kg
N=48
JT 2011
ROSC 50% if ≤2J/kg
ROSC if 3-5 J/kg

Australian Resuscitation
Council
Copyright ©2011 American Academy of Pediatrics
Meaney, P. A. et al. Pediatrics 2011;127:e16-e23
Outcomes according to shock dose

Australian Resuscitation
Council
Monitoring exhaled CO2
JT 2011

Australian Resuscitation
Council
1. To detect non-tracheal
intubation (standard of care)
2. Assess effectiveness of CPR
JT 2011

Australian Resuscitation
Council Monitoring end-tidal CO2
(PetCO2 )
ILCOR
• May guide effectiveness of
chest compressions. If
PetCO2 is < 15 mmHg,
improve chest compression
and reduce ventilation
• Cannot yet identify
threshold to stop CPR
ARC & NZRC
• Low PetCO2 may be due to
excessive positive
pressure ventilation or
inadequate chest
compressions or both

Australian Resuscitation
Council
End tidal C02 will rise as pulmonary blood
flow and overall cardiac output rises,
assuming that the amount of ventilation
(tidal volume and rate) does not change
Jin, CCM, 2000
Quantifying the effectiveness of CCs

Australian Resuscitation
Council Assessing effectiveness of CPR
Krep H, Mamier M, Breil
M, et al. Resuscitation.
2007;73(1):86.
JT 2011
No ROSC – low end-tidal CO2
ROSC – normal end-tidal CO2

Australian Resuscitation
Council
Partial pressure of end-tidal carbon dioxide successfully
predicts cardiopulmonary resuscitation in the field: a
prospective observational study. Kolar et al., Crit Care 2008; !2: R115
• 737 intubated cases out-of-hospital cardiac arrest
• After 20 minutes of CPR:
• 402 cases of ROSC when PetCO2 mean 33+/-9 mmHg
• 335 cases of non-ROSC when PetCO2 mean 7+/-2 mmHg
• PetCO2 <14 mmHg reliably predicts (100%) non-ROSC
• PetCO2 >14 mmHg reliably predicts (100%) ROSC

Australian Resuscitation
Council Oxygen
ILCOR
• Cannot specify oxygen
concentration during
resuscitation
• After resuscitation, titrate
oxygen concentration to
limit hyperoxemia
ARC & NZRC
• Use 100% oxygen initially
for resuscitation
• After resuscitation reduce
to yield PaO2 80-100
mmHg

Australian Resuscitation
Council Hypothermia
ILCOR
• Hypothermia (32-34
degrees) may be
considered for those
remaining comatose after
resuscitation
ARC & NZRC
• It is acceptable to induce
hypothermia (32-34
degrees) within 6 hours and
maintain up to 72 hours in
those remaining comatose
after resuscitation

Australian Resuscitation
Council
Principles of Guideline Formulation
Survival = Science x Education x Implementation
JT 2011

Australian Resuscitation
Council
... the debate will continue, especially
when data is lacking, after all …
“It’s not necessary to understand things in
order to argue about them ”
“Il n’est pas nécessaire de tenir les choses
pour en raisonner ” (Pierre Beaumarchais. Le Barbier de Séville)