Embed Size (px)
Citation preview

Il punto di vista del clinico
Fabio Puglisi, MD PhD
Ruolo della terapia antiangiogenica nel carcinoma mammario

Therapeutic Options in Metastatic Breast
Cancer• No single “Gold Standard” for
therapy in metastatic breast cancer
• Therapy should be individualized based on goals, tumor, and patient characteristics

Goals of Therapy
Judicious use of agents individualized
to the patient’s clinical situation• Maximize survival
• Maintain disease control
• Minimize symptoms from disease
• Minimize toxicity from treatment
QUALITYOF LIFE
Overt metastatic disease is generally incurable

Goals of Therapy
Maximize survival

Bevacizumab:First-line trials
Efficacy
E-2100 AVADO Ribbon-1 Capecitabine
Ribbon-1
A/TControl
Arm
Beva
Arm
Placebo
Arm
Beva
Arm
7.5/15 mg/kg
Placebo
Arm
Beva
Arm
Placebo
Arm
Beva
Arm
PFS months
5.9 11.8 8.2 9/10.1 5.7 8.6 8.0 9.2
HR0.60
P<.0001
0.86 P=.12 (7.5 mg)
0.77 P=.006 (15 mg)
0.69
P=.0002
0.64
P<.0001
OS months
25.2 26.7 31.9 30.8/30.3 21.2 29 23.8 25.2
HR0.88
P=.16
1.05/1.03
P=.72/.85
0.85
P=.27
1.03
P=.83

Endpoints in phase III Metastatic Breast Cancer trials
9/73 (12%) of trialsdemonstrated OSgains
OS gains lessfrequently noted infirst-line trials (8%)than in second-line+trials (22%)
Verma S, et al. The Oncologist 2011Verma S, et al. The Oncologist 2011

Why OS gain is rarely noted?
• Potentially active subsequent lines (including crossover) are not controlled in most RcTs
• Many RcTs lack statistical power to detect plausible increases in OS
• Larger sample size is requested• Longer follow-up period is requested

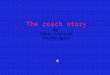
Survival post-progression
OS = PFS + SPPIf the progression eventis death, then SPP = 0
Broglio KR & Berry DA, JNCI 2009

Broglio, K. R. et al. J. Natl. Cancer Inst. 2009
Probability of statistically significant differences in overall survival (OS) as a function of median survival
postprogression (SPP)

Chance of seeing a survival benefit according to SPP
> 90% if SPP = 2 months
< 50% if SPP = 8 months
< 20% if SPP = 24 months

First-line trials and SPP
Efficacy
E-2100 AVADO Ribbon-1 Capecitabine
Ribbon-1
A/TControl
Arm
Beva
Arm
Placebo
Arm
Beva
Arm
7.5/15 mg/kg
Placebo
Arm
Beva
Arm
Placebo
Arm
Beva
Arm
OS months
25.2 26.7 31.9 30.8/30.3 21.2 29 23.8 25.2
HR0.88
P=.16
1.05/1.03
P=.72/.85
0.85
P=.27
1.03
P=.83
SPP
months19.3 14.9 23.7 21.8/20.2 15.5 20.4 15.8 16
SPP, mos 17.5 19.7 -
Meta-analysis: summary of results

Meta-Analysis crossover and post-study therapiesTherapies used upon progression in AVADO and
RIBBON-1a
Therapy, %CT + Beva
(n=1071)
CT(n=654)
Chemotherapy 65 71
Bevacizumab 40 51
Hormonal therapy 23 25
Number of subsequent agents– 1– 2– 3– ≥ 4
15261223
10271527
O’Shaugnessy J et al, ASCO 2010. Abstract 1005aData not available from E2100

Estimating scenarios for survival
• 36 first-line chemotherapy trials for metastatic breast cancer published from 1999 to 2009
– Mean for Median PFS: 7.6 months (6.0-9.0)– Mean for Median SPP: 14 months (10.8-15.6)– Mean for Median OS: 21.7 (18.2-24.0)– Mean for Median ratio OS/PFS: 3 (2.4-3.5)– Mean 1-year survival: 73% (69-78%)– Mean 2-year survival: 45% (38-50%)– Mean 5-year survival*: 12% (7-17%)
*information available only in 14 trials
Published Ahead of Print on December 28, 2010 as 10.1200/JCO.2010.30.2174

Survival curve percentiles and their corresponding scenarios
Published Ahead of Print on December 28, 2010 as 10.1200/JCO.2010.30.2174

Simple rules of thumb: bevacizumab
Estimates by multiplying median by four
simple multiples:
• 0.25 (worst-case) 0.25 x 26.7 = 6.67
• 0.5 (lower-typical) 2 (upper-typical) 0.5 x 26.7 = 13.3 2 X 26.7 = 53.4
• 3 (best-case) 3 x 26.7 = 80.1 (= 6.7 years)

The Main Question
Who are these patients, and what characteristics predict for the tail of the
curve?

Goals of Therapy
Maintain disease control
Minimize symptoms from disease

Endpoints in Clinical TrialsWhat Matters Most?
• Progression-free survival and response rate are important achievements in their own right
– Shrinking a cancer may minimize a patient's acute symptoms.
– Prolonging progression-free survival may be associated with enhanced quality of life, even without an improvement in overall survival.

0
20
40
60
80
100
Investigator assessment IRF assessment
aPatients with measurable disease at baseline
Klencke et al. ASCO 2008
Pat
ient
s, %
23%
Paclitaxel Bevacizumab + paclitaxel
48%
p<0.0001
Paclitaxel Bevacizumab + paclitaxel
p<0.0001
E2100: response ratea
0
20
40
60
80
100
22%
50%
Pat
ient
s, %

0
20
40
60
80
100
aPatients with measurable disease at baseline
Miles et al. SABCS 2009
Pat
ient
s, %
46%
Placebo + docetaxel(n=207)
Bevacizumab 15 mg/kg q3w +
docetaxel(n=206)
64%
p=0.0003
AVADO: Overall Response Ratea (Bevacizumab 15 mg/kg q3w)

Goals of Therapy
Minimize toxicity from treatment

Bleeding/hemorrage
• Serious hemorragic events (grade ≥ 3) were uncommon≤ 1.7% of patients in the bevacizumab arms
(only in the taxane-BV arm of RIBBON-1: 5.4%)
• Trials allowed use of anticoagulants and aspirin
• Exploratory analysis of AVADO data– No CNS bleeding events in pts who developed brain metastases
while on study
Hamilton EP & Blackwell KI. Oncology 2011; 80: 314-25

Wound-healing complications• Incidence of grade 3 or 4 wound-healing
complications≤ 1.5% of patients in the bevacizumab arms≤ 1% of patients in the control arms
• Interval between bevacizumab administration and elective surgery– Based on 20-day half-life– Do not administer bevacizumab at least 4 weeks
before and 4 weeks after surgery
Hamilton EP & Blackwell KI. Oncology 2011; 80: 314-25

Thromboembolic events
• Arterial thrombotic events– Twice as frequently in patients treated with
bevacizumab• 3.8% vs. 1.7% (meta-analysis of trials in mCRC,
MBC, NSCLC)
• No increased risk for venous thromboembolic events
Hamilton EP & Blackwell KI. Oncology 2011; 80: 314-25

When Meta-analyses add little to our body of evidence:
Bevacizumab and Heart Failure Risk• Retrospectively collected heart
failure data
• Lack of information about individual patients
• No information about underlying risk factors
– Cumulative anthracycline dose– Prior radiation– Atherosclerotic disease– Hypertension/Diabetes/Obesity
• Lack of accurate definition of heart failure
– Heart failure is not equilavent to cardiomyopathy or to left ventricular dysfunction
Verma & Swain, J Clin Oncol 2011
• TRIALS– Miller JCO 2005– E2100– AVADO– RIBBON-1– RIBBON-2
• Bevacizumab in pts with MBC increase the risk of G3-4 CHF five-fold with an overall incidence of 1.6% (vs 0.4% in the control/placebo group)
Choueri, J Clin Oncol 2011

Cardiovascular events
• RIBBON-1 is the only phase III trial including a prospective cardiac evaluation– No significant increase of grade ≥ 2 left
ventricular systolic dysfunction when bevacizumab was combined with anthracyclines • 6.2% vs. 6%, respectively, at the primary
data cut
Robert NJ, et al. J Clin Oncol 2011

To understand the
risk/benefit ratio

Clinical benefit and molecular heterogeneity of breast cancer
ORR/PFS
Survival
unselected population
• Predictors of response/PFS may not predict OS in unselected cases• A single predictive biomarker cannot fit all tumor types

Clinical benefit and molecular heterogeneity of breast cancer
Population A
Population C
Population B
ORR/PFS
Survival
unselected population
• Predictors of response/PFS may not predict OS in unselected cases• A single predictive biomarker cannot fit all tumor types
chemotherapy