Embed Size (px)
Citation preview

Introduction
Idiopathic hypertrophic pachymeningitis, a rare entity,is essentially a diagnosis of exclusion. Few cases havebeen reported [1–4]. We present four cases in which theclinical presentation was very varied.
Subjects and methods
We reviewed the clinical and imaging data of four patients labelledas having idiopathic hypertrophic pachymeningitis. In two con-trast-enhanced CT and in all four MRI before and after contrastmedium had been performed, the latter at 0.5 T or 1.5 T. T1- andT2-weighted images were obtained in different planes. In addition,MR angiography and venography had been performed in threepatients. Follow-up MRI was available in three patients. Open bi-opsy of the meninges had been performed in two.
Case reports (Table 1)Case 1
A 28-year-old man was admitted with progressive cranial nervepalsies over 2 years. At first there was involvement of the left I, IIand VI followed by the right I and then left II and VII–XII cranialnerves. Examination revealed no other significant finding; there
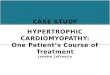
was no evidence of raised intracranial pressure. CT showed prom-inent contrast enhancement of the tentorium. To elucidate thisfinding MRI was performed, which showed extensive thickeningand enhancement of the pachymeninges (Fig. 1a). The MR angi-ography (MRA) and venography (MRV) were normal. Biopsy ofthe thickened pachymeninges revealed nonspecific inflamma-tion. The patient was discharged on steroids. MRI 2 years later(Fig. 1b–e) showed increase in the pachymeningeal thickeningwith commensurate clinical deterioration.
Case 2
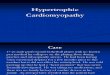
A previously healthy 62-year-old woman presented with headachefor 2 years, diplopia and visual loss for 5 months, and nasal regur-gitation and dysphagia for 2 months. Examination revealed left VI,IX, X and XII cranial nerve palsies. CT head (Fig. 2a) showedmarked contrast enhancement of the tentorium. MRI (Fig. 2b, c)and MRV revealed diffuse thickening and enhancement of thedura mater, including the tentorium; the dural sinuses were patent.A provisional diagnosis of hypertrophic pachymeningitis was en-tertained and open meningeal biopsy was performed. Histopatho-logical study revealed marked thickening and fibrosis of the duramater. The patient was discharged on steroids, and readmitted3 months later. There was subjective improvement of 90 % in thecranial nerve palsies, but vision in the left eye was unchanged. MRI(Fig. 2d, e) revealed significant reduction in the pachymeningealthickening and contrast enhancement.
Neuroradiology (1997) 39: 619–623 Springer-Verlag 1997 DIAGNOSTIC NEURORADIOLOGY
M. GoyalA. MalikN. K. MishraS.B.Gaikwad
Idiopathic hypertrophic pachymeningitis:spectrum of the disease
Received: 4 July 1996Accepted: 1 November 1996
M. Goyal ⋅ A.Malik ⋅ N.K. Mishra ⋅S.B.GaikwadDepartment of Neuroradiology,Neurosciences Centre,All India Institute of Medical Sciences,New Delhi, India 110029
Abstract Hypertrophic pachymen-ingitis is extremely rare. It is a fi-brosing inflammatory process whichinvolves the dura mater, includingthe tentorium. Numerous patholog-ical entities produce thickening ofthe pachymeninges, so that idopath-ic hypertrophic pachymeningitis is adiagnosis of exclusion. We describefour patients with idiopathic hyper-trophic pachymeningitis who had
varied clinical presentation. Imagingstudies revealed diffuse thickeningof the pachymeninges; in one pa-tient there was extensive dural sinusthrombosis. Since no identifiablecause was found, the cases were la-belled as idiopathic.
Key words Idiopathic hypertrophicpachymeningitis ⋅ Magneticresonance imaging

Case 3
A 34-year-old woman presented with a history of fever, proptosisand loss of vision in the right eye of 3 years duration. Recurrentepisodes of diminution of vision in the right eye improved on ste-roid therapy. In addition, she had had a right sided VII nerve palsy.On examination, there was proptosis, papilloedema, and optic at-rophy on the right, and a residual right facial weakness. A clinicaldiagnosis of right orbital pseudotumour was entertained. MRI(Fig. 3a) revealed diffuse thickening of the pachymeninges, withthickening of the superior rectus muscle suggestive of pseudotu-mour in the right orbit. MRI (Fig. 3b) after 1 month showed sig-nificant reduction in the extent of the orbital pseudotumour. Thepachymeningeal thickening, however, did not show any apprecia-ble change.
Case 4
A 19-year-old woman presented with fever for 3 weeks and head-ache and vomiting for 2 weeks. She was drowsy, with nuchal rigidityand bilateral papilloedema. Cerebrospinal fluid examination wasnormal. MRI and MRV revealed pachymeningeal thickening anddural sinus thrombosis (Fig. 4). The general condition of the patientdid not permit open biopsy of the meninges, although there was noevidence of systemic inflammation. The patient was started on sup-portive therapy for dural sinus thrombosis and is being followed.
There was no evidence of any systemic inflammatory disease inany of our patients, although in each case the sedimentation ratewas increased. No evidence of conditions known to cause pachy-meningeal thickening was found. There was also no evidence ofimmunosuppression or features suggestive of HIV infection. Noneof our patient had undergone dialysis. Cerebrospinal fluid exam-inations were normal.
Discussion
Pachymeningitis is a term used to define the state inwhich there is localised or diffuse thickening of the duramater, usually adjacent to an inflammatory focus.Causes of dural thickening include epidural abscess,rheumatoid arthritis, lymphoma, neurosyphilis, sarcoi-dosis, tuberculosis and intracranial fibromatosis. HTLV-1 infection and chronic dialysis have also been reported
620
a b
c
d e
Fig. 1a–e Case 1. a Contrastenhanced sagittal MRI reveal-ing thickening and enhance-ment of the dura mater. Noteextension into the upper cervi-cal spine (arrow). b T1-weight-ed sagittal image 2 years latershowing markedly thickeneddura mater on the dorsal aspectof the clivus with extension intoupper cervical spine. c T2-weighted axial image showinglow-signal, thickened tentori-um. d,e Sagittal and parasagit-tal contrast-enhanced imageshomogeneously enhancingdura mater, including tentori-um

to cause granulomatous thickening of the pachymenin-ges [5, 6]. Idiopathic hypertrophic pachymeningitis isthus a diagnosis of exclusion. It may extend to involvethe skull base and adjacent tissues. Pathologically, thereis diffuse thickening of the dura mater with considerable
fibrosis; chronic inflammatory cells including plasmacells and lymphocytes are seen on microscopy. Gener-ally, there is elevation of the erythrocyte sedimentationrate, and cerebrospinal fluid studies divulge elevatedlevels of cells and protein.
621
a b c
d e
Fig. 2a–e Case 2. a CT show-ing dense contrast enhance-ment of the tentorium.b, c Contrast-enhanced axialand parasagittal MRI revealingenhancing, thickened tentori-um and dura mater. d,e Similarimages 3 months later showingsignificant reduction in thethickening and extent of en-hancement of the pachymenin-ges
Table 1 Clinical profile, radilogical findings and follow-up
Age (years)/sex
Presentation Neurological findings Radiological findings Biopsy Treatment Follow-up
28/F Multiple lower cranialnerve palsies
Left I, II, VI–XII, right Icranial nerve palsies
Thickened pachy-meninges at base of skull
Yes Steroids Deteriorated
62/M Multiple cranial nervepalsies
Left VI, IX, X, XII cranialnerve palsies
Thickened pachy-meninges
Yes Steroids Improved
39/F Recurrent episodes ofproptosis and reducedvision right eye
Papilloedema and opticatrophy right eye,right VII palsy
Right orbital pseudo-tumour with pachy-meningeal thickening
No Steroids Improved
19/F Fever 3 weeks, headacheand vomiting 2 weeks
Bilateral papilloedema,neck rigidity
Dural sinus thrombosisand pachymeningealthickening
No Steroids Not available

Clinical presentation is inconstant and nonspecific.The disease commonly presents with longstandingheadache. Due to compression of the cranial nervesat the skull base by the thickened pachymeninges,the patient may present with multiple cranial nervepalsies or blindness, as in three of our patients. In-ternal carotid artery occlusion has also been reported[3]. Due to the proximity of the dura mater to thevenous sinuses, the process of fibrosis can also causeocclusion of the sinuses. This has been reported pre-
viously [1, 2], and was documented in one of ourcase.
The thickened dura mater appears isointense on T1-weighted images, and gives low signal on T2 weighting.The thickening is better appreciated on coronal andsagittal images than on axial images. There is uniform,dense contrast enhancement of the thickened mem-branes. The changes, unless marked, are comparativelydifficult to appreciate on CT; the thickened dura materis best appreciated adjacent to the tentorial hiatus oncontrast-enhanced CT. Normal meninges are usuallyinvisible on MRI without contrast medium, but may beseen on gadolinium-enhanced T1-weighted images[10].
Pachymeningeal thickening may in isolation involvethe spinal dura mater, leading to cord compression. Inpatients 1 and 2 the dural thickening was seen to extend
622
a b
Fig. 3a, b Case 3. a T1-weight-ed coronal image showing iso-intense, ill-defined mass in thesuperolateral quadrant of theright orbit and thickened supe-rior rectus muscle with bilater-ally thickened dura mater in theanterior cranial fossa. b Con-trast-enhanced image showinghomogeneous enhancement ofthe right orbital mass and thepachymeninges of the entirecranial cavity
a b c
Fig. 4 Case 4. a T1-weighted sagittal image showing absence offlow void in the dural venous sinuses suggestive of thrombosis.b, c Contrast-enhanced axial and coronal images revealing deltasign in the superior sagittal sinus. Note markedly thickened, en-hancing dura mater bilaterally

to the upper cervical spine from the posterior cranialfossa.
Hypertrophic spinal pachymeningitis with coexistentpulmonary nodule formation has been reported [7].Histopathological examination of the dura mater, liga-menta flava and pleural-based lung nodule showed adiffuse, chronic inflammatory process with marked fi-brosis. There was considerable clinical improvementwith immunosuppressive therapy. The authors suggest-ed that spinal pachymeningitis is probably related to id-iopathic systemic inflammation diseases. No evidence ofsystemic inflammation was present in our patients ex-cept for orbital pseudotumour in one patient.
Pachymeningeal thickening has been reported withorbital pseudotumour in a case of multifocal fibroscle-rosis [8]. Larger series of orbital pseudotumour haveindicated that intracranial extension, often of modestdegree, is in fact relatively common [9]. Orbital pseu-dotumour with diffuse pachymeningeal thickening wasseen in our case; however, there was no systemic evi-dence to suggest the diagnosis of multifocal fibrosclero-sis. It is, however, possible that the pachymeningealthickening was an early indication of fibrosclerosis.
Meningioma en plaque and tuberculoma en plaque[10] may produce thickening of the pachymeninges;however, the involvement is focal rather than genera-
lised and the clinical presentation is usually as a conse-quence of a mass rather than entrapment of nerves andvessels.
Pachymeningeal thickening in the posterior cranialfossa has been reported to result in hydrocephalus [11].There was no evidence of hydrocephalus in any of ourcases.
Intense enhancement of the normal dura mater fol-lowing gadolinium injection has been seen in cases ofintracranial hypotension, and may lead to an erroneousdiagnosis of hypertrophic pachymeningitis. However,the patients usually present with headache, and themarked dural enhancement resolves with treatment ofthe intracranial hypotension [12].
The natural course of pachymeningeal thickening isunknown. Spontaneous resolution has been reported[13]. The patient may show an initially good response tosteroid therapy, as in our cases 2 and 3. However, thereis a risk of steroid dependence. Although there are noverified clinical trials, immunosuppressive therapy hasresulted in clinical improvement [1, 7].
The varied presentation, in the absence of an identi-fiable cause, can lead to diagnostic dilemmas. We be-lieve that in such situations meningeal biopsy should beperformed to resolve the issue, and to understand thepathogenesis and natural course of the disease better.
623
References
1. Martin N, Masson C, Henin D, Mom-pint D, Marsult C, Nahum H (1989)Hypertrophic cranial pachymeningitis:assessment with CT and MR Imaging.AJNR 10: 477–484
2. Kioumer F, Au A, Rooholamini SA,Yaghmai I, Verma R (1994) Idiopathichypertrophic cranial pachymeningitis: acase report. Neuroradiology 36: 292–294
3. Willing SJ, Broghamer W (1992) Inter-nal carotid artery occlusion due to idio-pathic cranial pachymeningitis. AJNR13: 1594–1596
4. Uemura K, Matsumura A, Kobayashi E(1995) Idiopathic chronic hypertrophiccraniocervical pachymeningitis: casereport. Neurosurgery 37: 358
5. Kawano Y, Kira J (1995) Chronic hy-pertrophic cranial pachymeningitis as-sociated with HTLV-1 infection. J Neu-rol Neurosurg Psychiatry 59: 435–437
6. Feringa ER, Weatherbee L (1975) Hy-pertrophic granulomatous cranialpachymeningitis causing progressiveblindness in a chronic dialysis patient. JNeurol Neurosurg Psychiatry 38: 1170–1176
7. Adler JR, Sheridan W, Kosek J, LinderS (1991) Pachymeningitis associatedwith a pulmonary nodule. Neurosurgery29: 283–287
8. Berger JR, Snograss S, Glaser J, PostMJD, Norenberg M, Benedetto P(1989) Multifocal fibrosclerosis withhypertrophic intracranial pachymenin-gitis. Neurology 39: 1345–1349
9. Clifton AG, Borgstein RL, Moseley IF,Kendall BE, Show PJ (1992) Intracra-nial extension of orbital pseudotumour.Clin Radiol 45: 23–26
10. Lindner A, Schneider C, Hofmann E,Soerensen N, Toyka KV (1995) Isolatedmeningeal tuberculoma mimickingmeningioma: case report. Surg Neurol43: 81–84
11. Oku T, Yamashita M, Inoue T et al.(1995) A case of posterior fossahypertrophic pachymeningitis withhydrocephalus. No To Shinkei 47: 569–573
12. Mokri B, Parisi JE, Scheithauer BW,Piepgras DG, Miller GM (1995) Men-ingeal biopsy in intracranial hypoten-sion: meningeal enhancement on MRI.Neurology 45: 1801–1807
13. Nishio S, Morioka T, Togowa A et al.(1995) Spontaneous resolution of hy-pertrophic cranial pachymeningitis.Neurosurg Rev 18: 201–204

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具


























![GENETIC BASIS OF HYPERTROPHIC CARDIOMYOPATHYThroughout the years, names such as idiopathic hypertrophic subaortic stenosis[5], muscular subaortic stenosis[6] and hypertrophic obstructive](https://img.pdfslide.us/doc/110x75/60571329c95e4748070a14f6/genetic-basis-of-hypertrophic-cardiomyopathy-throughout-the-years-names-such-as.jpg)