Embed Size (px)
Citation preview

Running Head: Mobile Integrated Health 1
Identifying Additional Focus Areas for Las Cruces Fire Department’s Mobile Integrated Health
Program
Michael N. Daniels
Las Cruces Fire Department, Las Cruces, New Mexico
MOBILE INTEGRATED HEALTH 2
Certification Statement
I hereby certify that this paper constitutes my own product, that where the language of others is
set forth, quotation marks so indicate, and that appropriate credit is given where I have used
language, ideas, expressions, or writings of another.
Signed: _______________________________________
Michael N. Daniels
MOBILE INTEGRATED HEALTH 3
Abstract
The Las Cruces Fire Department (LCFD) implemented a Mobile Integrated Health Program
(MIH) in 2015 to reduce repeat 911 calls. The problem was LCFD had not formally identified
additional focus areas for the expansion of the MIH program. The purpose of this research was to
identify MIH focus areas relevant to LCFD and the City of Las Cruces and identify the
characteristics of successful MIH programs. Descriptive research methodologies were utilized to
complete this research. The research conducted as part of this applied research project (ARP)
sought to answer the following question: a) What are the characteristics of a successful Mobile
Integrated Health program? b) What focus areas are other Mobile Integrated Health programs
addressing in their communities? c) Which identified incident types or focus areas are risks for
the Las Cruces community that can be addressed by the Mobile Integrated Health program? The
literature review sought to identify the characteristics of successful MIH programs and current
focus areas outside of Las Cruces. The procedures used as for this research included two surveys
and a review of incident data for the City of Las Cruces. The surveys targeted outside
organizations and local providers to identify additional MIH focus areas and the perceived
effectiveness of those focus areas in Las Cruces. The research identified current MIH focus areas
and the key characteristics and recommendations for MIH program development. The
recommendations made were to conduct a review of the costs of current services to identify the
costs and benefits of expanding focus areas. The second recommendation was to identify clear
program objectives for the focus areas as identified in the successful characteristics of MIH
programs. Lastly, it was recommended that the focus areas be identified at a community level
and not just programs that are for the benefit of LCFD.
MOBILE INTEGRATED HEALTH 4
Table of Contents
Certification Statement……………………………………………….…………………………...2
Abstract……………………………………………………………………………………………3
Table of Contents………………………………………………………………………………….4
Introduction…………………………………………………………………………………….….6
Background and Significance…………………………………………….………………...……...7
Literature Review…………………………………………….………………………………..…13
Procedures………………………………………………………………………………………..26
Results...………………………………………………………………………………………….31
Discussion………………………………………………………………………………………..45
Recommendations………………………………………………………………………………..51
References………………………………………………………………………………………..54
Table of Figures
Figure 1: ………………………………….…………………….………………………………..34
Figure 2: …………………………………………...…………………………………………….35
Figure 3: ………………….…………………………………….………………………………..36
Figure 4: …………………………….………………...…………………………………………38
MOBILE INTEGRATED HEALTH 5
Table of Tables
Table 1: ………………………………………………………………………………………….37
Table 2: ……………………………...…………….…………………………………………….39
Table 3: ………………………………...………..………………………………………….…...40
Table 4: …………………………..……………….. ……………………………………………41
Table 5: …………………………...……………………………………………………………..42
Table 6: ………………………………………………………………………………………….43
Table 7: ………………………………………………………………………………………….44
Appendices
Appendix A: MIH/CP Survey………………….………….…………………………………….61
Appendix B: Queued Incident Types by Year…………………………………………………..64
Appendix C: Queued Condition Codes by Year……………………….………………………..65
Appendix D: Las Cruces Overdose and Psychiatric Incidents.…………………………….……67
Appendix E: Las Cruces Falls and Lift Assists…………………………………………….……68
Appendix F: Preventable/Unnecessary Emergency Room Visits………………………….……69

MOBILE INTEGRATED HEALTH 6
Improving Quality of Life for the Citizens of Las Cruces: Evaluating the Effectiveness of the Las
Cruces Fire Department’s Mobile Integrated Health Program
Introduction
In recent years, mobile integrated health (MIH) or community paramedicine has been a
favored subject in the fire service. The thought of community risk reduction from a broader
community perspective outside of preventing fire alone has helped contribute to this, along with
the financial benefits of hedging call volume growth for repeat 911 use and the potential for
reimbursement under the Patient Portability and Health Care Act of 2010 for preventing
unnecessary readmissions (Brown, 2015).
In 2015, the Las Cruces Fire Department began researching the feasibility of
implementing a mobile integrated health (MIH) program. Following the feasibility study and
implementation review, the MIH program was implemented in September 2016. The focus of the
program was to reduce the impact of those who repeatedly use the 911 system for primary care
issues that can be managed more appropriately through other means. Since the program’s
implementation, there has been a discussion on expanding the role of MIH beyond repeat 911
use. The problem is that the MIH program has not evaluated other focus areas for expansions
compared to the specific needs of the citizens of Las Cruces. The purpose of this research is to
identify other areas of focus that are reflective of the community’s needs.
Descriptive research methodologies will be used to identify focus areas that other
MIH/CP programs are using, comparing them to the call types and identified needs within the
City of Las Cruces, and evaluating the costs and benefits of each focus area by answering the
following research questions:
MOBILE INTEGRATED HEALTH 7
a. What are the characteristics of a successful Mobile Integrated Health program?
b. What focus areas are other Mobile Integrated Health programs addressing in their
communities?
c. Which identified incident types or focus areas are risks for the Las Cruces community
that can be addressed by the Mobile Integrated Health program?
Background and Significance
The City of Las Cruces covers over 76 square miles in South Central New Mexico and
according to the United States Census Bureau (2017), as of July 2017, Las Cruces, NM had an
estimated population of 101,712, an increase from 97,618 in 2010. The LCFD responded to
approximately 17,000 calls for service from July 1, 2015 through June 30, 2016 (City of Las
Cruces, 2016). It is the second largest city in the state of New Mexico and surrounded by several
volunteer and combination departments. The closest career municipal department is the El Paso
Fire Department over 40 miles from Las Cruces. There are an estimated 60,605 citizens over 25,
and nearly 35 percent of them have no college with 14.56 percent not graduating high school and
the other 19.46 percent having only a high school diploma/equivalent (USA.com, 2014).
Additionally, according to USA.com (2014), approximately 23.88 percent of Las Cruces’
population lives in poverty, compared to 20.88 percent and 15.59 percent across New Mexico
and the United States, respectively.
The LCFD is an Insurance Service Organization (ISO) Class 1, all-hazards organization,
serving the City of Las Cruces by providing primary fire response, fire prevention, emergency
medical services, hazardous materials response, technical rescue, airport rescue and firefighting,
and a Mobile Integrated Health (MIH) program. The organization is operated through two
MOBILE INTEGRATED HEALTH 8
divisions, Operations and Administration. Each division is managed by a deputy chief assigned
directly under the fire chief. The Operations Division consists of response personnel operating on
three shifts working a 24-hour on and 48-hour off schedule. There are eight stations with two
battalion chiefs and ten lieutenants per shift. The lieutenants manage crews consisting of three to
four personnel per unit. There are eight engine companies, two truck companies and two
transport capable squads in operations. The Administrative Division consists of operational
support, training, prevention, and emergency medical services. The Emergency Medical Services
Division is managed by a battalion chief who is the direct supervisor of the Mobile Integrated
Health program. The LCFD has strived to improve response models and service delivery as an
organization continually. The effort is exemplified by the addition of two-person squads that are
transport-capable and serve a dual purpose of transporting in case the private ambulance system
is unavailable in the Las Cruces city limits and alleviating four-person companies in responding
to an incident where only two people are needed. Also, the LCFD has implemented alternate
response vehicles (ARV’s), that are staffed by Truck Company crews to respond to calls where
the aerial apparatus is not needed, decreasing wear and tear on the unit. The result of each of
these has shown benefits with reduced response times and wear and tear on the apparatus where
squads and ARV’s are located.
In 2016, the LCFD implemented the MIH program with the primary goal reducing repeat
unnecessary 911 calls by evaluating the candidate’s needs and helping them access the
healthcare system or social programs in a manner that meets their specific requirements. The
MIH coordinator helps with access to primary care, referrals, and has even helped obtain access
ramps for wheelchair-bound citizens with the overarching goal of improving quality of life for
those in need and reducing the need for 911 response in preventable situations. The MIH office
MOBILE INTEGRATED HEALTH 9
is operated Monday through Friday by a single firefighter temporarily assigned to the program
based on his interest in the subject area. The MIH program candidates are identified by
operations crews who notice increased 911 usage for situations that appear to be poor healthcare
system access or other social conditions. While writing the report after the incident, the report
writer can select whether the individual is a candidate for the MIH program. The MIH
coordinator evaluates all candidates that are identified by operations personnel and placed on a
candidate list for follow up.
Regular audits of responses are performed based on incident address and person involved
as a means of proactively identifying repeat 911 users that may not have been identified by
operations personnel. As openings in the MIH program become available, the identified
individuals are screened to see if they need services that can be provided more effectively than
the emergency response system. There are also referrals from outside agencies to the program
where community partners identify citizens who may benefit from the resources available
through the MIH program. Such references often come from Adult Protective Services or home
health agencies that identify a client with social needs they cannot provide. In these cases,
LCFD’s MIH coordinator will seek solutions the MIH client’s problem such as building a wheel
chair ramp with union personnel. The original template has morphed to include referrals who
have never accessed the 911 system, yet still have needs that are not being met, leading to a
significant amount of scope creep from the original intent. LCFD’s MIH program to date
receives nearly 90 percent of its referrals outside of excessive 911 calls (P. Ford, personal
communication, December 10, 2018).
In August 2018, the MIH program received $50,000 from a local insurance carrier as part
of a cooperative pilot program to follow up with patients and see if they had any healthcare

MOBILE INTEGRATED HEALTH 10
needs that were not being met. The overall purpose is to help them navigate the healthcare
system and available services as a means of decreasing unnecessary emergency room visits. Of
the $50,000 allotment, $10,000 was for the purchase of the software needed by the program to
accurately track the program candidates and the remaining $40,000 to cover the associated cost
of bringing operations personnel in on overtime to help with patient follow-up. This agreement is
a one-time agreement that the LCFD hopes will trigger additional interest from other insurance
companies seeking to reduce unnecessary 911 access and improvement in the quality of care. In
late 2018, the initial success of the program was once again exemplified as a local health care
provider approached the organization on the willingness of LCFD to begin a post-discharge
follow-up for congestive heart failure (CHF) pilot program that would help fund the efforts of
the LCFD in maintaining the MIH program. Details of the pilot program were not released as of
the writing of this research but highlight the significance of LCFD needing to evaluate what
additional focus areas would be best suited for LCFD to consider adopting.
In discussion with Firefighter Paul Ford, the LCFD’s MIH Coordinator, there have been
77 people admitted to the LCFD’s MIH Program in addition to countless referrals without
admission since the program’s implementation in 2016. Additionally, of the 77 people admitted
to the program, not all of them have been high utilizers as many have been citizens with unmet
social needs or living in unsafe conditions. This has led to a significant increase in workload
without measurable benchmarks as the ancillary services provided to the end-user were not part
of the original program design but have been accepted by the organization. The acceptance of
such services, despite the lack of measurement tools or benchmarks, has been promoted as a
means of reducing community risk and increasing overall health as issues are identified, thus
preventing the potential for subsequent 911 use should the individual’s health deteriorate with
MOBILE INTEGRATED HEALTH 11
the social gaps present. Of the high utilizers of 911 enrolled in the MIH Program, there has been
a decrease of 74.8 percent in calls from six months before admission as compared to 6 months
after entry. Of the calls post admission, one individual who has significant needs has accounted
for nearly 50 percent of them. Most of the individuals enrolled have shown a decrease in overall
call volume to a range closer to 90-100 percent (P. Ford, personal communication, December 10,
2018).
In discussion with LCFD’s Fire Chief Eric Enriquez on November 20, 2018, he
expressed his observations on how the efforts of the MIH program have already begun to show
success in improving the overall quality of life of the citizens of Las Cruces, which is the
program’s primary goal. Increased 911 access was merely the means of identifying who may
need an alternative approach to solving their issues, as the continued use by a group of
individuals can help us point out where our citizens and community’s social system is struggling
to meet their needs. He expressed this is where LCFD fits in as the fire service has access to
those in need either personally or through data gathered by LCFD or other stakeholders willing
to share the information. He also expressed the decreased use of 911 by those who could be
served better through alternate service delivery models has allowed more time for operations
crews to train, making them better prepared to respond to other emergencies, further
exemplifying the benefits of MIH. Additionally, the LCFD has been contacted by private
organizations seeking public-private partnerships that can help improve the overall quality of life
for the citizens, as well as the healthcare system’s funds distributions (E. Enriquez, personal
communication, November 20, 2018).
The United States Fire Administration (USFA) maintains a strategic plan that is focused
on five strategic goals with a mission that reads “We provide national leadership to foster a solid
MOBILE INTEGRATED HEALTH 12
foundation for our fire and emergency services stakeholders in prevention, preparedness and
response” (USFA, 2014, p.8). MIH programs directly align with the first strategic goal of the
USFA to “Promote response, local planning, and preparedness for all hazards” and the third
strategic goal “Enhance the fire and emergency services’ capability for response to and recovery
from all hazards” (USFA, 2014, p. 9). Understanding community risks and helping the
community’s citizens live healthier lives through supporting integrated health solutions can have
a significant effect on promoting response since units can be more available for critical responses
within their respective districts in the City of Las Cruces. Additionally, money saved in
decreased unnecessary 911 access may help cities and states respond more effectively through
more effective distribution of public health funds.
This research aligns with the Executive Analysis of Community Risk Reduction
(EACRR) course. The goal of EACRR is to improve executive abilities in multi-hazard
community risk reduction, and strategic community risk reduction for both the citizens and
firefighters in the community (National Fire Academy [NFA], 2018). The LCFD’s MIH program
is geared toward identifying at-risk citizens and providing them a service that is geared toward
meeting their specific needs, thus reducing the impact of inefficient systems and increasing the
effective response at emergency incidents through increased availability.
Failing to evaluate the areas where the City of Las Cruces and LCFD can expand their
focus areas in MIH may lead to decreased effectiveness in reducing community risk proactively.
Additionally, failing to evaluate areas of expansion can lead to further additions of services that
are not aligned with the program’s scope or measured for success, decreasing the potential for
support by community stakeholders. Not proactively addressing the needs of the citizens
prevents the LCFD from improving their quality of life by preventing follow-up incidents as well

MOBILE INTEGRATED HEALTH 13
as the progression to 911 use and decreased overall quality of life. Additionally, the community’s
increased demand of fire department services may begin to outpace the growth and capacity of
the LCFD to effectively respond to community needs, stretching the fire department’s critical
resources because of a dated response model for dealing with non-emergent citizen needs.
Literature Review
A literature review was performed to evaluate current information related to mobile
integrated healthcare, community paramedicine, integrated health strategies. Additionally, the
literature review sought to identify the characteristics of successful MIH programs. Despite the
infancy of mobile integrated health programs and the variability in how or why they are
administered in the United States, there was a significant amount of literature available. The
search keywords used in Google and on the National Fire Academy Learning Resource Center’s
search bar were “community paramedic, community paramedicine, and mobile integrated
health.” The results were then limited to textbooks, journal articles/studies, and Executive Fire
Officer Applied Research Projects. Community specific information in addition to journal
articles, websites and books were reviewed and provided insight into MIH in the City of Las
Cruces. The literature is divided into three sections. The first section is an introduction into MIH
and how it became relevant in the United States. The second section pertains to question A and
the third section to questions B and C of this ARP.
MIH in the United States
The current healthcare system in the United States has continued to struggle from poor
management, which has led to increased fragmentation where providers operate in silos that have
no accountability to others, leading to an environment that is not conducive to improving overall

MOBILE INTEGRATED HEALTH 14
patient health, but geared toward profitability of the individual provider (Strange, 2009). It has
been a system designed around illnesses and conditions that are treated separately irrespective of
other determinants, failing to recognize the relationship between illnesses such as the impact of
mental health illnesses coupled with other chronic illnesses (Stanhope, Videka, Thorning, &
McKay, 2015). An example portrayed by Druss and Walker (2011) is how 68 percent of those
with mental health illnesses also have medical conditions, and how the treatment of chronic
medical conditions are an average 560 dollars more per visit than those without associated
mental health illnesses. Additionally, access to care has continued to be difficult, affecting the
country’s most vulnerable population, the homebound elderly, where there were approximately
922,000 of them in the United States in 2011 (O’Brian, 2017). Of those, it is estimated that less
than 12 percent of them receive primary health services in the home, leaving the remainder
without the adequate care needed to adequately sustain their health (Ornstein et al., 2015). It was
further evidenced that homebound elderly suffer from as much as two times the chronic medical
conditions and a significantly higher likelihood of being hospitalized due to the lack of regular
care, than those that are not homebound (Ornstein et al., 2015).
Healthcare reform in recent years has been geared toward improving patient experiences,
overall population health, and per capita healthcare costs through integration, also referred to as
triple aim (Stanhope et al., 2015). Integrated healthcare is defined by the Waddington and Egger
(2008) as “the organization and management of health services so that people get the care they
need, when they need it, in ways that are user-friendly, achieve the desired results and provide
value for money” (p. 5). The integrated approach seeks to address healthcare by emphasizing
population-based care and service availability with emphasis on prevention and care
collaboration across providers, reducing the impact of episodic illness-oriented care models
MOBILE INTEGRATED HEALTH 15
(Stanhope et al., 2015). The foundations of integrated healthcare are not recent, however, the
focus on integration was sparked by its emphasis in the Patient Portability and Accountability
Act of 2010 (PPACA) as well as the recognition of the need to assist patients in navigating the
healthcare system (Stanhope et al. 2015). Morganti, Alpert, Margolis, Wasserman, and
Kellerman (2014), reported that EMS care which resulted in appropriate levels of care in instead
of automatic transport to an emergency room could decrease overall Medicare costs ranging
from $283-$560 million per year.
The fire service has also been plagued with inefficiencies that are the result of operating
in the box of equal resource distribution (Boyd, 2009). The use of equal distribution principles
for all appears to almost always result in decreased efficiency where positive outcomes are
realized for some, but many others are left with poor outcomes (Boyd, 2009). Boyd (2009) states
“To date, fire if any emergency service organizations have explored the factors that drive
demand for those resources to guide locational decisions that might improve service delivery” (p.
1). It begs the question of whether the standard model for fire-based EMS deployment is the best
practice? As of 2015, over 60 percent of the nation’s fire departments provided some form of
EMS (Haynes & Stein, 2017). The current state must be challenged, and fire departments need to
ensure they understand the importance of sending the right number of resources are sent to an
incident rather than continuing to send everyone, all the time (Kostyrka, 2018). Fire service
expenditures have increased 170 percent from 1984 to 2014 after adjusting for inflation in 2015
dollars (Haynes & Stein, 2017). Risk-based approaches to planning that take into account
functionality tend to make the best possible uses if scarce resources (Canton, 2013). “As we
move into the future, more concentration should be placed on patient outcomes, patient
satisfaction, and transporting patients where the need to go for the best care” (Kostyrka, 2018, p.
MOBILE INTEGRATED HEALTH 16
11). The topic of efficient use of resources leads to discussions on community risk reduction
strategies that can be applied in healthcare and EMS, or MIH. EMS is uniquely positioned to
make significant impacts in ensuring the right care at the right time in the right setting (Zavadsky
& Hooten, 2016).
“Mobile integrated healthcare (MIH) is the provision of healthcare using patient-
centered, mobile resources in the out-of-hospital environment that are integrated with the entire
spectrum of healthcare and social service resources available in the local community” (Zavadsky
& Hooten, 2016, p. 11). The realm of MIH can be broad from a national perspective, but highly
specific to the individual community’s needs under this definition, not only providing but also
assisting in the coordination and management of care. It is a program that consists of a multi-
professional clinical team, creating a needs-matched system that not only results in patient
satisfaction, but also increased efficiency in care, and decreased overall healthcare costs
(Castillo, Myers, Mocko, & Beck, 2016). MIH efforts that are researched and developed to
target community subpopulations with the highest risk as compared to a generalized approach
were shown to yield the greatest overall results (Castillo et al., 2016). This observation is
supported by National Institute for Health Care Management or NIHCM (2012) in the estimation
that five percent of the population accounts for half of the nearly $1.8 trillion spent annually on
healthcare in the United States, reflecting an opportunity in the healthcare community to
capitalize from targeted efforts at reducing unnecessary healthcare expenditures.
Mobile integrated health or community paramedicine programs have been adopted by
prehospital providers to address the continued increase in demand of the 911 system for non-
emergent needs (Stowell, 2016). The increases in prehospital provider demand or 911 access,
according to Stowell (2016), are because those in need are uninsured and the 911 system will
MOBILE INTEGRATED HEALTH 17
facilitate access to care, or they have insurance but do not know how to access care. In either
situation, whether the patient is knowingly accessing the system inappropriately or not, an
inefficient response is likely to occur if traditional prehospital response models are utilized
(Stowell, 2016). Such responses often yield a trip to the emergency room where the patient is
later released with an order to follow up with their primary care physician or a specialist with
little to no direction on how to coordinate such care. When the patient does not follow up as
ordered, and their condition isn’t improved, another 911 call is likely to occur. The complex
healthcare system is a source of frustration and the ticket to alleviate those frustrations, at least
for the short term, is to call 911 or go to the emergency room for primary care (Zavadsky &
Hooten, 2016).
The number of MIH/CP programs has continued to grow in the United States with more
than 100 MIH/CP programs across the United States known as of 2014, and over 50 percent of
those having started within the previous year, according to a report published by the National
Association of Emergency Medical Technicians (NAEMT) (NAEMT, 2015). In 2017, a second
survey was published by the NAEMT reporting over 200 MIH/CP programs that were operating
across the United States (NAEMT, 2018). Public organizations have become the primary
providers of MIH/CP programs, accounting for over 60 percent of all MIH/CP programs, and
fire-based programs accounting for over 30 percent of all programs (NAEMT, 2018). As the
MIH/CP community continues to grow, it has been met with several challenges. One of the
challenges is resistance from those currently in the emergency medical services (EMS) field as
well as others who may feel the roles of MIH/CP providers are overlapping in areas that are
generally the responsibility of other healthcare personnel such as home health workers
(O’Meara, Ruest, & Martin, 2015). Another challenge that has been difficult to overcome is

MOBILE INTEGRATED HEALTH 18
funding the start-up and maintenance of the program, with much of the funding having to come
from local operational budgets and limited or no reimbursement opportunities (Pearson, Gale &
Shaler, 2014).
Research Question A
MIH/CP has grown over the last several years to encompass several focus areas that have
been identified where communities can improve the overall health and wellbeing of their citizens
(NAEMT, 2018). Areas of focus based on community needs have expanded far beyond the scope
of LCFD’s MIH program and can provide insight into potential areas of focus where the LCFD
can expand their community services when compared to the identified areas relevant to the City
of Las Cruces. A review of Zavadsky and Hooten’s (2016), Mobile Integrated Healthcare: An
Approach to Implementation, served as a framework for LCFD and other organizations to
continue in their review of potential focus areas. A review of published programs (Zavadsky &
Hooten, 2016) showed most MIH/CP programs at the time centered around reducing
unnecessary emergency room visits and 911 calls through measures such as health hotlines,
alternative transport programs, post-discharge follow-up programs, injury prevention, mental
health intervention, community referral programs, and incident surveillance. Currently, LCFD’s
MIH Program’s, as discussed in the background and significance, focus areas are incident
surveillance for repeat 911 use and community referrals through both community partners and
internal incident responders. Morganti et al. (2014) referred to several steps that innovative EMS
agencies are taking to manage less emergent calls in their agencies. The steps reported by
Morganti et al. (2014) were:
1. Telephone triage of callers with nonemergent problems
MOBILE INTEGRATED HEALTH 19
2. Proactive management of high-frequency callers to 9-1-1
3. On-site assessment and treatment of selected patients
4. Transport of patients with low-acuity complaints to non-ed settings, such as
community health centers
5. Provision of alternative means of transport, such as a taxi voucher, for patients
who do not require ambulance transport (p. 78)
There have been several areas where EMS programs have implemented programs that
started as small pilot programs within their respective organizations and grew to systemwide
programs (Morganti et al., 2014). Some recommendations from Morganti et al. (2014) for
agencies considering the implementation of a patient-centered EMS program are the
organizations implement strong educational components to minimize the ambiguity of
responders along with strong medical oversight, and a comprehensive quality improvement
program to ensure patients are dispositioned safely and appropriately. Additionally, a community
needs assessment, the consideration of key stakeholders, and an emphasis on the involvement of
a wide array of community health partners were also recommended as keys to successful
program implementation (Morganti et al., 2014).
The Mobile Integrated Healthcare Practice Collaborative (MIHPC) through Medtronic
Philanthropy (2014) included the following characteristics of a comprehensive and accountable
MIH program. The list of characteristics are as follows (MIHCP, 2014):
1. Program and healthcare outcome goals informed by a population health needs
assessment
2. Patient access through a patient-centered mobile infrastructure
MOBILE INTEGRATED HEALTH 20
3. Delivery of evidence-based interventions using multidisciplinary and
interprofessional teams composed of providers operating at the top of their respective
scopes of practice
4. Improved access to healthcare and health equity through 24-hour availability
5. Patient-centered healthcare navigation and population-specific healthcare services
6. Full utilization of existing infrastructure and resources, including telemedicine
technology
7. Integrated electronic health records and access to health information exchanges
8. Provider education and training based on assessments of program needs and provider
competencies
9. Physician medical oversight in program design, implementation, and evaluation
10. Strategic partnerships engaging a spectrum of healthcare providers and other key
stakeholders
11. Financial sustainability
12. Quality outcomes performance measurement and program evaluation (p. 6)
The International Association of Fire Chiefs (IAFC) has published a guide to MIH titled
Handbook on Mobile Integrated Healthcare (2017). The guide provides a history of MIH in the
fire service, outlines the importance of MIH and recommends 15 steps to implementing an MIH
program. Listed below are the steps recommended by the IAFC for implementing a successful
MIH program (IAFC, 2017):
Step 1- Determine if MIH is right for your department
Step 2- Identify and Analyze your MIH population pools

MOBILE INTEGRATED HEALTH 21
Step 3- Determine the type of medical personnel needed to staff an MIH unit.
Step 4- Identify those entities that will benefit and those that will be impacted by your
MIH program as well as stakeholders
Step 5- Determine the cost to implement and maintain your MIH program
Step 6- Identify the times and days when your MIH population calls 911
Step 7- Determine a billing rate
Step 8- Target your unit hour utilization rate and MIH patient interventions
Step 9- Implement a patient navigation center
Step 10- Develop agreements with local urgent care facilities to accept, treat, and refer
patients
Step 11- Implement legal authority to bill for MIH services
Step 12- Develop alternate transport methodologies
Step 13- Develop agreements with your local accountable care organizations and health
insurance companies
Step 14- Complete the development of the policies and procedures that will provide
strong medical control and risk avoidance strategies as well as structure and
guidance
Step 15- Develop and implement an effective training program
Zavadsky and Hooten (2016) also highlight several key characteristics of successful
MIH/CP programs that are based on the experience and evaluation of programs that have been

MOBILE INTEGRATED HEALTH 22
implemented in recent years. They list six principles that are identified as key to a successful
program (Zavadsky & Hooten, 2016):
1. Identify local community healthcare needs.
2. Collaborate with local healthcare system stakeholders in every aspect of the programs
3. Integrate with existing resources, do not seek to replace
4. Involve physician leaders who are committed to the program and patients
5. Start small, test programs
6. Learn and build the program from the mistakes made
Research Questions B and C
Health hotlines are phone lines that connect citizens with a health professional
telephonically and are designed to educate and direct callers to appropriate services regardless of
insurance status (Novant Health, n.d.). Regional Emergency Medical Services Authority
(REMSA) in the Reno, NV area provides this service to all Washoe County residents to ensure
adequate levels of care are provided, and patients are referred to the appropriate facility
(Zavadsky & Hooten, 2016). Novant Health in North Carolina (Novant Health, n.d.) and
Hometown Health (Hometown Health, n.d.) serving Nevada and California residents also
provide such services using registered nurses that are staffed both 24 hours a day during certain
hours.
Alternative transport programs are programs that are aimed toward transporting patients
to the appropriate facility and providing alternative transportation methods to health facilities as
a means of decreasing unnecessary emergency department (ED) visits (Zavadsky & Hooten,
2016). Such programs also seek to triage, treat, and release patients with that do not need an ED

MOBILE INTEGRATED HEALTH 23
or clinic visit following initial assessment and treatment. REMSA, in addition to their other
programs, has an Ambulance Transport Alternatives Program to provide alternative transport
locations outside of the ED, such as mental health facilities, detoxification facilities for
intoxicated persons, and urgent cares for low-acuity health issues (Zavadsky & Hooten, 2016).
According to Zavadsky and Hooten (2016), Wake County Emergency Medical Services (EMS)
in North Carolina, has a redirect program which offers similar services as REMSA and has
decreased ED visits by over 20 percent, saving an estimated 100 hospitalizations, 2,448 bed-
hours, and reduced overall care costs by $500,000. The savings reported appear to be based
solely on the impact of mental health issues and alternative transport to WakeBrook Behavioral
Health Facility (Zavadsky & Hooten, 2016). Christian Hospital EMS in St. Louis, MO and Eagle
County Paramedics (CO), have programs that use paramedics in the field to diagnose and treat
patients, with the goal of decreasing unnecessary ED visits (Zavadsky & Hooten, 2016). Lastly,
Mesa Fire & Medical Department (AZ) has a program that utilizes community paramedics with
either a nurse practitioner or a behavioral health specialist to decrease unnecessary ED visits and
ensure referral to appropriate care (Zavadsky & Hooten, 2016). This model, however, especially
with the use of only paramedics, has been met with scrutiny as Neeki et al. (2016) reported an
under-triage rate of 19.3% when using paramedics under the standard scope of practice and
training levels. The need for additional training is also supported by the NAEMT (2018) and was
recommended through the review of over 1,500 elderly patients treated by paramedics with
additional training who were able to reduce the need for an ED visit by nearly 25 percent in the
United Kingdom (Mason et al., 2007). Other agencies that utilize programs that route patients to
more appropriate facilities beyond the ED or treat at home services. Seattle and King County
EMS implemented a six-month pilot program where a total of 204 patients met inclusion criteria
MOBILE INTEGRATED HEALTH 24
where it was determined the program avoided 200 visits to the ED and an estimated cost savings
of $750,000 (Morganti et al., 2014).
Post-discharge follow-up programs have become a mainstay for funding MIH programs
as they are programs that can provide pass-through funding through the savings realized by
hospitals or insurance companies (NAEMT, 2018). Post-discharge follow programs are funded
on a per-patient contact basis, outcome-based payment system, or a shared savings model, which
the latter of the two rewards the success of the program through readmission reductions
(Zavadsky & Hooten, 2016). The Center for Medicare and Medicaid Services (CMS) has the
Hospital Readmissions Reduction Program (HRRP) which was mandated by Section 3025 of the
Affordable Care Act (ACA) and requires payment reductions or penalties for excessive
readmissions (CMS, 2019). According to CMS (2019), the measures HRRP focuses on
readmission reduction for are acute myocardial infarction (AMI), chronic obstructive pulmonary
disorder (COPD), heart failure (HF), pneumonia, coronary artery bypass graft (CABG) surgery,
and elective primary total hip arthroplasty or total knee arthroplasty (THA/TKA). The potential
for organizations to capitalize on helping reduce readmissions has continued to grow with more
and more MIH/CP programs partnering with hospitals and/or insurance companies (NAEMT,
2018). Zavadsky and Hooten (2016), reported seven of the ten highlighted MIH/CP programs in
the United States were reducing hospital readmissions as one of their respective focus areas.
Zavadsky and Hooten (2016) noted the many services that have partnered with local
organizations to receive payments for reducing preventable readmissions.
Fall prevention programs are programs geared toward preventing at-risk populations from
the catastrophic effects of falls. The most at-risk population for falls in adults over the age of 65
as they account for the greatest risk of death or serious injury from the fall (Kopp & Ofstead,
MOBILE INTEGRATED HEALTH 25
2010). The age group 65 and older has been shown to account for anywhere between 65 and 75
percent of all incident responses to falls (Theut, 2017). It is believed that fall prevention has a
significant education component that starts with adults at all ages as knowledge of the problem
and repercussions of such incidents can trigger changes in people’s attitudes toward falls (Theut,
2017). In 2012, unintentional falls were the third leading cause of unintentional injury for all
ages and the fourth leading of cause injury-related death in New Mexico, according to the New
Mexico Department of Health [NMDOH] (2014). Additionally, New Mexico’s fall-related death
rate of 97.6/100,000 people was 1.8 times higher than the national rate of 53.4/100,000 in 2011
(NMDOH, 2014). From 2010 through 2012, nearly half of the falls where the patient was
hospitalized in New Mexico resulted in either discharge to a skilled nursing facility or required
home health care services (NMDOH, 2014).
In 2015, it was estimated over 43 million people age 18 and older had a mental illness
and 9.8 million having a serious mental illness in the United States (Moss, 2018). Mental health
intervention by EMS resulting in transport to the ED is estimated to account for approximately
2.2 million transports in the United States annually (Trivedi, Glenn, Hern, Schriger & Sporer,
2018). Trivedi et al. (2018) reported “Only 0.3 percent of patients receiving involuntary holds
needed any critical interventions” (p. 50). Their study further showed that when a diversion
program in EMS exists, the paramedics’ expertise has allowed for 41 percent of those who would
receive an involuntary hold to be successfully diverted from an ED to a psychiatric facility based
on established screening protocols (Trivedi et al., 2018). Mental health issues in the United
States are much more than a behavioral health problem as it affects the entire health care system,
compromising the quality of care for all who visit the ER due to overcrowding and psychiatric
boarding (Alakeson, Pande, & Ludwig, 2010). According to Alakeson, Pande, & Ludwig (2010),

MOBILE INTEGRATED HEALTH 26
“Boarding times in Georgia, for example, average thirty-four hours, and many patients wait
several days for an inpatient bed in of the state’s seven psychiatric hospitals” (p. 1637). During
this time, scarce emergency room resources a being consumed, creating increased wait times for
all seeking emergency care (Alakeson, Pande, & Ludwig, 2010). Overall quality of care often
lacks through the traditional methods of EMS response and transport to the ED, where the care
of the patient is merely transferred from one agency that is ill-prepared to another (Bronsky,
Giordano, & Johnson, 2016). Over six months, with an average of 81 patients seen per month,
the Colorado Springs’ Community Response Team (CRT), was able to decrease ED transports of
their patients by over 85 percent (Bronsky, Giordano, & Johnson, 2016). Such program success
is seen when organizations come together in a coordinated manner to help ensure those with
mental health illnesses are receiving the appropriate care.
In summary, the literature reviewed for this ARP reviewed how MIH/CP programs
became a commonplace for EMS providers and more specifically fire-based EMS providers. The
literature review also sought to identify the common characteristics of successful programs or
recommended characteristics for a successful program. Additionally, a review of current
MIH/CP focus areas was performed, specifically targeting programs that LCFD has minimal data
to support through incident data.
Procedures
The purpose of this research was to identify focus areas beyond LCFD’s MIH program’s
current scope by reviewing the characteristics of successful MIH/CP focus areas, current
MIH/Community Paramedicine focus areas, and comparing and matching the identified focus
areas to the needs of the City of Las Cruces. A descriptive methodology was utilized to guide the
MOBILE INTEGRATED HEALTH 27
research for this ARP through an extensive literature review, a survey of other organizations, and
lastly a review of Las Cruces incident data for comparison and evaluation.
A survey instrument (See Appendix A) was developed to identify other organizations
who have MIH/CP programs. Additionally, the questions were designed to gather information on
the type and size of the organization, the focus areas of the organizations, the budgets assigned to
the programs, outside funding sources, obstacles, and benefits realized. The survey was a 10-
question survey that was developed using Survey Monkey, an internet-based survey development
software on November 21, 2018, and was open through December 15, 2018. The survey was
anonymous and only allowed for one response per IP address to limit the potential for duplicate
agency responses. It was sent across the fire service through posting on the International
Association of Fire Chiefs (IAFC) Knowledge Net on November 21, 2018. Additionally, the
survey link was sent to the president-elect of the National Association of Emergency Medical
Technicians, to be forwarded on a mailing list of MIH/CP personnel nationwide specifically
seeking to target most organizations with MIH/CP Programs. Following the deadline, there were
21 responses collected, and the data was evaluated and categorized. The survey’s design
provided data for research question B of this ARP in identifying organizations that had MIH/CP
programs, their organizational make-up (career, volunteer, or combination), population served,
respective focus areas, budgets/funding sources, obstacles, and benefits of their program.
Following the identification of other MIH/CP focus areas that are being addressed in
other organizations, a review of call data from Las Cruces Fire Department was performed for
the years of 2014, 2015, 2016 and 2017. The purpose of this was to help answer question B of
this ARP by identifying and aligning incident responses with the identified focus areas. National
Fire Incident Reporting System (NFIRS) codes as described in the 2015 edition of National Fire

MOBILE INTEGRATED HEALTH 28
Incident Reporting System: Complete Reference Guide (USFA, 2015) were utilized to limit the
call types across the years evaluated consistently. Specifically, the codes that were utilized to
limit calls related to the MIH areas of focus identified were the 300: Rescue and Emergency
Medicals Services Incidents, 500: Service Call, and 600: Good Intent Call series. The data from
the 300 series incidents were limited to 300: Rescue and EMS Incident- Other, 311: Medical
Assist, 320: Emergency Medical Services- Other, 321: EMS Call- Excluding Vehicle Accident.
The 500 series incidents were limited to 510: Person in Distress- Other, 512: Ring or Jewelry
Removal and 554: Assist Invalid. Lastly, the 600 series codes were limited to 600: Good Intent
Call- Other, and 661: EMS Call where Party has Left Scene (See Appendix B).
Incident data related to EMS incidents was also queried and cataloged by the condition
codes that were utilized by LCFD during the reported years for all incidents with patient care
reports attached (See Appendix C). Not known, not reporting, not applicable, and not available
codes utilized by the report writers were combined. These codes represent areas where LCFD
personnel were able to categorize patients that did not fit in to any of the pre-defined condition
codes available. The other codes were also used for incidents where reports were generated on
interactions with individuals not categorized as patients by LCFD. Additionally. All other codes
were combined by like types to condense the data from 74 individual lines to 42 commonly
themed conditions. The data gathered was then reduced to incidents that accounted for one
percent of the patient care reports completed or greater. In addition to the review of LCFD
incident data, an email was sent to the Mesilla Valley Regional Dispatch Authority (MVRDA)
on February 4, 2019 to identify the amount of mental health-related incidents and overdoses any
response unit was sent to in the City of Las Cruces from 2014 through 2017 since LCFD does
not respond to all behavioral calls. Behavioral issues and suicidal ideations incidents are

MOBILE INTEGRATED HEALTH 29
primarily referred to Las Cruces Police Department (LCPD) and American Medical Response
(AMR), the county’s contracted transport provider. A response was received on February 5,
2019, from Robert Milks, MVRDA’s National Crime Information Center (NCIC) Coordinator
(See Appendix D). An additional email to Robert Milks was sent on February 11, 2019,
requesting the number of times LCFD was dispatched to lift assists and falls from 2014 through
2017 since the data obtained through LCFD’s incident reporting system did not allow the
incidents to be specifically limited by the individual types. A response was received from Robert
Milks on February 13, 2019 (See Appendix E). Fall victims are dispatched when there is
generally an injury associated with the fall, while lift assist are generally dispatched when there
is no reported injury and the subject needs assistance back in bed or to their wheelchair and so
on. The areas where incident data was sparse, literature was reviewed to supplement the
available information.
A second survey was sent out to local providers on February 1, 2019, with a deadline of
February 15, 2019, seeking the input of prehospital paramedics and emergency department staff
from the two local hospitals, Mountain View Regional Medical Center and Memorial Medical
Center (See Appendix F). The survey asked respondents first to identify their role and answer
what percentage of ED visits were preventable/unnecessary as multiple-choice answers for the
first two questions of the survey. Questions three through ten of the survey asked them to rate
their perceived effectiveness of each of the identified focus areas utilizing a single-row Likert
Scale. The numerical score for each response was based on a one to five scale with very unlikely
scoring a one, unlikely scoring a two, neutral scoring a three, likely scoring a four, and very
likely scoring five points. Question 11 of the survey was a free text box seeking to answer what
the respondents perceived to be the condition that contributed to the majority of preventable or
MOBILE INTEGRATED HEALTH 30
unnecessary ED visits. Lastly, question 12 asked the respondents to rank the identified focus
areas from one through eight, with focus area one being the area with the most perceived
effectiveness and eight being the program with least perceived effectiveness. During the time
allotted, 45 people responded to the survey. The survey was anonymous and only allowed for
one response per IP address to limit the potential for duplicate agency responses. The questions
were tallied based on overall averages as well as by individual provider type to provide insight
into the provider group perspectives. The emergency room technicians yielded only one
response, providing for lack of representation of the impressions of those serving in such roles.
The results from questions three through ten were compared to question 12 to help identify the
focus areas with the highest levels of perceived effectiveness. The areas were then compared to
incident counts for the City of Las Cruces.
While the procedures performed sought to control the limitations of this research, there
were still several present. The first was the lack of response to the survey, potentially limiting the
response pool of focus areas in MIH. The posting locations sought to capitalize on reaching
members of organizations globally, but only yielded twenty-one responses. Additionally, while
the setting limited responses from the same IP address, there is a possibility that the same
organization could be represented since the responses were anonymous and did not identify the
represented organization by name. The survey responses were also likely influenced by those
interested in the subject matter and those who respond to most EFO surveys posted on the IAFC
Knowledge Net. This may correlate to the lack of response as the interest in MIH/CP programs
appears limited across the fire service. The NAEMT (2018) reports over 200 MIH/CP programs
across the United States. The seven respondents with MIH/CP programs are a small sample of
those programs.
MOBILE INTEGRATED HEALTH 31
Another limitation was found in the collection of the data and the difficulty in identifying
areas of focus. The reporting software utilized by the LCFD before October 2017 did not capture
detailed data points outside of general incident types and condition codes, significantly limiting
the author’s ability to capture information that can be utilized in the evaluation process. The extent
that the reporting software was able to capture incident data was limited to NFIRS call types and
National Emergency Medical Services Information Systems (NEMSIS) condition codes. The lack
of consistent documentation has led to difficulty in analyzing call volume.
Results
The data obtained to answer the three research questions presented in this ARP are
outlined below. The first research question was answered by performing a literature review of
available data regarding the characteristics of successful MIH programs. The second question of
this ARP was answered by performing a literature review of MIH programs and a survey
instrument that looked to identify current MIH programs. The third question was answered
through a review of LCFD incident data and local provider perspectives and then comparing it to
the focus areas identified as part of the second question of this ARP.
Research Question A: What are the characteristics of successful Mobile Integrated Health
programs?
The purpose of this question was to identify the characteristics of successful MIH/CP
programs which will allow LCFD to identify not only the programs that have been successful but
also how to ensure the focus areas that LCFD considers expanding to are built upon a successful
framework. The literature review conducted as part of this ARP identified several common
characteristics that were recommended for a successful MIH program. The characteristics of
MOBILE INTEGRATED HEALTH 32
successful programs that were identified appear to be universal recommendations across all focus
areas. Below, the characteristics identified in the literature review are highlighted below in no
particular order:
The programs implemented should be based on the results of a community risk
assessment as affirmed by IAFC (2017), MIHCP (2014), Morganti, et al. (2014), and Zavadsky
& Hooten (2016). Community risk assessments provide insight in to the community and its risks
based on health data and community demographics. Understanding the community facilitates
targeted approaches to strategic community risk reduction, where the areas addressed are not
blindly addressed, but supported by community specific data. Castillo et al. (2016) noted, MIH
efforts that are researched and developed to target community subpopulations with the highest
risk as compared to a generalized approach were shown to yield the greatest overall results.
Another characteristic of successful MIH programs is they have high stakeholder
engagement and integration as affirmed by IAFC (2017), Morganti, et al. (2014), MIHCP (2014),
and Zavadsky & Hooten (2016). Engaging stakeholders provides for integration among
community providers, programs, and services that are able to collectively address the problems
of those needing assistance. Stakeholder engagement is supported by O’Meara, Ruest, and
Martin (2015) as the involvement of as many stakeholders can reduce duplication of effort and
prevent feelings of encroachment from other providers in the community.
Program implementation should have a cost-analysis performed as recommended by
IAFC (2017), MIHCP (2014), and Zavadsky & Hooten (2016). Understanding the costs of
implementation when compared to the services currently provided can provide insight in to the
benefits that can be realized through program implementation. Utilizing the costs of services
MOBILE INTEGRATED HEALTH 33
provided and the services proposed allows for opportunity cost analysis for organizations to
determine the potential impacts of implementation or not.
The problem should also attempt to identify stable funding sources for the program as
suggested by IAFC (2017), MIHCP (2014), and Zavadsky & Hooten (2016)]. Ensuring
sustainability for the program to maintain its efforts is critical to the success of programs. MIH
programs failing to secure stable funding sources risk regression if the program is terminated
despite success due to lack of stable funding sources.
Another important characteristic is the providing of population specific navigation
services [IAFC (2017), Morganti, et al. (2014), MIHCP (2014), and Zavadsky & Hooten (2016)].
Based on the results of the community risk analysis, it is important for organizations with MIH
programs to take action in addressing the areas identified. As discussed, targeted approaches
yield the greatest results (Castillo et al., 2016). Additionally, population specific services can
minimize scope creep, ensuring the program is adhering to serving the populations with the
greatest needs.
Strong policy, protocol, medical direction and quality improvement programs are also
important characteristics of successful MIH programs [IAFC (2017), Morganti, et al. (2014),
MIHCP (2014), and Zavadsky & Hooten (2016)]. Policies, protocols, and medical direction
provide guidance on expectations of the program to ensure ambiguity and risk are minimized.
Quality improvement allows for the retrospective review of the care and services provided to
ensure they meet the guidance set by policy, protocol, and medical direction. Strong quality
improvement also helps identify the gaps in policy, protocol, and medical direction.
The last of the identified characteristics of successful MIH programs is a well-trained
provider team [IAFC (2017), Morganti, et al. (2014), MIHCP (2014), and Zavadsky & Hooten

MOBILE INTEGRATED HEALTH 34
(2016)]. Adequate training helps reduce risk and ensure high levels of quality care are provided.
The role of an MIH program is often proactive, where traditional EMS is reactive. Providers
should be trained in proactive measures as well as any expanded scope of practice provision that
have been approved. Mason et al. (2007), noted how additional training of paramedics in the
United Kingdom reduced unnecessary emergency room visits of elderly by nearly 25 percent.
Research Question B: What focus areas are other Mobile Integrated Health programs
addressing in their communities?
The survey that was sent out yielded minimal responses with 21 recorded responses
during the time period the survey was opened. Of the 21 responses, only seven of the
organizations had a MIH/CP program (See Figure 1). The literature review performed identified
that as of 2018 there were over 200 MIH/CP programs operating in the United States (NAEMT,
2018). Of the 200 plus programs, the NAEMT (2018) reported that 33 percent of the reporting
MIH/CP programs were public, fire-based systems that have started MIH/CP programs in their
respective communities. The results of the survey provided insight in to other MIH/CP program
focus areas but appeared lacking in response from other fire-based organizations that have
implemented MIH/CP programs in their respective communities.
0
10
20
714
Yes No
Figure 1: Presence of an MIH/CP program
MOBILE INTEGRATED HEALTH 35
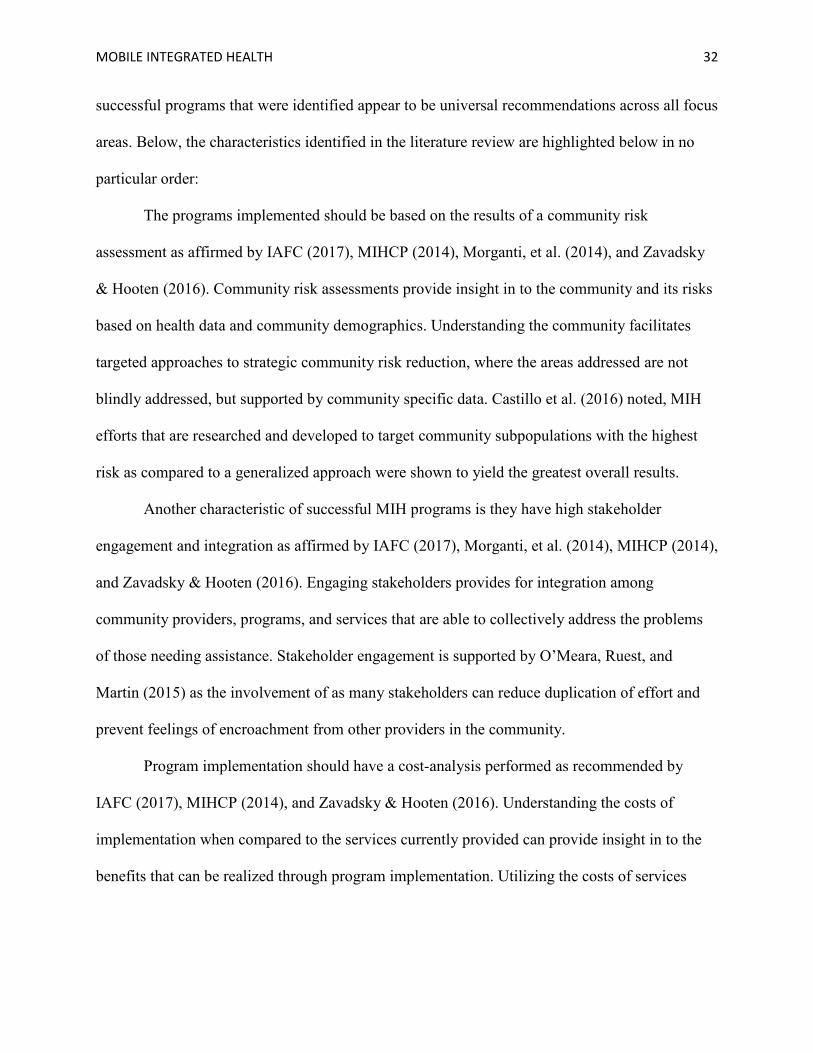
The organizational makeup of the seven respondents that currently have MIH/CP
programs consisted of four all career departments, three combination departments, and zero all
volunteer departments (See Figure 2). The literature review performed did not delineate the
organizational make-up of those with active MIH/CP programs. Of the 14, respondents that did
not currently have a MIH/CP program, 11 were all-career organizations, two combination, and
one all-volunteer organization. A review of the organizations highlighted by Zavadsky and
Hooten (2016), showed that all 10 of the represented organizations were career/combination type
organizations where the MIH/CP personnel assigned were paid.
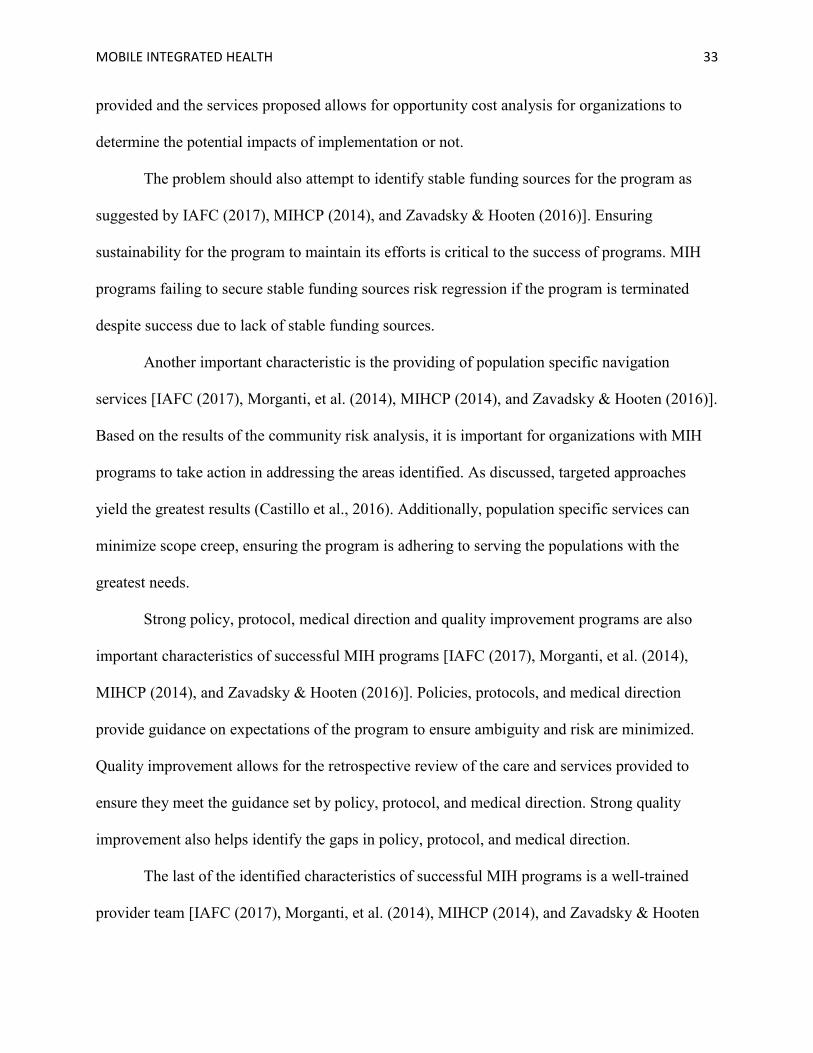
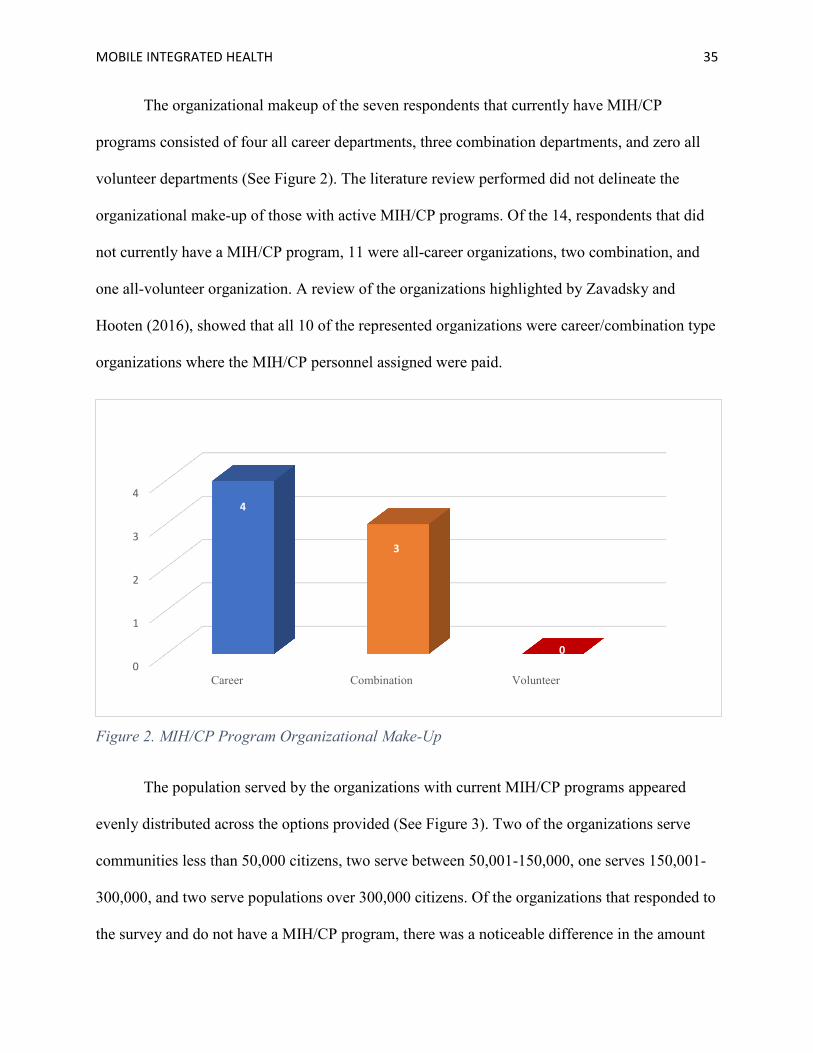
The population served by the organizations with current MIH/CP programs appeared
evenly distributed across the options provided (See Figure 3). Two of the organizations serve
communities less than 50,000 citizens, two serve between 50,001-150,000, one serves 150,001-
300,000, and two serve populations over 300,000 citizens. Of the organizations that responded to
the survey and do not have a MIH/CP program, there was a noticeable difference in the amount
0
1
2
3
4
Career Combination Volunteer
4
3
0
Figure 2. MIH/CP Program Organizational Make-Up
MOBILE INTEGRATED HEALTH 36
of organizations who served less than 50,000 citizens as compared to the other three options.
There were seven or 50 percent of the respondents that did not currently have MIH/CP programs.
None of the respondent organizations without an MIH/CP program served populations of less
than 50,000. Two organizations served populations of 50,001-150,000, three served populations
of 150,001-300,000, and two served populations greater than 300,000.
0
1
2
Less than 50,000 50,001-150,000 150,001-300,000 Over 300,000
2 2
1
2
Figure 3. Population Served
As identified in Table 1, the seven organizations that reported having MIH/CP programs
in the survey, reported a variety of focus areas they were concentrating on beyond high 911
utilizers, a focus area already performed by LCFD. Post-Discharge follow-up/Readmission
avoidance and prevention were reported as a focus area for four of the seven organizations that
responded to the survey. Post-Discharge follow-up/Readmission avoidance was also highly
represented as a focus area in the literature review with 70 percent of the highlighted
organizations utilizing it as a focus area for their organization (Zavadsky & Hooten, 2016).
Opioid outreach was represented by three of the seven organizations who responded to the
MOBILE INTEGRATED HEALTH 37
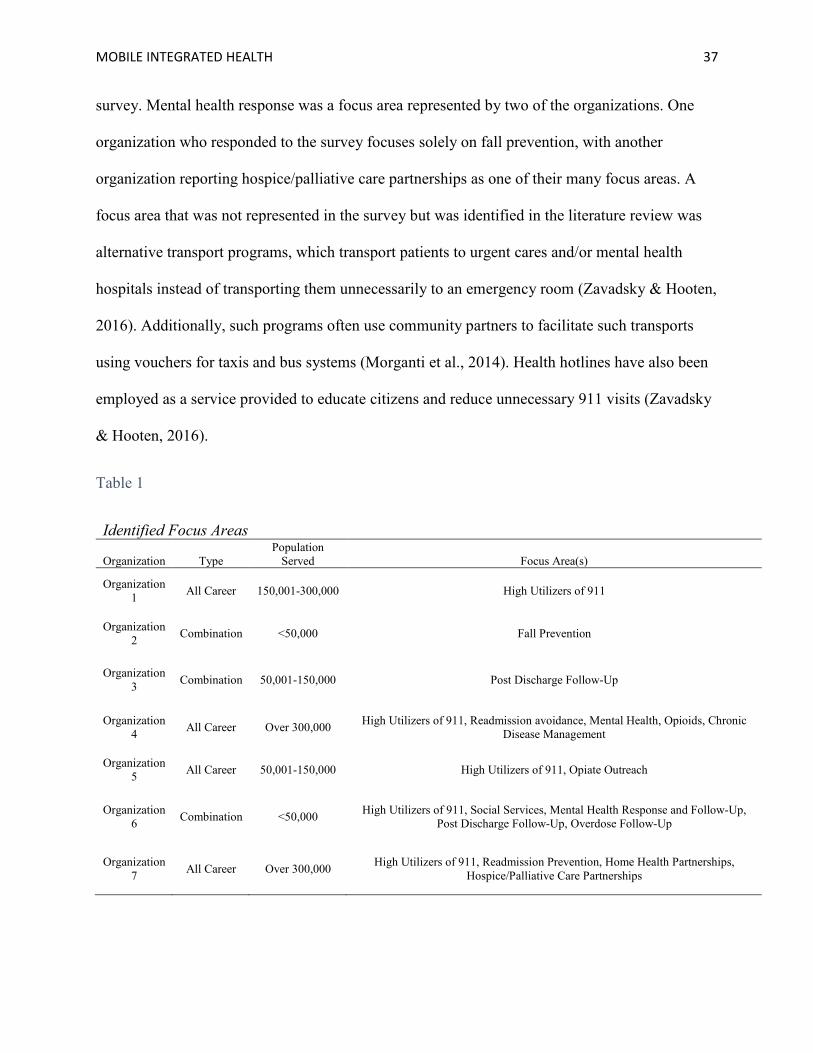
survey. Mental health response was a focus area represented by two of the organizations. One
organization who responded to the survey focuses solely on fall prevention, with another
organization reporting hospice/palliative care partnerships as one of their many focus areas. A
focus area that was not represented in the survey but was identified in the literature review was
alternative transport programs, which transport patients to urgent cares and/or mental health
hospitals instead of transporting them unnecessarily to an emergency room (Zavadsky & Hooten,
2016). Additionally, such programs often use community partners to facilitate such transports
using vouchers for taxis and bus systems (Morganti et al., 2014). Health hotlines have also been
employed as a service provided to educate citizens and reduce unnecessary 911 visits (Zavadsky
& Hooten, 2016).
Table 1
Identified Focus Areas
Organization Type Population
Served Focus Area(s)
Organization 1 All Career 150,001-300,000 High Utilizers of 911
Organization 2 Combination <50,000 Fall Prevention
Organization 3 Combination 50,001-150,000 Post Discharge Follow-Up
Organization 4 All Career Over 300,000 High Utilizers of 911, Readmission avoidance, Mental Health, Opioids, Chronic
Disease Management
Organization 5 All Career 50,001-150,000 High Utilizers of 911, Opiate Outreach
Organization 6 Combination <50,000 High Utilizers of 911, Social Services, Mental Health Response and Follow-Up,
Post Discharge Follow-Up, Overdose Follow-Up
Organization 7 All Career Over 300,000 High Utilizers of 911, Readmission Prevention, Home Health Partnerships,
Hospice/Palliative Care Partnerships
MOBILE INTEGRATED HEALTH 38
The following list contains the identified focus areas in the survey as well as the literature
review performed. The focus areas are listed in no particular order:
1. High-Utilizers of 911 (Already a LCFD MIH program focus area)
2. Fall Prevention
3. Alternative Transport
4. Post-Discharge Follow-Up / Readmission Prevention
5. Mental Health Response
6. Opiate / Drug Response and Outreach
7. Social Services / Health System Navigation
8. Hospice/Palliative Care Partnerships
9. Health Hotline Services
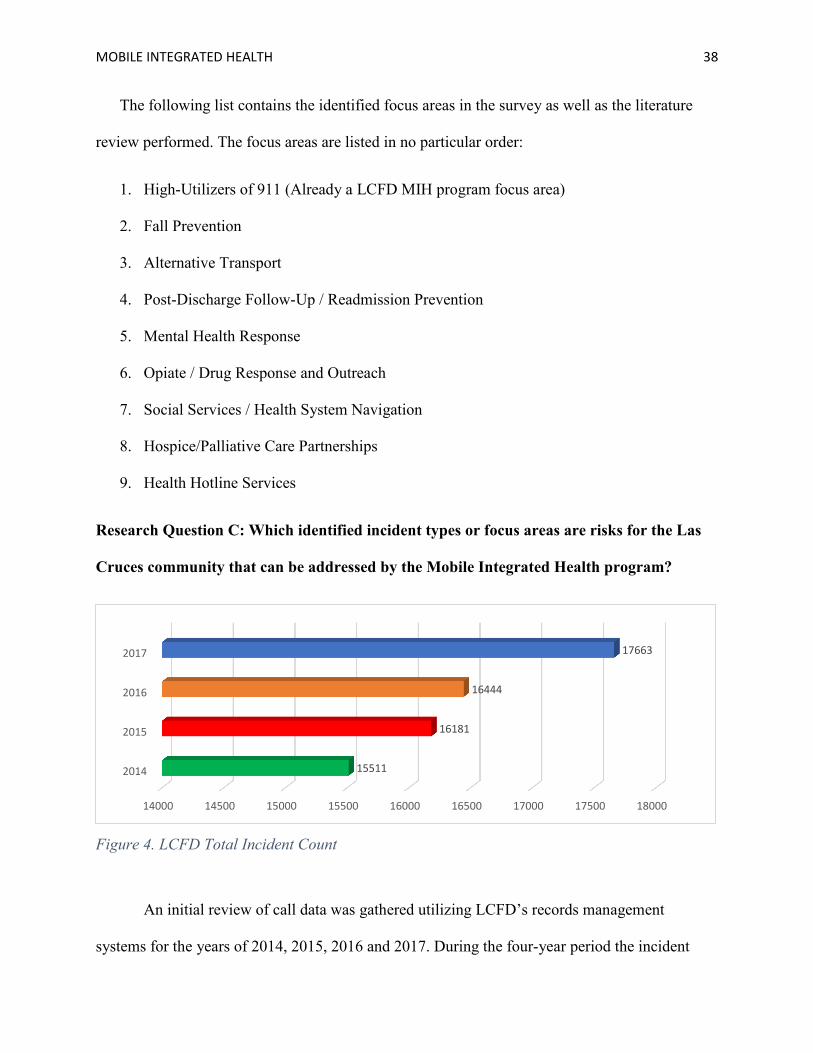
Research Question C: Which identified incident types or focus areas are risks for the Las
Cruces community that can be addressed by the Mobile Integrated Health program?
14000 14500 15000 15500 16000 16500 17000 17500 18000
2014
2015
2016
2017
15511
16181
16444
17663
Figure 4. LCFD Total Incident Count
An initial review of call data was gathered utilizing LCFD’s records management
systems for the years of 2014, 2015, 2016 and 2017. During the four-year period the incident

MOBILE INTEGRATED HEALTH 39
counts were 15,551, 16,181, 16,444 and 17,663 respectively (See Figure 4). The incident counts
over the four years show an annual increase of 2,152 incidents in 2017, as compared to the
number of incidents in 2015. The queued results utilizing the specified NFIRS codes were then
gathered, yielding 10,289, 10,529, 10,522 and 10,482 incidents for the same years (See Table 2).
Despite the overall call increases over the four-year period, the incident counts remained
relatively flat for the queued incidents of this ARP, as evidenced in Table 2. The areas reflecting
a significant increase can be attributed to how incidents were classified, and the changes
implemented in 2015 that limited patient care reports generated when the transport agency was
on scene prior to LCFD and when there were no injuries. Before this, a blank patient care report
with minimal incident information was attached to keep track of non-patient disclosures and the
assistance provided to the private EMS service. If any care is provided beyond assisting in
patient movement, a patient care report must still be completed. The changes sought to eliminate
patient care reports for manpower assists.
Table 2
Queued LCFD NFIRS Codes
Incident Types 2014 2015 2016 2017 300: Rescue and EMS Incident, other 546 427 340 312 311: Medical Assist 1,112 1,351 1,714 2,256 320: Emergency Medical Services, other 725 881 800 707 321: EMS Call, Excluding Vehicle Accident 7,413 7,261 6,970 6,429 510: Person in Distress, other 150 165 208 173 554: Assist Invalid 216 311 366 497 600: Good Intent Call 127 133 124 108 Total Incidents 10,289 10,529 10,522 10,482
Table 3 represents the incident distribution based on the patient care reports completed by
LCFD emergency response personnel from 2014-2017 utilizing the condition codes that
represented one percent or greater of the patient care reports completed. The data presented
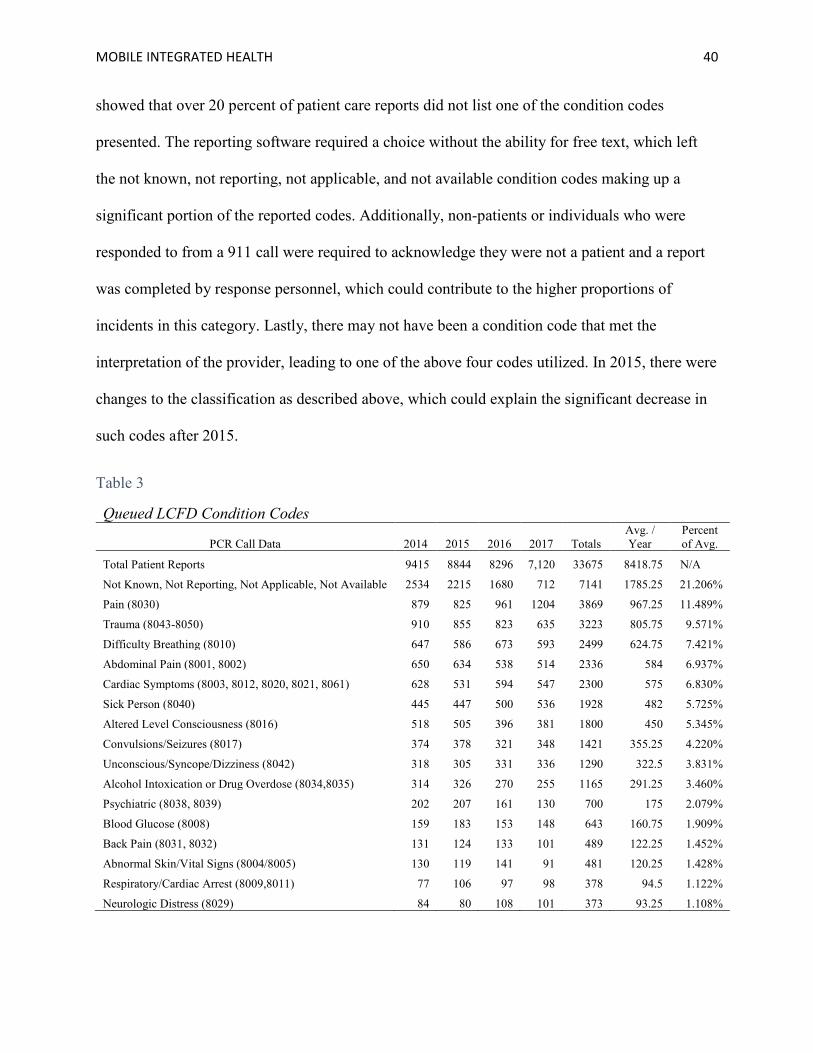
MOBILE INTEGRATED HEALTH 40
showed that over 20 percent of patient care reports did not list one of the condition codes
presented. The reporting software required a choice without the ability for free text, which left
the not known, not reporting, not applicable, and not available condition codes making up a
significant portion of the reported codes. Additionally, non-patients or individuals who were
responded to from a 911 call were required to acknowledge they were not a patient and a report
was completed by response personnel, which could contribute to the higher proportions of
incidents in this category. Lastly, there may not have been a condition code that met the
interpretation of the provider, leading to one of the above four codes utilized. In 2015, there were
changes to the classification as described above, which could explain the significant decrease in
such codes after 2015.
Table 3
Queued LCFD Condition Codes
PCR Call Data 2014 2015 2016 2017 Totals Avg. / Year
Percent of Avg.
Total Patient Reports 9415 8844 8296 7,120 33675 8418.75 N/A
Not Known, Not Reporting, Not Applicable, Not Available 2534 2215 1680 712 7141 1785.25 21.206%
Pain (8030) 879 825 961 1204 3869 967.25 11.489%
Trauma (8043-8050) 910 855 823 635 3223 805.75 9.571%
Difficulty Breathing (8010) 647 586 673 593 2499 624.75 7.421%
Abdominal Pain (8001, 8002) 650 634 538 514 2336 584 6.937%
Cardiac Symptoms (8003, 8012, 8020, 8021, 8061) 628 531 594 547 2300 575 6.830%
Sick Person (8040) 445 447 500 536 1928 482 5.725%
Altered Level Consciousness (8016) 518 505 396 381 1800 450 5.345%
Convulsions/Seizures (8017) 374 378 321 348 1421 355.25 4.220%
Unconscious/Syncope/Dizziness (8042) 318 305 331 336 1290 322.5 3.831%
Alcohol Intoxication or Drug Overdose (8034,8035) 314 326 270 255 1165 291.25 3.460%
Psychiatric (8038, 8039) 202 207 161 130 700 175 2.079%
Blood Glucose (8008) 159 183 153 148 643 160.75 1.909%
Back Pain (8031, 8032) 131 124 133 101 489 122.25 1.452%
Abnormal Skin/Vital Signs (8004/8005) 130 119 141 91 481 120.25 1.428%
Respiratory/Cardiac Arrest (8009,8011) 77 106 97 98 378 94.5 1.122%
Neurologic Distress (8029) 84 80 108 101 373 93.25 1.108%
MOBILE INTEGRATED HEALTH 41
The data represented above in Table 3 shows nearly 20 percent of all patient care reports
completed utilized condition codes related to pain, excluding chest pain which is captured in the
cardiac symptoms code grouping. Traumatic incidents accounted for the next highest amount of
patient care reports accounting for nearly 10 percent of all completed reports. Following
traumatic incidents, difficulty breathing, cardiac symptoms, sick person, and altered level of
consciousness accounted for 7.42, 6.83, 5.73, and 5.35 percent of all reports, respectively. The
remaining eight condition code groups accounted for approximately 21 percent of the total
PCR’s completed.
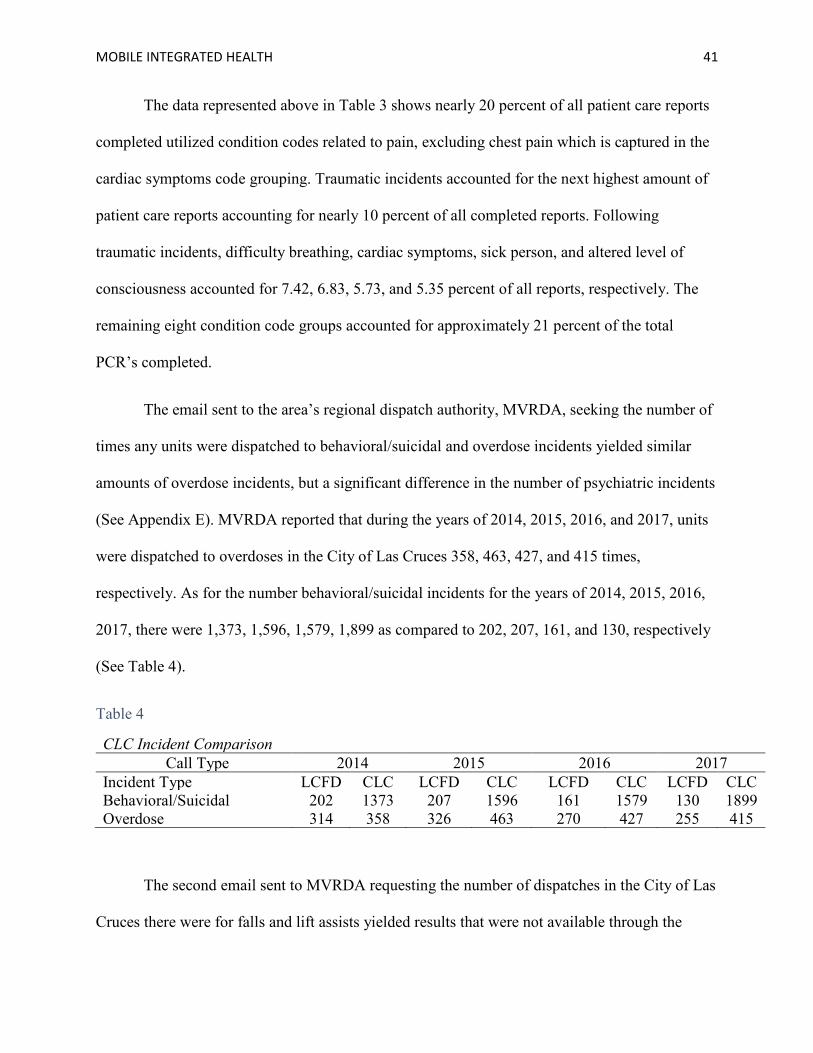
The email sent to the area’s regional dispatch authority, MVRDA, seeking the number of
times any units were dispatched to behavioral/suicidal and overdose incidents yielded similar
amounts of overdose incidents, but a significant difference in the number of psychiatric incidents
(See Appendix E). MVRDA reported that during the years of 2014, 2015, 2016, and 2017, units
were dispatched to overdoses in the City of Las Cruces 358, 463, 427, and 415 times,
respectively. As for the number behavioral/suicidal incidents for the years of 2014, 2015, 2016,
2017, there were 1,373, 1,596, 1,579, 1,899 as compared to 202, 207, 161, and 130, respectively
(See Table 4).
Table 4
The second email sent to MVRDA requesting the number of dispatches in the City of Las
Cruces there were for falls and lift assists yielded results that were not available through the
CLC Incident Comparison Call Type 2014 2015 2016 2017
Incident Type LCFD CLC LCFD CLC LCFD CLC LCFD CLC Behavioral/Suicidal 202 1373 207 1596 161 1579 130 1899 Overdose 314 358 326 463 270 427 255 415
MOBILE INTEGRATED HEALTH 42
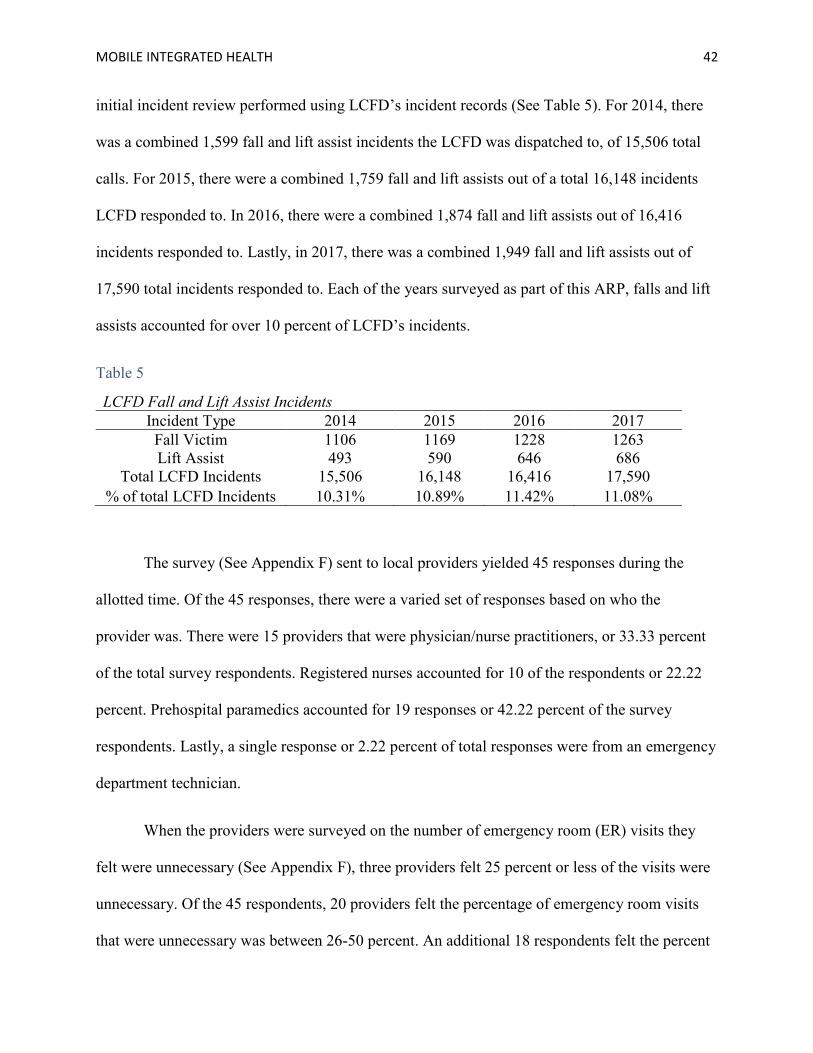
initial incident review performed using LCFD’s incident records (See Table 5). For 2014, there
was a combined 1,599 fall and lift assist incidents the LCFD was dispatched to, of 15,506 total
calls. For 2015, there were a combined 1,759 fall and lift assists out of a total 16,148 incidents
LCFD responded to. In 2016, there were a combined 1,874 fall and lift assists out of 16,416
incidents responded to. Lastly, in 2017, there was a combined 1,949 fall and lift assists out of
17,590 total incidents responded to. Each of the years surveyed as part of this ARP, falls and lift
assists accounted for over 10 percent of LCFD’s incidents.
Table 5
LCFD Fall and Lift Assist Incidents Incident Type 2014 2015 2016 2017 Fall Victim 1106 1169 1228 1263 Lift Assist 493 590 646 686
Total LCFD Incidents 15,506 16,148 16,416 17,590 % of total LCFD Incidents 10.31% 10.89% 11.42% 11.08%
The survey (See Appendix F) sent to local providers yielded 45 responses during the
allotted time. Of the 45 responses, there were a varied set of responses based on who the
provider was. There were 15 providers that were physician/nurse practitioners, or 33.33 percent
of the total survey respondents. Registered nurses accounted for 10 of the respondents or 22.22
percent. Prehospital paramedics accounted for 19 responses or 42.22 percent of the survey
respondents. Lastly, a single response or 2.22 percent of total responses were from an emergency
department technician.
When the providers were surveyed on the number of emergency room (ER) visits they
felt were unnecessary (See Appendix F), three providers felt 25 percent or less of the visits were
unnecessary. Of the 45 respondents, 20 providers felt the percentage of emergency room visits
that were unnecessary was between 26-50 percent. An additional 18 respondents felt the percent

MOBILE INTEGRATED HEALTH 43
of unnecessary visits to the ER was between 51-75 percent. Lastly, four respondents felt 76-100
percent of the visits were unnecessary. The provider response distribution showed most
providers perceived the number of unnecessary visits to be between 26-75 percent, as only one of
each of the providers listed, with exception to emergency room technicians, perceived the
percentage to be either zero-25 percent or 76-100 percent (See Table 6). The responses show a
significant number of what is perceived by first-hand providers to be unnecessary visits to the
ER.
Table 6
Unnecessary ER Visits: Provider Distribution Prehospital Paramedic
% Unnecessary ER Visits 0-25% 26-50% 51-75% 76-100% Respondents 1 8 9 1
Registered Nurse % Unnecessary ER Visits 0-25% 26-50% 51-75% 76-100%
Respondents 1 4 4 1 Physician/Nurse Practitioner
% Unnecessary ER Visits 0-25% 26-50% 51-75% 76-100% Respondents 1 7 6 1
Emergency Room Technician % Unnecessary ER Visits 0-25% 26-50% 51-75% 76-100%
Respondents 0 1 0 0
The identified focus areas were then rated individually and against one another to
evaluate the perceived effectiveness the respondents to the survey felt about the focus areas (See
Table 7). The results of the survey showed that the highest rated perceived effectiveness was
among five of the eight focus areas. The area with the highest weighted average of perceived
effectiveness when rated alone was mental health response and outreach but was third when
ranked against the other focus areas. Post-discharge follow-up/readmission prevention programs
had the second highest weighted average as well as ranked second among all other focus areas. A
Social services/health system navigation program was ranked the highest overall when compared
to the other focus areas and had the third highest weighted average of perceived effectiveness.

MOBILE INTEGRATED HEALTH 44
Alternative transport and fall prevention ranked fourth and fifth, in both weighted average and
ranked among the others in perceived effectiveness. Health hotline was sixth in weighted average
and ranking among the other focus areas. Hospice/palliative services navigation was seventh in
the weighted average scores and eighth in the overall ranking among the focus areas. Lastly,
opioid response and outreach programs were rated to be the least effective in reducing
unnecessary 911 visits in the weighted average scoring but ranked seventh in perceived
effectiveness when compared to the other identified focus areas.
Table 7
Focus Area Weighted Average vs. Ranking
Focus Area Weighted Average Ranked Scores Incidents
Mental Health Response and Outreach 4.51 5.33 1,612
Post Discharge Follow-Up/Readmission Prevention 4.49 5.70 Unknown
Social Services/Health System Navigation 4.47 5.74 Unknown
Alternative Transport 4.43 5.30 Unknown
Fall Prevention 4.18 4.96 1,795
Health Hotline 4.07 3.11 Unknown
Hospice/Palliative Services Navigation 4.00 2.84 Unknown
Opioid Response and Outreach 3.80 3.05 291
Table 7 also shows the number of incident responses the City of Las Cruces responds to,
based on a four-year average of 911 calls for service and incident reports if available for the
specific focus area. In the City of Las Cruces, there were incident counts that were
representative of three of the eight identified focus areas. Falls in the City of Las Cruces
accounted for a four-year average of approximately 1,795 incidents. Behavioral/mental health
incidents in the City of Las Cruces had a four-year annual average of approximately 1,612
incidents. Lastly, the four-year annual average for opioid overdose incidents is approximately
291 incidents. Each of the incident types with counts also showed an increase in incidents from
2014 to 2018.
MOBILE INTEGRATED HEALTH 45
Discussion
The results of this ARP show that in many areas LCFD is on the right track as many of
the organizations identified are also addressing repeat 911 use as one of their primary focus areas
as reported by NAEMT (2018) and Zavadsky and Hooten (2016). The focus areas identified and
the incident data support many of the informal discussions that have occurred as well as the
programs expansions already being considered such as CHF readmission reduction. The results
of this research provide a framework for LCFD to expand the focus area discussions with local
stakeholders. The incident and survey data, as well as the information gathered in the literature
review, appears to present opportunities as there are several areas not being proactively
addressed by LCFD. Such results can help the organization move forward in selecting focus
areas. The research did highlight a significant lack of understanding of the workload possibilities
of LCFD’s MIH program.
MIH in the United States became a focus of many fire-based EMS organizations
following the passing of the Patient Portability and Accountability Act of 2010. As of 2017,
there were over 200 MIH programs in the United States, with over 30 percent of them being fire-
based (NAEMT, 2018). Three years prior, in 2014, there were just over 100 known MIH
programs (NAEMT, 2015). The research performed provided insight into the characteristics of
successful programs. There have been many programs that have found success and upon
evaluation seem to share some common characteristics or procedural recommendations. The
PPACA of 2010 focuses very heavily on the importance of integrated care in creating healthier
populations to reduce skyrocketing healthcare costs (Stanhope, 2015). Some of the common
characteristics of or recommendations for a successful MIH program is to integrate with local
providers, maximizing stakeholder engagement and the collective resources of the entire
MOBILE INTEGRATED HEALTH 46
healthcare system. Such recommendations were presented by Morganti et al. (2014), MIHCP
(2014), IAFC (2017), and Zavadsky and Hooten (2016). Community risk knowledge based on
demographics, incident data for the community, as well as emergency room visit data and
provider perspectives should be gathered as part of an organization’s community health risk
analysis. Morganti et al. (2014), MIHCP (2014), IAFC (2017), and Zavadsky and Hooten (2016)
each documented the importance of community-specific data as a basis for program
identification and implementation. This concept for identification and implementation is further
supported by Castillo et al. (2016) as they highlighted how MIH efforts that are researched and
developed to target community subpopulations with the highest risk as compared to a
generalized approach were shown to yield the greatest overall results.
All programs must consider funding sources in whether the organization will fund the
program, or will they leverage community partnerships and seek reimbursement for service
options (IAFC, 2017). Zavadsky and Hooten (2016) highlighted the difficulties of
reimbursement for MIH programs as many states do not have provisions for such
reimbursements, leaving the primary means of reimbursement being from partnerships.
Additional considerations should be given to the savings realized through the impacts to
emergency services through reductions in call volume, if applicable (Stowell, 2016). It is the
author’s belief that 911 reductions can serve as a hedge against growth, especially in times when
there are significant budgetary constraints serving as the primary bottleneck in effective
emergency response.
In addition to the financial security of the program, there needs to be a significant effort
in developing the program scope and outcome objectives with a comprehensive policy and
protocol implementation with continuous review. As discussed by Morganti et al. (2014),
MOBILE INTEGRATED HEALTH 47
medical oversight, strong training curriculums, and a comprehensive quality improvement
program are some of the recommended pillars for successful programs. Ensuring such measures
are in place limits the risk of mistakes, improves overall outcomes, and also helps prevent scope
creep.
The review of focus areas yielded common areas that appear to be problems in
communities across the nation. The focus areas identified by Zavadsky and Hooten (2016), as
well as NAEMT (2018), were like those identified in the survey sent to agencies outside LCFD.
The respondents to the survey showed similar demographics to the organizations represented.
The author found that the commonalities listed in the survey and text could have been better
investigated if the surveys were not anonymous. Additionally, follow up with each of the
responding agencies may have yielded additional characteristics of successful programs beyond
those identified in the literature review, or further supported them similar to how the focus areas
identified were supported.
The survey sent to local providers highlights the perceptions that most providers feel the
identified focus areas can be effective in reducing unnecessary emergency room visits. A
reduction in unnecessary emergency room visits using integrated healthcare measures benefits
both the patient and the community. Alakeson, Pande and, Ludwig (2010) noted that emergency
room boarding for unnecessary emergency room visits decreases the quality of care to those
awaiting care for significant emergencies. This may correlate to the enthusiasm displayed in the
perceived effectiveness of several of the programs from physicians/nurse practitioners in the
clinic setting.
The focus areas that were identified by Zavadsky and Hooten (2016) in several of the
programs highlighted, in no particular order, were alternative transport programs, hospital
MOBILE INTEGRATED HEALTH 48
readmission prevention, social system navigation, and mental health response and fall prevention
programs. Such programs also yielded the highest perceived effectiveness among the local
providers in reducing unnecessary emergency room visits. Morganti et al. (2014) noted that
alternative transport programs are one of the innovative EMS programs being performed. As of
the writing of this section, LCFD received a grant to seek transport vouchers to minimize 911
usage for non-emergency situations. Stowell (2016) noted that a barrier to appropriate care is
often attributed to lack of transportation, making transport to the emergency room via ambulance
a convenient option. Seattle and King County EMS saved an estimated $750,000 to the local
health system using alternative transport programs (Morganti et al., 2014).
A staple for MIH programs has been hospital readmission prevention where the program
aligns with an accountable care organization based on a fee for service schedule since it has
yielded the most consistent funding source for MIH programs across the nation. The Center for
Medicare and Medicaid Services (CMS) has the Hospital Readmissions Reduction Program
(HRRP) which was mandated by Section 3025 of the Affordable Care Act (ACA) and requires
payment reductions or penalties for excessive readmissions (CMS, 2019). Over 75 percent of
MIH/CP programs have hospital readmission reduction programs as a focus area (NAEMT,
2018). There appears to be a significant amount of opportunity in readmission reduction
programs in the United States with nearly 20 percent of all Medicaid fee-for-service patients
being readmitted within 30 days of discharge from the hospital, costing hospitals a significant
amount of money (NAEMT, 2018). Readmission prevention programs had the highest ranked
score when ranked among the other programs and the second highest perceived effectiveness at
reducing unnecessary emergency room visits by local providers. The findings of both surveys
support the literature.
MOBILE INTEGRATED HEALTH 49
The research performed as part of this ARP showed that social system navigation had
become one of the primary focus areas of LCFD along with repeat 911 use. The author feels this
research displayed evidence that the extent of scope creep has not been realized by LCFD since
the initial intent of the program was to reduce repeat 911 calls yet most of the referrals to
LCFD’s MIH program are not repeat 911 users. Social system navigation is an important
component to reducing repeat 911 use, however. Stowell (2016) noted, that perceived barriers to
care due to lack of knowledge leads to 911 use for non-emergency situations as it is the path of
least resistance for many. Additionally, low income/socioeconomic status is also an indicator of
health system navigation barriers (Stowell, 2016).
Mental health response accounts for a significant number of incidents in the City of Las
Cruces. Despite the lack of incidents LCFD responded to, the City reported nearly 1,900
incidents in 2017 and had a handful of fatal encounters with police in 2018. Locally, mental
health programs are perceived to be able to provide a significant reduction in unnecessary
emergency room visits. Such a program can vary widely in scope based on the needs and
available resources of the community. Research shows that deliberate attempts to reduce
unnecessary visits to the emergency room can be effective, supporting the perceived
effectiveness of a program the local providers felt. The current state in the City of Las Cruces is
representative of the case noted by Bronsky, Giordano, and Johnson (2016), where the care of
the patient is merely transferred from one agency that is ill-prepared to another. The City of
Colorado Springs was able to decrease ED transports of their patients by over 85 percent through
the use of a Community Emergency Response Team (CERT) (Bronsky, Giordano, & Johnson,
2016). Trivedi et al. (2018) noted that when a diversion program exists, EMS agencies have been
shown to successfully diver over 40 percent of mental health encounters, freeing up necessary

MOBILE INTEGRATED HEALTH 50
beds for emergencies since less than 0.3 percent of mental health patients seen in the emergency
room required any emergency interventions.
While fall prevention programs ranked toward the middle of perceived effectiveness both
individually and when ranked by local providers, they account for over ten percent of LCFD’s
incidents. Additionally, the deaths from falls rate in New Mexico is 1.8 times higher than the
national average at 97.6 people per 100,000 population as compared to 53.4 people per 100,000
population in 2011, respectively (NMDOH, 2014). The author believes proactive programs that
are focused on identifying risks and providing solutions may provide relief in the number of falls
experienced in the City of Las Cruces. Theut (2017) believes that fall prevention has a significant
education component that starts with adults at all ages as knowledge of the problem and
repercussions of such incidents can trigger changes in people’s attitudes toward falls. This
sentiment is shared by the author.
One area that was of surprise to the author was opioid outreach. Not only was the
perceived effect on the lower end based on the responses to the local survey, but the incident data
was also very low. This was an area where the author’s perceptions were not supported by the
provider perceptions or the incident data in the City of Las Cruces. The author fell victim to the
constantly reported “Opioid Epidemic” and made assumptions that Las Cruces, less than 50
miles from the border, was guaranteed to have such problems. While it may be for certain sub-
populations, it does not appear to be a significant problem for the City of Las Cruces based on
incident data and provider perception, or it is grossly underreported in the area.
Overall, LCFD’s MIH program has started on the right track and its successes have
generated community interest in the program. The research performed highlighted the positive
attitude about MIH programs in the City of Las Cruces and is hopefully reflective of a
MOBILE INTEGRATED HEALTH 51
willingness to continue building community partnerships geared toward improving the quality of
life of its citizens. MIH provides a framework for positive community interactions and greater
patient satisfaction with their healthcare system experience (Zavadsky & Hooten, 2016). The
author believes this research shows a need for expansion and to proactively seek ways of
improving the quality of life for its citizens while creating positive outcomes for all involved.
LCFD incident data points to several areas where targeted efforts may have significant positive
impacts on the community.
Recommendations
The purpose of this applied research project was to identify additional focus areas that
LCFD MIH program may consider expanding their services to, based on a review of the
characteristics of successful MIH/CP focus areas, identification of focus areas addressed by other
departments, and a comparison of the identified focus areas to the incident data and perceived
effectiveness by local providers. The research and review of the literature identified several
common areas that MIH programs have focused that are also relevant to LCFD. Based on the
results of this research, the following are recommended.
The first recommendation is LCFD conduct a comprehensive study on the cost of
services provided to the public based on available budgetary information, incident data, and
operational expenditures. Having a clear understanding of the costs of services provided to the
citizen will also allow for the calculation of the opportunity costs of implementing a program or
expanding MIH focus areas for LCFD. Organizations seeking to expand their services or add
programs will be faced with similar challenges to those presented in this ARP with limited
literature on the cost of response or a framework for the individual organization to quantify the
costs and benefits of their respective programs.
MOBILE INTEGRATED HEALTH 52
The second recommendation is LCFD establish clear program objectives for MIH with
each focus area clearly defined in its scope and objectives. This research provided insight into
the current state of LCFD’s MIH program concerning scope creep, and the lack of using the
program to reduce unnecessary repeat 911 calls. In the realm of establishing a clear scope and
objectives, this ARP is not de-emphasizing LCFD’s MIH program’s effectiveness at its current
state when looking at the value to the community. It has, however, morphed to more of a social
referral program with many clients having never been identified as a repeat 911 user, requiring
an evaluation and revision of the current program’s scope and objectives. Minimizing creep will
allow resources to be utilized and tracked effectively to ensure adequate unit hour utilization.
The last recommendation is that the focus areas considered be considered at a community
level, irrespective of the obvious financial benefits of LCFD, taking in to account the end-user
benefit. This ARP highlighted how incidents such as psychiatric/behavioral incidents, while they
are a small number of incidents for LCFD, they are a larger issue for the community at large.
Additionally, it is evident through this research how reducing unnecessary ED visits impacts the
entire community with improved access to emergency care and decreased costs of care for those
diverted from an unnecessary ED visit. Ensuring stakeholders at all levels are accounted for will
help LCFD implement programs of social benefit, where hours spent have a direct impact on
quality of life for its citizens in need. Should the recommendations presented be approved and
implemented, a framework for successful focus area expansion should be realized.
The above recommendations seek to ensure the focus areas yield the greatest return on
investment through improving the quality of life of the citizens of Las Cruces. Researchers
seeking to replicate this study should consider the specific need of their respective communities
based on a risk analysis and utilize available literature and external information to supplement
MOBILE INTEGRATED HEALTH 53
and support the needs of the community. The anonymity of respondents for this research proved
to be unnecessary and limited the content potential for review. Future research should provide
opportunities for follow-up with survey respondents.
MOBILE INTEGRATED HEALTH 54
References:
Alakeson, V., Pande, N., Ludwig, M. (2010). A health plan to reduce emergency room
“boarding” of psychiatric patients. Health Affairs, 29(9), 1637-1642. Retrieved from:
https://www.healthaffairs.org/doi/10.1377/hlthaff.2009.0336
Boyd, R. C. (2009). Local public sector allocation of scarce emergency assets: An evaluation of
the fire service [Doctoral Dissertation]. Retrieved from:
https://usfa.kohalibrary.com/app/work/181690
Bronsky, S., Giordano, K., Johnson, R. (2016). Mobile integrated healthcare program changing
how ems responds to behavioral health crises. Journal of Emergency Medical Services,
41(10). Retrieved from: https://www.jems.com/articles/print/volume-41/issue-
10/features/mobile-integrated-healthcare-program-changing-how-ems-responds-to-
behavioral-health-crises.html
Brown, A. C. (2015). Evaluation of mobile integrated healthcare program implementation for the
Nashville Fire Department. Executive Fire Officer Program: Applied Research Project.
Emmitsburg, MD: National Fire Academy. Retrieved from: https://nfa.usfa.fema.gov/pdf/
efop/efo48967.pdf
Canton, L.G. (Aug. 7, 2013). All-hazards doesn’t meant plan for everything [Blog]. Emergency
Management. Retrieved from: http://www.govtech.com/em/emergency-blogs/managing-
crisis/Allhazards-Doesnt-Mean-Plan-for-Everything.html
Castillo, D.J., Myers, J.B., Mock, J., Beck, E.H. (2016). Mobile integrated healthcare:
Preliminary experience and impact analysis with a Medicare Advantage population.
Journal of Health and Outcomes Research, 6(2), 172-187. Retrieved from:
MOBILE INTEGRATED HEALTH 55
https://www.evolution.net/resources/articles-case-studies-white-papers/mih-preliminary-
experience-and-impact-analysis-wit.pdf
Center for Medicare & Medicare Services (CMS). (2019). [Website]. Retrieved from:
https://www.cms.gov/Medicare/Medicare-Fee-for-Service-
Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html
City of Las Cruces. (2016). Las Cruces Fire Department 2015-2016 Report to the Community.
Retrieved from: http://www.las-cruces.org/~/media/lcpublicwebdev2/site%20documents
/article%20documents/fire%20department/fireannrept2016%20fweb.ashx?la=en
Druss, B., Walker, E. (2011). Mental disorders and medical comorbidity [Research Synthesis
Report No. 21]. Princeton, NJ: Robert Wood Johnson Foundation.
Haynes, H.J., Stein, G.P. (2017). U.S. fire department profile-2015. Quincy, MA: National Fire
Protection Association. Retrieved from: https://www.nfpa.org/-/media/Files/News-and-
Research/Fire-statistics-and-reports/Emergency-responders/osfdprofile.pdf
Hometown Health. (n.d.). Hometown Health Hotline [website]. Retrieved from: http://www.one-
healthcare.com/hometown-health/
International Association of Fire Chiefs (IAFC). (2017). Handbook on Mobile Integrated
Healthcare. Chantilly, VA: IAFC. Retrieved from: https://www.iafc.org/topics-and-
tools/resources/resource/mih-handbook
Kopp, B., Ofstead, C. (2010). The burden of falls in Wisconsin. Madison, WI: Wisconsin
Department of Health Services.
MOBILE INTEGRATED HEALTH 56
Kostyrka, M. (2018). Feasibility and effectiveness of a quick response vehicle for medical
emergencies in the City of Winston-Salem. Executive Fire Officer Program: Applied
Research Project. Emmitsburg, MD: National Fire Academy. Retrieved from:
https://nfa.usfa.fema.gov/pdf/efop/efo245244.pdf
Mason, S., Knowles, E., Colwell, B., Dixon, S., Wardrope, J., Gorringe, R., Snooks, H., Perrin,
J., Nicholl, J. (2007). Effectiveness of paramedic practitioners in attending 999 calls from
elderly people in the community: cluster randomized controlled trial. BMJ, 335(7626).
Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2048868/pdf/bmj-335-
7626-res-00919-el.pdf
Mobile Integrated Healthcare Practice Collaborative (MIHCP). (2014). Principles for
Establishing a Mobile Integrated Healthcare Practice. Minneapolis, MN: Medtronic
Philanthropy.
Morganti, K.G., Alpert, A., Margolis, G., Wasserman, J., Kellermann, A.L. (2014). The state of
innovative emergency medical service programs in the United States. Prehospital
Emergency Care, 18(1), 76-85. doi: 10.3109/10903127.2013.831508
Moss, C. (2018). State of mental health in New Mexico. Santa Fe, NM: New Mexico Department
of Health. Retrieved from: https://nmhealth.org/data/view/general/2193/
National Association of Emergency Medical Technicians (NAEMT). (2015). Mobile integrated
healthcare and community paramedicine (MIH-CP): A national survey. Clinton, MS:
NAEMT.
MOBILE INTEGRATED HEALTH 57
National Association of Emergency Medical Technicians (NAEMT). (2018). Mobile integrated
healthcare and community paramedicine (MIH-CP): 2nd national survey. Clinton, MS:
NAEMT.
National Fire Academy (NFA). (2018). Executive Analysis of Community Risk Reduction
(5th ed.). Emmitsburg, MD: United States Fire Administration.
National Institute for Health Care Management. (2012). The concentration of healthcare
spending [Data brief], July 2012. Retrieved from: https://www.nihcm.org/pdf/DataBrief3
%20Final.pdf
Neeki, M. M., Dong, F., Avera, L., Than, T., Borger, R., Powell, J., Vaezazizi, R., Pitts, R.
(2016). Alternative destination transport? The role of paramedics in optimal use of the
emergency department. Western Journal of Emergency Medicine, 17(6), 690-97.
Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5102593/pdf/wjem-17-
690.pdf
New Mexico Department of Health (NMDOH) Office of Injury Prevention. (2014).
Unintentional Fall-Related Injuries Among Older Adults in New Mexico. Santa Fe, NM:
New Mexico Department of Health. Retrieved from:
https://nmhealth.org/data/view/injury/447/
Novant Health. (n.d.). Novant Health Care Line [website]. Retrieved from:
https://www.novanthealth.org/home/services/emergency/novant-health-care-line.aspx
O’Brian, A.J. (2017). Comparing staffing models for fire based mobile urgent medical services.
University of Arizona [Doctoral Dissertation]. Retrieved from:
http://hdl.handle.net/10150/626318
MOBILE INTEGRATED HEALTH 58
O’Meara, P., Ruest, M., Martin, A. (2015). Integrating a community paramedicine program with
local health, aged care and social services: An observational ethnographic study.
Australasian Journal of Paramedicine, 12(5). Retrieved from: http://www.ircp.info/
Portals/11/Downloads/Networks/Integrating%20a%20community%20paramedicine%20p
rogram.pdf?ver=2015-11-02-110923-000
Ornstein, K.A., Leff, B., Covinsky, K.E., Ritchie, C.S., Federman, A.D., Roberts, L., Kelley,
A.S., Siu, A.L., Szanton, S.L. (2015). Epidemiology of the homebound population in
the United States. Journal of the American Medical Association Internal Medicine,
175(7),1180–1186. doi:10.1001/jamainternmed.2015.1849.
Pearson, K., Gale, J., Shaler, G. (2014). The evidence for community paramedicine in rural
areas: State and local findings and the role of the state flex program. Flex Monitoring
Team: Rural Health Research Centers. Retrieved from https://www.naemt.org/Files
/MobileIntegratedHC/CP%20Policy%20Brief%202.pdf
Stanhope, V., Videka, L., Thorning, H., McKay, M. (2015). Moving toward integrated health:
An opportunity for social work. Social Work in Healthcare, 54(5), 383-407. Retrieved
from: http://dx.doi.org/10.1080/00981389.2015.1025122
Stowell, C. (2016). Integration of community paramedics into San Diego Fire-Rescue
Department. Executive Fire Officer Program: Applied Research Project. Emmitsburg,
MD: National Fire Academy. Retrieved from: https://nfa.usfa.fema.gov/pdf/efop/
efo49989.pdf
MOBILE INTEGRATED HEALTH 59
Strange, K. C. (2009). The problem of fragmentation and the need for integrative solutions.
Annals of Family Medicine, 7(2), 100-103. Retrieved from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2653966/
Theut, J. (2017). Ferndale fall prevention. Executive Fire Officer Program: Applied Research
Project. Emmitsburg, MD: National Fire Academy. Retrieved from:
https://nfa.usfa.fema.gov/pdf/efop/efo244516.pdf
Trivedi, T.K., Glenn, M., Hern, G., Schriger, D.L., Sporer, K.A. (2018). Emergency medical
services use among patients receiving involuntary psychiatric holds and the safety of an
out-of-hospital screening protocol to “medically clear” psychiatric emergencies in the
field, 2011 to 2016. Annals of Emergency Medicine, 73(1), 42-51. Retrieved from:
https://www.annemergmed.com/article/S0196-0644(18)31158-2/pdf
United States Census Bureau. (2017). Retrieved from: https://www.census.gov/quickfacts/
lascrucescitynewmexico
United States Fire Administration (USFA). (2014). Strategic plan: Fiscal years 2014-2018.
Retrieved from: https://www.usfa.fema.gov/downloads/pdf/publications/strategic_plan_
2014-2018.pdf
United States Fire Administration (USFA). (2015). NFIRS 5.0 Complete Reference Guide.
Emmitsburg, MD: United States Fire Administration. Retrieved from:
https://www.usfa.fema.gov/data/nfirs/support/documentation.html
USA.com. (2014). Retrieved from: http://www.usa.com/las-cruces-nm-population-and-races.htm
MOBILE INTEGRATED HEALTH 60
Waddington, C., Egger, D. (2008). Integrated health services- What and why (Technical Brief
No. 1). Geneva, Switzerland: World Health Organization (WHO).
Zavadsky, M., Hooten, D. (2016). Mobile integrated healthcare: Approach to implementation.
Burlington, MA: Jones and Bartlett Learning.
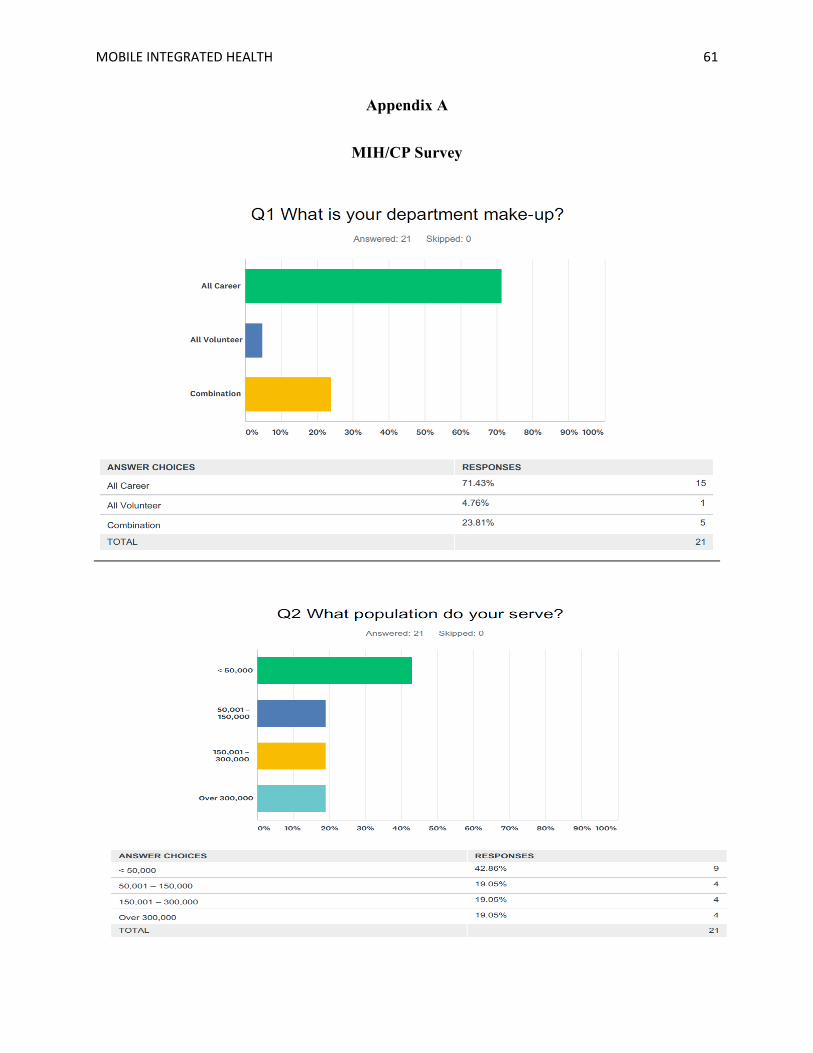
MOBILE INTEGRATED HEALTH 61
Appendix A
MIH/CP Survey
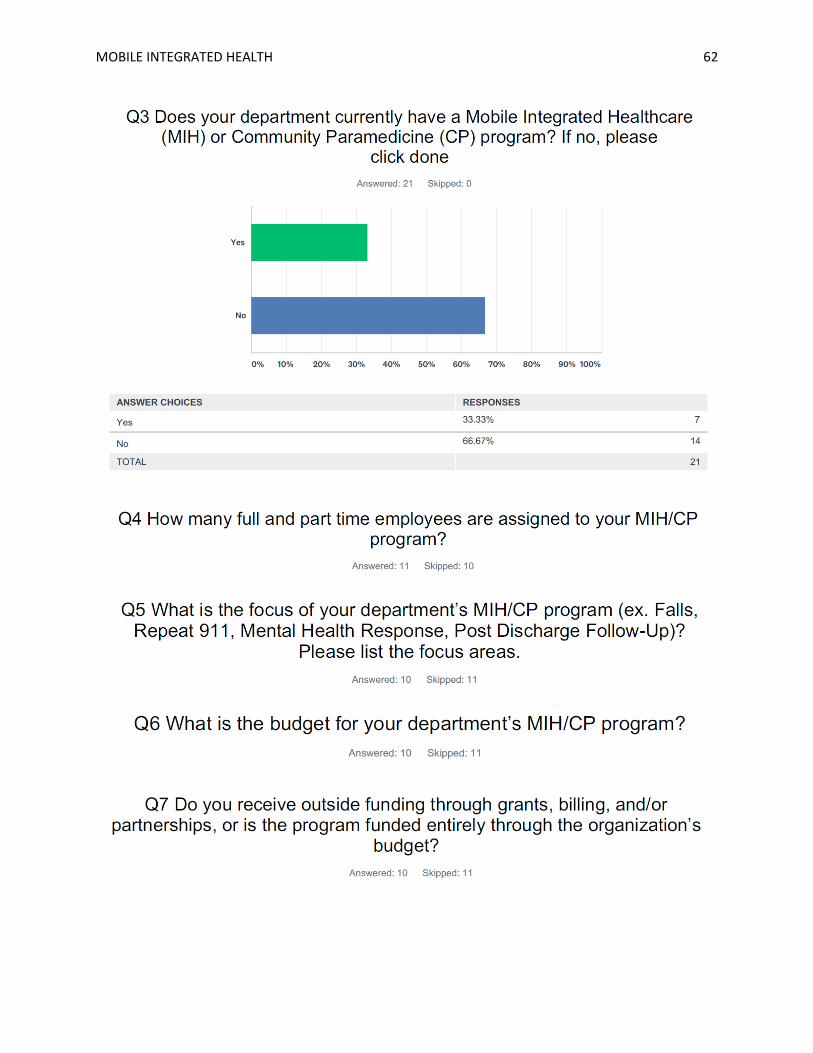
MOBILE INTEGRATED HEALTH 62
MOBILE INTEGRATED HEALTH 63
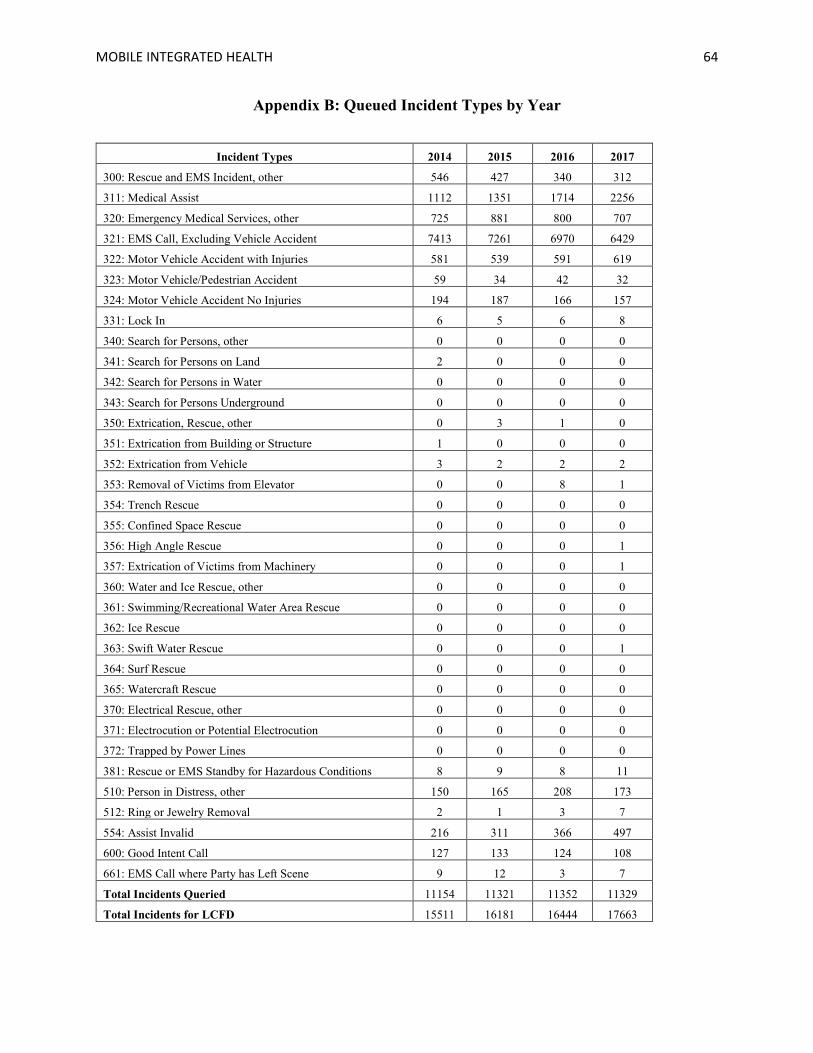
MOBILE INTEGRATED HEALTH 64
Appendix B: Queued Incident Types by Year
Incident Types 2014 2015 2016 2017
300: Rescue and EMS Incident, other 546 427 340 312
311: Medical Assist 1112 1351 1714 2256
320: Emergency Medical Services, other 725 881 800 707
321: EMS Call, Excluding Vehicle Accident 7413 7261 6970 6429
322: Motor Vehicle Accident with Injuries 581 539 591 619
323: Motor Vehicle/Pedestrian Accident 59 34 42 32
324: Motor Vehicle Accident No Injuries 194 187 166 157
331: Lock In 6 5 6 8
340: Search for Persons, other 0 0 0 0
341: Search for Persons on Land 2 0 0 0
342: Search for Persons in Water 0 0 0 0
343: Search for Persons Underground 0 0 0 0
350: Extrication, Rescue, other 0 3 1 0
351: Extrication from Building or Structure 1 0 0 0
352: Extrication from Vehicle 3 2 2 2
353: Removal of Victims from Elevator 0 0 8 1
354: Trench Rescue 0 0 0 0
355: Confined Space Rescue 0 0 0 0
356: High Angle Rescue 0 0 0 1
357: Extrication of Victims from Machinery 0 0 0 1
360: Water and Ice Rescue, other 0 0 0 0
361: Swimming/Recreational Water Area Rescue 0 0 0 0
362: Ice Rescue 0 0 0 0
363: Swift Water Rescue 0 0 0 1
364: Surf Rescue 0 0 0 0
365: Watercraft Rescue 0 0 0 0
370: Electrical Rescue, other 0 0 0 0
371: Electrocution or Potential Electrocution 0 0 0 0
372: Trapped by Power Lines 0 0 0 0
381: Rescue or EMS Standby for Hazardous Conditions 8 9 8 11
510: Person in Distress, other 150 165 208 173
512: Ring or Jewelry Removal 2 1 3 7
554: Assist Invalid 216 311 366 497
600: Good Intent Call 127 133 124 108
661: EMS Call where Party has Left Scene 9 12 3 7
Total Incidents Queried 11154 11321 11352 11329
Total Incidents for LCFD 15511 16181 16444 17663

MOBILE INTEGRATED HEALTH 65
Appendix C: Queued Condition Codes by Year
PCR Call Data 2014 2015 2016 2017 Totals Avg. / Year
Percent of Avg.
Total Patient Reports 9415 8844 8296 7,120 33675 8418.75 Not Known, Not Reporting, Not Applicable, Not Available 2534 2215 1680 712 7141 1785.25 21.206%
Pain (8030) 879 825 961 1204 3869 967.25 11.489%
Trauma (8043-8050) 910 855 823 635 3223 805.75 9.571%
Difficulty Breathing (8010) 647 586 673 593 2499 624.75 7.421%
Abdominal Pain (8001, 8002) 650 634 538 514 2336 584 6.937%
Cardiac Symptoms (8003, 8012, 8020, 8021, 8061) 628 531 594 547 2300 575 6.830%
Sick Person (8040) 445 447 500 536 1928 482 5.725%
Altered Level Consciousness (8016) 518 505 396 381 1800 450 5.345%
Convulsions/Seizures (8017) 374 378 321 348 1421 355.25 4.220%
Unconscious/Syncope/Dizziness (8042) 318 305 331 336 1290 322.5 3.831%
Alcohol Intoxication or Drug Overdose (8034,8035) 314 326 270 255 1165 291.25 3.460%
Psychiatric (8038, 8039) 202 207 161 130 700 175 2.079%
Blood Glucose (8008) 159 183 153 148 643 160.75 1.909%
Back Pain (8031, 8032) 131 124 133 101 489 122.25 1.452%
Abnormal Skin/Vital Signs (8004/8005) 130 119 141 91 481 120.25 1.428%
Respiratory/Cardiac Arrest (8009,8011) 77 106 97 98 378 94.5 1.122%
Neurologic Distress (8029) 84 80 108 101 373 93.25 1.108%
Hemorrhage (8024) 70 80 89 70 309 77.25 0.918%
Non-Traumatic Headache (8019) 54 41 50 38 183 45.75 0.543%
Allergic Reaction (8006, 8007) 55 52 41 34 182 45.5 0.540%
Heat Exposure (8022, 8023) 29 29 23 30 111 27.75 0.330%
Pregnancy/OB (8037) 21 33 30 27 111 27.75 0.330%
Patient Safety (8068-8071) 33 26 25 20 104 26 0.309%
Dehydration (8041) 21 25 22 23 91 22.75 0.270%
Choking (8013) 18 21 29 19 87 21.75 0.258%
Poisons (8033) 19 23 24 12 78 19.5 0.232%
Eye Symptoms/Injury (8018, 8058) 17 15 18 27 77 19.25 0.229%
Animal Bites and Stings (8053, 8054) 13 17 16 29 75 18.75 0.223%
Medical Device Failure (8027,8028) 12 6 12 16 46 11.5 0.137%
Post Operative Procedure Complications (8036) 11 12 12 10 45 11.25 0.134%
Burns (8051, 8052) 13 8 6 6 33 8.25 0.098%
IV Meds Required (8063) 4 12 4 3 23 5.75 0.068%
Third Party Assistance Required (8067) 3 4 6 8 21 5.25 0.062%
Special Handling (8072-8074) 7 5 3 6 21 5.25 0.062%
Sexual Assault (8059, 8060) 5 3 2 3 13 3.25 0.039%
Cold Exposure (8014, 8015) 1 1 3 3 8 2 0.024%
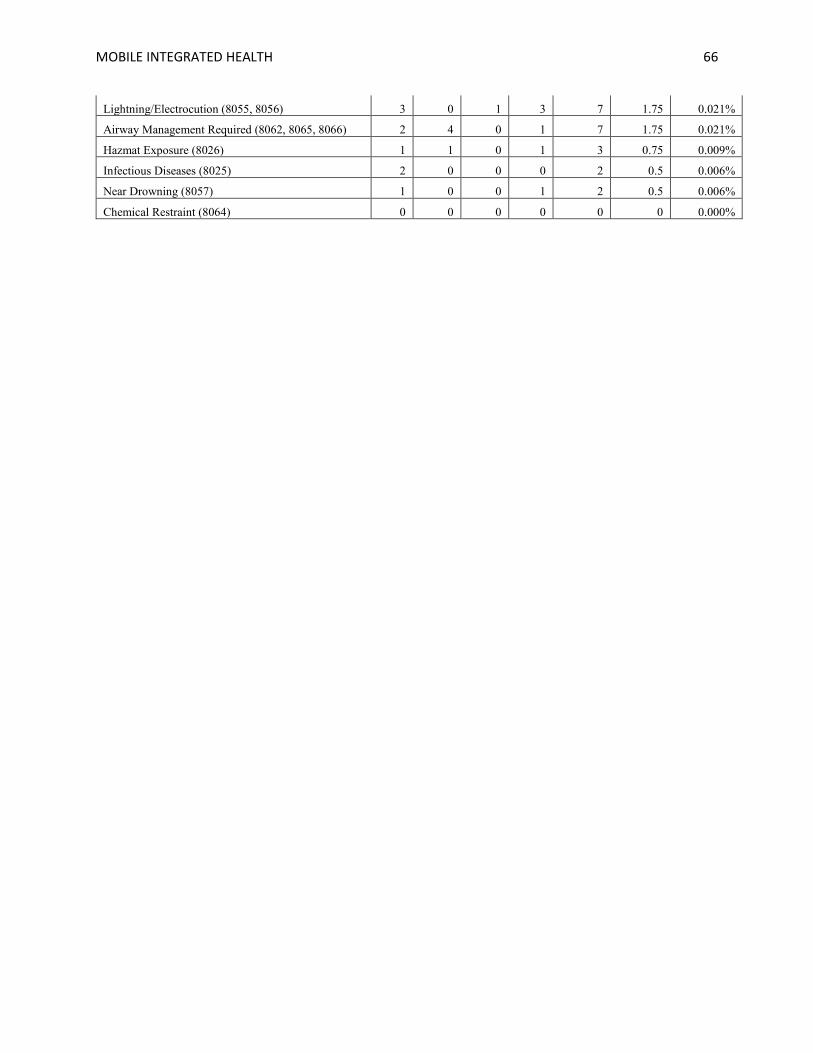
MOBILE INTEGRATED HEALTH 66
Lightning/Electrocution (8055, 8056) 3 0 1 3 7 1.75 0.021%
Airway Management Required (8062, 8065, 8066) 2 4 0 1 7 1.75 0.021%
Hazmat Exposure (8026) 1 1 0 1 3 0.75 0.009%
Infectious Diseases (8025) 2 0 0 0 2 0.5 0.006%
Near Drowning (8057) 1 0 0 1 2 0.5 0.006%
Chemical Restraint (8064) 0 0 0 0 0 0 0.000%
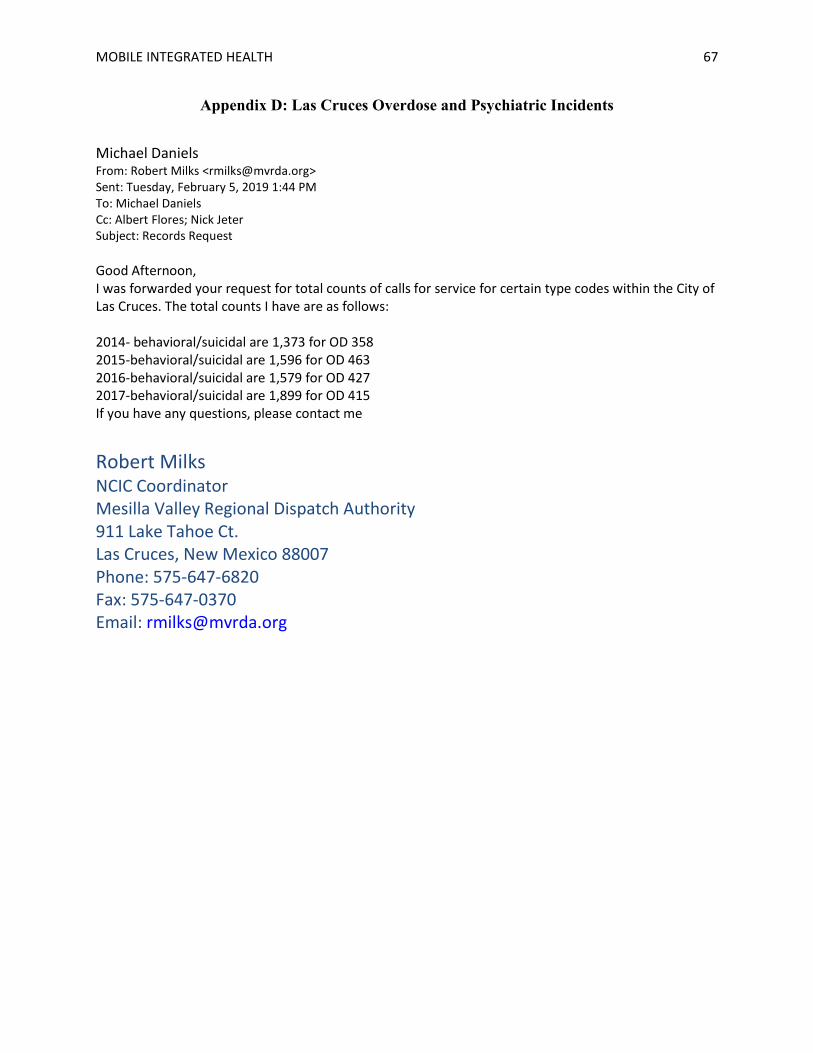
MOBILE INTEGRATED HEALTH 67
Appendix D: Las Cruces Overdose and Psychiatric Incidents
Michael Daniels From: Robert Milks <[email protected]> Sent: Tuesday, February 5, 2019 1:44 PM To: Michael Daniels Cc: Albert Flores; Nick Jeter Subject: Records Request Good Afternoon, I was forwarded your request for total counts of calls for service for certain type codes within the City of Las Cruces. The total counts I have are as follows: 2014- behavioral/suicidal are 1,373 for OD 358 2015-behavioral/suicidal are 1,596 for OD 463 2016-behavioral/suicidal are 1,579 for OD 427 2017-behavioral/suicidal are 1,899 for OD 415 If you have any questions, please contact me
Robert Milks NCIC Coordinator Mesilla Valley Regional Dispatch Authority 911 Lake Tahoe Ct. Las Cruces, New Mexico 88007 Phone: 575-647-6820 Fax: 575-647-0370 Email: [email protected]
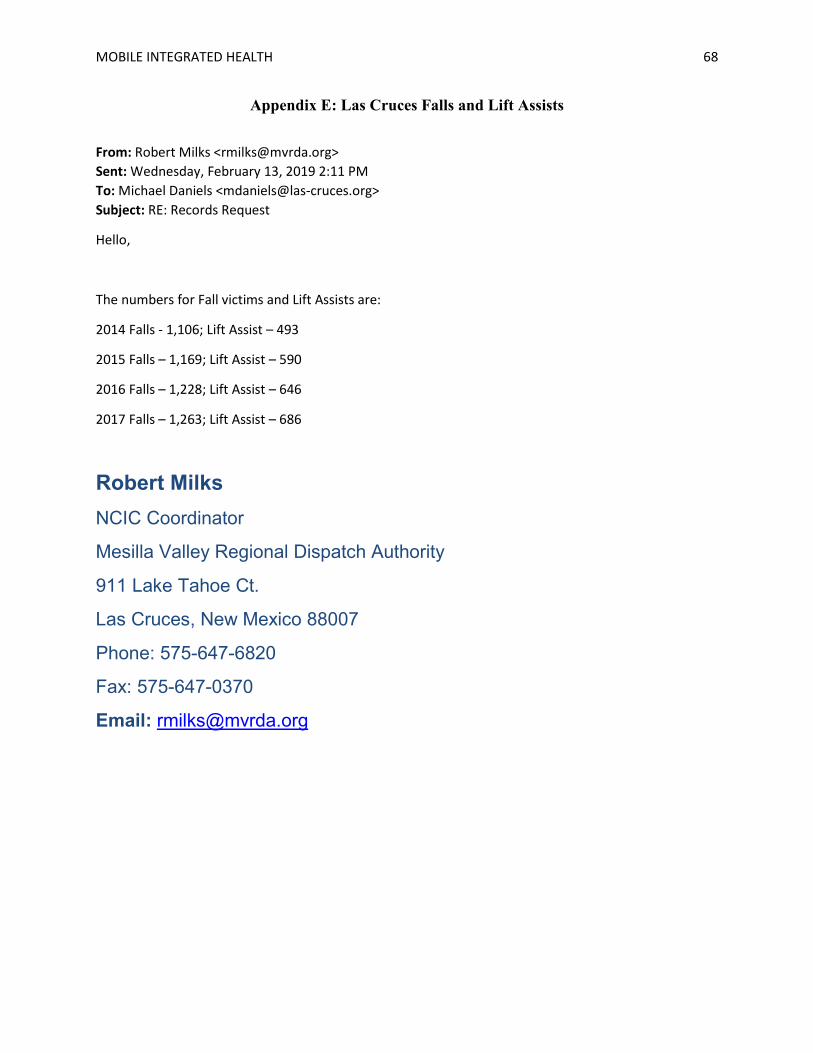
MOBILE INTEGRATED HEALTH 68
Appendix E: Las Cruces Falls and Lift Assists
From: Robert Milks <[email protected]> Sent: Wednesday, February 13, 2019 2:11 PM To: Michael Daniels <[email protected]> Subject: RE: Records Request
Hello,
The numbers for Fall victims and Lift Assists are:
2014 Falls - 1,106; Lift Assist – 493
2015 Falls – 1,169; Lift Assist – 590
2016 Falls – 1,228; Lift Assist – 646
2017 Falls – 1,263; Lift Assist – 686
Robert Milks NCIC Coordinator
Mesilla Valley Regional Dispatch Authority
911 Lake Tahoe Ct.
Las Cruces, New Mexico 88007
Phone: 575-647-6820
Fax: 575-647-0370
Email: [email protected]
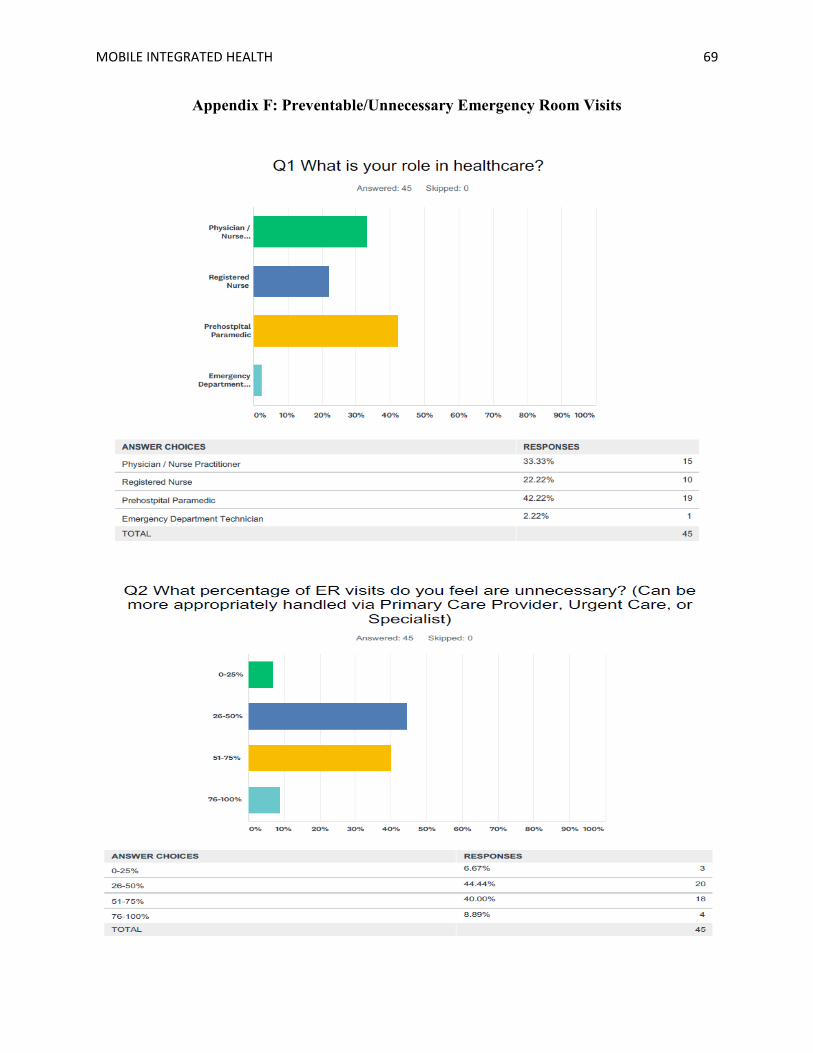
MOBILE INTEGRATED HEALTH 69
Appendix F: Preventable/Unnecessary Emergency Room Visits

MOBILE INTEGRATED HEALTH 70
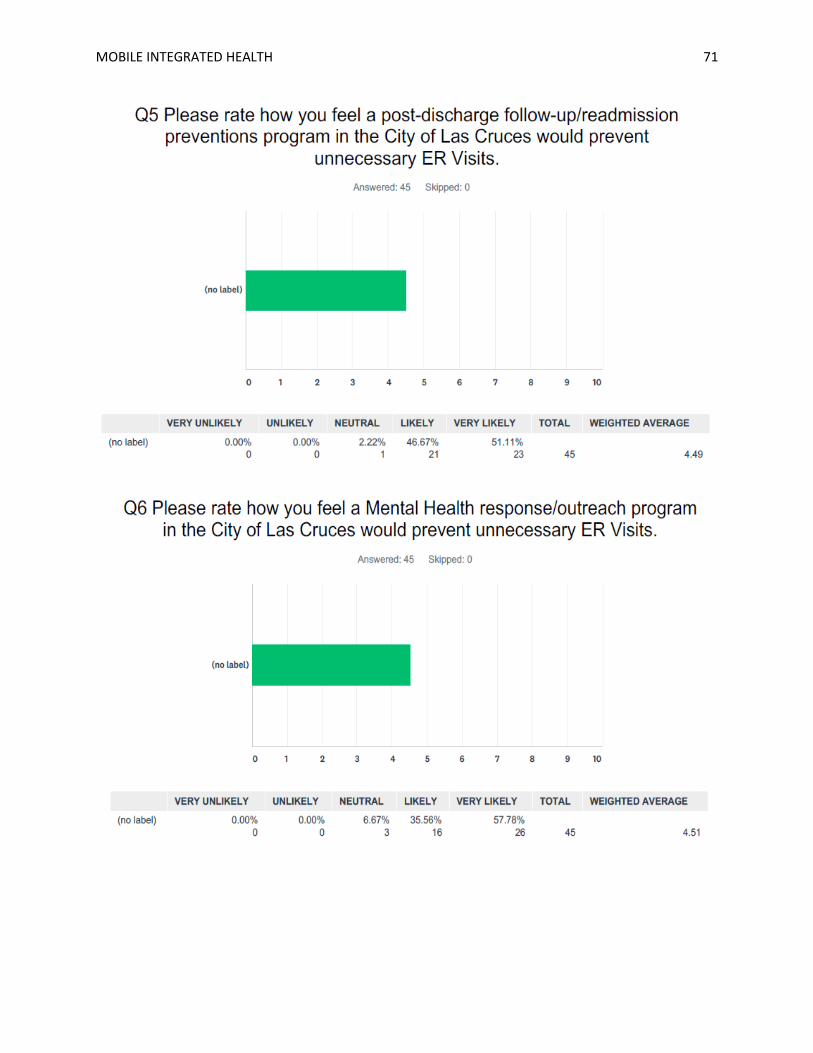
MOBILE INTEGRATED HEALTH 71
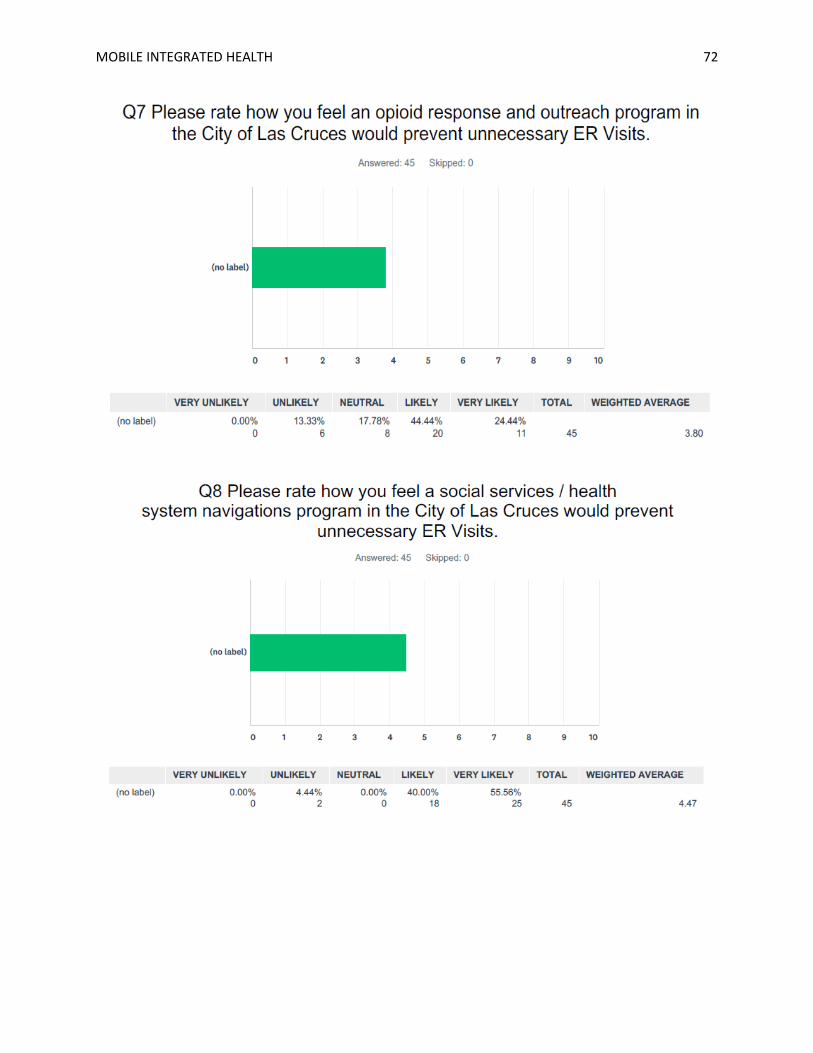
MOBILE INTEGRATED HEALTH 72
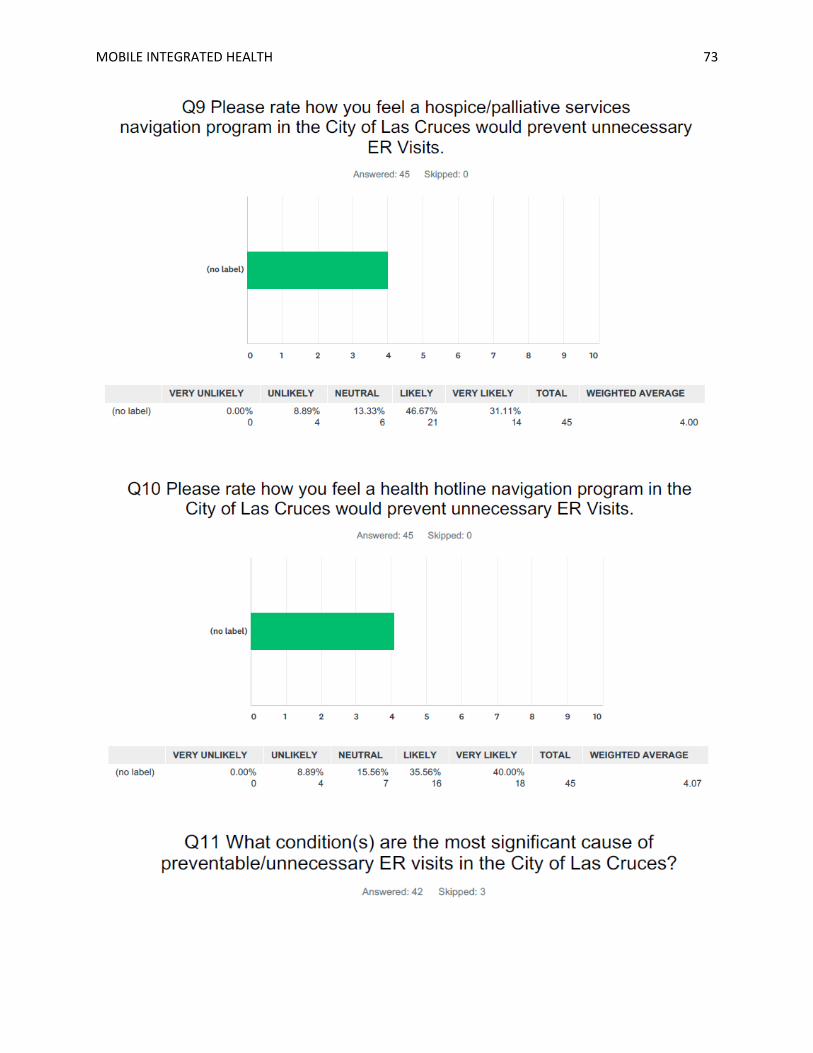
MOBILE INTEGRATED HEALTH 73

MOBILE INTEGRATED HEALTH 74