Embed Size (px)
Citation preview

IM2005, Vienna, April 2005 1
General Guidelines for the Assessment of Internal Dose from Monitoring Data (Project IDEAS)
H. Doerfel, FZK, KarlsruheA Andrasi, KFKI, Hungary
M Bailey, J Marsh, J Stather, NRPB, UKV Berkovski, RPI, Ukraine
C-M Castellani, ENEA, ItalyC Hurtgen, SCK•CEN, Belgium
J-R Jourdain, E Blanchardon, I Laniece, IRSN, FranceB LeGuen, EDF, France
I Malatova, RPI Czech Rep. (corresponding member)R Cruz-Suarez, J Zeger, IAEA (corresponding members)
IDEAS

IM2005, Vienna, April 2005 2
Background
Monitoring data
Assumptions:•Pathway of intake•Time course of intake•Biokinetic Model(s)•Parameter values for material & subject
Assumptions:•Pathway of intake•Time course of intake•Biokinetic Model(s)•Parameter values for material & subject
Influencing factors:•Amount and quality of data•Skill and experience of the dosimetrist•Computational tools available
Influencing factors:•Amount and quality of data•Skill and experience of the dosimetrist•Computational tools available
Intake & Committed Dose
General experience:When a set of bioassay data is given to two different assessors, it is likely that different assumptions will be made, and perhaps different methods applied and therefore that different results will be obtained.
General experience:When a set of bioassay data is given to two different assessors, it is likely that different assumptions will be made, and perhaps different methods applied and therefore that different results will be obtained.
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS

IM2005, Vienna, April 2005 3
What we have learned from recent intercomparison exercises
There is a clear need to develop guidelines on assessments of intake and internal doses, in order to promote harmonisation in assessments, especially, but not only, across the EU.
Such guidelines have formed the core of the IDEAS project.
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS

IM2005, Vienna, April 2005 4
Presentation to Intercomparison Workshop 18 April 2005
1: The IDEAS Project
2: The IDEAS guidelines
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS

IM2005, Vienna, April 2005 5
Cost-shared action in 5th FP42 Months: October 2001 – March 2005(extended to June 2005, to co-ordinate intercomparison exercisewith IAEA and this Workshop with IM 2005)
Cost-shared action in 5th FP42 Months: October 2001 – March 2005(extended to June 2005, to co-ordinate intercomparison exercisewith IAEA and this Workshop with IM 2005)
The project:
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
The aims:
To develop guidelines to standardise assessments of internaldoses
To develop guidelines to standardise assessments of internaldoses
By application of such guidelines, different assessors shouldobtain the same result from the same data
By application of such guidelines, different assessors shouldobtain the same result from the same data

IM2005, Vienna, April 2005 6
Work package 1Collection of
incorporation cases(C. Hurtgen)
Survey of open literatureSurvey of open literature
Contacts with industry and research institutionsContacts with industry and research institutions
Selection of cases for assessment by consortium(WP3)
Selection of cases for assessment by consortium(WP3)
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Bibliographic database•Compilation of references (author, year, title, journal)•Content: 547 references (mainly Health Phys. (229), Rad. Prot. Dos. (60))
Bibliographic database•Compilation of references (author, year, title, journal)•Content: 547 references (mainly Health Phys. (229), Rad. Prot. Dos. (60))
Incorporation case database•Detailed information (case description, monitoringresults, dose assessment)•Content: 209 cases
Incorporation case database•Detailed information (case description, monitoringresults, dose assessment)•Content: 209 cases

IM2005, Vienna, April 2005 7
Work package 1Collection of
incorporation cases
Work package 2Preparation of
evaluation software(V. Berkovski)
Investigate improved mathematical methods to assess intakes from monitoring data
Investigate improved mathematical methods to assess intakes from monitoring data
Implement in existing software (IMIE: RPI)
Implement in existing software (IMIE: RPI)
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Implementation of new features:• Mixed fractions of pathway of intake (inhalation, ingestion, injection)• Mixed fractions of absorption types (F, M and S)• Wound simulated as chronic injection and/or multiple injection• AMADs up to 20 micron• Import of individual retention and excretion functions
Implementation of new features:• Mixed fractions of pathway of intake (inhalation, ingestion, injection)• Mixed fractions of absorption types (F, M and S)• Wound simulated as chronic injection and/or multiple injection• AMADs up to 20 micron• Import of individual retention and excretion functions

IM2005, Vienna, April 2005 8
Work package 1Collection of
incorporation cases
Work package 2Preparation of
evaluation software
Work package 3Evaluation of
incorporation cases(C-M. Castellani)
Identification of factors and assumptions for whichguidance is needed
Identification of factors and assumptions for whichguidance is needed
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
•Evaluation of 52 cases (29 of them by 2 or more evaluators) •Application of both IMIE and IMBA ExpertTM
•Selection of the best estimates•Identification of important issues related to the guidelines
•Evaluation of 52 cases (29 of them by 2 or more evaluators) •Application of both IMIE and IMBA ExpertTM
•Selection of the best estimates•Identification of important issues related to the guidelines
Evaluation database•Compilation of all information (Word and Excel files)•Content: 95 independent evaluations of 52 cases
Evaluation database•Compilation of all information (Word and Excel files)•Content: 95 independent evaluations of 52 cases

IM2005, Vienna, April 2005 9
Work package 1Collection of
incorporation cases
Work package 2Preparation of
evaluation software
Work package 3Evaluation of
incorporation cases
Work package 4Development of
general guidelines(H. Doerfel)
Develop common approach for evaluation of monitoring data
Develop common approach for evaluation of monitoring data
Consider data handling (intake pattern, multiple data sets, errors, rogue data etc.)
Consider data handling (intake pattern, multiple data sets, errors, rogue data etc.)
Discuss with experts in open „Virtual“Workshop (1) on the Internet
Discuss with experts in open „Virtual“Workshop (1) on the Internet
Develop draft guidelines based on Workshop discussions
Develop draft guidelines based on Workshop discussions
Prepare report on draft guidelinesPrepare report on draft guidelines
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS

IM2005, Vienna, April 2005 10
Work package 4 (Development of general guidelines)
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Details and discussion in Part 2 of presentation
(later)
Details and discussion in Part 2 of presentation
(later)

IM2005, Vienna, April 2005 11
Special webpage (www.ideas-workshop.de) for posting the guidelinesSpecial webpage (www.ideas-workshop.de) for posting the guidelines
Virtual workshop for discussion of the guidelines with the community
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Discussion forum for every stage of the guidelines where anyone could place his (orher) comments
Discussion forum for every stage of the guidelines where anyone could place his (orher) comments
Start of the workshop on 31 May 2004; end is still openStart of the workshop on 31 May 2004; end is still open
Announcement of the workshop through contacts, relevant national and international organisations etc. (including IRPA Madrid)
Announcement of the workshop through contacts, relevant national and international organisations etc. (including IRPA Madrid)

IM2005, Vienna, April 2005 12
Statistics of the visits of the website (www.ideas-workshop.de) Statistics of the visits of the website (www.ideas-workshop.de)
Virtual workshop for discussion of the guidelines with the community
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Month Number of Visits
May 2004 188
June 2004 1140
July 2004 237
August 2004 209
September 2004 205

IM2005, Vienna, April 2005 13
Statistics of the visits of the discussion forumStatistics of the visits of the discussion forum
Virtual workshop for discussion of the guidelines with the community
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage Subject Visits Comments1 First check of data 207 102 Check of statistical
significance134 8
3 Standard procedure 109 34 Special procedure –
definition of pathways101 0
5 (5.1 – 5.3) Special procedure forinhalation
366 16
6 (6.1 – 6.3) Special procedure foringestion
238 2
7 (7.1 – 7.3) Special procedure forinhalation and ingestion
116 1
Total 1271 40

IM2005, Vienna, April 2005 14
Special webpage (www.ideas-workshop.de) for posting the guidelinesSpecial webpage (www.ideas-workshop.de) for posting the guidelines
Virtual workshop for discussion of the guidelines with the community
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Start of the workshop on 31 May 2004; end is still open,Continuation, linked to CONRAD FP6 Project (Carlo-Maria Castellani & Hans Doerfel)
Start of the workshop on 31 May 2004; end is still open,Continuation, linked to CONRAD FP6 Project (Carlo-Maria Castellani & Hans Doerfel)
Information exchange for internal dosimetry communityInformation exchange for internal dosimetry community
Develop guidelines furtherDevelop guidelines further

IM2005, Vienna, April 2005 15
Work package 1Collection of
incorporation cases
Work package 2Preparation of
evaluation software
Work package 3Evaluation of
incorporation cases
Work package 4Development of
general guidelines
Work package 5Practical testing
of general guidelines
Organise Joint Intercomparison Exercise on Internal Dose Assessment together with IAEA•Prepare, distribute cases & guidelines•Compile results
Organise Joint Intercomparison Exercise on Internal Dose Assessment together with IAEA•Prepare, distribute cases & guidelines•Compile results
Workshop (2) with participants to discuss results
Workshop (2) with participants to discuss results
Modify draft guidelines according to results of discussion
Modify draft guidelines according to results of discussion
Publish report and General GuidelinesPublish report and General Guidelines
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS

IM2005, Vienna, April 2005 16
General philosophybased on the evaluation (Work package 3)
General philosophybased on the evaluation (Work package 3)
Work package 4 (Development of general guidelines)
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Levels of taskbased on general philosophy
Levels of taskbased on general philosophy
General guidelines for the evaluationbased on „Level of task“ structure
General guidelines for the evaluationbased on „Level of task“ structure

IM2005, Vienna, April 2005 17
Harmonisation:by following the procedures any two assessors should obtain the same estimate of dose from a given data set
Harmonisation:by following the procedures any two assessors should obtain the same estimate of dose from a given data set
General philosophy
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Best estimate:the “best” estimate of dose should be obtained from the available data
Best estimate:the “best” estimate of dose should be obtained from the available data
Proportionality:the effort applied to the evaluation should be proportionate to the dose – the lower the dose, the simpler the process should be.
Proportionality:the effort applied to the evaluation should be proportionate to the dose – the lower the dose, the simpler the process should be.
Discussion point?
Sometimes there is conflict between these principles. Which has priority?

IM2005, Vienna, April 2005 18
The general guidelines provide
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS•processing of data before use,•handling of single data and multiple data sets,•number and type of data required for the dose assessment•assessment of the uncertainty on data, •handling of data below the limits of detection, •handling of data influenced by chelation therapy •and the identification of rogue data
•processing of data before use,•handling of single data and multiple data sets,•number and type of data required for the dose assessment•assessment of the uncertainty on data, •handling of data below the limits of detection, •handling of data influenced by chelation therapy •and the identification of rogue data
Detailed information about data handlingDetailed information about data handling
General information about the evaluation of the monitoring data reflecting the general philosophy
General information about the evaluation of the monitoring data reflecting the general philosophy
Structured approach to the dose assessment reflecting the levels of task.Structured approach to the dose assessment reflecting the levels of task.
IM2005, Vienna, April 2005 19
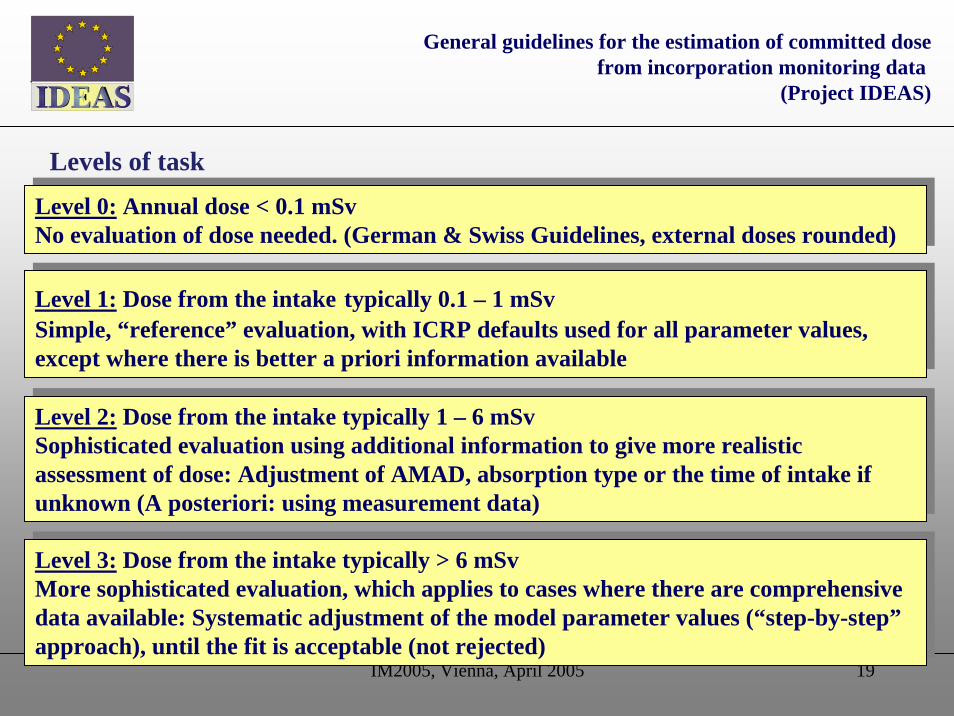
Level 0: Annual dose < 0.1 mSv No evaluation of dose needed. (German & Swiss Guidelines, external doses rounded)
Level 0: Annual dose < 0.1 mSv No evaluation of dose needed. (German & Swiss Guidelines, external doses rounded)
Levels of task
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Level 1: Dose from the intake typically 0.1 – 1 mSvSimple, “reference” evaluation, with ICRP defaults used for all parameter values, except where there is better a priori information available
Level 1: Dose from the intake typically 0.1 – 1 mSvSimple, “reference” evaluation, with ICRP defaults used for all parameter values, except where there is better a priori information available
Level 2: Dose from the intake typically 1 – 6 mSvSophisticated evaluation using additional information to give more realistic assessment of dose: Adjustment of AMAD, absorption type or the time of intake if unknown (A posteriori: using measurement data)
Level 2: Dose from the intake typically 1 – 6 mSvSophisticated evaluation using additional information to give more realistic assessment of dose: Adjustment of AMAD, absorption type or the time of intake if unknown (A posteriori: using measurement data)
Level 3: Dose from the intake typically > 6 mSvMore sophisticated evaluation, which applies to cases where there are comprehensive data available: Systematic adjustment of the model parameter values (“step-by-step”approach), until the fit is acceptable (not rejected)
Level 3: Dose from the intake typically > 6 mSvMore sophisticated evaluation, which applies to cases where there are comprehensive data available: Systematic adjustment of the model parameter values (“step-by-step”approach), until the fit is acceptable (not rejected)

IM2005, Vienna, April 2005 20
Stage 1 (Level 0)
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Single routine measurement, M
Compare with tabulated value MC
If measurement M< MC implies “Annual dose”(committed effective dose from intakes in year) <0.1 mSv; assuming similar intakes in all monitoring intervals.
Record dose = 0.0 mSv. Record measurement. STOP
Single routine measurement, M
Compare with tabulated value MC
If measurement M< MC implies “Annual dose”(committed effective dose from intakes in year) <0.1 mSv; assuming similar intakes in all monitoring intervals.
Record dose = 0.0 mSv. Record measurement. STOP

IM2005, Vienna, April 2005 21
Stage 1:Check of the need for evaluation
Stage 1:Check of the need for evaluation
Structured approach to dose assessment
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEASStage
1
1.1Identify monitoring value M
1.2M < Mc(1)
1.2.1Level 0:
No evaluation neededEnd
Stage 2
yesno
1.3Above Level 0:
Evaluation needed

IM2005, Vienna, April 2005 22
Stage 1 (Level 0) Step 1.1
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Identify measurement (M) and duration of monitoring interval (T)
Data treatment (if needed)
Other radionuclides present as well as „Indicator“ thatwas measured?
Identify measurement (M) and duration of monitoring interval (T)
Data treatment (if needed)
Other radionuclides present as well as „Indicator“ thatwas measured?

IM2005, Vienna, April 2005 23
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEASStage
1
1.1Identify monitoring value M
1.2M < Mc(1)
1.2.1Level 0:
No evaluation neededEnd
Stage 2
yesno
1.3Above Level 0:
Evaluation needed

IM2005, Vienna, April 2005 24
Step 1.2: Example of the critical monitoring quantity Mc
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Radionuclide Absorption
type (chemical
form)
Type of monitoring
Monitoring interval
(d)
Critical monitoring value MC
H-3
HTO
Urine
14 30 60
4400 Bq/d 5500 Bq/d 3900 Bq/d
Co-60
M
Whole body
90 180 360
160 Bq 230 Bq 290 Bq
Sr-90
F
Urine
90 180 360
0.4 Bq/d 0.2 Bq/d 0.2 Bq/d
I-131
F
Thyroid
7 14 30
18 Bq 26 Bq 26 Bq
Cs-137
F
Whole body
90 180 360
1200 Bq 1800 Bq 2000 Bq
U-235
S
Lungs
90 180 360
0.2 Bq < LLD 0.3 Bq < LLD 0.5 Bq < LLD
Pu-239
M
Urine
90 180 360
0.007 mBq/d < LLD0.011 mBq/d < LLD0.017 mBq/d < LLD

IM2005, Vienna, April 2005 25
Stage 2 (Level 1)
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Measurement M>MC
•Check whether M is significant:
•Need realistic estimate of uncertainty
•If so “reference” procedure (ICRP 78): Default
values, a priori parameter values, route of intake, etc.
•If “annual” dose <1 mSv (record dose) STOP
Measurement M>MC
•Check whether M is significant:
•Need realistic estimate of uncertainty
•If so “reference” procedure (ICRP 78): Default
values, a priori parameter values, route of intake, etc.
•If “annual” dose <1 mSv (record dose) STOP

IM2005, Vienna, April 2005 26
Stage 1:Check of the need for evaluation
Stage 1:Check of the need for evaluation
Structured approach of the dose assessment
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 2:Check of the significance of measurement and consistency with previous evaluations
Stage 2:Check of the significance of measurement and consistency with previous evaluations
Stage 2
2.1Assessment of uncertainty on
measured value M (or application of default uncertainty)
2.2Calculation of contributions from
previous intakes (P)
2.3M > SF*P
Stage 3
2.4P/SF < M < P*SF End
2.3.1There is a new significant intake; calculation of net measured value
N = M - P
2.4.1There is no new significant intake
(confirmation of previous assessments)
2.5There is a discrepancy with previous
evaluations
2.6Value is reliable
2.7Make corrections on the measured value, if possible; otherwise repeat
measurement
2.6.1Special evaluation of
previous intakes needed
Stage 4
Yes
No
Yes
No
Yes
No

IM2005, Vienna, April 2005 27
Stage 2 (Level >0) Step 2.1
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Assess overall uncertainty on measurement:• New intake?•Consistent with previous intakes?•(Rogue point: inconsistent with other data?)•(Weighting in fitting more than one measurement)•(Objective criteria to determine whether model fitsdata) •(Objective criteria to choose between models)
Assess overall uncertainty on measurement:• New intake?•Consistent with previous intakes?•(Rogue point: inconsistent with other data?)•(Weighting in fitting more than one measurement)•(Objective criteria to determine whether model fitsdata) •(Objective criteria to choose between models)

IM2005, Vienna, April 2005 28
Stage 2 (Level >0) Step 2.1
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Assess overall uncertainty on “measurement” for
comparison with model (Scattering Factor, SF):
•Type A (Poisson counting statistics) and Type B (other)
•Measurement of activity in sample (or in organs) and its
use to estimate modelled activity (e.g. daily excretion
rate), sampling errors, biological variability
Assess overall uncertainty on “measurement” for
comparison with model (Scattering Factor, SF):
•Type A (Poisson counting statistics) and Type B (other)
•Measurement of activity in sample (or in organs) and its
use to estimate modelled activity (e.g. daily excretion
rate), sampling errors, biological variability

IM2005, Vienna, April 2005 29
Stage 2 (Level >0) Step 2.1
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Guidance on estimating SF:
•Log-normal. Not exact, but pragmatic (approximate
better than nothing, or only some contributions)
•Some details available for in vivo measurements
•General defaults (Table 2.3, Guthrie Miller) excretion
etc. based on plutonium.
Guidance on estimating SF:
•Log-normal. Not exact, but pragmatic (approximate
better than nothing, or only some contributions)
•Some details available for in vivo measurements
•General defaults (Table 2.3, Guthrie Miller) excretion
etc. based on plutonium.

IM2005, Vienna, April 2005 30
Step 2.1: Default values for the components of log-normal uncertainty for various types of measurement
Quantity SF
true 24-hr urine 1.1simulated 24-hr urine, specific gravity normalization 1.3
spot urine sample 2.0
fecal sample 3 to 7
chest count 1.2 to 1.6
nasal swipe 3 to 7
room air monitor 7 to 20
Discussion point!!!•excretion etc. based on plutonium.
•Need more: typical SF for other radionuclides -
•contributions please!!!

IM2005, Vienna, April 2005 31
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 2
2.1Assessment of uncertainty on
measured value M (or application of default uncertainty)
2.2Calculation of contributions from
previous intakes (P)
2.3M > SF*P
Stage 3
2.4P/SF < M < P*SF End
2.3.1There is a new significant intake; calculation of net measured value
N = M - P
2.4.1There is no new significant intake
(confirmation of previous assessments)
2.5There is a discrepancy with previous
evaluations
2.6Value is reliable
2.7Make corrections on the measured value, if possible; otherwise repeat
measurement
2.6.1Special evaluation of
previous intakes needed
Stage 4
Yes
No
Yes
No
Yes
No
Discussion Point!
P/SF2<M<P*SF2
chance of false intakes or inconsistency >30%
Use eg SF2 ?

IM2005, Vienna, April 2005 32
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 2
2.1Assessment of uncertainty on
measured value M (or application of default uncertainty)
2.2Calculation of contributions from
previous intakes (P)
2.3M > SF*P
Stage 3
2.4P/SF < M < P*SF End
2.3.1There is a new significant intake; calculation of net measured value
N = M - P
2.4.1There is no new significant intake
(confirmation of previous assessments)
2.5There is a discrepancy with previous
evaluations
2.6Value is reliable
2.7Make corrections on the measured value, if possible; otherwise repeat
measurement
2.6.1Special evaluation of
previous intakes needed
Stage 4
Yes
No
Yes
No
Yes
No

IM2005, Vienna, April 2005 33
Stage 3 (Level > 0) Standard evaluation
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Measurement M due to new intake
•Confirm routine (not special, Stage 4)•Reference assumptions, as ICRP 78, eg. single intake(inhalation) at mid-point•Parameter values related to material (eg AMAD) ifknown before (a priori)
•If annual dose <1 mSv record and STOP
Measurement M due to new intake
•Confirm routine (not special, Stage 4)•Reference assumptions, as ICRP 78, eg. single intake(inhalation) at mid-point•Parameter values related to material (eg AMAD) ifknown before (a priori)
•If annual dose <1 mSv record and STOP
IM2005, Vienna, April 2005 34
Stage 1:Check of the need for evaluation
Stage 1:Check of the need for evaluation
Structured approach of the dose assessment
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 2:Check of the significance of measurement and consistency with previous evaluations
Stage 2:Check of the significance of measurement and consistency with previous evaluations
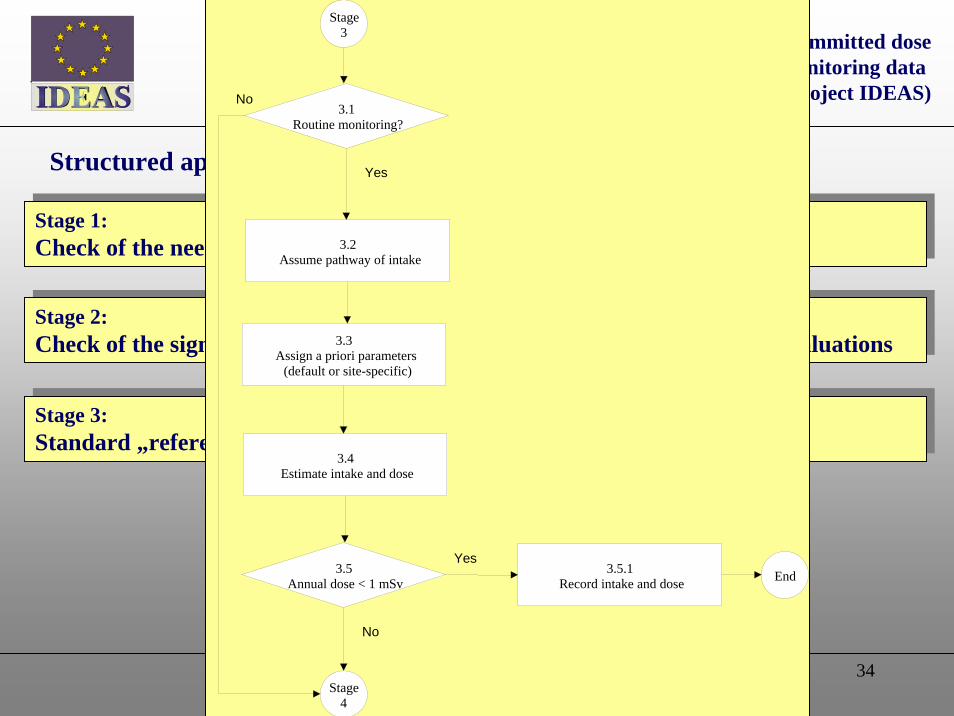
Stage 3:Standard „reference“ evaluation procedure
Stage 3:Standard „reference“ evaluation procedure
Stage 3
3.5Annual dose < 1 mSv
3.4Estimate intake and dose
End
Stage 4
3.2Assume pathway of intake
3.3Assign a priori parameters
(default or site-specific)
Yes
No
3.5.1Record intake and dose
3.1Routine monitoring?
No
Yes

IM2005, Vienna, April 2005 35
Stage 1:Check of the need for evaluation
Stage 1:Check of the need for evaluation
Structured approach of the dose assessment
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 2:Check of the significance of measurement and consistency with previous evaluations
Stage 2:Check of the significance of measurement and consistency with previous evaluations
Stage 3:Standard „reference“ evaluation procedure
Stage 3:Standard „reference“ evaluation procedure
Stage 4:Special evaluation procedure: Identification of pathway of intake
Stage 4:Special evaluation procedure: Identification of pathway of intake
Stage 4
4.1Pure inhalation?
Stage 5
Yes
No
4.1.1Special evaluation for inhalation
4.2Pure ingestion?
Stage 6
Yes4.2.1
Special evaluation for ingestion
4.3Inhalation and
ingestion?
Stage 7
Yes 4.3.1Special evaluation for inhalation and
ingestion
No
4.5.1The wound pathway not considered by the guidelines at the present state.
No
4.5Wound
involved?
No
Yes
4.4Injection or
skin absorption?
Stage 8
Yes4.4.1
Special evaluation for Injection
No
End

IM2005, Vienna, April 2005 36
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 4
4.1Pure inhalation?
Stage 5
Yes
No
4.1.1Special evaluation for inhalation
4.2Pure ingestion?
Stage 6
Yes4.2.1
Special evaluation for ingestion
4.3Inhalation and
ingestion?
Stage 7
Yes 4.3.1Special evaluation for inhalation and
ingestion
No
4.5.1The wound pathway not considered by the guidelines at the present state.
No
4.5Wound
involved?
No
Yes
4.4Injection or
skin absorption?
Stage 8
Yes4.4.1
Special evaluation for Injection
No
End
Discussion point!
Understand the case:•Plot graph of data•Hand calculation?
Room air contamination(Default)
External contamination
Room air and external contamination AND justification
Stage 4: Special Assessment
IM2005, Vienna, April 2005 37
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
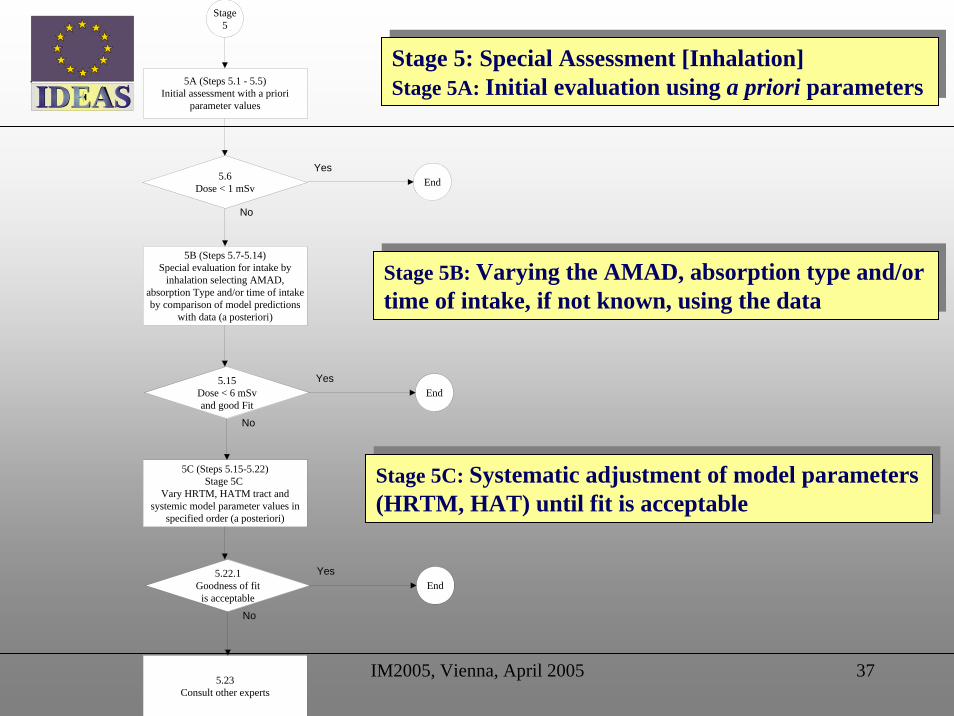
Stage 5
5A (Steps 5.1 - 5.5)Initial assessment with a priori
parameter values
5B (Steps 5.7-5.14)Special evaluation for intake by
inhalation selecting AMAD, absorption Type and/or time of intake by comparison of model predictions
with data (a posteriori)
5.6Dose < 1 mSv End
Yes
No
5C (Steps 5.15-5.22)Stage 5C
Vary HRTM, HATM tract and systemic model parameter values in
specified order (a posteriori)
5.15Dose < 6 mSvand good Fit
EndYes
No
5.23Consult other experts
5.22.1Goodness of fit
is acceptableEnd
Yes
No
Stage 5: Special Assessment [Inhalation]Stage 5A: Initial evaluation using a priori parameters
Stage 5: Special Assessment [Inhalation]Stage 5A: Initial evaluation using a priori parameters
Stage 5B: Varying the AMAD, absorption type and/ortime of intake, if not known, using the data
Stage 5B: Varying the AMAD, absorption type and/ortime of intake, if not known, using the data
Stage 5C: Systematic adjustment of model parameters(HRTM, HAT) until fit is acceptable
Stage 5C: Systematic adjustment of model parameters(HRTM, HAT) until fit is acceptable

IM2005, Vienna, April 2005 38
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 5A
5.1Identification of all measured data
representing the case
5.2Assessment of contributions from previous intakes and calculation of
net values of measured data
5.3Assign a priori parameters (default or site-specific)
5.5Calculate the dose with a priori
parameters
5.6Dose from intake
< 1 mSv
5.6.1Record dose with a priori parameters End
5.4Time of intake is known
No
Yes
Yes
Stage5B
No
5.6: If dose from intake <1 mSv,
•(for every measurement type)
•(for every radionuclide)
Record and STOP
Stage 5A: Special assessment
Inhalation: Standard evaluation
As Stage 3, but >1 measurement
5.4:
Routine measurement
•inconsistent with previous or
•standard evaluation, dose >1 mSv
5.5: Calculate intake (dose?) Ii from each measurement Mi
Best estimate = mean (Ii)

IM2005, Vienna, April 2005 39
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 5B:
Special assessment Inhalation:
vary AMAD, F/M/S, Time of intake
5A
5.8Time of intake
is known
5.9Early lung and faeces
data available
5.10Derive effective AMAD from early
lung and faeces data
5.11Assessment of dose by fitting of the
absorption type
5.12Assessment of dose by simultaneous fitting of both the time of intake and
the absorption type
5.7.1Get additional dose relevant data
5.7There are suffcient
relevant data
5.11.1Goodness of fit
is acceptable
5.13Assessment of dose by fitting of the mixture of default absorption types
(F,M,S)
5.14Assessment of dose by simultaneous fitting of both the time of intake and
the mixture of default absorption types (F,M,S)
5.12.3Record dose with all parameters
5.12.1Goodness of fit
is acceptable
5.11.2Dose from intake
< 6 mSv
5.11.4Check the number of data required for evaluation at this level and get more
data, if necessary(Table)
5.12.2Dose from intake
< 6 mSv
5.12.4Check the number of data required for evaluation at this level and get more
data, if necessary(Table)
No
No
Yes
No
Yes
No
Yes
Yes
NoYes
No
Yes
NoYes
No
5.11.3Record dose with all parameters
Stage5B
Stage5CEnd End
Stages 5A & 5B: select parameter values by fitting model predictions to the data
Procedure stops when model fits, i.e. data do not reject model.
Easy if few data, hence steps 5.6, 5.11.4, 5.12.4:
Are there enough data ?
Depends on dose

IM2005, Vienna, April 2005 40
Criteria for rejecting fit: Discussion Point!!!
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Model should fit data for unbiased estimateProposed criteria for rejecting fit:•Chi-squared test statistic: 1% level if dose <6 mSv; 5% level if dose >6 mSv; OR•Fit looks unreasonable by eye (series of data under-or over-estimated.
Model should fit data for unbiased estimateProposed criteria for rejecting fit:•Chi-squared test statistic: 1% level if dose <6 mSv; 5% level if dose >6 mSv; OR•Fit looks unreasonable by eye (series of data under-or over-estimated.

IM2005, Vienna, April 2005 41
Number and type of data needed for assessment of dosefor selected radionuclides and monitoring procedures
Required m onitoring data
D < 1 m Sv
1 m Sv < D < 6 m Sv
D > 6 m Sv
Radio- nuclide
Type of m onitoring
Num ber Tim e range
(days) Num ber Tim e range
(days) Num ber Tim e range
(days)
H-3 Urine 1 - 3 14 5 14
Co-60 W hole body 1 - 3 30 5 30
S r-90 Urine Faeces
1 - 3 30 3 3
30 30
Ag-110m I-125 I-131 Th yroid
Urine 1 - 3 7 3
3 7 7
Cs-137 W hole body 1 - 3 90 5 90
U-235 Urine Faeces Lungs
1 - 2 2 2
30 30 30
5 3 3
30 30 30
Pu-239 Urine Faeces
n.a. - 3 3
30 30
5 5
30 30
Am -241 Urine Faeces Lungs
Skeleton
1 - 2 2 2
30 30 30
3 3 3 1
30 30 30 30
Discussion point!!!
This is only a start (“place-holder”)
Help is needed to:
• confirm (or improve)
• extend to other situations
Hopefully workplace monitoring will ensure that sufficient data are available.

IM2005, Vienna, April 2005 42
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 5B:
Special assessment Inhalation:
vary AMAD, F/M/S, Time of intake
5A
5.8Time of intake
is known
5.9Early lung and faeces
data available
5.10Derive effective AMAD from early
lung and faeces data
5.11Assessment of dose by fitting of the
absorption type
5.12Assessment of dose by simultaneous fitting of both the time of intake and
the absorption type
5.7.1Get additional dose relevant data
5.7There are suffcient
relevant data
5.11.1Goodness of fit
is acceptable
5.13Assessment of dose by fitting of the mixture of default absorption types
(F,M,S)
5.14Assessment of dose by simultaneous fitting of both the time of intake and
the mixture of default absorption types (F,M,S)
5.12.3Record dose with all parameters
5.12.1Goodness of fit
is acceptable
5.11.2Dose from intake
< 6 mSv
5.11.4Check the number of data required for evaluation at this level and get more
data, if necessary(Table)
5.12.2Dose from intake
< 6 mSv
5.12.4Check the number of data required for evaluation at this level and get more
data, if necessary(Table)
No
No
Yes
No
Yes
No
Yes
Yes
NoYes
No
Yes
NoYes
No
5.11.3Record dose with all parameters
Stage5B
Stage5CEnd End
Step 5.8 Procedure splits based on time of intake:
•known (5.9-5.13) or
•unknown (5.12, 5.14)

IM2005, Vienna, April 2005 43
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 5B:
Special assessment Inhalation:
vary AMAD, F/M/S (Time of intake)
Step 5.8: time of intake known
Main effect of AMAD is partition between:
•upper respiratory tract (ET, BB, bb) mostly early fecal excretion
•lower respiratory tract (AI) mostly lung retention
Hence estimate “effective” AMAD

IM2005, Vienna, April 2005 44
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 5B:
Special assessment Inhalation:
vary AMAD, F/M/S (Time of intake)
Main effect of AMAD is partition between:
•upper respiratory tract (ET, BB, bb) mostly early fecal excretion
•lower respiratory tract (AI) mostly lung retention
Hence estimate “effective” AMAD
0
2
4
6
8
10
12
14
0 1 2 3 4 5 6 7 8 9 10
AMAD, µm
Cum
ulat
ive
activ
ity in
faec
es fr
om 1
to 3
day
s /
activ
ity in
lung
on
day
3
Type M
Type S
Relatively insoluble materials
Ratio of early fecal excretion to lung retention (day 3) for Am-241
Could extend to other situations

IM2005, Vienna, April 2005 45
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 5B:
Special assessment Inhalation:
vary AMAD, F/M/S (Time of intake)
Step 5.8: time of intake known
Step 5.11 Fit absorption type
A priori assignment based on chemical form (Step 5.3)
Check “goodness” of fit (Step 5.11.1). If fit rejected try other Types (F/M/S)

IM2005, Vienna, April 2005 46
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 5B: Special assessment Inhalation:
vary AMAD, F/M/S (Time of intake)
Step 5.8: time of intake known
Steps 5.11.1&2 Model fits data, if dose <6 mSv record dose and stop.
Step 5.13 If fit rejected or additional data, try mixture of Types (F/M/S)
Steps 5.11.4 Enough data for 6 mSv?

IM2005, Vienna, April 2005 47
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Stage 5B: Special assessment Inhalation:
vary (AMAD), F/M/S Time of intake
Step 5.8: time of intake unknown
(Cannot determine “effective” AMAD)
Step 5.12 Simultaneous fit of time of intake and absorption.
If model fits data, and if dose <6 mSv record dose and stop.
Step 5.14 If fit rejected or additional data, try mixture of Types (F/M/S)
Step 5.12.4 Enough data for 6 mSv?
Discussion point!!!
If model fits, then probably several sets of parameter values (intake times and mixtures of absorption Types) will fit. Not straightforward to harmonise best fit with two variables. Needs more work.

IM2005, Vienna, April 2005 48
Stage 5C: Advanced evaluation
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
Vary parameter values in order: check fit after each step
•HRTM absorption parameters (fr, sr, ss)
•GI tract absorption f1•HRTM particle transport parameters
•GI tract transit
•Systemic biokinetic model
Vary parameter values in order: check fit after each step
•HRTM absorption parameters (fr, sr, ss)
•GI tract absorption f1•HRTM particle transport parameters
•GI tract transit
•Systemic biokinetic model

IM2005, Vienna, April 2005 49
Development of Guidelines
1. IDEAS: refine from outcome of the exercise, and discussions at the Workshop. Publish summer 2005.
2: ICRP Guidance Document to accompany revision of publications 30/54/68/78. Publish 2007?
General guidelines for the estimation of committed dosefrom incorporation monitoring data
(Project IDEAS)IDEAS
3: IDEAS web site. CONRAD 2005-2007. FP7? Another exercise around 2007-8?





























