Embed Size (px)
Citation preview

E
Iia
AMA
a
Hb
c
R
0d
pilepsy Research (2008) 79, 90—96
journa l homepage: www.e lsev ier .com/ locate /ep i lepsyres
ctal impending danger — ‘‘sixth sense seizures’’ —n patients with benign focal epileptic seizures ofdolescence�
ntonino Romeoa,∗, Rosanna Chifari a, Giuseppe Capovillab, Maurizio Viri a,onica Lodia, Valentina Dell’Oglioa, Francesca Beccariab,ntonio Gambardellac
Epilepsy Center, Department of Child Neuropsychiatry and Neurophysiology, ‘‘Fatebenefratelli e Oftalmico’’ospital, Corso di Porta Nuova 23, 20121 Milano, ItalyEpilepsy Center, Department of Child Neuropsychiatry, ‘‘Carlo Poma’’ Hospital, Via Albertoni 1, 46100 Mantova, ItalyInstitute of Neurology, University Magna Graecia, Campus Universitario Germaneto, 88100 Catanzaro, Italy
eceived 3 October 2007; received in revised form 28 November 2007; accepted 30 December 2007
KEYWORDSBenign focal seizures;Benign focal epilepsy;Frontal seizures;Cingulate seizures;Idiopathic epilepsy;Adolescence
SummaryPurpose: We describe nine consecutive patients with diagnosis of benign focal epileptic seizuresof adolescence (BFSA), who experienced an ictal sensation of impending danger.Materials and methods: We collected nine BFSA patients after a comprehensive clinical andlaboratory investigation, video-EEG analysis and neuroimaging study.Results: All patients displayed a distinct electro-clinical pattern of seizures characterized by apeculiar subjective feeling of impending danger coming from behind, followed by a coordinatedbehavior of ‘‘head-turning’’ toward the danger. This feeling was described in all patients as ‘‘ashadow behind me on one side’’ or ‘‘something or someone behind me’’. All of our patientsexplained that, at the beginning of their seizures, they felt an early warning of a high-risksituation. Electrophysiologic data favored a frontal origin of these seizures.Conclusion: We have described for the first time a distinct electro-clinical pattern of seizures in
the context of BFSA, characterized by the ictal feeling of early warning of a high-risk situation,which we thought to term ‘‘sixth sense seizure’’. In the light of current neuro-anatomicalknowledge, seizure discharge within anterior cingulate cortex (ACC) structures is the likelyexplanation for this situation. Further studies are needed to establish if this is an electroclinicalvariant of BFSA or a new distinct epileptic syndrome.© 2008 Elsevier B.V. All rights reserved.� This work has been presented as final thesis by Dr. Laura Perego at the Neurology School University, Milano.∗ Corresponding author. Tel.: +39 02 6363 2345; fax: +39 02 6363 2867.
E-mail address: [email protected] (A. Romeo).
920-1211/$ — see front matter © 2008 Elsevier B.V. All rights reserved.oi:10.1016/j.eplepsyres.2007.12.017

R
TTshrf
S
AoiboopwIopeImdrroavs#
spdd
I
AgpiifGr
ia
I
Sixth sense seizures and BFSA
Introduction
Benign focal seizures of adolescence (BFSA) were firstlydescribed in 1972 by Loiseau et al. (1972), who reporteda small series of patients, whose seizures started from thesecond decade of life, with a peak of age-at-onset around13 years and had a very benign course and a family history ofepilepsy was rare. Afterwards, Loiseau and Orgogozo (1978)reported a larger series of 83 adolescents with BFSA, andemphasized the existence of a peculiar electroclinical pat-tern of BFSA, characterized by cluster of focal sensory orsomatomotor seizures with or without a Jacksonian march.A normal interictal EEG recording as well as normal neuro-logic and neuroradiologic examinations were also claimed(Loiseau and Orgogozo, 1978). The authors concluded thatthis entity is not an epilepsy syndrome, but a seizure-susceptibility syndrome. This series was further increasedto 108 cases in 2002 (Loiseau et al., 2002).
Afterwards, very few studies focused on this particularcondition and confirmed the existence of the aforemen-tioned electroclinical pattern of somatosensory seizures(King et al., 1999; Caraballo et al., 2004, 2007). This electro-clinical pattern also emerged from a large series of 37 newpatients that we reported previously (Capovilla et al., 2001).In this study, we found a high rate of positive family historyfor epilepsy and also identified a second type of electro-clinical pattern that consisted of versive seizures and focalspikes or sharp waves over the posterior regions (Capovillaet al., 2001). Probably, the latter was identified becauseof the large number of patients we collected data from.Indeed, the existence of some patients with BFSA who hada different electroclinical picture has also been claimed byother researchers (King et al., 1999), but they did not reportany detail of such patients, presumably because the num-ber was too small to draw any conclusions from King et al.(1999).
Subsequently, we have continued to collect patients withBFSA, and now we wish to report a series of nine patientswith BFSA who experienced a peculiar ictal sensation ofimpending danger described as a ‘‘shadow behind me on oneside’’ or ‘‘something or someone behind me’’. which wasfollowed by a coordinated behavior of purposeful ‘‘head-turning’’ toward the danger.
Methods
From June 2000 to July 2007, we consecutively collected ninepatients (seven male, mean age at seizure onset: 13.9 years, ±2years, range: 11—17; mean age: 20.1 years, ±4.1 years; range:12.10—24.10 years) who received a diagnosis of BFSA after a com-prehensive clinical and laboratory investigation. Inclusion criteriaare benignity, age-related, autolimited epileptic syndrome appear-ing during the second decade of life, with a peak between 13 and 14years of age, with focal motor, somatosensory and versive seizureswith or without secondary generalization occurring isolated or incluster in the first 24—48 h after onset. Neurological examinationand brain MRI are normal (Loiseau and Loiset, 1992; Capovilla etal., 2001; Caraballo et al., 2007).
We excluded patients with neuroradiologically documentedlesions, or neurological or mental deficits. Some of the remainingcases, who matched the electroclinical pictures of benign child-hood epilepsy with centro-temporal or occipital spikes, were alsoexcluded from this study.
IFas
91
esults
he main electro-clinical features are summarized inable 1. Two/nine patients had family histories of afebrileeizures or febrile convulsions (FCs). None of our patientsad personal histories of FCs. All patients had normal neu-opsychological development at onset of epilepsy and duringollow-up.
eizure characteristics
ll nine patients had seizures during wake and, at the onsetf their seizures, all of them referred a sensation of impend-ng danger behind them, associated with fear and followedy a coordinated behavior of head turning in the directionf the danger. Such seizures lasted from 10 to 30 s and couldccur in cluster within a 2 min. After close questioning allatients gave us a strikingly homogeneous description ofhat they had experienced at the onset of their seizures.
ndeed, it was typically described as ‘‘a shadow behind men one side’’ or ‘‘something or someone behind me’’. Allatients also specified that they were aware of the ipsilat-ral ‘‘head-turning’’, as they were trying to see the shadow.n some instances, such seizures could evolve into frankotor attacks with loss of consciousness and tonic headeviation, while secondarily generalized seizures were veryare. At the end of the seizures, the patients were able toefer their symptoms, unless secondary generalization hadccurred. Overall, the frequency of seizures was very low,nd in three/nine patients seizures recurred at short inter-als of minutes or hours, within 1 or 2 days. This type ofeizures occurred within 24 h in all patients, except patient2 who had clustered seizures within 48 h.
Other types of focal seizures particularly focal motoreizures with or without secondary generalization wereresent in all patients and in seven of them could occururing sleep. In patient #3, manual automatisms were alsoescribed.
nterictal EEG
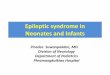
ll patients had awake and asleep EEG recordings. Back-round activities were always normal. Theta activity wasresent in three patients; sharp-wave complexes were seenn eight/nine cases (Fig. 1), appeared more often dur-ng sleep and were localized mostly over the frontal andronto-central regions bilaterally or on either side (Table 1).eneralized epileptiform discharges and photoparoxysmal
esponses were never found.During follow-up, repeated awake and sleep EEG record-
ngs showed progressive improvement until normalization inll patients.
ctal EEG
n four patients (patient #2, #3, #6 and #7, see Table 1 andigs. 2 and 3), we were able to record a typical seizure. Inll four patients, the clinical manifestations were strikinglyimilar and consisted of the initial sensation of impending

92A.
Romeo
etal.
Table 1 Main clinical and EEG features of nine patients with BFSA and ‘‘sixth sense seizures’’
Patient, age(years), sex
Age at onset(years)
Other types of seizures Clusterof sz
Interictal EEG Ictal EEG Therapy Prognosis(follow-up)
(1) 21.4, M 16 FMS + SG awake No Theta on F4-C4 No No therapy Seizure free (5years 4 months)
(2) 24.10, M 16 FMS + SG during sleep Yes Theta and SW onFp2-F4, Fp1-F3
Onset on Fp2-F4-Fz CBZ stopped Seizure free (8years 10months)
(3) 12.10, F 11 FS (manual automatism)during sleep
Yes Theta and SW onFp2-F4, Fp1-F3
Onset on Fp2-F4-Fz OXC 1.0 g/d Seizure free (1year 10months)
(4) 18.3 M 12.8 FMS during sleep Yes SW on Fp2-F4 No OXC stopped Seizure free (5years 7 months)
(5) 15.5 F 13.10 FMS during sleep No SW on Fp2-F4, Fp1-F3 No VPA 600 mg/d Seizure free (1year 7 months)
(6) 24.4 M 17.1 FMS during sleep Yes SW on Fp1-F3-F7 Onset on Fp1-F3-Fz No therapy Seizure free (7years 3 months)
(7) 20.4 M 13 FMS during sleep Yes SW on Fp2-F4-F8,Fp1-F3
Onset on Fp2-F4-Fz No therapy Seizure free (7years 4 months)
(8) 19.6 M 11.6 FMS + SG during sleep Yes SW on F4-C4, F3-C3 No CBZ 600 mg/d Seizure free (8years)
(9) 24.6 M 13.4 FMS during sleep No SW on F4-C4, F3-C3 No VPA stopped Seizure free(11years 2months)
FS: focal seizure; FMS: focal motor seizure; SG: secondary generalization; SW: sharp-wave complexes; CBZ: carbamazepine; OXC: oxcarbazepine; VPA: valproate.

Sixth sense seizures and BFSA 93
sharp
aroLacBs1emcr1roisthecotooa
Figure 1 Patient 3: interictal EEG shows theta activity and
danger behind them, like ‘‘a shadow behind me on oneside’’ or ‘‘something or someone behind me’’, associatedwith a coordinated behavior of ‘‘head-turning’’ toward theshadow. Eventually, a forced deviation of trunk, eyes andhead with extension of ipsilateral arm could also occur.There was no definite loss of consciousness. On EEG record-ing a fast activity appeared at frontal electrodes, followedby theta rhythmic activity mostly on Fp2 and F4 or Fp1 andF3 and Fz (Figs. 2 and 3). Seizures length ranged between20 and 30 s in all patients.
Therapy and follow-up
Therapy and follow-up are summarized in Table 1.The three patients with a brief cluster of seizures never
had any therapy. In the remaining six patients, seizureswere always easily controlled. Recurrence of seizures dur-ing the treatment never occurred. The utilized drugs werecarbamazepine (two cases), oxcarbazepine (two cases) andsodium valproate (two cases). Three patients had stoppedtheir medications with non-recurrence of their seizures aftera mean follow-up period of 6 years and 3 months (range: 1year 7 months to 6 years 10 months).
Discussion
All nine patients fulfilled the criteria so far utilized tomake a diagnosis of BFSA (Loiseau et al., 1972; Loiseauand Orgogozo, 1978; King et al., 1999; Capovilla et al.,2001; Caraballo et al., 2004), as partial seizures startedduring adolescent within a clinical context of neurological
cr
to
waves on frontal regions predominant on right hemisphere.
nd neuroradiological normality, regardless of the occur-ence of paroxysmal epileptiform abnormalities, which mayr may not occur in such condition (Loiseau et al., 1972;oiseau and Orgogozo, 1978; King et al., 1999; Capovilla etl., 2001; Caraballo et al., 2004). Two main electroclini-al patterns have so far been recognized in patients withFSA: the first one is characterized by motor or somatosen-ory focal seizures (Loiseau and Orgogozo, 1978; King et al.,999; Capovilla et al., 2001; Loiseau et al., 2002; Caraballot al., 2004, 2007). Motor signs occurred with jacksonianarch followed or not by secondarily generalized tonic-
lonic seizures, occurring as a single event or, more often,epeated in cluster within 24—48 h (Loiseau and Orgogozo,978; Loiseau et al., 2002; Caraballo et al., 2004). Morearely, focal seizure are characterized by motion arrest andral automatism followed or not by secondarily general-zed tonic-clonic seizures. Autonomic symptoms, vertigo andpeech deficiencies have been described as added symp-oms, whereas auditory, olfactory and gustatory symptomsave been never reported (Loiseau et al., 2002). Capovillat al. (2001) underlined the presence of focal theta dis-harges over the centroparietal regions in the interictal EEGsf these patients. Another electroclinical pattern is charac-erized by versive seizures with eye and/or head deviation,ften followed by loss of consciousness with or without sec-ndary generalization (Capovilla et al., 2001; Caraballo etl., 2007). In these patients, the interictal EEG pattern
onsists of focal spikes or sharp waves over the occipitalegions.The patients presented here give us strong evidence, forhe first time, for a third distinct electro-clinical patternf seizures characterized by a peculiar subjective feel-

94 A. Romeo et al.
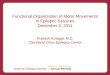
Figure 2 Patient 2: the electroclinical features occurred during ictal video-EEG. (A and B) The seizures begins with initial sensationof impending danger behind them (like a presence); the EEG shows fast activity over Fp2-F4-Fz; (C) initial coordinated behavior ofl D ans
isbi‘c
stialsa
rbwiautAt
wop
woaasilttIsoppa
eft ‘‘head-turning’’ associated with attenuation activity EEG; (low waves activity.
ng of impending danger that comes from behind on oneide, associated with fear and followed by a coordinatedehavior of head turning in the direction of the danger, typ-cally described as ‘‘a shadow behind me on one side’’ or‘something or someone behind me’’. Rarely the seizuresould evolve in a secondary generalization.
We have thought to term this type of seizure as a ‘‘sixthense seizure’’, as all of our patients made it clear that, athe beginning of their seizures they had felt an early warn-ng of a high-risk situation. It is important to underline thatlarm in our series of patients was different from the iso-ated feeling of fear associated with an ascending epigastricensation described in temporal mesial epilepsies (French etl., 1993).
Of interest, a recent study suggests that the ante-ior cingulate cortex (ACC), described as part of therain’s ’’oops‘‘center, may actually function as an earlyarning system — a sixth sense for danger — that mon-
tors environmental cues, weighs possible consequences
nd helps us adjust our behavior to avoid dangerous sit-ations (Brown and Braver, 2005). On this basis, it isempting to speculate that a seizure discharge withinCC structures is the likely explanation for this situa-ion in our patients. Ictal EEG findings are in agreementgmcwm
d E) ongoing ‘‘head-turning’’ associated by recruiting rhythmic
ith this hypothesis as there was evidence of a frontalrigin of such ‘‘sixth sense’’ epileptic seizures in ouratients.
In the literature, there are very few reports of patientshose ictal manifestations may resemble those reported inur series and, importantly, all had focal epilepsy associ-ted with ACC dysplasia (Mihara et al., 1997; Biraben etl., 2001). It is possible, however, that this type of ‘‘sixthense seizure’’ might have been underestimated, especiallyn patients with BFSA. Reasons for under-diagnosis are theack of close questioning so one could easily misinterprethe head turning as a simple motor versive seizure, orhe presence of amnesia after secondary generalization.n two of our patients, indeed, we recorded ‘‘sixth senseeizures’’ with and without secondary generalization, andnly after seizures without secondary generalization bothatients were able to give us a very good description of sucheculiar ictal feeling of a ‘‘shadow behind me’’. They werelso aware of a purposeful head turning in direction of dan-
er. This kind of ‘‘sixth sense’’ epileptic seizures could beistaken with a psychiatric disorder or could also be mis-onstrued as psychogenic non-epileptic seizures, especiallyhen they are not followed by loss of consciousness or majorotor manifestations.

Sixth sense seizures and BFSA 95
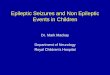
Figure 3 Patient 3: the electroclinical features occurred during ictal video-EEG. (A) Initial sensation of impending danger behindnd C’ asso
B
C
C
C
F
K
L
L
them corresponding fast activity with spikes over Fp2-F4-Fz; (B awith attenuation activity EEG; (D and E) ongoing ‘‘head-turning’spreading.
Conclusion
We have described for the first time a pattern of ‘‘sixthsense seizures’’ in the context of BFSA. In the light ofcurrent neuro-anatomical knowledge, a seizure dischargewithin ACC structures is the likely explanation for this sit-uation. Epileptologists should be aware of these peculiarseizures as, in most instances, ‘‘sixth sense seizures’’ maybe diagnosed on clinical grounds. Further studies are neededto establish if this is an electroclinical variant of BFSA ora new distinct epileptic syndrome. Moreover a prospectivestudy should be done to better define the nosological placeof this electroclinical picture.
Conflict of interest
None.
Acknowledgement
We are grateful to our colleague Dr. Amedeo Bianchi for hisprecious scientific suggestion. We thank Elena Verdasio andClarissa Ghiroldi for technical support.
References
Biraben, A., Taussig, D., Thomas, P., Even, C., Vignal, J.P.,Scarabin, J.M., Chauvel, P., 2001. Fear as the main feature
L
) initial coordinated behavior of left ‘‘head-turning’’ associatedciated by recruiting rhythmic slow waves activity with bilateral
of epileptic seizures. J. Neurol. Neurosurg. Psychiatry 70,186—191.
rown, J.W., Braver, T.S., 2005. Learned predictions of error likeli-hood in the anterior cingulated cortex. Science 307, 118—121.
apovilla, G., Gambardella, A., Romeo, A., Beccaria, F., Mon-tagnini, A., Labate, A., Viri, M., Sgro, V., Veggiotti, P., 2001.Benign partial epilepsies of adolescence: a report of 37 newcases. Epilepsia 42, 1549—1552.
araballo, R.H., Cersosimo, R.O., Fejerman, N., 2004. Benignfocal seizures of adolescence: a prospective study. Epilepsia 45,1600—1603.
araballo, R.H., Cersosimo, R.O., Capovilla, G., Fejerman, N.,2007. Benign focal seizures of adolescence. In: Fejerman, N.,Caraballo, R.H. (Eds.), Benign Focal Epilepsies in Infancy, Child-hood and Adolescence. John Libbey Eurotext, Paris, France, pp.243—252.
rench, J.A., Williamson, P.D., Thadani, V.M., Darcey, T.M., Matt-son, R.H., Spencer, S.S., Spencer, D.D., 1993. Characteristics ofmedial temporal lobe epilepsy. I. Results of history and physicalexamination. Ann. Neurol. 34, 774—778.
ing, M.A., Newton, M.R., Berkovic, S.F., 1999. Benign partialseizures of adolescence. Epilepsia 40, 1244—1247.
oiseau, P., Loiset, P., 1992. Benign partial seizures of adolescence.In: Roger, J., Bureau, M., Dravet, C., et al. (Eds.), Epileptic Syn-dromes in Infancy, Childhood and Adolescence, 2nd ed. JohnLibbey Eurotext, London, pp. 343—345.
oiseau, P., Orgogozo, J.M., 1978. An unrecognized syndrome
of benign focal epileptic seizures in teenagers? Lancet 2,1070—1071.oiseau, P., Jogeix, M., Lafitte, M., 1972. Crises epilepticsans suite chez les adolescents. Bord. Med. 5, 2623—2629.

9 A. Romeo et al.
L
6
oiseau, P., Jallon, P., Wolf, P., 2002. Isolated partial seizures ofadolescence. In: Roger, J., Bureau, M., Dravet, C., et al. (Eds.),Epileptic Syndromes in Infancy, Childhood and Adolescence, 3rded. John Libbey Eurotext, London, pp. 327—330.
M
ihara, T., Tottori, T., Matsuda, K., Otsubo, T., Inoue, Y., Yagi, K.,Seino, M., 1997. Analysis of seizure manifestation of ‘‘pure’’frontal lobe origin. Epilepsia 38 (Suppl. 6), 42—47.