Embed Size (px)
Citation preview

By Joseph S. Zasa, Principal –Woodrum/Ambulatory SystemsDevelopment
We received numerous responsesregarding a quote in a recent edi-tion of this newsletter. The state-
ment generated interesting questions andresponses. A paraphrase of the quote is:
Staffing costs should be 20% of net revenue or lower. If not, it is an indicator of mismanagement.
As the author of this statement, the respons-es were surprising since there is at best avague recollection of the quote and the inter-view. In fact, I had to research back issues ofthis periodical to find the quote. The wholescenario reminded me of the Jimmy Buffetsong, “I Heard I was in Town.” Interestingly,at the risk of sounding like Charles Barkleywho said he was misquoted in his autobiog-raphy, I do not necessarily agree with “myown” statement since it is accurate in someinstances, but potentially misleading in oth-ers. In this instance, the problem may be thatthe statement was not expanded on in itsproper context. Nevertheless, the responsesare appreciated since it provides a good basisfor this article and allows us to examine thevery important issue of measuring staffingcosts in ambulatory surgery centers.
The Inherent Dilemma
Staffing costs are the first or second highestexpenditure in a surgery center and effectivemanagement of this cost is a key function ofeffective administration. The challenge isthat staffing is not a variable cost in the tra-ditional sense whereby the more patients atthe center, the more staff are hired. Rather,the ASC industry consists of generally smallbusinesses that we estimate, on average, per-form 200 cases per month. In fact, 64% of all
There are many misconceptions aboutambulatory surgery centers and thebest ways to run them. To help you
better understand ambulatory surgery centers, here is a list of thirty-three thingsthat you should know about surgery centers. Should you have comments or disagree with an item, please email [email protected].
1. CMS’ Proposed New Rates DecreaseASC Reimbursement. The new proposedMedicare rates for surgery centers are gener-ally very negative. They essentially set reim-bursement at an amount equal to 62% of theprice paid for the same surgical proceduresat hospital outpatient departments. Theserates, if made final, will take full effect in2008. Under the proposed rates, of the top20 procedures performed in surgery centers,17 will suffer a decrease in reimbursement.For many procedures, the decreases will besignificant. For example, reimbursement formany gastroenterology and pain manage-ment procedures will decrease nearly 20 to30%. Many ophthalmology procedures willexperience a 10 to 15% reduction in reim-bursement. Ultimately, many high volumeprocedures will cease to be profitable to per-form. The lower reimbursement rates canresult in unintended impacts. For example,the proposed lower rates will increase thenumber of parties that attempt to “game thesystem” through joint ventures that operate“under arrangements.” In addition, lowerreimbursements at surgery centers and high-er reimbursements at hospitals may incen-tivize physicians to develop (and convert to)small hospitals instead of surgery centers.
2. Many ASCs Still Fail. Despite theirgrowth throughout the country (nearly 6,000ASCs), a number of ambulatory surgicalcenters still fail. The failures occur mostlydue to bad management, low volume, poorreimbursement, or overbuilding. Knowingthe risks involved in developing an ASC can
help to ensure that your ASC will prosperand not fail. Working with experienced man-agers in developing a center can also helpprevent failures
3. RNs Often Make Superior Admin-istrators. Experienced registered nurses often make great ASC admin-istrators. The RN must study and beinterested in the business side of ASCs.Generally, RNs are trained to be disciplined and dedicated workers; a workethic that carries over to the administratorposition. As such, RNs are often vibrantand willing to contribute in a myriad ofways to improve the surgery center.
4. Leasing Equipment From Physician-Investors is Often a Bad Idea. While itcan look attractive, leasing equipment fromentities owned by ASC physicians is often alegally risky business. Often these arrange-ments can be viewed as thinly veiled disguises to incentivize physicians to use thecenters; arrangements generally viewed by thegovernment as illegal. As such, as a rule thesearrangements should be supported by a fairmarket value analysis, make business senseregardless of referrals, and preferably be set asa fixed annual fee and not as “per click. “
November/December 2006Vol. 2006 No. 6
continued on page 8
continued on page 4
INSIDE2 Letter from the Editor10 Five Signs You’re In Need Of
Outside Intervention: ASCOA’s Perspective
12 An ASC In Need of Drastic Improvement – 26 Questions You Should Ask
13 How to Keep Results Up and Sustainable
15 Five Signs You’re In Need Of Outside Intervention: Regent Surgical Health’s Perspective
17 Staffing a Turnaround Center
33 Things You Should Know About Ambulatory Surgery CentersBy Scott Becker
I Heard I Was In Town –Measuring ASCStaffing Costs

2 visit www.beckersasc.com
Letter from the Editor
This is a tremendously uncertain timefor ambulatory surgical centers andfor providers who believe in a com-
petitive healthcare environment in general.There are a number of different issues per-colating that have the ability to deeplystrengthen or deeply harm competitivehealthcare. This issue provides a discus-sion of a broad array of healthcare topics.It also focuses to a certain extent on “turn-ing around” surgery centers.
Certain of the issues that are impactinghealthcare include:
1. Political Balance. Before the election,there existed a political balance on healthcare issues between the House ofRepresentatives and the Senate. At thattime, a Republican controlled house provided a balance to a Senate (alsoRepublican majority) that was more hostileon some issues towards competition inhealthcare. The change in makeup of theHouse of Representatives and Senate, anda move towards a more Democratic consti-tuted House and Senate will likely have along term negative impact on competition
in healthcare. This is largely due to the factthat the Democrats as opposed to theRepublicans have been more supportive ofsingle payor initiatives, and expansions oflaws such as the Stark Act that wouldrestrict physician ownership of healthcarefacilities with which they work. Whilechanges may not occur fast, there is cer-tainly a possibility that a change in themakeup of the House of Representativeswould particularly have a negative impacton competition in healthcare.
2. Reimbursement Rates for SurgeryCenters. As most people are aware, CMShas proposed substantial reductions inpayment rates for ambulatory surgery cen-ters. These can have significant impacts onthe profitability of surgery centers and themotivation to continue to grow and devel-op ambulatory surgical centers. In the faceof such changes, different research analystsand investment banks have taken differentpositions on the potential impact on surgery centers. For example, one invest-ment bank, Bank of America, lowered itsratings on the entire industry based in parton changes on out of network business andin part based on changes in Medicare reim-bursement. Here, it downgraded the stock
of each of Amsurg, United SurgicalPartners, and Symbion. In contrast, anoth-er investment bank actually raised its out-look on Symbion based on its view that thechanges in Medicare reimbursementwould have an overall mildly positiveimpact on Symbion due to its mix of ortho-pedic cases versus other types of cases.
3. Texas Sized Credentialing Case. Inwhat has been called a Texas-sized verdict,a hospital and certain physicians were hitwith a $366 million verdict in a lawsuitbased on the improper or malicious revoca-tion of privileges of a physician. The casediscussed the concept of summarily suspending the physician without properdue process and a whole number of otheritems that lead to this verdict. In a fascinat-ing situation, the hospital and its physicians were caught in a real “Catch22.” If they did not suspend the physician,they potentially ran the risk of malpracticecases due to allowing the physicians topractice. They might also face Texas-sizedverdicts. They acted quickly to suspendthe privileges and in their view to protectpatients and ended up with a horrible verdict.

3visit www.beckersasc.com
This lawsuit, which we expect will beappealed, points to the continued need tobe extremely careful with respect to credentialing decisions whether in theambulatory surgical center setting or thehospital setting.
4. Deals and Transactions. We havehad the great privilege, at the end of thethird quarter, of helping to complete threedifferent and interesting transactions.First, we had the chance to help a mid-sized hospital in California sell theirhospital to a newly formed company calledTru Medical. This transaction involved thesale of 50 percent of the ownership of thehospital as well as the related real estate ofthe company. It was truly an exciting trans-action to be a part of. Second, we had theopportunity to help Ambulatory SurgicalCenters of America and its physician part-ners to help sell a surgical center in Texas toUnited Surgical Partners. Finally, werecently completed the sale of a surgerycenter in Colorado to National SurgicalCare. For information regarding TruMedical, please contact Tim Lavendar at972-870-5142. For information regardingNational Surgical Care, please contact RickPence at 972-447-8285. For informationregarding Ambulatory Surgical Centers ofAmerica, please contact Brent Lambert at781-258-1533. For information regardingUnited Surgical Partners, please contactBrett Brodnax at 972-713-3500.
We also had the opportunity to work tocomplete investments by each HealthMarkPartners in a surgery center in Tennesseeand to help Regent Surgical Health joinwith physicians and a hospital in Indianato joint venture a center. Finally, weworked closely on a project led by physi-cians to develop a large hospital inCalifornia. There, Cirrus Healthcare ishelping to drive the project forward. For information regarding HealthMarkPartners, please contact Bill Southwick at615-329-9000. For information regardingRegent Surgical Health, please contact TomMallon at 708-492-0531. For informationregarding Cirrus Health, please contactJohn Thomas at 817-837-1187.
5. Turning Around Ambulatory SurgicalCenters. The formula for turning aroundambulatory surgical centers is misleading-ly simple. In short, it amounts to increasecases, increase reimbursement, and/or reduce costs. Notwithstanding the simplicity of the formula, these steps areoften extremely difficult to implement.
First, the recruitment of physicians inmany markets is extremely difficult.Further, many physicians do not wish tojoin a facility that is not already succeed-ing. Where a facility is already succeedinggreatly, physicians do not want to pay fairmarket value for the shares they need tobuy to become owners in the center.
Second, increasing reimbursement takes amix of finesse and strong resolve. First,parties can attempt to renegotiate withtheir payor. There are, of course, experts inhandling such types of renegotiations.Naya Kehayes of Eveia Consulting andManagement comes to mind. They can dothis by themselves or with the help of Nayaor a third party management company.Second, as part of the negotiations, theycan work toward carve outs, they can worktoward attempting to fix reimbursementfor their top 10 to 20 procedures or they canhandle it as an across the board negotia-tion. The negotiation is a mix of relation-ship building over the long run plus playing hardball from time to time.Increasingly, hospitals and payor periodi-cally play hardball and have well publi-cized disputes over their differences overcontracts. For surgery centers, many do nothave the market power of hospitals. Thus,they often need to play hardball in a different manner. Specifically, they willlook at methods by which to treat patientsout of network rather than taking substan-dard reimbursement.
The third core method for improving profitability is to cut costs. This oftencomes from reducing staffing, which is thelargest single expense of most surgery cen-ters. This often does not mean laying peo-ple off but it does often mean not hiringanother person when somebody quits,closing the center a few days a week andtrying to cluster as many cases over two orthree days as possible, and attempting toreduce hours that the surgery center isopen. We believe in paying the highestrates per hour but attempting to run atighter ship. With regard to the cutting ofcosts, it takes tremendous discipline andwillpower. Nine out of ten centers will tellyou it cannot possibly reduce cost.However, in my experience, a willing leadership board can find ways to cut costsif they are willing to take some of the negative feedback that comes with it.Centers can cut costs through the betterpurchasing of equipment and supplies. It isoften the situation where leadership of acenter is “persuaded” to buy the newest or
most exciting supplies, implants, or tech-nology. Often, the older technology andsupplies and equipment can be cheaperbut effective. One of the best examples ofthis I have witnessed related to a urologycenter. There, the urology center had todecide between buying a used stationarylithotripter, this was about ten years ago, orbuying a brand new lithotripter. Theyended up buying the used lithotripter forabout $200,000. The lithotripter paid foritself within about six months. Finally,recently, they actually had to step up to theplate and buy a newer model. The experience though, was convincing interms of how effective it can be to purchaseinexpensively.
6. Electronic Medical Records. Withstops and starts, larger physician practicesand some smaller practices as well asambulatory surgical centers are starting tolook regularly at the implementation ofelectronic medical records. Two of the lead-ing sources which serve the ASC marketplace include ZChart and AMKAI,Inc. For information on either company,please contact Tom Felstead at ZChart at866-924-2787 or contact Craig Veach atAMKAI, Inc. at 866-265-2434.
Should you have any questions on any ofthe items listed in this letter or any of thearticles in this newsletter, please contactmyself at 312-750-6016 or by email [email protected].
Very truly yours,
Scott Becker
The ASC Review is published 6 times per year. It is distributed to approximately 15,000 personsper issue with distribution of 20,000 issues for each the May–June issue and theSeptember–October issue. For informationregarding advertising or subscribing, pleasecontact Ken or Michelle Freeland at 858-565-9921or by email at [email protected] [email protected].
To advertise inor subscribe to the
ASC Review, please contactMichelle or Ken Freeland
at 858-565-9921.

4 visit www.beckersasc.com
33 Things You Should Know About Ambulatory Surgery Centers continued from page 1
5. High-Quality Management is Key toSuccess. High-quality management is crit-ical to an ambulatory surgical center’s suc-cess. Many management companies offersuperior services. However, many are of littlevalue. All management companies are notequal. For this reason, it is important to workwith an experienced management companythat has a proven track record of successes.Working with a low-quality, inexperiencedcompany will do more harm than good.
6. Paying Fees Plus Equity to aManagement Company is Often theNorm. In addition to a management fee,increasingly, the leading management com-panies are requiring fees, as well as a smallportion of equity in the surgery center.Before writing off such an arrangement,evaluate how that management companycompares to other management companies.
7. Buying Out Non-Productive PartnersIs an Option. There is no silver bullet forbuying out the equity in a center held by aphysician who does not produce as expect-ed. There are heavily weighted legal issuesthat relate to such issues. Whether or not youcan buy out a partner is a critical legal ques-tion that must be examined in light of theASC safe harbor regulations and their “1/3rd
– 1/3 rules, amongst other factors. Newlytouted strategies like “squeeze out” mergersoften carry substantial risk.
8. Distributing Income Based onReferrals is Illegal. A surgery center can-not distribute ASC income, whether the ASCis owned indirectly or directly by physicians,based on the referrals or the value or volumeof referrals by physicians. The federal (andmany state) government deems these typesof distributions illegal. There is no “clean”way to avoid this rule.
9. Growth Strategy is Key. An ASC willnot succeed long-term without an ongoingcomprehensive growth strategy. A growthstrategy should include goals for increasingcase volume and types of procedures, andpotentially increasing the ASC’s size andnumber of physician investors. A stagnantASC will not be able to effectively competewith other centers and hospitals that areactively vying for business.
10. An ASC Can Have Too ManyPhysician Investors. Perhaps you cannotbe too thin or too rich, but you can have toomany physician partners. With too manyphysician investors, there is often a dilutionof individual physician responsibility andownership interests. With less “skin in the
game,” physician investors often lose theircommitment to the ASC and often look forother alternatives.
11. Think Twice Before Opening aSecond Site. Business may be boomingand you may be considering opening a sec-ond site. Before embarking on this project,STOP! The surgery center business is basedon economies of scale and therefore the morecases that can be performed at any one sitewith one staff results in higher profits.Opening another site, with double over-heads, often results in diluting the profits atboth sites. For this reason, opening a secondsite is generally bad, not good, for business.
12. Third Party Reimbursement. Highreimbursement of procedures by third partypayors at ambulatory surgery centers is becoming more difficult to obtain. Further, reimbursement differs dramaticallythroughout the country. For this reason, amediocre ASC located in an area with strongthird party reimbursement may do betterthan a great ASC in a bad reimbursementmarket. There is almost no way to fix a center that is built in a market with poorreimbursement from third party payors.
13. Ophthalmology Procedures are StillProfitable. While many parties scoff at

5visit www.beckersasc.com
ophthalmology procedures, do not make ablanket decision to not seek ophthalmology asa specialty. Even with the changes in Medicarereimbursement, ASCs can still profit fromophthalmology procedures if the ASC has sig-nificant volumes and has effective internalcost control ( i.e., it is run very efficiently).
14. Pain Can be a Four Letter Word.Pain management services are often provid-ed in an office setting. Centers are increas-ingly concerned that physician investors willperform their pain management proceduresin their own offices rather than in the ASC.Medicare’s site of service differentials, whichoften pay more for in-office procedures,along with other incentives, may very wellencourage physician investors to performthese procedures in their own offices.Because of this, ASCs should plan accord-ingly and diversify services to accommodatea potential loss of pain management rev-enue. CMS has also proposed large reduc-tions in pain management reimbursementfor ASCs.
15. Endoscopy. Gastroenterologists willincreasingly have to minor in anesthesiolo-gy. Increasingly, payors will not pay physicians separately for anesthesia proce-dures provided in connection with gastroen-terology procedures. Thus, increasingly gastroenterologists must be competent atoffering all types of anesthesia procedures.
16. Plastics. Plastics, at least cosmeticsdriven plastics, are procedures that are bestleft to discussion in the movie “TheGraduate.” In “The Graduate,” DustinHoffman’s character is advised that plasticswill be the future. In surgery centers, plastics,particularly cosmetic procedures, do not pro-vide the type of future that we would like tosee. In many situations where the physicianbills globally, the ASC and physician can beadverse to each other and the ASC mustnegotiate its own rates with the surgeon.
17. Do Not Count on Bariatrics as aLong-Term Profit Center. Bariatric proce-dures are growing rapidly and increasinglybeing performed in ASCs. Initially, ASCs willearn outsized profits from these procedures.However, as the number of bariatricproviders increases and price competitionevolves, the prices on these procedures willeventually normalize and become less profitable. For this reason, and because thereremains substantial concerns regarding thesafety and risks related to bariatric programs, ASCs should use caution and beconservative when developing bariatric pro-grams. For more information on the risksinvolved in bariatric surgery see ModernHealthcare September 11, 2006.
18. Lasik. Lasik is best left to practicesrather than surgery centers.
19. Do Not Overbuild. Overbuilding anASC can result in its demise. A center thathas substantial fixed building and equip-ment costs, will likely face long term costproblems. To prevent this from happening,the ASC should be built to meet the expect-ed volume and specialty needs. There arenot many things that can predict the longterm death of a center more than over expen-diture on fixed building costs and fixedequipment costs. These are costs that almostnever go away. Where appropriate and fis-cally viable, an ASC may consider buildingto accommodate future growth but thisshould be done with caution.
20. A Great Staff Makes for aSuccessful ASC. A great staff is crucial toan efficient and profitable ASC. You need notnecessarily employ your staff full time.However, you are best off paying your staffextremely well and attempting to obtain thehighest quality staff – even if paid high on anhourly basis. It is also critical that you treatthe staff extremely well so that you are ableto recruit and retain the best possible staff.Finding and retaining an experienced andcompetent staff can be difficult.
21. Partnering with Single Physicians isRisky. An ASC developed with only one ortwo physician investors is a risky proposi-tion in most cases. It can create both politicaland financial problems. Often, one or two

6 visit www.beckersasc.com
physicians generally cannot generateenough business to make the operationprofitable. However, there are some situa-tions where an ASC can be profitable withonly one or two physician investors. Forexample, an ear, nose and throat physicianspecializing in sinus procedures may suc-ceed himself or with a single partner if theASC is run efficiently and the procedurevolume is high.
22. Small Hospitals Can Be a GoodAlternative. Increasingly, ASCs are success-fully converting into small surgical hospi-tals. Investors benefit because reimburse-ments tend to be higher and small hospitalshave more flexibility to add a variety of pro-cedures, which increases profits. However,there are substantial increased costs andrisks related to operating a small hospital.

7visit www.beckersasc.com
and coders or a billing company with specific ASC billing experience.
29. Do Not Discriminate Against Public Payors and TheirPatients.

ASC’s have 20 or fewer employees. Source:Federated Ambulatory Surgery Association.This means that surgery centers do not initially generate significant economies ofscale that lend themselves to formula driv-en sliding scale measures. The reason isthat a center must employ a core group ofstaff in order to operate. As an example, asurgery center will have relatively thesame number of staff to perform 100 casesper month that it will to perform 175 casesper month. This creates a measurementdilemma because staffing costs are fixedfor a base level of cases, and become some-what variable once the center performsadditional cases. Thus, there is no slidingscale or easy measure that states for eachadditional case, staffing should be “x.” Thefact remains that staffing is a “quasi-vari-able” cost. A core staff is required to oper-ate a center regardless of the number ofcases, but a variable element is introducedonce the center meets a base level of vol-ume each month. Using the previousexample, a surgery center may have 11.0FTEs to perform 125 cases, 12.0 FTEs for150 cases, and 13.0 FTEs for 200 cases permonth. Therefore, in this example,economies of scale begin to be derivedafter the initial 150 cases per month and donot play a significant part in staffing
options until the center reaches 200 or morecases a month.
Slicing the Data
With this dichotomy between fixed andvariable costs, how does a manager effectively measure and control this cost?We suggest that:
Staffing costs are measured based on the relative size of the ambulatorysurgery center as determined by its average number of cases performed relative to its case mix, market conditions and reimbursement.
This means that surgery centers should be“sliced” based on:
1.The number of cases performed per year.2.The type of cases performed by
specialty, or the case mix.3.The market conditions in terms of
wages paid to employees; and 4.The amount of reimbursement on the
cases performed by each specialty.
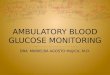
As discussed previously, there are feweconomies of scale until a center generatesat least 200 cases per month, or 2,400 casesper year. These centers (less than 2,400annual cases) should be grouped togetherand compared against one another since
their data is significantlydifferent than the largercenters. For example, amulti-specialty surgerycenter that performs 150cases per month musthave higher staffing costper case than a centerwith the same mix per-forming 500 cases permonth since there are feweconomies of scale gener-ated. See above.
Second, and perhaps more importantly, centersshould be grouped basedon the type of cases per-formed. A plastic surgerycenter will have radicallydifferent ratios than anendoscopy center. Thus,the data must be sortedbased on case mix.
Third, the common meas-urement tools shownbelow will be skewed ifthe market conditions areabnormal. For example,the wage paid to a
registered nurse in San Francisco will besignificantly different than the wage to thesame nurse paid in Thibodaux, Louisiana.The annual FASA Salary Survey is a goodtool to assess the relative impact of thissince it is sorted by region.
Finally, payer reimbursement also radicallyimpacts the ratio analysis. This is best illustrated by comparing a center that per-forms the majority of its cases at contractedrates with a center that performs a majori-ty of its cases out of network. While beingout of network impacts the number ofcases, the reimbursement per case is typi-cally higher. This will skew the ratios andmust be factored into the analysis.
Dicing – Key Measurement Tools
Once the surgery center is categorized withits peers, it should be further “diced” usingkey measurement tools to assess staffing.
Prior to using the measuring tools, anagreed upon definition of staffing costsmust be determined in order to best ana-lyze the data. We suggest hours worked atthe surgery center for the period (exclusiveof bonuses, paid time off and vacations) isbest for operational measures such asstaffing hours per patient and staffing costper patient. The benefits and bonusesshould be separated on the income state-ment and measured separately using easilyfound benchmarks that are beyond thescope of this article.1 Additionally, businessoffice staff must be included in the measurealong with administrative staff. The fol-lowing are key measures along with somegeneral guidelines:
1.Staffing as Percentage of Net Revenue - the total staffing cost (defined above) divided by the net revenue. Again, this should be interpreted based on the type of cases performed, the number of cases (small or large center), and the payer mix. For a large multi-specialty center, a range of between 23-25% is normal. For a high volume, high turnover center (i.e., endoscopy) this number is typically lower.
2.Staffing Cost Per Patient – the total staffing cost divided by the number of patients. This is a good measure, but must be interpreted properly. Again, the type of cases performed will be the major factor in determining an appropriate benchmark. Market salary conditions are also important. For a multi-specialty center performing 3,000 cases per year in a normal market, we like to see this below $325.00 per case.
8 visit www.beckersasc.com
I Heard I Was In Town – Measuring ASC Staffing Costs continued from page 1
1 For the benefit of the reader, we see benefits running between 23-25% of payroll exclusive of bonuses.

3.Staffing Hours Per Patient – this is one of the best tools. It is the total hours worked divided by the number of cases. This filters salary anomalies and revenue anomalies and measures productivity. Again, it is a per-patient measure and this necessitates that the data be interpreted based on the type of cases performed (i.e. a pediatric center

10 visit www.beckersasc.com
If a surgery center is supposed to be a for-profit venture, why are so many in thered? Over the past twenty-plus years
Luke Lambert, who is president ofAmbulatory Surgery Centers of America,or ASCOA, has started and/or turnedaround dozens of ASCs. Lambert sees five


12 visit www.beckersasc.com
1. Can you expand the types of procedures the ASC is performing?
2. Can you recruit additional partners?
3. Is there a local hospital that might buy into the venture?
4. Should you replace the adminis-

Here are nine tips from an outstanding ASC* leader on improving profits:
1. Nothing, NOTHING falls through the cracks. Our business manager looks to bill tons of stuff that was unbilled, not properly billed, etc.
2. We analyze every case with implants, etc., so that we don’t end up owing thousands of dollars for things like spinal cord stimulators that we will never be reimbursed for.
3. We relentlessly collect tons of deductibles and copays at the front desk on the day of service.
4. We are cutting down our expenses on everything from internet, phone bills, unnecessary generator maintenance, etc.
5. Our case load is up thanks to pain guys, ENT guys and working closely with surgeons.
6. Great collection efforts from the team.7. We have ridden ourselves of some less productive employees.8. We relentlessly track down money owed to us by surgeons and others. 9. We have decreased the monthly debt load.
In summary:
Increase case load + improved collections + renegotiating contracts +1000% increase in efficiency of our business office + relentless efforts on thecourting of surgeons + decreased monthly debt load after new loan =hopefully sustainable improvements.
* These are the editor’s comments and not the author’s comments.
How to Keep Results Up and SustainableBy Robert Welti, M.D. – Santa Barbara Surgical Center

14 visit www.beckersasc.com

15visit www.beckersasc.com
By some estimates, one-third to one-half of all surgery centers lose money. One reason: as the ASC marketmatures, increased competition has led to increased
pressures on existing ASCs. Yet that’s not the only reason.Listen to Tom Mallon, CEO of Regent Surgical Health, whichdevelops and turns around ASCs: “In one center we took over,the physicians were doing penile implants, which cost $6,000per procedure,” he says. “Yet reimbursement was only $400per procedure. So you might have happy patients, but yourpartners shouldn’t be happy.”
Beyond increased competition and out-of-control costs,Mallon has identified ten “fatal flaws” that routinely occur atunprofitable centers. The top five are:
■ Gross charges set at less than two times Medicare leads to unprofitability
Medicare reimburses surgery centers at 50 percent to 60 per-cent of costs, so if a center charges two times Medicare andgets paid full charges, nothing is left for debt repayment anddistributions, according to Mallon. The solution is to use ahigher multiple to set the center’s charge master. Mallon rec-ommends centers charge five to six times Medicare and to con-tinually review to ensure that costs are set at the right level.“With Medicare reimbursing you for 55 percent of costs, a lowcharge master is a certain way to lose money,” says Mallon.
■ Signing every contract doesn’t ensure a healthy center
In healthcare, administrators often sign insurance contractsthat aren’t profitable for the center. Mallon reminds centersthat an opening offer is usually not the best offer, and that con-tracts need to be negotiated and monitored over time. He rec-ommends that centers only contract with payers that representmore than 10 percent of a center’s patients, and that high costcases should be carved out.
■ Allowing one physician to run the business can lead to disenfranchisement
Most centers have a star physician that has been a catalyst forthe center’s development and is, on the flip side, a reason whythe center has not fulfilled its potential. Mallon and Regentwork with high profile physicians to give them the respect
Five Signs You’re In Need Of OutsideIntervention: RegentSurgical Health’sPerspectiveBy John Harris and Tom Mallon*

they deserve while coaching them on how tohelp grow the business. “Your greatest strengthcan be your greatest weakness,” he says. “Thetrick is to work with your biggest asset andwork to build something that is bigger andmore sustainable.”
■ Encouraging productive physicians to leave and start a new center
In centers that have been open for several years,Mallon says it is not uncommon for a group ofphysicians to leave and start a new center. Toprevent this, he recommends that centers andphysicians agree to long term agreements withlarge financial commitments. “You need tohave that commitment and buy-in from everyone at the center to start and continue tobe successful,” he says.
■ Controlling costs begins with knowing them
Many centers, Mallon says, don’t have a firmhandle on costs of staff, supplies and equip-ment. He routinely sees centers that are openfor 40 hours per week yet don’t have enoughcases, leaving employees idle between proce-dures, which drains the center financially.
Purchasing can be a problem; Mallon encour-ages centers to join a GPO and/or to shoparound. He also says used equipment not onlycomes with a warranty but costs 40 to 60 percent less than new equipment.
Mallon stresses that while centers are strongclinically, they often are not run like businesses.And if they aren’t, they’re probably not makingmoney, like the center that was doing $6,000penile implants and getting $400 for the procedure. It takes commitment on the part ofthe physician owners, the developer involvedand staff to turn a center around and keep itprofitable. And if it is profitable, not only willpatients be healthier, but the center will livelonger too.
* John Harris is the Founder of a5 Group, Inc. a consulting, marketingand public relations firm. He can be reached at 312-706-2529. TomMallon is the CEO of Regent Surgical Health. He can be reached at 708-492-0531.
16 visit www.beckersasc.com
To advertise inor subscribe to the
ASC Review, please contactMichelle or Ken Freeland
at 858-565-9921.

Surgery Centers change ownershipfrequently these days. Besides thefinancial, legal and regulatory
concerns, significant staffing concerns canimpede a smooth transition between owner-ship groups.
How did the employees hear about thesale of the center?
This can have a tremendous impact on theemployees. Do they feel that they were treat-ed fairly? With respect? With honesty?Although the responsibility of informing thestaff lies with the original owner, this delicatesituation is not always handled properly.
I recently took control of a center whererumors of an impending sale filled the hallswhile the employees and most of the physi-cians remained in the dark about the cen-ter’s future.
By the time the anxious and frustratedemployees met me, they posed many ques-tions I could not answer. Instead, I promiseda search for honest answers.
During most sales, the center’s original own-ers will fire all current employees, leavingthem to reapply for their old positions.Questions they may have include: Will mysalary stay the same? Will I keep myaccrued benefits, including vacation andsick time? Will my hours change? How willmy insurance coverage be affected? This isjust the beginning.
The center’s new owners often view allemployees as new hires. That means accruedvacation time, sick days and level on thesalary scale could be wiped clean, regardlessof an employee’s tenure.
In most instances, new owners strive to befair when dealing with salary history.Vacation equity may be more difficult fornew owner’s to match, and some companiesdon’t even differentiate between vacationtime and sick days. These are significantissues for employees who expect to havetheir earned time off honored.
Health Insurance.
Problems arise when the center had been
covered by a large group policy and the newowners secure individual coverage based onthe small number of employees. The costsincurred by employees will be much higher,and probably for fewer services, includingthe elimination of dental or vision coverage.Dependent coverage may cost hundreds ofdollars. If COBRA was not secured, pre-exist-ing conditions may apply. Be aware thatemployees may leave if insurance expensesincrease while coverage drops.
The next hurdle involved “guaranteedhours.”
Financial success of an ASC depends on con-trolling staffing costs, meaning employeescannot be guaranteed hours. Optimalstaffing is composed of a small group of corestaff who work full-time. This includes theBusiness Office staff, Administrator, ClinicalCoordinator, a few RNs and surgical techs.All other employees should be hired on apart-time or per diem basis.
Problems arise when the new owners comein with a new staffing philosophy that
Staffing a Turnaround CenterBy Ann Geier, RN, MS, CNOR, CASC Vice President of Operations, Ambulatory Surgical Centers of America, 843-216-2432
17visit www.beckersasc.com

eliminates full-time positions. This will notsit well with most of the employees.
So how do you get staff buy-in?
Meet with the employees.
Explain your staffing policies and be pre-pared to discuss the impact of those policieson the staff. Have alternate employmentsuggestions available for their considera-tion, as their hours will likely be reducedduring the transition and during the cen-ter’s start up.
Consider whether an employee needs towork a certain number of hours to be eligi-ble for health benefits. What are the mini-mum hours required by your insurer? Is theemployee cross-trained? If so, to whatareas? If not, are they agreeable to work inother areas?
Can you assign two employees to one posi-tion in a job-sharing scenario? Are per diempositions available in other local facilities?Suggest that employees work in more thanone facility until your volume builds up.
Is your work environment a positiveone?
Do people like being there? Are they treatedwell? Remember, you bring a fresh perspec-tive to the facility and have an opportunityto create a place where people want to work.
Attempt to keep the good employees.
Seek input from the previous managers andphysicians about the skills and qualifica-tions of the employees. I believe in keepingthe entire staff for a 90-day evaluation peri-od. Some workers may not be a good fit andwill leave, whether on their own or becauseof your coaxing. Talk with those who stay,and ask for their help, as things may be a bittight in the short term.
Ask your doctors for referrals.
Interview with a purpose. Look for employ-ees with a priority on customer service,strong work ethic, and the ASC mindset, asnot all clinical staff can adapt easily to theambulatory setting.
During the ownership transition you mayhave closed the center for one or two days aweek to reduce operating costs and fill theschedule. Staff will be swamped when thecenter is open, and, as always, ASC nurses
need to make pre-op and post-op calls. Ifthey are working long hours on Tuesday, thecenter is closed on Wednesday, and youhave a long day on Thursday, who willmake the calls? Develop a schedule tospread the responsibility throughout theentire staff.
Managing a center with new owners ismuch like overseeing a start-up center.Verify all information appearing on theemployee’s application and allow time fororientation and training in all requiredareas, like OSHA and fire safety. Eachemployee also needs to be familiar with thenew policies and procedures.
It may take a few months to build up thevolume of cases, especially if you areawaiting insurance contracts. You willneed loyal and dedicated employees, as thework will be hard and the hours may belong. Staff will stick with you if they seethat you are truly working with their bestinterests in mind. When a nurse you want-ed to keep leaves to work elsewhere,returns as a per diem, then turns down afull-time offer from a competitor becauseshe likes working in your center, then youknow you’ve succeeded.
18 visit www.beckersasc.com

19visit www.beckersasc.com

ASC Communications, Inc.77 West Wacker, Ste. 4100Chicago, Illinois [email protected]
PRSRT STDUS Postage
PAIDMerrill WI
54452Permit No 24