Embed Size (px)
Citation preview

Challenges and solutions
Stephanie Garcia-Tarodo, MD
02/07/2019

I have no actual or potential conflict of interest in relation to this presentation

1. Introduction
Epilepsy surgery: current trends
Particularities in infant population
2. Clinical application of MEG in infants
Technical perspective
Role in surgical decision process
3. Clinical outcome after surgery
Results of retrospective analysis

30% children with epilepsy develop drug refractory epilepsy (DRE)
Repercussions on development and cognition
DRE children are potential surgery candidates
Early surgery = longer period for developmental plasticity
Single-center RCT in children aged 10 mo – 17 yrs :
77% seizure free in surgery group compared to 7% in medical group
And yet, only 1% receive epilepsy surgery
(NEJM, 2017; 377(17): 1639-1647)

Obstacles vs Incentives for epilepsy surgery
Obstacles/disadvantages Incentives/advantages
Subtle/non-localizing semiology Preliminary epilepsy network
Generalized EEG pattern Developmental plasticity
Multiple etiologies Costs in the long-term
Supplementary investigations:
- Sedation
- Technical difficulties (head size…)
Improvement of QoL
- Motor
- Cognition
Limitation of intracranial EEG recording
Parental fear/opposition
Independency

Categorical predictors :
Age at seizure onset
Pathology
Identified lesion on MRI
Localized ictal EEG finding
Conditional predictors :
Timing of surgery
Surgery type‘Children 4 years or less were more likely to undergo
large resective operations (hemispherectomy and
multilobar procedures)’ ILAE Pediatric Epilepsy Surgery Survey Taskforce, 2008
Epilepsia 2008; 49(1): 146-155

Seizure
semiology
Infancy Childhood
Noninvasive presurgical evaluation
Scalp EEGMRI
SPECT
PET
MEG
Phase II
Surgery
Subdural grids SEEG

Detecting the origin of seizure activity
Sensitivity of 70% (Stefan et al, Brain 2003)
Non-redundant information in 33-35% of cases (Stefan et al, 2003; Sutherling et al, 2008)
Complimentary MEG-EEG data : tangential vs radial orientations of spikes
Concordance with the epileptogenic zone (Englot et al, Epilepsia 2015)
0
20
40
60
80
100
MEG + lobe ofresection
MEG + ECoG MEG + MRI
%
1. Presurgical evaluation 2. Postsurgical evaluation
Ages 5-79 years
Ages 3-68 years

Detecting the origin of seizure activity : sensitivity = 100% interictal, 55% ictal
Concordance with the epileptogenic zone
2 infants / 9 subjects 1 infant / 13 subjects
- MEG identified 1 clear focus with generalized EEG
findings in all 3 cases
- 62-67% concordance with MRI and/or ictal EEG
- No data on post-surgical outcome

Past reservations for use of MEG in infants
Head size and increased head to sensor distance
(1) Alternate head-side position (L/R hemisphere)
(2) ‘Reference’ or ‘neutral’ head position
Head movement and artifact
(1) Pre-recording : preparation procedures (allocation of time, parental accompaniment)
(2) Peri-recording : continuous head position monitoring (+/- 5 cm)
(3) Post-recording : temporally extended signal space separation (tSSS)

Effect of one anesthetic exposure on long-term behavioral changes in children Chemaly et al, J Clin Anesth 2014
DiMaggio et al, Anesth Analg 2011

MEG technologists : pediatric-trained, familiar to parents/child (PEMU)
Recording during natural sleep Sleep pattern, sleep deprivation
Time adaptation to feeding routine
Comfort/T°(heated blanket wrapping)
Time allocation : ‘Being on their schedule′o Preparation/installation : 1-2 hours
o Recording time : 60-80 minutes
Calming techniques o Parental presence during electrode placement
o Acknowledging specific anxiety/agitation trigger factors
o Technician remaining in the magnetically shielded room
o Maintains eye/physical contact
o Rapid to address signs of distress (sing a song, tell a story, calming voice)
Use of sedatives since 2013 :
0 infants

Technical adequacy : Non-sedative, non-invasive study
Head size and signal attenuation
tSSS and movement compensation
Localization of seizure focus : Concordance with the epileptogenic zone
Effect of MEG results on surgical management in infants : Additional information to the work-up
Surgical outcome

Inclusion criteria
- Children aged < 2 years (infants)
- Refractory epilepsy
- MEG in pre-surgical work-up between 01/2007 and 7/2017
Data collection
- Seizure history : semiology, age at onset, etiology
- Work-up : continuous vEEG, brain MRI, additional imagery (PET…)
- Phase II : SEEG, subdural grids
- If surgery :
Type of surgery
Follow-up (short/long term)
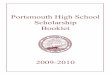
Total study population = 31 infants

Total pediatric MEG (2007-2017)
N = 407
Total number of patients : 341
Children (2-18 yrs)
n = 310 (91%)
Surgery
n= 126 (40.6%)
No surgery
n= 184 (59.4%)
Infant (< 2yrs)
n = 31 (9%)
Surgery
n = 18 (58%)
No surgery
n = 13 (42%)
0 10 20 30 40 50 60 70 80
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
Total MEG pediatric cases Infant cases Infant surgery cases
A
B

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Age at seizure onset Age at MEG Time MEG to surgery
< 1 month 1-6 months 7-12 months 13-24 months
3.5 mo 12 mo 3.5 mo
Age at seizure onset, MEG and surgery (with mean)
Seizure classification at onset
Generalized Focal Unknown
45.1%51.6%
Seizure etiology
TSC
FCD
Hemimegalencephaly
Vascular
Genetic
Unknown7
7

Supine position, magnetically shielded room
(248-) or 306-channel whole-head neuromagnetometer(Elekta, Helsinki; MAGNUS, San Diego)
5 head position indicator coils, continuous head position monitoring
Simultaneous EEG : 22- or 32-channels
Acquisition parameters :- Sampling rate : 1000 Hz
- Band-pass filter : 0.1 to 330 Hz
tSSS method
Source analysis : multiple ECD model
Dipole fitting Reduced Chi square, ~2.0
Goodness to fit > 80%

Positive interictal spikes on MEG recordings : sensitivity
MEG findings 1st exam Total exams
Positive (interictal +/- ictal) 28 33
Negative (normal or inconclusive) 3 4
90% 89%
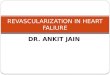
0 2 4 6 8 10 12 14 16 18
MRI
EEG
MEG
MEG, EEG and MRI localizing results
Multifocal, bilateral Multifocal, unilateral Focal Negative
- Interictal foci : MEG = 14, EEG = 6
- MRI negative group = 9/31 infants
- 4/9 focal localization on MEG
- 8/9 multifocal discharges on EEG

18/31 infants subsequently had surgery within 12 months of MEG recordings
2 infants had subdural grid placement
1 with bilateral EEG but unilateral MEG findings focal resection, Engel I (46 mo)
0 2 4 6 8 10 12 14
Surgey outcome
Type of surgery
Focal resection
Partial disconnection
Hemispherectomy
Engel I
Engel II
Engel III-IVFollow-up period:
- Mean 20.6 mo
- Range 4-55 mo

Influence of MEG results on surgery type :
Focal resection (total = 9)
5/9 focal findings on EEG + MEG Engel I
2/9 focal findings on MEG + bifocal on EEG + normal/multifocal on MRI Engel I and II
Partial disconnection or corpus callosotomy (total = 5): multiple lesions and seizure types
1/5 multifocal findings EEG + focal on MEG Engel I
Hemispherotomy : extensive lesions to one hemisphere
3/4 multifocal and lateralizing on EEG + MEG Engel I
MRI negative
4/9 focal on MEG (8/9 multifocal on EEG) : 3/4 surgery Engel I (1), Engel II (1)

GroupPatients with good post-surgery outcome/patients with surgery
Both MEG and MRI identify focal 7/8 (correct prediction)
Neither MEG and MRI identify focal 0/1 (wrong prediction)
Negative MRI but MEG identifies focal 2/3 (correct prediction by MEG)
Positive MRI but multifocal MEG 5/7 (correct prediction by MRI)
Correlation between MEG and MRI
and effect on outcome prediction
Seizure free
(Engel I)
Non seizure free
(Engel II-IV)
Sensitivity/PPV
Positive likelihood ratio
Focal MEG 8 2 61.5%/80%
1.53Multifocal MEG 5 3
Positive MRI 12 3 92%/80%
1.53Negative MRI 1 2
Focal EEG 5 0 36%/100%
Multifocal EEG 9 4
Sensitivity :
MRI > MEG > EEG
Positive predictive value :
EEG > MRI = MEG

Well established protocols for MEG recording in infants
Counteract technical issues with head size and movement
Non invasive and non-sedative method of data retrieval
MEG has a good sensitivity in depicting epileptiform activity in infants
MEG provides additional information to EEG/MRI
Generalized EEG pattern
Negative MRI
MEG has a predictive role in surgical outcome
80% of infants with a focal MEG became seizure free after surgery
Widespread use in all age groups
Valid
Complementary
Broaden surgical candidacy in infants
Applicability of MEG to infants = earlier surgery interventions, better outcomes

Michael Funke, MD, PhD – Director of MEG
Gretchen Von Allmen, MD – Director UT Pediatric Epilepsy Program
Michael Watkins, MD – Pediatric Epileptologist
Jeremy Lankford, MD – Pediatric Epileptologist
Manish Shah, MD – Pediatric Epilepsy Neurosurgeon
Nitin Tandon, MD –Epilepsy Neurosurgeon
Lisa Caballero and Wayne Mead – MEG Technicians

Bagic A, Funke ME, Ebersole J. American Clinical MEG Society (ACMEGS) position statement: the value of magnetoencephalography (MEG)/magnetic source imaging (MSI) in noninvasive presurgical evaluation of patients with medically intractable localization-related epilepsy. J Clin Neurophysiol 2009; 25: 1-4
Stefan H, Hummel C, Scheler G et al. Magnetic brain source imaging of focal epileptic activity: a synopsis of 455 cases.Brain 2003; 126: 2396-2405.
Englot DJ, Nagarajan SS, Imber BS et al. Epileptogenic zone localization using magnetoencephalography predicts seizure freedom in epileptic surgery. Epilepsia 2015; 56: 949-958.
Albert GW, Ibrahim GM, Otsubo H et al. Magnetoencephalography-guided resection of epileptogenic foci in children. J Neurosurg Pediatrics 2014; 14: 532-537.
Shibata S, Mosher JC, Kotagal P et al. Magnetoencephalographic recordings (MEG) in infants using a standard-sized array: technical adequacy and diagnostic yield. J Clin Neurophysiol 2017; 34: 461-468.
Shukla G, Kazutaka J, Gupta A et al. Magnetoencephalographic identification of epileptic focus in children with generalized electrographic (EEG) features but focal imaging abnormalities. J Child Neurol 2017; 32: 981-995.
Harvey AS, Cross JH, Shinnar S, Mathern GW, ILAE Pediatric Epilepsy Surgery Survey Taskforce. Defining the spectrum of international practice in pediatric epilepsy surgery patients. Epilepsia 2013; 49(1): 146-155
Chemaly M, El-Rajab MA, Ziade FM, Naja ZM. Effect of one anesthetic exposure on long-term behavioral changes in children. J Clin Anesth 2014; 26(7): 551-556
Englot DJ, Han SJ, Rolston JD et al. Epilepsy surgery faliure in children: a quantitative and qualitative analysis. J Neurosurg Pediatrics 2014; 14: 386-395