-
Neuroprognostication
San Francisco, September 28TH 2018
-
Disclosures:
➢No stocks, stock options etc.
➢ I have received restricted educational grants from, or given
lectures at sponsored events for, the following companies: Zoll,
Baxter, Otsuka, and Medivance (now Bard).
➢No relevance to the content of this presentation
➢The conclusions and recommendations in this talk are my
own.
-
“Predicting is tricky, especially about the future”
– Niels Bohr / Yogi Berra
The problem:
-
“Predicting is tricky, especially about the future”
– Niels Bohr / Yogi Berra
The problem:
-
What are the causes of death in cardiac arrest
patients who achieve ROSC and reach the
hospital alive?
➢Early mortality is usually related to initial myocardial
stunning and cardiogenic shock, leading to tissue hypoperfusion and
development of multiple organ failure [5, 6].
➢ In patients who survive the first 24-48 hours of admission,
prognosis is mostly related to the severity of brain injury
Lemiale V et al. Intensive Care Med 2013;39:1972–1980; Sandroni
C et al. Minerva Anestesiol
2016;82:989–999
-
Hemodynamic monitoring…….
The simple measurements:
➢ Blood pressure
➢ Heart rate
➢ Urinary output, capillary refill, peripheral temperature,
etc.
More sophisticated measurements: continuous or intermittent,
pressure or volume
➢ Cardiac output (PA catheter, PiCCO, LidCO, FloTrac,
Echocardiography)
➢ Stroke volume variation (arterial line, PiCCO, LidCO,
FloTrac)
➢ Venous saturation (Central venous catheter)
➢ Mixed venous saturation (PA catheter)
➢ Extra-vascular lung water (PiCCO device)
➢ Blood volume (PiCCO, LidCO device)
➢ Intra-thoracic blood volume (PiCCO device)
➢ Systolic/diastolic function (TEE/TTE, PiCCO, LidCO)
➢ Biochemical parameters: base excess, (serial) lactate
measurements, creatinin
-
Neuromonitoring:
➢ To guide treatment
➢ To predict prognosis
-
➢ Clinical assessment: sensorium, reflexes, “wake up test”, GCS,
clinical assessment of epileptic activity
➢ “General” monitoring: lab values, circulation, oxygenation/
saturation
CNS monitoring - 1
-
➢ Clinical assessment: sensorium, reflexes, “wake up test”, GCS,
clinical assessment of epileptic activity
➢ “General” monitoring: lab values, circulation, oxygenation/
saturation
➢ Radiological evaluation: CT scan, MRI
➢ Electroencephalography (raw EEG, compressed spectral arrays
(CSA), 95% spectral edge, etc.)
CNS monitoring - 1
-
➢ Non-invasive monitoring: Near infrared spectroscopy (NIRS)
➢ Invasive monitoring: Intracranial pressure (ICP, Licox,),
other
➢ Evoked potentials (esp. somatosensory evoked potentials)
➢ Transcranial doppler studies (MCA flow velocity)
➢ Jugular bulb saturation (central line)
➢ Lab: neuron-specific enolase, CRP, others?
➢ Automated Pupillometry
CNS monitoring - 2
-
➢ Clinical exam
➢ EEG
➢ Evoked potentials (esp. somatosensory evoked potentials)
➢ CT
➢ MRI
➢ Automated Pupillometry
CNS monitoring - 3
-
Monitoring patients with brain injuries…
-
If and when you decide to use a device
to obtain hemodynamic and CNS
measurements:
Always ask yourself beforehand:
➢Which data do I really need? Which
parameters am I actually going to use?
➢What am I going to do with these data?? (how will this improve
the outcome in my patients??)
➢ Is this information worth the (procedural) risk in
this patient? (The more invasive a measurement, the more urgent
this question becomes!)
-
Production of
free radicals (O2,
NO2, H2O2, OH-)
Reperfusion
injury
Immune response,
neuroinflammation
Ion pump
dysfunction, influx of
calcium into cell,
neuroexcitotoxicity
Cell membrane leakage, formation of
cytotoxic edema, intracellular acidosis
Mitochondrial
injury and
dysfunction
Increased
vascular permeability,
edema formation
“Cerebral thermo-
pooling” and local
hyperthermia
Coagulation
activation,
formation of
micro-thrombi
Harmful
changes in
cerebral
metabolism
Permeability of the
blood-brain barrier,
edema formation
Epileptic activity &
seizures
Apoptosis, calpain-
mediated proteolysis,
DNA injury
Local generation of
endothelin & TxA2;
generation of
prostaglandins
Decreased
tolerance for
ischemia
Spreading
depression-like
depolarizations
Activation of
protective
“Early genes”
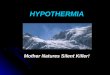
Destructive processes following
ischemia/reperfusion. that can be
Blue lettering = early mechanisms
Red lettering = late mechanisms
Adapted from: Polderman KH. Mechanisms of action,
physiologic effects and complications of hypothermia.
Crit Care Med 2009; 37[Suppl.]:S186 –S202
Decrease in cerebral
repair mechanisms;
acidosis, production of
toxic metabolites
-
Direct neuronal disruption Blood-brain barrier injury
Cytotoxic oedemaVasogenic oedema
IschemiaHyperemia
Intracranial hypertension
Hematoma
CSF volume(due to blocking of ventricular drainage)
Increased cerebral blood volume
-
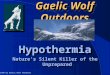
100
0
40
60
80
20
Volume
ICP mm Hg
ICP controlled due
to compensation
Small volume
marked ICP
ICP-Volume Curve
-
So:
ICP may be a marker for ongoing cerebral injury
ICP may be a cause of additional cerebral injury
-
➢Brain tissue oxygen monitoring
-
Partial Pressure of Brain oxygen tension
• Licox® : brain oxygen tension monitor : PbtO2
– pO2 sensitive area is 14 mm3
– Normal white matter PbtO2 = 25 mmHg
Normal tissue
• PbtO2 normal
• Autoregulation intact
Penumbral tissue
• PbtO2 low
• Autoregulation may be disturbed,
Dead tissue
• PtiO2
-
DIRECT Cerebral blood flow
• Measuring method
– CTP/MRP : Temporal resolution
– Xenon CT: Availability?
– TCD: surrogate for CBF (mFV )
– Laser Doppler
– Hemedex Perfusion monitor
ρсδΤ/δt = Δ(K ΔT) + CBF*ρblood*сblood*ρ(ΔT) + Qm
Thermal energy
movementPassive
Conduction
Active
convection by
CBF
Metabolic heat
generation
stable
Calculation after
calibration
-
May help guide appropriate CPP
target in individual patients• Range of autoregulation •
Clinical utility: trend monitor
– Vasospasm after SAH Vajkoczy P J Neurosurg 2003
– Aneurysm surgery and
vessel occlusion
Thome C J Neurosurg 2001
– Traumatic brain injury
deterioration
Jaeger M Acta Neurochir (Wien) 2005
– Ischemic stroke progression
– ECA/ICA bypass
– Early detection of hyperperfusion
syndrome after stenting
-
Trans-cranial Doppler (TCD)
➢ Ultrasound at frequencies of 2 MHz
➢ Trans-temporal route above the zygomatic arch➢ ACA, MCA,
PCA
➢ Trans-orbital approach➢ Carotid artery
➢ Sub-occipital route through the foramen magnum➢ BA, VA
➢ Limitation: ➢ Small or absent trans-temporal
windows or thick calvaria
➢ Keeping the probe in the same position
-Nousheh Saidi et al. Sem Cardiothor Vasc Anesth 2005; 9:17 -
23.
-
Near-infrared Reflectance
Spectroscopy (NIRS)
➢ Cerebral Oximetry
➢ Wavelength of 650~1100nm
➢ Bi-hemispheric measure of cerebral
regional oxygen saturation (rSO2)
through the intact calvarium
➢ A positive predictive value between low
rSO2 and adverse CNS outcomes
Murkin JM. Semin Cardiothor Vasc Anesth 2004; 8:167 - 171.
-
Brain metabolism: Microdialysis
Cerebral microdialysis
-
(Continuous) EEG
➢ Requirement of a dedicated technician
for placement of the electrodes
➢ Subjective nature of interpretation
➢ Electrical signal interference
-
(Continuous) EEG
➢ 12-45% of cardiac arrest patients may
develop seizure activity, which is often sub-
clinical
-
Jugular Bulb oximetry
➢ Normal SjO2 55-70 %
➢ Higher extraction in case of ischemia; lower SjO2
➢ Global indicator for brain oxygenaton
➢Monitor hyperventilation
-
MRI, CT, ultrasound, TEE etc. in the ICU…
• Portable, 64 Slice
• High-resolution
• CT, CTA, CTP
-
CT scan
-
MRI scan
-
MRI scan
-
Automated Pupillometry
➢ Tamura T, Namiki J, Sugawara Y, Sekine K, Yo K, KanayaT,
Yokobori S, Roberts R, Abe T, Yokota H, Sasaki J. Quantitative
assessment of pupillary light reflex for early prediction of
outcomes after out-of-hospital cardiac arrest: A multicentre
prospective observational study. Resuscitation. 2018
Oct;131:108-113. doi: 10.1016/j.resuscitation.2018.06.027. Epub
2018 Jun 26.
➢ Solari D, Rossetti AO, Carteron L, Miroz JP, Novy J, Eckert P,
Oddo M. Early prediction of coma recovery after cardiac arrest with
blinded pupillometry. Ann Neurol. 2017 Jun;81(6):804-810. doi:
10.1002/ana.24943. Epub 2017 Jun 2.
➢ Suys T, Bouzat P, Marques-Vidal P, Sala N, Payen JF, Rossetti
AO, Oddo M. Automated quantitative pupillometry for the
prognostication of coma after cardiac arrest.NeurocritCare. 2014
Oct;21(2):300-8. doi: 10.1007/s12028-014-9981-z.n
-
Automated Pupillometry➢ The 0-hour PLR best predicted both
90-day survival
(AUC = 0.82, cutoff 3%, sensitivity 0.87, specificity 0.80) and
favourable neurological outcomes (AUC = 0.84, cutoff 6%,
sensitivity 0.92, specificity 0.74). No patient with a 6-hour PLR
less than 3% survived for 90 days after CA.
➢ At 48 hours, a quantitative PLR 0.20).
-
Automated Pupillometry➢ The 0-hour PLR best predicted both
90-day survival
(AUC = 0.82, cutoff 3%, sensitivity 0.87, specificity 0.80) and
favourable neurological outcomes (AUC = 0.84, cutoff 6%,
sensitivity 0.92, specificity 0.74). No patient with a 6-hour PLR
less than 3% survived for 90 days after CA.
➢ At 48 hours, a quantitative PLR 0.20).
➢ However, presence of pupillary reflexes at 72 h does not
reliably predict good neurological recovery (PPV 60%). Absence in
the first 24 hrs still has FPR of 10%
-
Outcome prediction…..
https://www.resus.org.uk/resuscitation-guidelines/post-resuscitation-
care/#prognostication
https://www.google.com/url?sa=i&source=images&cd=&cad=rja&uact=8&ved=2ahUKEwjw0YOJ_5DbAhVDVLwKHejGCbcQjRx6BAgBEAU&url=https://www.pinterest.com/pin/529947081137319786/&psig=AOvVaw207uaA2vJ5j5sdtYv7q7N5&ust=1526792388595745
-
➢ Poor neuro exam
➢ (Absence of) sensory-evoked potentials
➢ MRI (edema, low DWI)
➢ CT (cerebral edema, decreased gray–white
differentiation)
➢ Neuron-specific enolase
➢ “Flat” EEG…
Outcome prediction…..
-
➢ Poor neuro exam: Bilateral absence of pupillary light
reflex at 72hrs from ROSC predicts poor outcome (0-4%
FPR) but the sensitivity is only 19%➢ I.E., only 1 in 5 of those
who eventually have a bad outcome will have fixed
pupils at 72 h.
➢ Similar numbers for bilaterally absent corneal reflex
➢ Absent or extensor motor response at 72hrs from ROSC
has a 75% sensitivity for prediction of poor outcome, with
an FPR of 27%.
➢ Presence of myoclonic jerks is not consistently associated
with poor outcome (FPR 9%). Status myoclonus >48hrs
from ROSC is associated with poor outcome (FPR 0-2%.
95% CI 0–5%; sensitivity 8–16%.
Outcome prediction…..
-
➢ The most sensitive indicator is (absence of)
sensory-evoked potentials, though even this should
not be used by itself to make decisions to withdraw
care (false-negative 0-4%)
➢ FPR 0–2% with upper 95% CI of about 4%
➢ SSEP recording requires appropriate skills and
experience, and utmost care should be taken to
avoid electrical interference from muscle artefacts
Outcome prediction…..
-
➢ “Flat” EEG… FPR of 0–2% (upper 95% CI of about
7%).
Outcome prediction…..
-
Outcome prediction…..
-
➢ Poor neuro exam with no improvement in several
days; no sedation effect; absent pupillary, corneal
reflex➢ (Remember, TTM can slow hepatic clearance of sedatives,
especially
benzo’s!!)
➢ Absent sensory-evoked potentials: high sensitivity and
specificity.
➢ MRI (edema, low DWI) high sensitivity, decent specificity.
➢ CT (cerebral edema, decreased gray–white
differentiation) high sensitivity, decent specificity
➢ Neuron-specific enolase moderate sensitivity and
specificity
➢ “Flat” EEG… high sensitivity and specificity
➢ Automated pupillometry: very promising initial data.
Outcome prediction…..
-
Jackson MJ et al.
Prognostication of patients after
cardiopulmonary resuscitation
BJA Education,2018;1e7
https://www.resus.org.uk/resuscit
ation-guidelines/post-
resuscitation-
care/#prognostication
-
Thank you for your attention!
[email protected]
-
Thank you!
-
Monitoring patients with brain injuries…
-
☺ My aim today is to get you to look at
a few things that you may take for
granted in a slightly different way.