Embed Size (px)
Citation preview

Journal of The Association of Physicians of India ■ Vol. 64 ■ June 201674
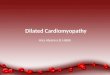
Fig. 1: ECG on day 1
Hypocalcemic Cardiomyopathy and Pseudohypoparathyroidism Due to Severe Vitamin D DeficiencyCM Batra1, Rajiv Agarwal2
AbstractHypocalcemic cardiomyopathy is a rare entity. We describe a patient with severe heart failure, decreased ejection fraction and global hypokinesia documented on echocardiogram, associated with severe hypocalcemia, very low vitamin D status, increased QT intervals, increased BNP (serum brain natriuretic peptide) levels and CPK (creatine phosphokinase) levels. All these defects reversed on treatment with vitamin D and calcium within a few days without any specific cardiac intervention.
1Senior Consultant Endocrinologist, Indraprastha Apollo Hospital; 2 Senior Consultant Cardiologist, Batra Hospital and Medical Research Centre, New DelhiReceived: 12.12.2013; Revised; 12.05.2014; Accepted: 02.08.2014
Introduction
Heart failure in elderly patients can be due to several etiologies.
An elderly female was admitted with severe heart failure. The underlying cause was found to be hypocalcemia secondary to severe hypovitaminosis-D.
Case Report
A 68 year old female was admitted w i t h c o m p l a i n t s o f r e s t l e s s n e s s orthopnea and drowsiness since 4 days. She had diabeties since 15 years controlled on 5 mg of glibenclamide.
S h e w a s d i a g n o s e d w i t h cholelithiasis 6 years ago with constant
dull abdominal pain and three episodes of colicky pain. She also had recurrent episodes of urinary tract infection for the last 2 years. Her calcium intake was poor. She was a vegetarian, who avoided milk and milk products due to dyspepsia. There was no family history of seizures, tetany or hypocalcemia and no history of neck surgery or radiation.
On examination she had a pulse rate of 92/minute, blood pressure 150/90 mm of Hg, jugular venous pressure was increased. She was afebrile, had bilateral pedal edema and bilateral basal crepts, Chvostek’s and Trousseau’s signs were negative. Her heart sounds were accentuated but there was no murmur. She was drowsy but oriented to time, place and person. There was no focal neurological deficit.
No papilledema was noted.A clinical diagnosis of congestive
h e a r t f a i l u r e , h y p e r t e n s i o n a n d m e t a b o l i c e n c e p h a l o p a t h y w a s made and the patient was started on furosemide, ramipril, spironolactone and subcutaneous insulin. The initial set of investigations were done (Table 1 and Figure 1).
A further set of investigations was done on the second day of admission and the results of these were as in Table 2 . This pat ient had chronic severe hypocalcemia with severe hyperphosphatemia, high normal PTH, severe vitamin D deficiency, with inadequate response of PTH to vitamin D deficiency and renal insufficiency, type 2 diabetes , cardiomyopathy, nephropathy, urinary tract infection with severe dilutional hyponatremia. The patient was treated with slow infusion of hypertonic saline, calcium g l u c o n a t e , i n j e c t i b l e v i t a m i n D and injectible antibiotics. She was also dialyzed in view of refractory hypophosphatemia.
She responded well to this treatment regimen Serum calcium increased g r a d u a l l y a n d s e r u m p h o s p h a t e decreased. After 5 days of treatment her repeat tests were as shown in Table 2. The ECG showed that ST flattening had reversed but QTc was still elevated (Figure 2).
A repeat echocardiogram on the fourth day of treatment showed left ventricular ejection fraction of 60% and there was no hypokinesia. All her cardiac drugs were stopped. When her serum calcium became 8.1 mg/dl on the tenth day, the calcium infusion was also stopped and antibiotics were also stopped. She was put on subcutaneous insulin, 2 grams of calcium and 1 ug of
Table 1: Investigations – 1st day
X-ray chest Features of pulmonary edema
ECG Flattening of ST segment and a prolonged corrected QT segment of 520 milliseconds (n<440 ms)
2D-Echocardiogram Global hypokinesia with a reduced ejection fraction of 45%
Renal functions Blood urea 75 mg/dl, serum creatinine 1.6 mg/dl, serum sodium 115 meq/l, potassium 4.7 meq/l
Serum brain naturietic peptide (NT-Pro BNP)
5973 PG/DL (>900 indicates congestive heart failure)
Creatine phospokinase (CPK)
626 u/l (n=24-195)
CPK (MB) 3.54%Haemogram Hb 8.9 gm%, TLC 14000/
cumm, (P65 L35)
C a s e R e p o R t s

Journal of The Association of Physicians of India ■ Vol. 64 ■ June 2016 75
calcitriol /day and discharged (Figure 3).
S h e wa s r e a d m i t t e d , a m o n t h later for cholecystectomy and al l her biochemical parameters were reassessed Tables 2 and 3.
Discussion
Hypocalcemic cardiomyopathy is a rare entity but well documented in literature. The physiological basis of hypocalcemic cardiomyopathy is that impaired intracellular calcium metabolism plays an important part in the pathogenesis of congestive heart failure. Extracellular calcium is needed to init iate myocardial contraction because sarcoplasmic reticulum does not have enough calcium. Calcium ion is needed for the depolarization repolarization phase of the cardiac cycle and activation of actin so that myosin can form cross bridges to cause contract ion. 2 Hypocalcemia can cause delays in the conduction of cardiac impulse and also weaken contractibil ity.3 The most common c a u s e o f h y p o c a l c e m i c i n d u c e d heart failure in children is vitamin D deficiency whereas in adults primary h y p o p a r a t h y r o i d i s m , v i t a m i n D deficiency, chronic kidney disease and bisphosphonate therapy.4
Calci tr iol has direct ef fects on
myocardial cell function. Calcitriol receptors have been demonstrated in heart myoblast cells and myocytes. An intracellular vitamin D dependant calcium binding protein has been i s o l a t e d f r o m t h e h e a r t m u s c l e . Calcitriol rapidly increases heart tissue calcium uptake which can be blocked by calcium channel blockers.5
Endomyocardial biopsy in cases o f l o n g s t a n d i n g h y p o c a l c e m i c cardiomyopathy in two cases of untreated primary hypoparathyroidism showed degenerated and regenerated muscle fibres with rough, hyperchromatic nuclei and myocytes without nuclei and with pale cytoplasm together with increased fibrous tissue between myocytes, amyloid staining was found negat ive . 6 Sect ions of myocardial tissue from vitamin D deficient rats demonstrated that total myofibrillar area was reduced.This reduction was accompanied by doubl ing of non myofibrillar tissue which was found to be collagen.5
The biochemical features of vitamin D d e f i c i e n c y a r e h y p o c a l c e m i a , hypophosphatemia, increased PTH and increased alkaline phosphatase. Hypophosphatemia is due to decreased intestinal absorption and exaggerated phosphaturic effect of PTH on renal tubular cells.7
Renal resistance to parathyroid
h o r m o n e ( P T H ) i s a w e l l c h a r a c t e r i z e d a b n o r m a l i t y i n pseudohypoparathyroidism. In most patients this resistance is manifested by both impaired cyclic adenosine monophosphate (C AMP) generation in response to PTH and hyperphosphatemia due to increased tubular reabsorption o f p h o s p h a t e . T h i s s y n d r o m e i s called pseudohypoparathyroidism type 1 . In a few patients there is hyperphosphatemia despite a normal CAMP response to PTH, This is called pseudohypoparathyroidism type 2.8
Furthermore biochemical findings resembling pseudohypoparathyroidism have been found in in several patients with vitamin D depletion.8
Rao first reported that in 6/8 of his patients with severe hypocalcemia due to vitamin D deficiency, PTH increased and basal excretion of cAMP increased but phosphaturic response was blunted. This was restored in all 6 of these patients after correction of vit D and calcium levels.8 In contrast, in 13 patients of normocalcemic vitamin D deficiency the phosphaturic response was increased and normalized after treatment. The phosphaturic response was also increased in 72 of his cases of primary hyperparathyroidism. Rao concluded that the effect of endogenous PTH on phosphate reabsorption varies with the level of serum calcium and that dissociation between this effect and generation of cAMP is non specific and can be a consequence of hypocalcemia. Rao has suggested that vit D deficiency must be excluded for a diagnosis of pseudo-hypoparathyroidism type 2 in a patient presenting with low serum calcium, high phosphate and high PTH levels without somatic features of Albright’s Hereditary Osteodystrophy.8
Bhansali reported a case of severe vit D deficiency and hypocalcemia mimicking pseudohypoparathyroidism type 2 in which, in spite of increased PTH, there was hyperphosphatemia
Table 2: Investigations - 2nd to 30th day
Investigations 2nd Day 5th Day 30th Day Serum calcium (mg/dl) 4.3 7.1 9.6 Serum phosphorous (mg/dl) 14.3 5.5 5.2 Serum PTH (pg/ml) 57.8 48.4 18.35 Serum 25 oh vitamin D (ng/dl) <4 9.71 39.2 Serum magnesium (mg/dl) 2.1 1.7 2.2 Blood urea (mg/dl) 75 64 40 Serum creatnine (mg/dl) 1.6 1.4 1.2 24 hours urinary Ca (mg/day) 29.7 14.6 120 24 hours urinary phosphorous (mg/day) 260 114 700 24 hours urinary protein (mg/day) 317.9 214 Creatnine clearance (ml/min) 21 14.7 32 TRP (tubular reabsorption of phosphate) 95% Not done 79%
Fig. 2: ECG after 4 days
Fig. 3: ECG after 20 days
Table 3: Investigations day 30
DMSA renal scan Showed a photon deficient area in upper pole of right kidney suggestive of pyelonephritis. The GFR in right kidney was 5 ml/min and left kidney 27 ml/min.
25 (OH)2 vitamin D 40 pg/ml (15-60 pg/ml)CT brain Calcification of basal
ganglia Serum electrophoresis normal

Journal of The Association of Physicians of India ■ Vol. 64 ■ June 201676
and TRP was 95% with a 24 hours urinary excretion of phosphate of 298 mg/day. Vitamin D and calcium therapy normalized the excretion of phosphorous to 780 mg/day and TRP to 75%.7,9
Our patient had severe hypocalcemia 4.3 mg/dl, severe hyperphosphatemia 14.3mg/dl, severe vitamin D deficiency <4 ng/dl, high normal PTH of 57 pg/ml, and an increased tubular reabsorption of phosphate of 95%. She also had impaired renal funct ions in form of a blood urea of 75 mg/dl, serum creatinine 1.6 mg/dl and 24 hours urinary protein of 317 mg/day with a creatinine clearance of 21 ml/min.
The severe hyperphosphatemia and decreased clearance of phosphorous gradually improved with calcium and vitamin D therapy and the treatment of urinary tract infection leading to improved creatinine clearance from 21 ml/min to 32 ml/min. TRP of 95% on 2nd day of admission normalized to 79% on after 1 month of treatment and 24 hours urinary phosphate excretion increased from 240 mg/day to 700 mg/day after 1 month of treatment.
T h e i m p r o v e m e n t i n hyperphosphatemia and increase in phosphaturia was partly due to correction of renal dysfunction. It is very difficult to say how much was
due to resolution of pseudo hypo parathyroidism by calcium and vitamin D therapy and how much was due to improvement of renal failure. The renal failure with a creatinine of 1.6 mg/dl and a creatinine clearance of 21 ml/min was not severe enough to cause a rise in serum phosphate to 14.3mg/dl as seen in our patient. The increase in creatnine clearance from 21 to 32 ml/min alone does not explain the improvement in TRP from 95% to 79%. We postulate that calc ium, vi tamin D and 1 ,25 (OH)2vitamin D therapy had a role in increasing the phosphate excretion by reversing pseudohypoparthyroidism type 2 that this patient had in addition to renal dysfunction.
This patient had a PTH of 57 pg/ml in spite of severe vitamin D deficiency and renal insufficiency. A blunted PTH response to low vitamin D has been termed functional hypoparathyroidism (FHPT) which is common. Only 30-50% of pat ients respond to vi tamin D deficiency with increased PTH.10
Conclusion
Hypocalcemic cardiomyopathy is a rare but reversible cause of congestive heart failure. Chvostek and Trousseau’s s ign . Increased QTc inteval >440 milliseconds is a clue to check serum calcium levels. Severe hypocalcemic
vitamin D deficiency can present as pseudohypoparathyroidism type 2, which is reversible on treatment.
References1. Brown J, Nunez S, Russell M, Spurney C. Hypocalcemic rickets
and dilated cardiomyopathy: case reports and review of literature. Pediatr Cardiol 2009; 30:818-23.
2. Lehmann G, Deisenhofer I, Ndrepepa G, Schmitt C. ECG changes in a 25-year-old woman with hypocalcemia due to hypoparathyroidism. Hypocalcemia mimicking acute myocardial infarction. Chest 2000; 118:260-2.
3. Harrigya A, Schwartz A. Rate of calcium binding and uptake in normal animal and failing human cardiac muscle. Circulation Res 1969; 25:781.
4. Kazmi AS, Wall BM. Reversible congestive heart failure related to profound hypocalcemia secondary to hypoparathyroidism. Am J Med Sci 2007; 333:226-9.
5. Weishaar RE, Simpson RU. The involvement of the endocrine system in regulating cardiovascular function: emphasis on vitamin D3. Endocr Rev 1989; 10:351-65.
6. Altunbaş H, Balci MK, Yazicioğlu G, Semiz E, Ozbilim G, Karayalçin U. Hypocalcemic cardiomyopathy due to untreated hypoparathyroidism. Horm Res 2003; 59:201-4.
7. Shriraam M, Bhansali A, Velayutham P. Vitamin D deficiency masquerading as pseudohypoparathyroidism type 2. J Assoc Physicians India 2003; 51:619-20.
8. Rao DS, Parfitt AM, Kleerekoper M, Pumo BS, Frame B. Dissociation between the effects of endogenous parathyroid hormone on adenosine 3’,5’-monophosphate generation and phosphate reabsorption in hypocalcemia due to vitamin D depletion: An acquired disorder resembling pseudohypoparathyroidism type 2. J Clin Endocrinol Metab 1985; 61:285-90.
9. Dandona P, Freedman DB, Mohiuddin J, Jeremy JY, Weerakoon J. Hyperphosphataemic rickets: a new variant. Br Med J (Clin Res Ed) 1983; 287:1765.
10. Sahota O, Gaynor K , Har wood RH, Hosk ing DJ. Hypovitaminosis D and functional Hypoparathyroidism-the NONOF study. Age and Ageing 2001; 30:467-472.