Embed Size (px)
Citation preview

Hyperlipidemia and COPD: 2 Old Problems with New Therapies and Goals Activity Number: 0217-0000-16-116-L01-P 1.50 hours of CPE credit; Activity Type: An Application-Based Activity
Monday, October 24, 2016 9:15 a.m. to 10:45 a.m. Great Hall 3
Moderator: E. Kelly Hester, Pharm. D., FCCP, BCPS Associate Clinical Professor, Department of Pharmacy Practice, Auburn University Harrison School of Pharmacy, Auburn, Alabama
Agenda
9:15 a.m. Is 50 the New 70? Exploring the Value of Intensified LDL reduction with PCSK-9 Inhibitors and Ezetimibe Tran H. Tran, Pharm. D., BCPS Associate Professor, Midwestern University, Chicago College of Pharmacy, Downers Grove, Illinois
10:00 a.m. Update in COPD Pharmacotherapy: Is New Better? Christopher K. Finch, Pharm. D., BCPS Director of Pharmacy, Methodist University Hospital; Associate Professor, University of Tennessee College of Pharmacy, Memphis, Tennessee
Conflict of Interest Disclosures
Christopher K. Finch: no conflicts to disclose E. Kelly Hester: no conflicts to discloseTran H. Tran: no conflicts to disclose
Learning Objectives 1. Explain the relationship between serum LDL level and residual cardiovascular diseases.2. Evaluate the literature describing the use of the PSCK-9 inhibitors for reducing cardiovascular disease.3. Interpret the literature pertaining the use of ezetimibe for reducing cardiovascular disease.4. Construct an evidence-based pharmacotherapy regimen for reducing residual cardiovascular disease in
at risk patients.5. Compare and contrast the pharmacological and cost differences with new therapy options for COPD
compared to older medications.6. Discuss the evidence-based outcomes of newer pharmacologic options based on clinical trials
compared to older medications.7. Explain the role of new agents in the medical management of COPD.
Self-Assessment Questions
Self-assessment questions are available online at www.accp.com/am
© American College of Clinical Pharmacy 1

2016 ACCP Annual Meeting
Is 50 the new 70? Exploring the value of intensified LDL reduction with PCSK‐9 inhibitors and ezetimibe
Tran H. Tran, Pharm. D., BCPSAssociate Professor
Midwestern University Chicago College of Pharmacy
Downer’s Grove, ILOctober 24, 2016
© American College of Clinical Pharmacy 2

2016 ACCP Annual Meeting
Conflict of Interest
• None to disclose
© American College of Clinical Pharmacy 3

2016 ACCP Annual Meeting
Learning Objectives Explain the relationship between serum LDL level and residual cardiovascular diseases. Evaluate the literature describing the use of the PCSK‐9 inhibitors for reducing cardiovascular disease. Interpret the literature pertaining to the use of ezetimibe for reducing cardiovascular disease.Construct an evidence‐based pharmacotherapy regimen for reducing residual cardiovascular disease in at risk patients.
© American College of Clinical Pharmacy 4

2016 ACCP Annual Meeting
CVD Remains an Area of High Unmet Need• CVD remains the leading cause of death in the US accounting for 1 out of every 7 deaths
• Costs > $320 billion each year
High Morbidity, Mortality, and Cost
• Despite effective treatments like statins, many patients are not achieving optimal LDL‐C levels
Suboptimal LDL Management
• Statin intolerance occurs in ~ 10–20% of patients and commonly results in treatment discontinuationStatin Intolerance
• Beyond statins, existing nonstatin agents provide only modest LDL‐C reduction
Limited Treatment Options
CVD = cardiovascular disease; LDL = low‐density lipoprotein; LDL‐C = LDL‐cholesterol.Mozaffarian D, et al. Circulation. 2015; 131(4):e29‐322; CDC. Heart Disease Facts. www.cdc.gov/heartdisease/facts.htm. Accessed 3/24/15; Go AS, et al. Circulation. 2014;129(3):E28‐E292; Rosenson RS, et al. J Clin Lipidol. 2014;8(3 Suppl):S58‐S71. PRIME®.
© American College of Clinical Pharmacy 5

2016 ACCP Annual Meeting
ACC/AHA 2013 Guidelines: 4 Statin Benefit Groups and Intensity of Statin Therapy
• Age ≤ 75: High‐intensity statin• Age > 75: Moderate‐intensity statin
Secondary Prevention Clinical ASCVD
• High‐intensity statinPrimary PreventionLDL‐C ≥ 190 mg/dL
• Low risk (10‐year risk < 7.5%): Moderate‐intensity statin• High risk (10‐year risk ≥ 7.5%): High‐intensity statin
Primary PreventionAge 40–75 with diabetes and LDL 70–189 mg/dL, no clinical ASCVD
• Consider moderate‐ or high‐intensity statin
Primary Prevention Age 40–75 with no diabetes or
clinical ASCVD, LDL 70–189 mg/dL, estimated 10‐year ASCVD ≥ 7.5%
Stone NJ, et al. Circulation. 2013;129(25 Suppl 2):S1‐S45.
© American College of Clinical Pharmacy 6
2016 ACCP Annual Meeting
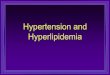
Despite Treatment with High‐Dose Statins, Many Patients Do Not Achieve Goal*
Distribution of Achieved LD
L‐C Levels (%
)
Hazard Ra
tio (H
R; %)
LDL‐C (mg/dL)
10
20
30
020015010050
0
0.50
0.75
1.00
0.25
250
40
*< 70 mg/dLAdapted from: Boekholdt SM, et al. J Am Coll Cardiol. 2014;64(5):485‐494. PRIME®.
LDL‐C levels
Risk of major CV events
On‐Statin LDL‐C Levels and Risk of Major Cardiovascular Events
© American College of Clinical Pharmacy 7

2016 ACCP Annual Meeting
PCSK9 inhibitors
© American College of Clinical Pharmacy 8
2016 ACCP Annual Meeting
Heterozygous FH• Characterized by high LDLC levels (≥ 190 mg/dL)• Primarily caused by mutations in LDL‐R gene, as well as in APOB or PCSK9 genes
• Believed to occur in one in every 200 individuals• Leads to 10‐ to 20‐fold lifetime increased risk of heart attack
• Men with HeFH have a 50% chance of a heart attack by age 50 without treatment and in women there’s a 30% chance by age 60
HeFH = heterozygous familial hypercholesterolemia, LDLC = LDL cholesterol, LDL‐R = LDL‐receptor.
© American College of Clinical Pharmacy 9
2016 ACCP Annual Meeting
PCSK9: A Compelling New Hypercholesterolemia Target
• The key role of PCSK9 in LDL‐C metabolism:
• Promotes intracellular degradation of hepatic LDL‐R
• Prevents LDL‐R recycling to cell surface
• Reduces LDL‐R population on cell surface
• Reduces LDL clearance from circulation
LDL‐R = LDL‐receptor.Lambert G, et al. J Lipid Res. 2012;53(12):2515‐2524.
© American College of Clinical Pharmacy 10
2016 ACCP Annual Meeting
Role of PCSK9 in Regulation of LDL‐R Expression
© American College of Clinical Pharmacy 11

2016 ACCP Annual Meeting
FDA Approved PCSK9 Inhibitors:Alirocumab Evolocumab
IndicationPatients with HeFH or clinical atherosclerotic CVD
In addition to diet and maximally tolerated statin therapy
Dosage and administration
• Two different doses: 75 mg or 150 mg dose every 2 weeks
• Available in a single 1 mL SQ injection delivered in a single‐dose prefilled pen or syringe that patients self‐administer
• Two different doses: 140 mg dose every 2 weeks or 420 mg dose every month
• Available in a single prefilled SQ autoinjector or on‐body infusor with prefilled cartridge
HeFH = heterozygous familial hypercholesterolemia, CVD = cardiovascular diseaseFDA News Release. FDA approves Praluent to treat certain patients with high cholesterol. Released July 24, 2015. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm455883.htm
© American College of Clinical Pharmacy 12

2016 ACCP Annual Meeting
Alirocumab: ODYSSEY Trial ProgramType of Study Trial Name N Duration (weeks)
Moderate CV Risk MONO 103 24
Statin Intolerant ALTERNATIVE 314 24
High LDL‐C
High CV Risk
CHOICE II*
CHOICE I*
OPTIONS I
OPTIONS II
COMBO I
COMBO II
LONGTERM
803
233
355
305
316
720
2,341
24
24
52
104
52
24
78
HeFHFH I
FH II
High FH
471
250
105
78
78
78
High CV Risk
Recent CV EventOUTCOMES 18,000 5–6 years Ongoing
Plus max statin dose
Not receiving statins
Moderate statin dose
*CHOICE I & II evaluated alirocumab every 2 weeks and monthly.; PRIME®.
© American College of Clinical Pharmacy 13

2016 ACCP Annual Meeting
Alirocumab: ODYSSEY LONGTERM Study Design
Placebo SC Q2W
R
W4 W12 W24 W52 W64 W78
W0 W8 W16 W36Assessments
Double‐Blind Treatment (18 months)Follow‐up (8 weeks)
Primary efficacy endpoint
Pre‐specified analysisEfficacy endpoints: All patients up to W52 on the ITT analysis and population Safety analysis: All patients randomized and treated whatever the duration of exposure
N = 1,553
N = 788
Robinson JG, et al. N Engl J Med. 2015;372(16):1489‐1499.; PRIME®.
HeFH or high CV risk patients on maximally tolerated statin +/‐other lipid‐lowering
therapyLDL‐C ≥ 70 mg/dL
Alirocumab 150 mg SC Q2W Administered via single 1 mL injection using prefilled pen for self‐injection
© American College of Clinical Pharmacy 14

2016 ACCP Annual Meeting
Alirocumab (ODYSSEY LONGTERM) Calculated LDL‐C Levels Over Time (ITT)
Least‐Squa
res M
ean Ca
lculated
LDL‐C Level (mg/dL)
Time (weeks)4 8 12 16 24 52 64 78
20
40
60
80
100
120
140
0.00
0.60
1.20
2.40
3.00
3.60
1.80
‐52.4%*
57.9 mg/dL (1.50 mmol/liter)
122.6 mg/dL (3.17 mmol/liter)
48.3 mg/dL (1.25 mmol/liter)
Placebo + statin therapy at maximum tolerated dose +/‐ LLTAlirocumab + statin therapy at maximum tolerated dose +/‐ LLT
(mmol/liter)
3600
*P < 0.001 LLT = lipid‐lowering therapy. Robinson JG, et al. N Engl J Med. 2015;372(16):1489‐1499; PRIME®.
118.9 mg/dL (3.08 mmol/liter)
‐0.8%
‐61.0%*
‐3.6%
© American College of Clinical Pharmacy 15

2016 ACCP Annual Meeting
Alirocumab (ODYSSEY LONGTERM) Safety Analysis
Summary of AEsAlirocumab(n = 1,550)
Placebo(n = 788) P Value
SAEs 290 (18.7%) 154 (19.5%) 0.66
AE leading to discontinuation 111 (7.2%) 46 (5.8%) 0.26
AE leading to death 8 (0.5%) 10 (1.3%) 0.08
General allergic reaction events 156 (0.1%) 75 (9.5%) 0.71
Treatment‐related injection site reactions 91 (5.9%) 33 (4.2%) 0.10
Neurologic events 65 (4.2%) 35 (4.4%) 0.83
Neurocognitive events 18 (1.2%) 4 (0.5%) 0.17
Robinson JG, et al. N Engl J Med. 2015;372(16):1489‐1499. PRIME®.
Among patients who received alirocumab, 575 (37.1%) had a calculated LDL‐C level of < 25 mg/dL at 2 consecutive measurements. Rates of AEs were similar to those in the overall alirocumab group.
© American College of Clinical Pharmacy 16

2016 ACCP Annual Meeting
Alirocumab (ODYSSEY LONGTERM)Safety Analysis: Cardiovascular Adverse EventsCardiovascular AE Alirocumab
(n = 1,550)Placebo(n = 788) P Value
CHD death 4 (0.3%) 7 (0.9%) 0.26
Non‐fatal MI 14 (0.9%) 18 (2.3%) 0.01
Fatal + non‐fatal ischemic stroke 9 (0.6%) 2 (0.3%) 0.35
Unstable angina requiring hospitalization 0 1 (0.1%) 0.34
Positively adjudicated CV events, including all those listed above 72 (4.6%) 40 (5.1%) 0.68
Adjudicated major AEs in post‐hoc analysis* 27 (1.7%) 26 (3.3%) 0.02
*The post‐hoc analysis was not specified in the study protocol. It included the following CV event categories, which also form the endpoint for the ODYSSEY OUTCOMES study: Death from CHD, non‐fatal MI, fatal and non‐fatal ischemic stroke, and unstable angina requiringhospitalization. “Unstable angina requiring hospitalization” is limited to the unstable angina events with definite evidence of progression of the ischemic condition (strict criteria). Robinson JG, et al. N Engl J Med. 2015;372(16):1489‐1499; PRIME®.
© American College of Clinical Pharmacy 17
2016 ACCP Annual Meeting
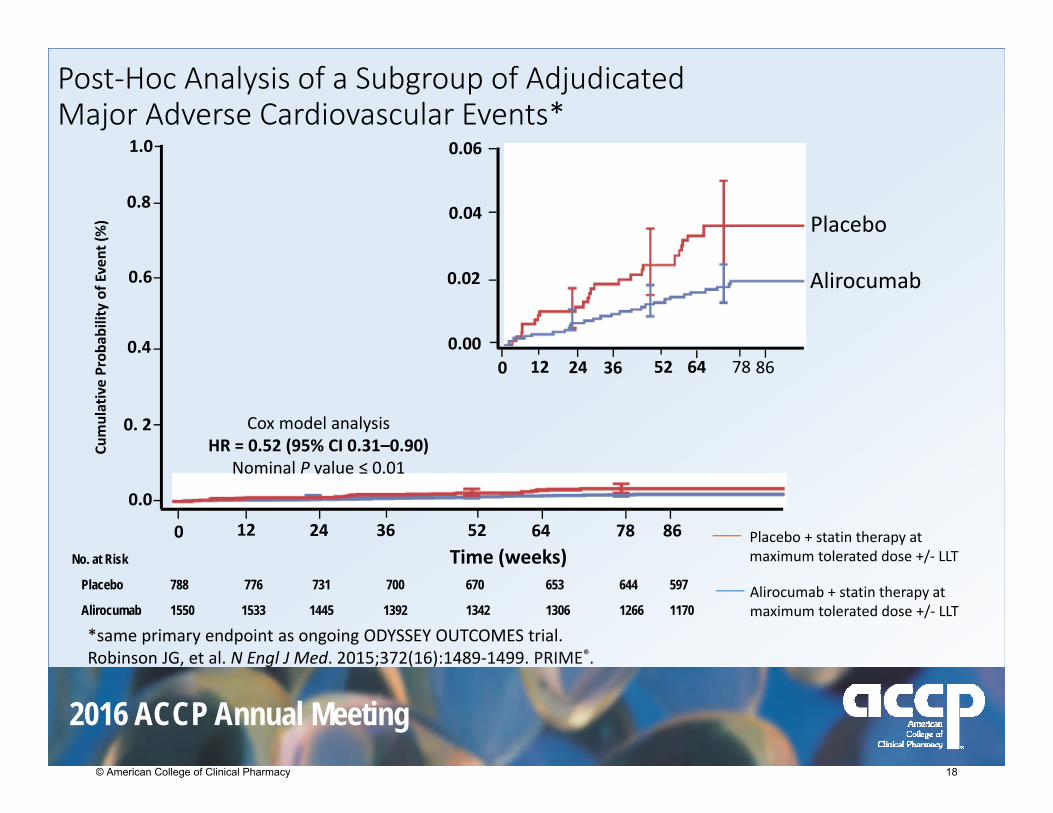
Post‐Hoc Analysis of a Subgroup of Adjudicated Major Adverse Cardiovascular Events*
0.00
0.02
0.04
0.06
0 12 24 52 64 78 8636
0.6
0.4
0. 2
0.8
1.0
0.0
0 12 24 36 52 64 78 86
Cumulative Prob
ability of Event (%
)
Time (weeks)
Cox model analysis HR = 0.52 (95% CI 0.31–0.90)
Nominal P value ≤ 0.01
*same primary endpoint as ongoing ODYSSEY OUTCOMES trial.Robinson JG, et al. N Engl J Med. 2015;372(16):1489‐1499. PRIME®.
No. at Risk
Placebo 788 776 731 700 670 653 644 597
Alirocumab 1550 1533 1445 1392 1342 1306 1266 1170
Placebo + statin therapy at maximum tolerated dose +/‐ LLT
Alirocumab + statin therapy at maximum tolerated dose +/‐ LLT
Placebo
Alirocumab
© American College of Clinical Pharmacy 18

2016 ACCP Annual Meeting
Evolocumab: Select Trials from the PROFICIO Clinical Trial Program*
Type of Study Trial Name N Duration(weeks)
Monotherapy MENDEL‐2 614 12
Statin IntolerantGAUSS‐2GAUSS‐3
307500;100
12
24 Ongoing
Combination Therapy LAPLACE‐2 1,896 12
High CV Risk DESCARTES 901 52
GLAGOV 950 78 Ongoing
FHRUTHERFORD‐2 (HeFH)
TESLA (HoFH)
TAUSSIG
329
58
250
12
12
5 years Ongoing
Established CVD FOURIER 22,500 5 years Ongoing
Not Receiving Statins
Receiving Statin Therapy
*Evaluated evolocumab every 2 weeks and monthly.PRIME®.
© American College of Clinical Pharmacy 19

2016 ACCP Annual Meeting
Evolocumab: Open‐Label Studies of Long‐Term Evaluation Against (OSLER‐1 and OSLER‐2)
Standard of Care Alone
(n = 1,489)
Evolocumab + Standard of Care
(n = 2,976)
MENDEL‐1 (n = 406)
MENDEL‐2 (n = 614)
Phase 2 trials
Phase 3 trialsTHOMAS‐1(n = 149)
THOMAS‐2(n = 164)
LAPLACE‐TIMI 57 (n = 629)
LAPLACE‐2 (n = 1,896)
GAUSS‐2(n = 307)
GAUSS‐1(n = 157)
RUTHERFORD‐1(n = 167)
RUTHERFORD‐2(n = 329)
YUKAWA‐1(n = 307)
DESCARTES(n = 901)
Sabatine MS, et al. N Engl J Med. 2015;372(16):1500‐1509. PRIME®.
4,465 patients (74%) elected to enroll into OSLER extension study program1,324 from phase 2 trials into OSLER‐13,141 from phase 3 trials into OSLER‐2
Eligible if medically stable and on study drug
Randomized 2:1
Irrespective of treatment assignment in parent study
© American College of Clinical Pharmacy 20

2016 ACCP Annual Meeting
Evolocumab (OSLER‐1 and OSLER‐2): LDL‐C Levels Over Time
No. at Risk
Standard therapy 1489 394 1388 1376 402 1219
Evolocumab 2976 864 2871 2828 841 2508
Absolute reduction (mg/dL) 60.4 73.4 70.4 72.7 70.5
Percentage reduction 56.3 60.9 58.8 54.0 58.4
P value < 0.001 < 0.001 < 0.001 < 0.001 < 0.001
Baseline 4 12 24 36 48
Evolocumab + Standard of Care
Standard of Care
20
40
60
80
100
120
140LD
L‐C (m
g/dL)
0
Time (weeks)
Sabatine MS, et al. N Engl J Med. 2015;372(16):1500‐1509. PRIME®.
© American College of Clinical Pharmacy 21
2016 ACCP Annual Meeting
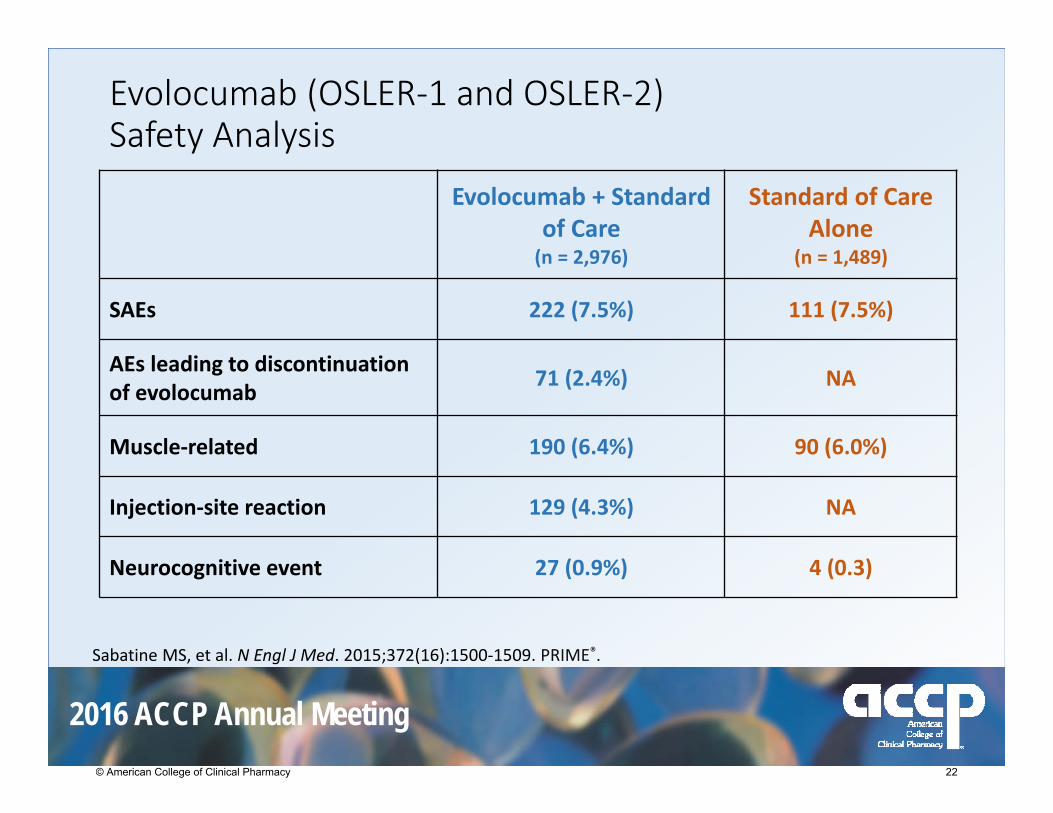
Evolocumab (OSLER‐1 and OSLER‐2)Safety Analysis
Evolocumab + Standard of Care(n = 2,976)
Standard of CareAlone
(n = 1,489)
SAEs 222 (7.5%) 111 (7.5%)
AEs leading to discontinuation of evolocumab 71 (2.4%) NA
Muscle‐related 190 (6.4%) 90 (6.0%)
Injection‐site reaction 129 (4.3%) NA
Neurocognitive event 27 (0.9%) 4 (0.3)
Sabatine MS, et al. N Engl J Med. 2015;372(16):1500‐1509. PRIME®.
© American College of Clinical Pharmacy 22

2016 ACCP Annual Meeting
Evolocumab (OSLER‐1 and OSLER‐2)Patient Incidence of Cardiovascular Clinical Events
Endpoint
Evolocumab +Standard Therapy
(n = 2,976)
Standard TherapyAlone
(n = 1,489)
HR (95% CI)
All CV events 29 (0.95%) 31 (2.18%) 0.47 (0.28–0.78)
Death 4 (0.14%) 6 (0.41%) 0.33(0.09–1.18)
Coronary events(MI, hospitalization for unstable angina, coronary revascularization)
22 (0.75%) 18 (1.30%) 0.61(0.33–1.14)
Cerebrovascular events (stroke or TIA) 4 (0.14%) 7 (0.47%) 0.29
(0.08–0.98)
Heart failure requiring hospitalization 1 (0.03%) 1 (0.07%) 0.52
(0.03–8.30)Sabatine MS, et al. N Engl J Med. 2015;372(16):1500‐1509. PRIME®.
© American College of Clinical Pharmacy 23

2016 ACCP Annual Meeting
Evolocumab (OSLER‐1 and OSLER‐2)Cumulative Incidence of Cardiovascular Events
Sabatine MS, et al. N Engl J Med. 2015;372(16):1500‐1509. PRIME®.
© American College of Clinical Pharmacy 24

2016 ACCP Annual Meeting
LDL‐C reduction with PCSK9 inhibitors• Long‐term effects of very low levels of LDL‐C induced by PCSK9 inhibitors are unknown
• Effect on cardiovascular morbidity and mortality has not been determined.
• Potential for immunogenicity• Safety and effectiveness not established in pediatric patients with primary hyperlipidemia or HeFH
LDL‐C = low density lipoprotein cholesterol; HeFH = heterozygous familial hypercholesterolemia
© American College of Clinical Pharmacy 25

2016 ACCP Annual Meeting
LDL‐C reduction a reliable surrogate for cardiovascular outcomes?
• Statin approvals based on the LDL cholesterol surrogate (1987)
• Ezetimibe approval based on LDL cholesterol surrogate (2002)
• Nonstatin trials did not support correlation • ILLUMINATE study• HPS2‐THRIVE
© American College of Clinical Pharmacy 26

2016 ACCP Annual Meeting
What Can We Learn from IMPROVE‐IT?Ezetimibe/Simvastatin vs Simvastatin
© American College of Clinical Pharmacy 27

2016 ACCP Annual Meeting
IMPROVE‐IT: Ezetimibe/Simvastatin vs Simvastatin• Large scale (N = 18,144) RCT of high‐risk post‐ACS patients
• Intervention: Ezetimibe 10 mg added to simvastatin 40 mg• Comparator: Simvastatin 40 mg
• Simvastatin dose uptitrated to 80 mg in patients with LDL‐C > 79 mg/dL
• 27% in simvastatin group and 6% in ezetimibe/simvastatin group
• Primary endpoint: • Composite of cardiovascular death, MI, unstable angina requiring hospitaliziation, coronary revascularization, or stroke
• Study took 9 years; follow‐up was 7 years
ACS = acute coronary syndrome. Cannon CP, et al. N Engl J Med 2015;372(25):2387‐2397. PRIME®.
© American College of Clinical Pharmacy 28

2016 ACCP Annual Meeting
IMPROVE‐IT: LDL‐C and Lipid Changes
QE 1R 9648 60 72 84124 8 2416 36
40
50
60
70
80
90
100
Mean LD
L‐C (m
g/dL)
Median Time avg69.5 vs 53.7 mg/dL
1‐yr Mean LDL‐C TC TG HDL hsCRP
Simvastatin 69.9 145.1 137.1 48.1 3.8
EZ/Simva 53.2 125.8 120.4 48.7 3.3
∆ in mg/dL ‐16.7 ‐19.3 ‐16.7 +0.6 ‐0.5
Time Since Randomization (months)
TC = total cholesterol; TG = triglycerides; hsCRP = high sensitivity C‐reactive protein. Cannon CP, et al. N Engl J Med 2015;372(25):2387‐2397. PRIME®.
Ezetimibe/SimvastatinSimvastatin
© American College of Clinical Pharmacy 29

2016 ACCP Annual Meeting
IMPROVE‐IT: Results for Primary Endpoint*
32.7%34.7%
0%
10%
20%
30%
40%
50%% Sub
jects who
Experienced
an Even
t2% Absolute Risk Reduction
*The primary composite endpoint was CV death, nonfatal myocardial infarction (MI), nonfatal stroke, rehospitalization for unstable angina (UA), and coronary revascularization (≥ 30 days postrandomization). Cannon CP, et al. N Engl J Med 2015;372(25):2387‐2397. PRIME®.
HR = 0.936P = 0.016NNT = 50
Simvastatin 40 mg (n = 9,077)
Ezetimibe 10 mg / Simvastatin 40 mg
(n = 9,067)
2,572 events 2,742 events
© American College of Clinical Pharmacy 30

2016 ACCP Annual Meeting
IMPROVE‐IT: Individual Primary and Secondary Endpoints (7‐year event rates)
Clinical OutcomesSimvastatin n = 9,077 (%)
Ezetimibe/Simvastatin n = 9,067 (%) P Value
All‐cause death 15.3 15.4 0.782
MI 14.8 13.1 0.002
Stroke 4.8 4.2 0.052
Ischemic stroke 4.1 3.4 0.008
Unstable angina 1.9 2.1 0.618
Coronary revascularization 23.4 21.8 0.107
Cannon CP, et al. N Engl J Med 2015;372(25):2387‐2397. PRIME®.
© American College of Clinical Pharmacy 31

2016 ACCP Annual Meeting
Key Takeaways from IMPROVE‐IT• Addition of a nonstatin (ezetimibe) to a moderate dose statin may lower cardiovascular event risk
• Reaffirms “lower is better” with proven risk‐reducing therapies
• Confirms safety profile of ezetimibe • No differences observed in cancer or muscle, or gallbladder‐related events
• Questions remain: • What is the optimal LDL?• How low to go?• Should guidelines be changed?
Cannon CP, et al. N Engl J Med 2015;372(25):2387‐2397. PRIME®.
© American College of Clinical Pharmacy 32

2016 ACCP Annual Meeting
Patient Case #1
• Man followed in lipid clinic for multiple decades
• PMH: HeFH, known CAD• FH: 2 brothers dying from cardiovascular causes in their 20s.
• SH: highly motivated, getting lots of exercise, trying to eat the right foods, taking 4 lipid‐lowering medications (maximum statin therapy as well as other LDL‐lowering medications )
• Despite that his LDL‐C level is 150 mg/dL
Would you consider a PCSK‐9 inhibitor in this patient?
© American College of Clinical Pharmacy 33

2016 ACCP Annual Meeting
Patient Case #2
• 40 YO Male • LDL of 110 mg/dL after maximally tolerated statin
• Recurrent CV events with multiple stents
Would you consider a PCSK‐9 inhibitor in this patient?
© American College of Clinical Pharmacy 34

2016 ACCP Annual Meeting
PCSK9 inhibitors: Sticker Shock • Evolocumab costs $14,100 per year• Alirocumab costs $14,600 per year• In Europe, PCSK9 inhibitors cost ~ $6,800 USD per year in the United Kingdom
• Every statin is available as a generic medication at a fraction of that cost
• According to ICER, the PCSK9 inhibitor price would need to come down to $2100 per year to be cost‐effective in FH patients, and to approximately $2,500 per year in the secondary‐prevention setting
Institute for Clinical and Economic Review. PCSK9 inhibitors for treatment of high cholesterol: effectiveness, value, and value‐based price benchmarks draft report. Published September 8, 2015
© American College of Clinical Pharmacy 35

2016 ACCP Annual Meeting
Statin Intolerance• Prevalence of statin‐associated muscle symptoms ranges from 7% to 29%
• In a large retrospective cohort study, 6579 of 11,124 patients who discontinued a statin due to adverse effects were rechallenged, with 92% success in restoring therapy
• Try multiple statins before labeling statin‐intolerant and considering a $14,000 alternative
© American College of Clinical Pharmacy 36
2016 ACCP Annual Meeting
Key Points• Establishing improved cardiovascular outcomes is key.• Ongoing trials are necessary for PCSK 9 inhibitors.• PCSK9 inhibitors are not for patients simply reluctant to take a statin.
• PCSK9 inhibitors are reserved for patients with “high” LDL cholesterol levels despite maximal therapy with statins and ezetimibe.
© American College of Clinical Pharmacy 37

2016 ACCP Annual Meeting
QUESTIONS
Thank You
Tran H. Tran, PharmD
© American College of Clinical Pharmacy 38

2016 ACCP Annual Meeting
REFERENCES• Mozaffarian D, et al. Circulation. 2015; 131(4):e29‐322; CDC. Heart Disease Facts.
www.cdc.gov/heartdisease/facts.htm. Accessed 3/24/15.
• Go AS, et al. Circulation. 2014;129(3):E28‐E292; Rosenson RS, et al. J Clin Lipidol. 2014;8(3 Suppl):S58‐S71.
• Stone NJ, et al. Circulation. 2013;129(25 Suppl 2):S1‐S45.
• Boekholdt SM, et al. J Am Coll Cardiol. 2014;64(5):485‐494.
• Lambert G, et al. J Lipid Res. 2012;53(12):2515‐2524.
• FDA News Release. FDA approves Praluent to treat certain patients with high cholesterol. Released July 24, 2015. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm455883.htm
• Robinson JG, et al. N Engl J Med. 2015;372(16):1489‐1499.
• Sabatine MS, et al. N Engl J Med. 2015;372(16):1500‐1509.
• Cannon CP, et al. N Engl J Med 2015;372(25):2387‐2397.
• Institute for Clinical and Economic Review. PCSK9 inhibitors for treatment of high cholesterol: effectiveness, value, and value‐based price benchmarks draft report. Published September 8, 2015
© American College of Clinical Pharmacy 39

2016 ACCP Annual Meeting
Christopher K. Finch, Pharm.D., BCPS, FCCM, FCCPDirector of Pharmacy
Methodist University HospitalAssociate Professor
University of Tennessee, College of PharmacyMemphis, TN
October 24, 2016
Update in COPD Pharmacotherapy: Is New Better?
© American College of Clinical Pharmacy 40
2016 ACCP Annual Meeting
Conflict of Interest
• I have no conflicts of interest to disclose.
© American College of Clinical Pharmacy 41

2016 ACCP Annual Meeting
Learning Objectives
• Compare and contrast the pharmacological and cost differences with new therapy options for COPD compared to older medications.
• Discuss the evidence-based outcomes of newer pharmacologic options based on clinical trials compared to older medications.
• Explain the role of new agents in the medical management of COPD.
© American College of Clinical Pharmacy 42

2016 ACCP Annual Meeting
Abbreviations• COPD—chronic obstructive pulmonary
disease
• FEV1—forced expiratory volume in 1 second
• R—randomized
• DD—double dummy
• DB—double blind
• PC—placebo controlled
• PG—parallel group
• CAT—COPD assessment test
• mMRC—modified medical research council dyspnea scale
• GOLD—Global Initiative on Chronic Obstructive Lung Disease
• SABA—short acting beta agonist
• SAMA—short acting muscarinic antagonist
• LABA—long-acting beta agonist
• LAMA—long-acting muscarinic antagonist
• ICS—inhaled corticosteroids
• QoL—quality of life
• AUC—area under the curve
• TDI—transient dyspnea index
• PIFR—peak inspiratory flow rate
© American College of Clinical Pharmacy 43

2016 ACCP Annual Meeting
What is COPD?
A common preventable and treatable disease
Characterized by persistent airflow limitation that is usually progressive
Associated with an enhanced chronic inflammatory response in the airways and the lung
Global Initiative for Chronic Obstructive Lung Disease 2016. http://www.goldcopd.com. Accessed 8/4/16
© American College of Clinical Pharmacy 44

2016 ACCP Annual Meeting
Epidemiology and Burden of COPD
• 24 million Americans have COPD; half don’t know it• 4th leading cause of death in the world• 2nd to heart disease as a cause of disability
• Approximately 70% of COPD patients are <65 yearsand COPD patients under the age of 65 account for:
• 52% of total hospital outpatient visits for COPD• 63% of emergency department visits for COPD• 33% of COPD Hospitalizations
• Since 2000, female deaths have exceeded male deaths
Mannino DM. Chest. 2002;121:121S-126S. Guarascio AJ et al. Clinicoecon Outcomes Res. 2013;5:235-245.AHRQ Pub No. 02-M016, March 2002. Mannino DM et al. MMWR 2002;51(SS-6):1-16.
© American College of Clinical Pharmacy 45

2016 ACCP Annual Meeting
Significant Burden Associated With Managing COPD
• Each year due to COPD, there are approximately:• 16.3 million office visits• 672,000 hospitalizations
• More than 22% of Medicare patients hospitalized for COPD in 2003–2004 were readmitted within 30 days of discharge; 36% of these readmissions were for COPD
Jencks SF et al. N Engl J Med. 2009;360:1418-1428.
© American College of Clinical Pharmacy 46
2016 ACCP Annual Meeting
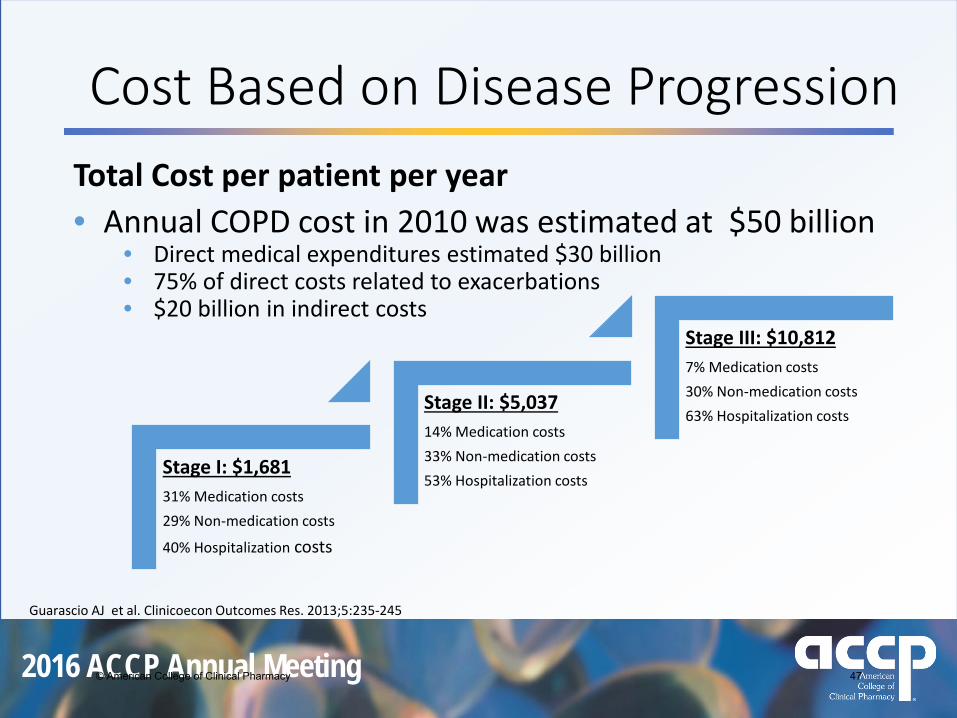
Total Cost per patient per year• Annual COPD cost in 2010 was estimated at $50 billion
• Direct medical expenditures estimated $30 billion• 75% of direct costs related to exacerbations• $20 billion in indirect costs
Cost Based on Disease Progression
Guarascio AJ et al. Clinicoecon Outcomes Res. 2013;5:235-245
Stage I: $1,68131% Medication costs29% Non-medication costs
40% Hospitalization costs
Stage II: $5,037 14% Medication costs33% Non-medication costs53% Hospitalization costs
Stage III: $10,812 7% Medication costs30% Non-medication costs63% Hospitalization costs
© American College of Clinical Pharmacy 47

2016 ACCP Annual Meeting
The Major Risk Factor for COPD
• Cigarette smoking is the most important risk factor for COPD worldwide
• About 15% of smokers will develop COPD but the majority of smokers will develop loss of lung function
• Recommendation from the GOLD Guidelines:• Any current or former smoker over age 40 or never a smoker with a
family history of COPD who complains of dyspnea, chronic cough, or chronic sputum production should seek testing for COPD with spirometry
Global Initiative for Chronic Obstructive Lung Disease. www.goldcopd.com. Accessed July 2016.American Lung Association. www.lungusa.org/lung-disease/copd/resources/facts-figures/COPD-Fact-Sheet.html . Accessed July 2016.
© American College of Clinical Pharmacy 48

2016 ACCP Annual Meeting
Goals of Therapy
Global Initiative for Chronic Obstructive Lung Disease 2016. http://www.goldcopd.com. Accessed 8/4/16
Smoking cessation has the greatest capacity to
influence the natural history of COPD.
Appropriate pharmacologic therapy can reduce COPD symptoms, reduce the frequency and severity of
exacerbations, and improve health status and exercise tolerance.
© American College of Clinical Pharmacy 49

2016 ACCP Annual Meeting
COPD Assessment and Therapeutic Options
Airf
low
Lim
itatio
n(G
OLD
Cla
ssifi
catio
n)FE
V1 <
50%
pre
dict
ed
Risk
(Exa
cerb
atio
n an
d ho
spita
lizat
ion
hist
ory)
≥ 2
1
0Symptoms=CAT > 10
4
3
2
1
ICS + LABAand/orLAMA
Adapted from Global Initiative for Chronic Obstructive Lung Disease 2016. http://www.goldcopd.com. Accessed 8/4/16
A B
C D
SAMA prnor
SABA prn
LAMA or
LABA
ICS + LABAor
LAMA
Breathlessness=mMRC > 2
© American College of Clinical Pharmacy 50
2016 ACCP Annual Meeting
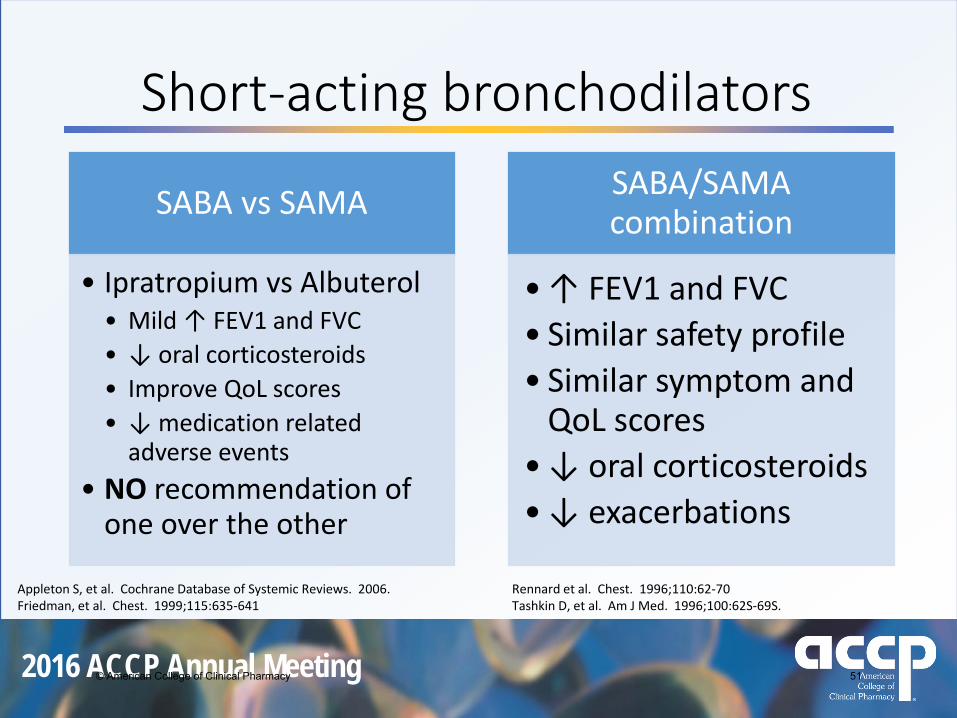
Short-acting bronchodilators
SABA vs SAMA
• Ipratropium vs Albuterol• Mild ↑ FEV1 and FVC• ↓ oral corticosteroids• Improve QoL scores • ↓ medication related
adverse events• NO recommendation of
one over the other
SABA/SAMA combination
• ↑ FEV1 and FVC• Similar safety profile• Similar symptom and
QoL scores• ↓ oral corticosteroids• ↓ exacerbations
Appleton S, et al. Cochrane Database of Systemic Reviews. 2006. Rennard et al. Chest. 1996;110:62-70Friedman, et al. Chest. 1999;115:635-641 Tashkin D, et al. Am J Med. 1996;100:62S-69S.
© American College of Clinical Pharmacy 51

2016 ACCP Annual Meeting
Long-acting bronchodilatorsLong-Acting Beta Agonist
• Salmeterol, Formoterol, Arformoterol• Q 12 hr dosing
• Vs. SABA• Improve compliance• ↑ FEV1 • ↓ symptoms• ↓ exacerbations• ↑ QoL
Long-Acting Muscarinic Antagonist
• Tiotropium• Qday dosing
• Vs. active comparator• UPLIFT Trial• ↑ Lung function and QoL• ↓ Dyspnea, exacerbations, and
hospital days
Mahler DA, et al. Chest. 1999;115:957-965. Brusasco V, et al. Thorax. 2003;58:399-404.Rennard SI, et al. Am J Respir Crit Care Med. 2001;163:1087-1092 Tashkin D, et al. N Engl J Med. 2008;359:1543-54
© American College of Clinical Pharmacy 52

2016 ACCP Annual Meeting
Inhaled Corticosteroids
• None have an indication for COPD as monotherapy• This isn’t asthma!
Copenhagen Euroscope Lung Health II Isolde
Pts / Length (mo) 290 / 36 912 / 36 1116 / 40 751 / 36
Med Budesonide Budesonide Triamcinolone Fluticasone
Baseline FEV1 % predicted 86% 77% 64% 46%
Exacerbations ↔ ↔ ↔ ↓
FEV1 response None None None ↑
FEV1 Decline ↔ ↔ ↔ ↔
Vestbo et al. Lancet. 1999;35:1819. Anthonisen et al. N Engl J Med. 2000;343:1902.Pauwels et al. N Engl J Med. 1999;340:1948. Burge et al. BMJ. 2000;320:1297.
© American College of Clinical Pharmacy 53

2016 ACCP Annual Meeting
ICS/LABA combinationTORCH study
Combination therapy vs LABA• ↑ FEV1• ↑ QoL• ↓ exacerbations• ↑ pneumonia
Type of trial • R,DB,PC of 6112 pts• Baseline FEV1 % predicted-44%
Intervention • Placebo• Fluticasone• Salmeterol• Fluticasone/Salmeterol combo
Primary Endpoint Mortality - ↓ 2.6% vs placebo (p=NS)
Secondary Endpoints • Exacerbations• 25% ↓ vs placebo (NNT=4)• ↓ exacerbations vs. all Tx arm (p<0.05)
• Hospitalizations• 17% ↓ vs placebo (p<0.03)
• FEV1• ↑ FEV1 vs each arm (p<0.05)
• Pneumonia• ↑ risk by 7.3% vs placebo (NNH=14)
Calverley PMA, et al. N Engl J Med 2007;356:775-89.
© American College of Clinical Pharmacy 54

2016 ACCP Annual Meeting
How do we keep up?!!!
• 10 New Drugs in 5 yearsPre-1990Albuterol Ipratropium
1990-2010TiotropiumInhaled SteroidsSalmeterol or FormoterolCombos
2011--Present11 NEW FDA meds since 2011PDE4 inhibitorsUltra LABAOnce daily ICS/LABA comboFour new LAMAFour new LABA/LAMA combos
© American College of Clinical Pharmacy 55

2016 ACCP Annual Meeting
New COPD Products
Phosphodiesterase 4 (PDE-4) inhibitor
Roflumilast—2011
Long-acting beta agonist (LABA)
Indacaterol—2011Olodaterol—2014
Long-acting muscarinic
antagonist (LAMA)Aclidinium—2012
Umeclidinium—2014Glycopyrrolate--2015
Inhaled Corticosteroid/LABA Combination
Fluticasone/vilanterol—2013
LABA/LAMA CombinationUmeclidinium/vilanterol—2013
Glycopyrrolate/indacaterol—2015Tiotropium/olodaterol—2015
Glycopyrrolate/formoterol—2016
© American College of Clinical Pharmacy 56

2016 ACCP Annual Meeting
Phosphodiesterase 4 Inhibitors
© American College of Clinical Pharmacy 57
2016 ACCP Annual Meeting
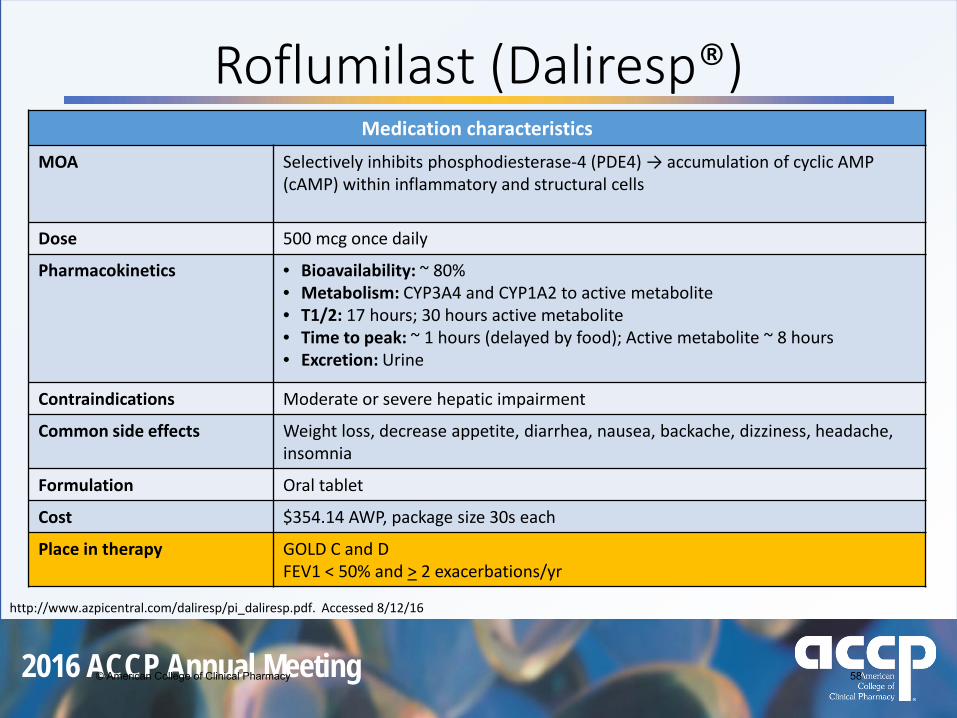
Roflumilast (Daliresp®) Medication characteristics
MOA Selectively inhibits phosphodiesterase-4 (PDE4) → accumulation of cyclic AMP (cAMP) within inflammatory and structural cells
Dose 500 mcg once daily
Pharmacokinetics • Bioavailability: ~ 80%• Metabolism: CYP3A4 and CYP1A2 to active metabolite• T1/2: 17 hours; 30 hours active metabolite• Time to peak: ~ 1 hours (delayed by food); Active metabolite ~ 8 hours • Excretion: Urine
Contraindications Moderate or severe hepatic impairment
Common side effects Weight loss, decrease appetite, diarrhea, nausea, backache, dizziness, headache, insomnia
Formulation Oral tablet
Cost $354.14 AWP, package size 30s each
Place in therapy GOLD C and DFEV1 < 50% and > 2 exacerbations/yr
http://www.azpicentral.com/daliresp/pi_daliresp.pdf. Accessed 8/12/16
© American College of Clinical Pharmacy 58

2016 ACCP Annual Meeting
Roflumilast vs Placebo• Replicate, R,DB, PC, PG x 56 weeks• Patients:
• Age > 40 with exacerbation within the past year• FEV1 % predicted < 50%• n=3091
Trial Outcomes Roflumilast Placebo Change p Value
M2-124Δ in Trough FEV1 at 56wks (mL)
45 8 37 p<0.0003
Exacerbations perpatient/year
1.08 1.27 15% p<0.0278
M2-125Δ in Trough FEV1 at 56wks (mL)
33 -25 58 p<0.05
Exacerbations perpatient/yr
1.2 1.5 18% p<0.05
Calverley PM et al. Lancet. 2009 Aug 29;374(9691):685-94.
© American College of Clinical Pharmacy 59

2016 ACCP Annual Meeting
Long-acting Beta Agonists
© American College of Clinical Pharmacy 60

2016 ACCP Annual Meeting
Indacaterol (Arcapta™ Neohaler™)Medication characteristics
MOA Ultra-LABA
Dose 75 mcg inhaled once daily
Pharmacokinetics Metabolism: CYP3A4, CYP2D6, and CYP1A1T1/2: 40-56 hours Time to peak: ~15 minutes Excretion: Feces and urine
Contraindications Hypersensitivity to indacaterol or any component of the formulation
Common side effects Cough, headache, nausea, nasopharyngitis, oropharyngeal pain
Formulation Capsule, inhalation - PIFR of 52-133 L/min
Cost $256.33 AWP, package side 30s each
Place in therapy Monotherapy GOLD BCombination therapy in GOLD C and D
https://www.pharma.us.novartis.com/sites/www.pharma.us.novartis.com/files/arcapta.pdf. Accessed 8/13/16
© American College of Clinical Pharmacy 61

2016 ACCP Annual Meeting
Indacaterol vs Placebo or Twice Daily LABA
Clinical Trial Data
Indacaterol vs Placebo Indacaterol vs BID LABAType of trial Six randomized, double blinded placebo controlled
trial Meta-analysis of 4 studiesIndacaterol daily vs BID LABA’s for > 24 wks
Patients 5,474 patients with COPD• ≥ 40 years of age• History of smoking at least 10 pack years • FEV1 of at least 30% and less than 80% of
predicted
4708 patients with COPD• ≥ 40 years of age• History of smoking at least 10 pack years • FEV1 of at least 30% and less than 80% of
predicted
Outcomes • Significantly greater 24-hour post-dose trough FEV1 vs placebo
• ↑ Trough FEV1 by > 120 mL (p<0.05)• Reduced exacerbations by 31% vs
placebo
Improved:• Trough FEV1 73 mL (p<0.05)• Dyspnea 0.54 via TDI (p<0.05)No difference in:• Peak FEV1• QoL scores• Exacerbations or Mortality• Adverse effects
Kerwin EM et al. Clin Ther. 2011;33:1974. Geake JB et al. Cochrane Database of Systematic Reviews 2015, Issue 1. Art. No.: CD010139Wedzicha JA et al. Respir Med. 2015 Jan;109(1):105-11.
© American College of Clinical Pharmacy 62

2016 ACCP Annual Meeting
Indacaterol vs TiotropiumLABA vs LAMA – 14 Days
Type of trial Randomized, DB, PC, DD, crossover (n=169)
Intervention Indacaterol vs Tiotropium
Outcomes Indacaterol was at least as effective as tiotropium with a faster onset
Day 1 and 14: Both treatments with Indacaterol resulted in statistically superior FEV1 to Tio p < 0.001
LABA vs LAMA – 6 Month Duration
Type of trial R, PG study
Patients 1422 pts in GOLD A or B
Intervention Indacaterol vs Tiotropium
Outcomes ↑FEV1 30 mL; ↓ rescue SABA; dyspnea↑QoL (All p<0.05)
Vogelmeier et al. Respir Res. 2010;5(11):135.Mahler DA et al. Respir Med. 2015; 109(8);1031-1039.
© American College of Clinical Pharmacy 63

2016 ACCP Annual Meeting
Medication characteristicsMOA Long-acting Beta Agonist
Dose Two inhalations once daily (2.5 mcg/actuation)
Pharmacokinetics Bioavailability: 30%Metabolism: Direct glucuronidation and O-demethylation t1/2: 7.5 hoursTime to peak: 10-20 minutesExcretion: Feces and urine
Contraindications Patients with asthma not taking a long-term controller medication
Common side effects nasopharyngitis, skin rash, UTI, back pain, bronchitis
Formulation Aerosol Solution, inhalation
Cost $155.70 AWP
Place in therapy Monotherapy GOLD BCombination therapy in GOLD C and D
Olodaterol (Striverdi™ Respimat®)
https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/203108s000lbl.pdf. Accessed 8/13/16
© American College of Clinical Pharmacy 64
2016 ACCP Annual Meeting
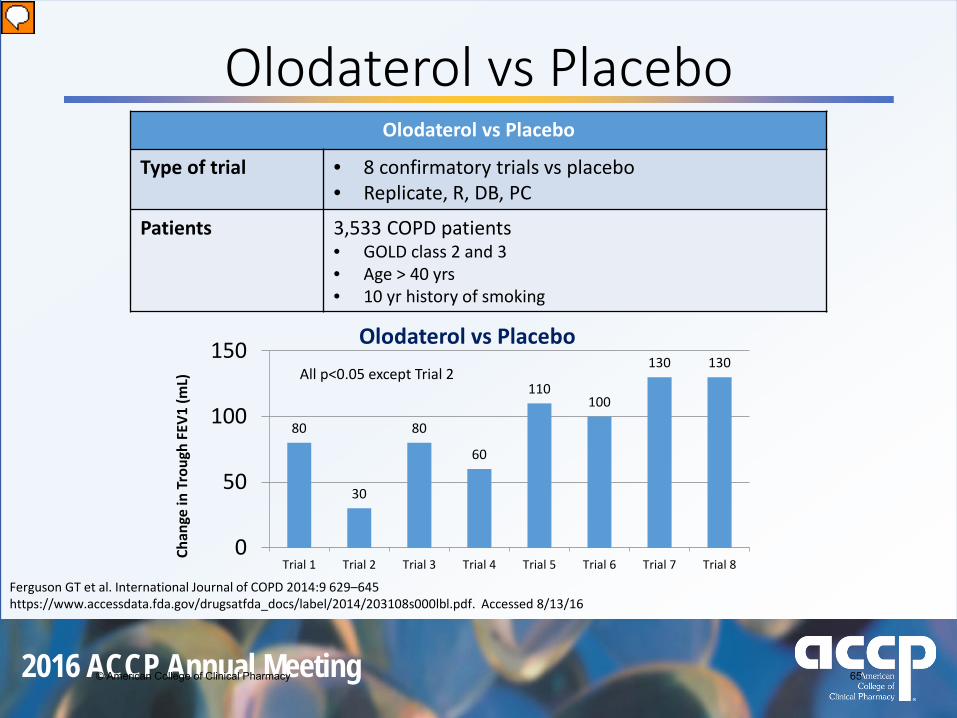
Olodaterol vs Placebo
80
30
80
60
110100
130 130
0
50
100
150
Trial 1 Trial 2 Trial 3 Trial 4 Trial 5 Trial 6 Trial 7 Trial 8
Chan
ge in
Tro
ugh
FEV1
(mL)
Olodaterol vs Placebo
Olodaterol vs Placebo
Type of trial • 8 confirmatory trials vs placebo• Replicate, R, DB, PC
Patients 3,533 COPD patients • GOLD class 2 and 3• Age > 40 yrs• 10 yr history of smoking
All p<0.05 except Trial 2
Ferguson GT et al. International Journal of COPD 2014:9 629–645https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/203108s000lbl.pdf. Accessed 8/13/16
© American College of Clinical Pharmacy 65

2016 ACCP Annual Meeting
Olodaterol vs Formoterol or Tiotropium
131
153123
164
0
50
100
150
200
Trial 7(n=397)
Trial 8(n=439)
mL
Olodaterol5 mcg
Tiotropium5 mcg
p=NSp=NS
Koch A. et al. Int J COPD 2014:9 697–714. Lange P et al. J Pulm Respir Med 2014;4: 196
Olodaterol Formoterol
Trial 5 (n=906)
78 mL* 54 mL*
Trial 6 (n=937)
53 mL* 42 mL*
Olodaterol vs Formoterol Olodaterol vs TiotropiumType of Trial Two R, DB, DD trials Two R, DB trials
Intervention vs Formoterol 12mcg BID vs Tiotropium
Outcomes Change in Trough FEV1 from baselineSimilar profiles for all other metrics
Change in FEV1 AUC 12-24
*p<0.05 vs placebo
© American College of Clinical Pharmacy 66

2016 ACCP Annual Meeting
Long-acting AntimuscarincAntagonists
© American College of Clinical Pharmacy 67

2016 ACCP Annual Meeting
Medication characteristicsMOA Long-acting muscarinic antagonist
Dose 1 inhalation twice daily (400 mcg/actuation)
Pharmacokinetics Metabolism: Hydrolysis t1/2: 5-8 hoursTime to peak: within 10 minutes Excretion: Urine
Contraindications Severe hypersensitivity to milk proteins, aclidinium, or any of the excipients
Common side effects Headache, diarrhea, nasopharyngitis, cough
Formulation Aerosol power breath activated, inhalationMinimal PIFR of 35 L/min
Cost $301.10 AWP
Place in therapy Monotherapy GOLD BCombination therapy in GOLD C prior to steroids
Aclidinium (Tudorza® Pressair®)
http://www.azpicentral.com/tudorza/tudorza_pi.pdf. Accessed 8/13/16
© American College of Clinical Pharmacy 68

2016 ACCP Annual Meeting
Aclidinium vs Placebo
12472
128
0
50
100
150
ACCORD 1 ACCORD 2 ATTAIN
mL
Difference in Trough FEV1 vs Placebo
Kerwin EM et al. COPD. 2012;9:90-101. Rennard SI et al. Clin Drug Investig. 2013;33:893-904.Jones PW et al. Eur Respir J. 2012;40:830-836.
Aclidinium study
Type of Trial Randomized, double blind, placebo controlled
Patients 1,933 subjects with COPD• ≥ 40 years of age• History of smoking at least 10 pack
years • FEV1 of at least 30% and less than 80%
predicted FEV1/FVC of less than 0.7
Outcomes • Improvement in FEV1• ↓ rescue SABA use
All values p<0.05 vs placebo
© American College of Clinical Pharmacy 69

2016 ACCP Annual Meeting
Aclidinium vs Tiotropium
163 14399 107
0
50
100
150
200
Day 1 Day 15
Chan
ge in
mor
ning
trou
gh
FEV 1
from
bas
elin
e (m
L)
Aclid (n=29)
Tio (n=28)
p=NS p=NS
Fuhr et al. CHEST. 2012; 141(3):745-752
Aclidinium vs Active ComparatorType of Trial Randomized, DB, DD, PC, crossover
Intervention Aclidinium BID, Tio QD, placebo15 days
Outcomes Improvements in 24-h bronchodilation were comparable to Tiotropium
© American College of Clinical Pharmacy 70

2016 ACCP Annual Meeting
Medication characteristicsMOA Long-acting muscarinic antagonist
Dose 1 inhalation once daily (62.5 mcg/actuation)
Pharmacokinetics Metabolism: CYP2D6t1/2: 11 hours Time to peak: 5 – 15 minutes Excretion: Feces and urine
Contraindications Severe hypersensitivity to milk proteins or any component
Common side effects Tachycardia, nasopharyngitis, upper respiratory tract infection, cough
Formulation Aerosol power breath activated, inhalationMinimal PIFR of 35 L/min
Cost $252.60 AWP
Place in therapy Monotherapy GOLD BCombination therapy in GOLD C prior to steroids
Umeclidinium (Incruse® Ellipta®)
https://www.gsksource.com/Prescribing_Information/Incruse_Ellipta/pdf/INCRUSE-ELLIPTA-PI-PIL.PDF. Accessed 8/13/16
© American College of Clinical Pharmacy 71

2016 ACCP Annual Meeting
Umeclidinium vs PlaceboUmeclidinium studies
Type of trial Randomized, double-blind, placebo controlled, parallel group trials• 24-week placebo controlled trial • 12 week placebo controlled trial
Patients n=1,738 pts• 10 yr history of smoking• FEV1 < 70% predicted• FEV1/FVC < 0.70
Outcomes • Mean ↑ in Trough FEV1 of 127 mL (p<0.05)• QoL scores improved 30%
Trivedi R et al. Eur Respir J. 2014;43:72–81https://www.gsksource.com/Prescribing_Information/Incruse_Ellipta/pdf/INCRUSE-ELLIPTA-PI-PIL.PDF. Accessed 8/13/16
© American College of Clinical Pharmacy 72

2016 ACCP Annual Meeting
Umeclidinium vs other LAMA’s
95154
123 99
050
100150200
Tio/Umec(n=1017)
Umec/Glyc(n=1034)
ΔTr
ough
FEV
1 (m
L) fr
om
base
line
Tiotropium 18 mcg Qday
Umeclidinium 62.5 mcg Qday
Glycopyrronium 44mcg Qday
p<0.001
Feldman et al. Int J Chron Obstruct Pulmon Dis. 2016. 7;11:719-30https://clinicaltrials.gov/ct2/show/study/NCT02236611?sect=X70156. Accessed 8/11/16
p=NS
Umeclidinium vs Tiotropium Umeclidinium vs Glycopyrronium
Type of trial R, B, DD, PG x 12 wks R, Open label, PG x 12 wks
Patients • Age > 40• GOLD 2 and 3 with mMRC > 2
• Age > 40• GOLD 2 and 3 with mMRC > 2
© American College of Clinical Pharmacy 73

2016 ACCP Annual Meeting
Glycopyrrolate (Seebri™ Neohaler®)Medication characteristics
MOA Long-acting muscarinic antagonist
Dose 1 inhalation twice daily (15.6 mcg/actuation)
Pharmacokinetics Metabolism: multiple CYP enzymest1/2: 33-43 hours Time to peak: 5 minutes Excretion: Feces and urine
Contraindications Hypersensitivity to glycopyrrolate or to any of the ingredients
Common side effects Sinusitis, nasopharyngitis, upper respiratory tract infection, oropharyngeal pain, urinary tract infection
Formulation Capsule, inhalation PIFR of 52-133 L/min
Cost $ 297.80 AWP
Place in therapy Monotherapy GOLD BCombination therapy in GOLD C prior to steroids
https://www.pharma.us.novartis.com/sites/www.pharma.us.novartis.com/files/seebri.pdf. Accessed 8/13/16.
© American College of Clinical Pharmacy 74

2016 ACCP Annual Meeting
Glycopyrrolate vs Placebo
139 12311586
0
50
100
150
GEM 1 GEM 2
mL
Difference in FEV1 AUC0-12 and Trough FEV1 from Placebo
FEV1 AUC0-12 Trough FEV1
LaForce C et al. Int J of Chron Obst Pulmon Dis. 2016 Jun 8;11:1233-43Kerwin E et al. Chronic Obstr Pulm Dis (Miami). 2016; 3(2): 549-559
Glycopyrrolate study
Type of Trial Randomized, double blind, placebo controlled, parallel group x 12 wks
Patients 867 subjects with COPD• ≥ 40 years of age• History of smoking at least 10
pack years • FEV1 of at least 30% and less than
80% predicted • mMRC > 2
Outcomes • Improvement in FEV1• ↓ rescue SABA use • ↑ QoL and dyspnea scores
All values p<0.05
© American College of Clinical Pharmacy 75

2016 ACCP Annual Meeting
Glycopyrrolate vs Indacaterol
56 60
0
20
40
60
80
Day 1
(mL)
Change in morning trough FEV1 from baseline
Glycopyrrolate (n=254)
Indacaterol (n=257)
p=NS
Mahler DA et al. Respiratory Medicine, 2016;115:39-45
Aclidinium vs Active ComparatorType of Trial Randomized, DB, PC study x 52 weeks (GEM 3 Study)
Intervention Glycopyrrolate 15.6 mcg INH BID vs Indacaterol 75 mcg INH daily
Outcomes Improvements in 24-h bronchodilation were comparableIndacaterol reduced SABA use vs Glycopyrrolate (p<0.05)Safety was comparable
© American College of Clinical Pharmacy 76

2016 ACCP Annual Meeting
Inhaled Corticosteroid/Long-acting Beta Agonist Combination
© American College of Clinical Pharmacy 77

2016 ACCP Annual Meeting
Medication characteristicsMOA Inhaled corticosteroid and long-acting beta agonist combination
Dose 1 inhalation once daily (100mcg/25mcg per actuation)
Pharmacokinetics Metabolism: CYP3A4t1/2: ~24 hours Time to peak: Fluticasone < 1 hr/ Vilanterol 10 minExcretion: Feces and Urine
Contraindications Primary treatment of acute asthma or COPD exacerbationSevere hypersensitivity to milk proteins or any ingredients
Common side effects Cough, headache, nausea, nasopharyngitis, oropharyngeal pain
Formulation Aerosol power breath activated, inhalation PIFR 43-81 L/min
Cost $267.00 AWP, package size 60 blisters
Place in therapy GOLD C (potentially after LABA/LAMA combo)
https://www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Anoro_Ellipta/pdf/ANORO-ELLIPTA-PI-MG.PDF. Accessed 8/13/16
Fluticasone/vilanterol(Breo® Ellipta®)
© American College of Clinical Pharmacy 78
2016 ACCP Annual Meeting
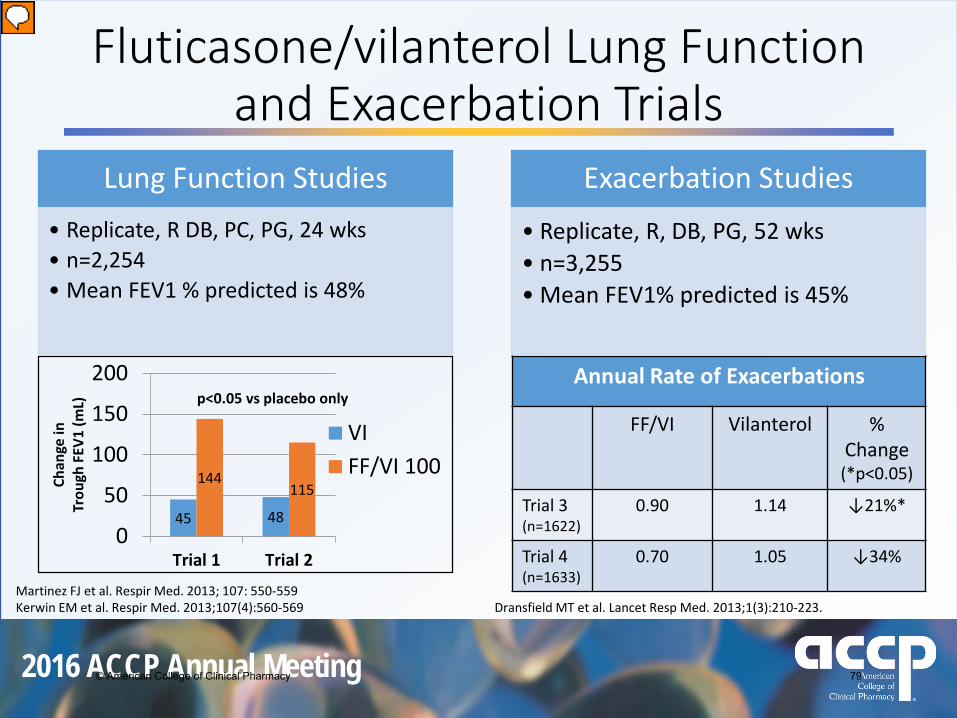
Fluticasone/vilanterol Lung Function and Exacerbation Trials
Martinez FJ et al. Respir Med. 2013; 107: 550-559Kerwin EM et al. Respir Med. 2013;107(4):560-569 Dransfield MT et al. Lancet Resp Med. 2013;1(3):210-223.
45 48
144115
0
50
100
150
200
Trial 1 Trial 2
Chan
ge in
Tr
ough
FEV
1 (m
L)
VIFF/VI 100
p<0.05 vs placebo onlyAnnual Rate of Exacerbations
FF/VI Vilanterol % Change(*p<0.05)
Trial 3 (n=1622)
0.90 1.14 ↓21%*
Trial 4(n=1633)
0.70 1.05 ↓34%
Lung Function Studies• Replicate, R DB, PC, PG, 24 wks• n=2,254• Mean FEV1 % predicted is 48%
Exacerbation Studies
• Replicate, R, DB, PG, 52 wks• n=3,255• Mean FEV1% predicted is 45%
© American College of Clinical Pharmacy 79

2016 ACCP Annual Meeting
Long-acting Beta Agonist/Long-acting
Muscarinic Antagonist Combination
© American College of Clinical Pharmacy 80
2016 ACCP Annual Meeting
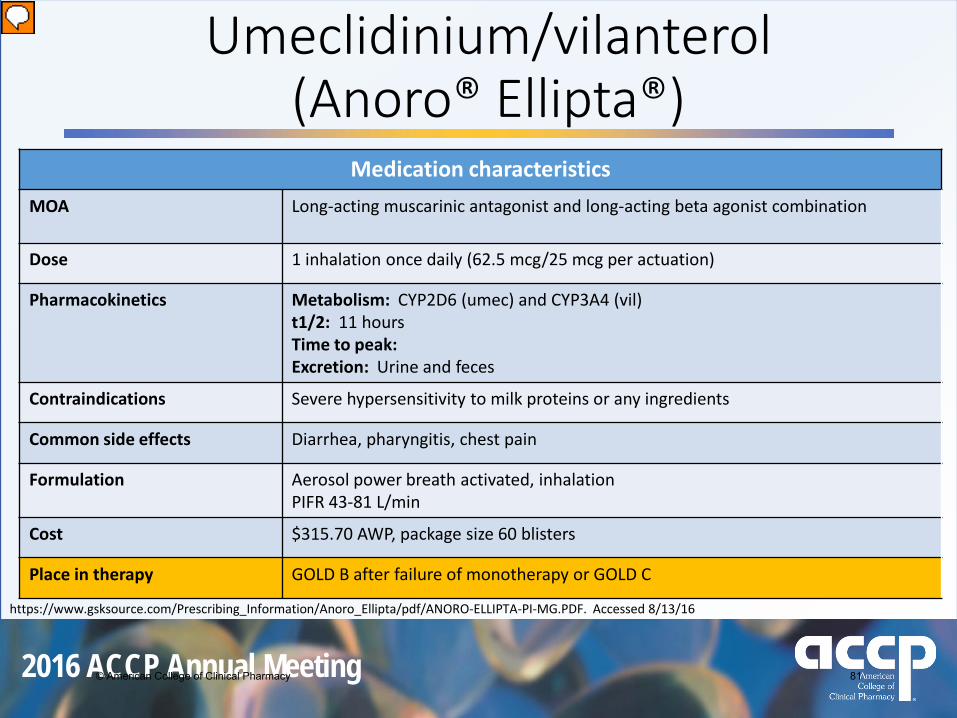
Medication characteristicsMOA Long-acting muscarinic antagonist and long-acting beta agonist combination
Dose 1 inhalation once daily (62.5 mcg/25 mcg per actuation)
Pharmacokinetics Metabolism: CYP2D6 (umec) and CYP3A4 (vil) t1/2: 11 hoursTime to peak:Excretion: Urine and feces
Contraindications Severe hypersensitivity to milk proteins or any ingredients
Common side effects Diarrhea, pharyngitis, chest pain
Formulation Aerosol power breath activated, inhalation PIFR 43-81 L/min
Cost $315.70 AWP, package size 60 blisters
Place in therapy GOLD B after failure of monotherapy or GOLD C
https://www.gsksource.com/Prescribing_Information/Anoro_Ellipta/pdf/ANORO-ELLIPTA-PI-MG.PDF. Accessed 8/13/16
Umeclidinium/vilanterol(Anoro® Ellipta®)
© American College of Clinical Pharmacy 81

2016 ACCP Annual Meeting
Umeclidinium/Vilanterol Clinical TrialsDonohue et al Decramer et al
Type of trial Randomized, DB, PC, PG over 24 wks Replicate, Randomized, blind, DD, PG, 24 wks
Intervention Combo, UMEC 62.5 mcg, VI 25 mcg, placebo
Umec/VI vs Tiotropium
Patients n=1,532 mMRC ≥ 2
Decramer 1- n=846Decramer 2- n=872
Outcomes • FEV1 +52 mL versus 95 mL and 167 mL respectively (p<0.05)
• Dyspnea and QoL similar in all groups
• ↓ exacerbations
Cohen JS et al. Int J COPD. 2016;11:785-797. Decramer M et al. Lancet Respir Med. 2014;2(6):472-486Donohue JF et al. Respir Med. 2013;107(10):1538-1546.
No difference for QoL, symptoms, and exacerbations
© American College of Clinical Pharmacy 82
2016 ACCP Annual Meeting
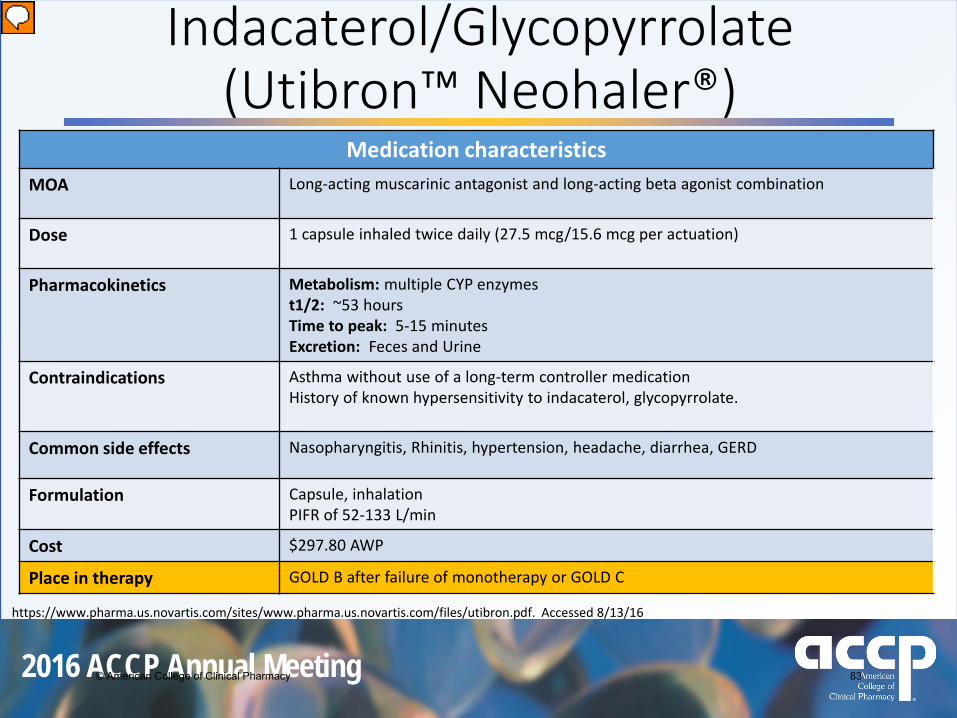
Medication characteristicsMOA Long-acting muscarinic antagonist and long-acting beta agonist combination
Dose 1 capsule inhaled twice daily (27.5 mcg/15.6 mcg per actuation)
Pharmacokinetics Metabolism: multiple CYP enzymes t1/2: ~53 hours Time to peak: 5-15 minutes Excretion: Feces and Urine
Contraindications Asthma without use of a long-term controller medicationHistory of known hypersensitivity to indacaterol, glycopyrrolate.
Common side effects Nasopharyngitis, Rhinitis, hypertension, headache, diarrhea, GERD
Formulation Capsule, inhalation PIFR of 52-133 L/min
Cost $297.80 AWP
Place in therapy GOLD B after failure of monotherapy or GOLD C
https://www.pharma.us.novartis.com/sites/www.pharma.us.novartis.com/files/utibron.pdf. Accessed 8/13/16
Indacaterol/Glycopyrrolate(Utibron™ Neohaler®)
© American College of Clinical Pharmacy 83

2016 ACCP Annual Meeting
Indacaterol/Glycopyrrolate vs Active ComparatorSHINE SPARK ILLUMINATE
Type of trial R, DB, PC, PG R, DB, PG R, DB, DD
Intervention • Inda/Gly vs Tiotriopium• 26 wks
• Inda/Gly vs Tiotriopium• 64 wks
• Inda/Gly vs Salmeterol/fluticasone• 26 wks
Patients FEV1 % Predicted of 30-80% FEV1 < 50% with > 1 exacerbation FEV1 % Predicted of 30-80%
Take Home: Improvements in FEV1, QoL, symptoms, rescue SABA, and exacerbations *NOTE: ALL studies conducted with higher than FDA approved dose
Cohen JS et al. Int J COPD. 2016;11:785-797. Bateman ED et al. Eur Respir J 2013;42:1484-1494.Wedzicha J et al. Lancet Respir Med. 2013;1:199-209. Vogelmeier CF et al. Lancet Respir Med. 2013;1:51-60.
12080
200150
295
0
157
050
100150200250300350
SHINE(n=2,144)
SPARK(n=2,224)
ILLUMINATE(n=523)
Chan
ge in
Tro
ugh
FEV1
(m
L)
TiotropiumInda/GlycoSalm/flut
p<0.05 for all
Δ 80 mL
Δ 70 mL
Δ 138 mL
© American College of Clinical Pharmacy 84

2016 ACCP Annual Meeting
FLAME StudyIndacaterol/Glycopyrrolate vs Salmeterol/Fluticasone
Type of trial R, DB, DD, PG, non-inferiority, multi-center, 52 wks
Intervention Indacaterol/Glycopyrrolate 110/50 mcg QdaySalmeterol/Fluticasone 50/250 mcg bid
Patients n=3,362Age > 40FEV1 % predicted 25-60%mMRC > 2
Indacaterol/Glycopyrrolate
Salmeterol/Fluticasone
p value
Primary OutcomeExacerbations/yr 3.59 4.03 0.003
Secondary Outcomes
Time to first exacerbation 71 days 51 days <0.001Incidence of pneumonia 3.2% 4.8% 0.02Change in Trough FEV1 from baseline
15 mL -48 mL <0.001
Wedzicha JA et al. N Engl J Med 2016;374:2222-34.
© American College of Clinical Pharmacy 85
2016 ACCP Annual Meeting
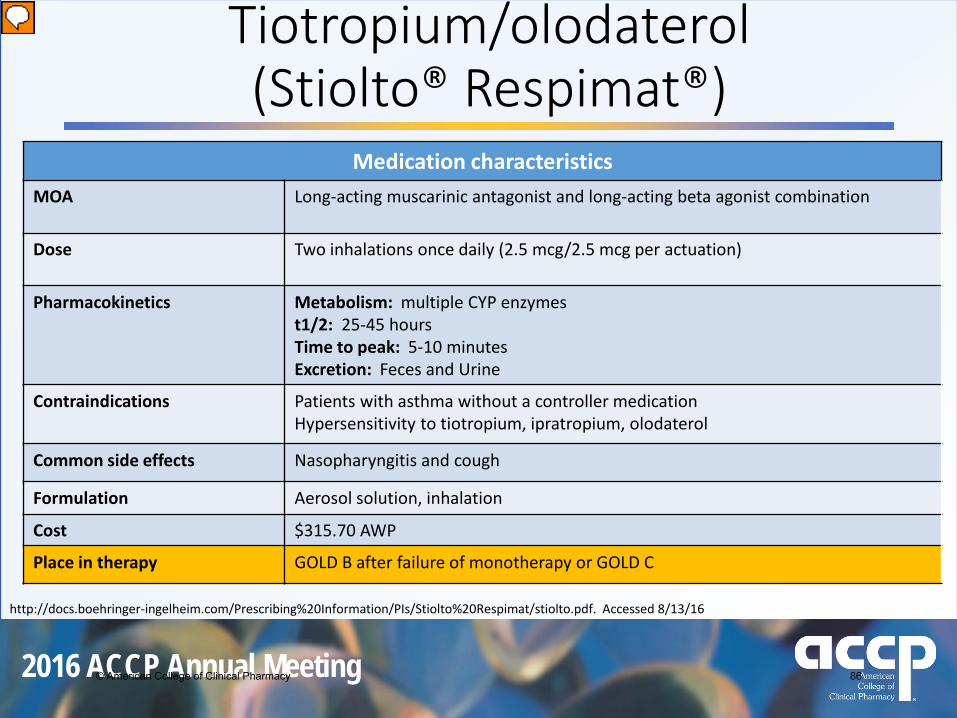
Medication characteristicsMOA Long-acting muscarinic antagonist and long-acting beta agonist combination
Dose Two inhalations once daily (2.5 mcg/2.5 mcg per actuation)
Pharmacokinetics Metabolism: multiple CYP enzymest1/2: 25-45 hours Time to peak: 5-10 minutes Excretion: Feces and Urine
Contraindications Patients with asthma without a controller medication Hypersensitivity to tiotropium, ipratropium, olodaterol
Common side effects Nasopharyngitis and cough
Formulation Aerosol solution, inhalation
Cost $315.70 AWP
Place in therapy GOLD B after failure of monotherapy or GOLD C
http://docs.boehringer-ingelheim.com/Prescribing%20Information/PIs/Stiolto%20Respimat/stiolto.pdf. Accessed 8/13/16
Tiotropium/olodaterol(Stiolto® Respimat®)
© American College of Clinical Pharmacy 86

2016 ACCP Annual Meeting
Tiotropium/Olodaterol vs Individual Components
Buhl R et al. Eur Respir J 2015; 45: 869–871
TOnado 1 and 2Type of trial Randomized, double-blind, parallel group Outcomes
Intervention • Treatment groups (daily dose) • T/O 2.5/5 mcg• T/O 5/5 mcg• TIO 2.5 mcg• TIO 5 mcg• OLO 5 mcg
• 52 weeks
Patients • 5,163 COPD patients • ≥ 40 yrs old• Smoking history of > 10 pack-
years• Moderate to very severe
pulmonary impairment • ↑ FVC and QoL• ↓ rescue SABA and exacerbations
© American College of Clinical Pharmacy 87

2016 ACCP Annual Meeting
ENERGITO Study
Type of trial Randomized , double-blind, double-dummy with four 6 wktreatment arms, each followed by 3 wk washout
Patients n=220 pts• 10 yr history of smoking• FEV1/FVC < 0.70• GOLD Class 2 and 3
Adjusted Mean FEV1 AUCTio/Olo 2.5/2.5 Salmeterol/Fluticasone
50/250Difference
FEV1 AUC (0-12hrs) 317 mL 192 mL 125 mL*
FEV1 AUC (12-24hrs) 172 mL 132 mL 40 mL*
Conclusion Improved lung function and hyperinflation at all time pointsBeeh KM et al. Int J COPD. 2016;11:193-205
Tiotropium/Olodaterol vs Salmeterol/Fluticasone
*p<0.05
© American College of Clinical Pharmacy 88

2016 ACCP Annual Meeting
Medication characteristicsMOA Long-acting muscarinic antagonist and long-acting beta agonist combination
Dose Two inhalations twice daily (9mcg/4.8 mcg per inhalation)
Pharmacokinetics Metabolism: CYP2D6 and CYP2Ct1/2: 11.8 hours Time to peak: 5-20 minutes Excretion: Feces and Urine
Contraindications Patients with asthma without use of a long-term control medicationHypersensitivity to glycopyrrolate, formoterol, or any component
Common side effects Nasopharyngitis and cough
Formulation Aerosol, inhalation
Cost Not available
Place in therapy GOLD B after failure of monotherapy or GOLD C
http://www.azpicentral.com/bevespi/bevespi_pi.pdf. Accessed 8/13/16
Glycopyrrolate/formoterol (Bevespi Aerosphere™)
© American College of Clinical Pharmacy 89

2016 ACCP Annual Meeting
Glycopyrrolate/formoterol vs Individual Components
PINNACLE 1 and 2Type of trial Replicate, randomized, double-blind,
placebo controlled, parallel groupOutcomes
Intervention • Treatment groups (2 puffs bid)• Gly/For 9/4.8 mcg• Gly 9 mcg• For 4.8 mcg• Placebo
• 24 weeks
Patients • 3,699 COPD patients • ≥ 40 yrs old• Smoking history of > 10 pack-
years• Moderate to very severe
pulmonary impairment
150
103
59 5464 56
0
20
40
60
80
100
120
140
160
PINNACLE 1 PINNACLE 2
mL
Change in Trough FEV1
Gly/For vsPlacebo
Gly/For vs Gly
Gly/For vs For
http://www.azpicentral.com/bevespi/bevespi_pi.pdf. Accessed 8/13/16
© American College of Clinical Pharmacy 90
2016 ACCP Annual Meeting
So, which agent do we choose?
Too many choices!
Disease assessment Cost
Delivery system Adherence
© American College of Clinical Pharmacy 91
2016 ACCP Annual Meeting
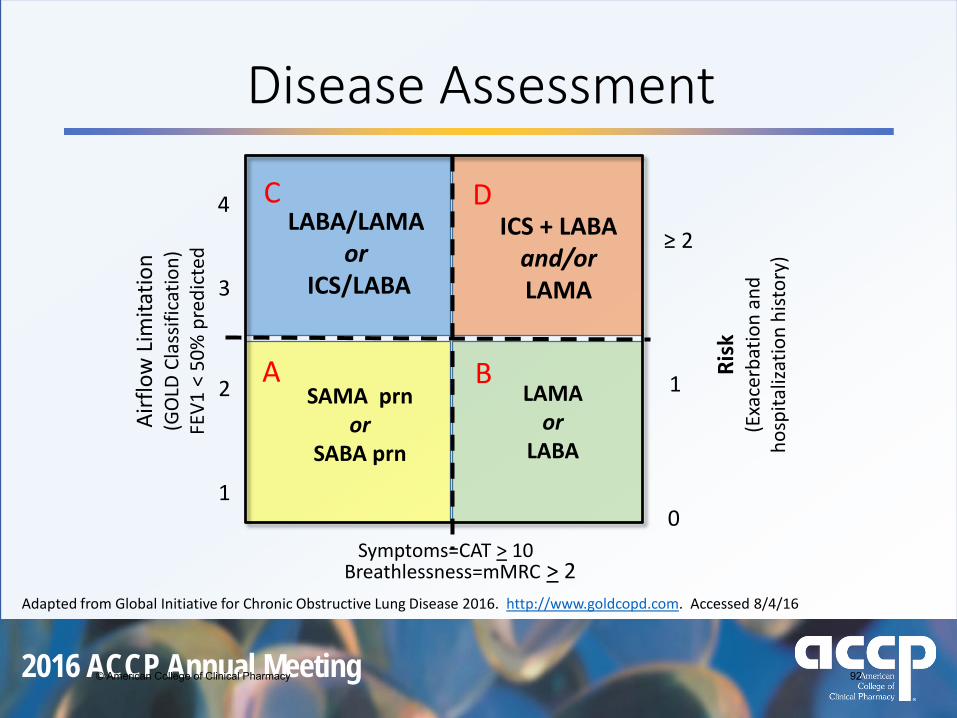
Disease AssessmentAi
rflo
w L
imita
tion
(GO
LD C
lass
ifica
tion)
FEV1
< 5
0% p
redi
cted
Risk
(Exa
cerb
atio
n an
d ho
spita
lizat
ion
hist
ory)
≥ 2
1
0Symptoms=CAT > 10
4
3
2
1
ICS + LABAand/orLAMA
Adapted from Global Initiative for Chronic Obstructive Lung Disease 2016. http://www.goldcopd.com. Accessed 8/4/16
A B
C D
SAMA prnor
SABA prn
LAMA or
LABA
LABA/LAMAor
ICS/LABA
Breathlessness=mMRC > 2
© American College of Clinical Pharmacy 92
2016 ACCP Annual Meeting
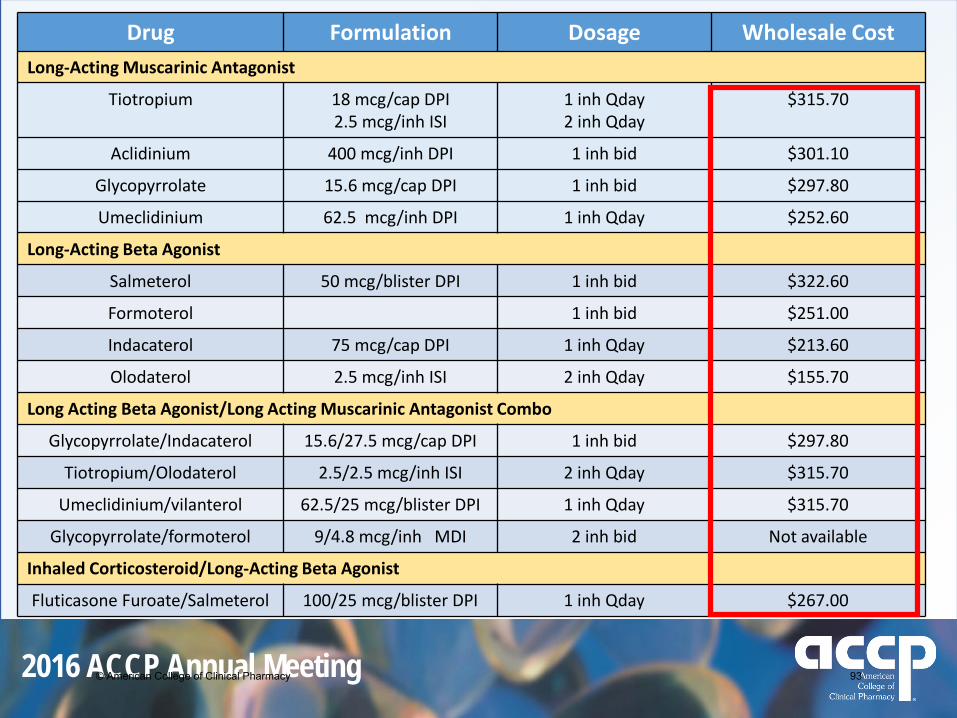
Drug Formulation Dosage Wholesale CostLong-Acting Muscarinic Antagonist
Tiotropium 18 mcg/cap DPI2.5 mcg/inh ISI
1 inh Qday2 inh Qday
$315.70
Aclidinium 400 mcg/inh DPI 1 inh bid $301.10
Glycopyrrolate 15.6 mcg/cap DPI 1 inh bid $297.80
Umeclidinium 62.5 mcg/inh DPI 1 inh Qday $252.60
Long-Acting Beta Agonist
Salmeterol 50 mcg/blister DPI 1 inh bid $322.60
Formoterol 1 inh bid $251.00
Indacaterol 75 mcg/cap DPI 1 inh Qday $213.60
Olodaterol 2.5 mcg/inh ISI 2 inh Qday $155.70
Long Acting Beta Agonist/Long Acting Muscarinic Antagonist Combo
Glycopyrrolate/Indacaterol 15.6/27.5 mcg/cap DPI 1 inh bid $297.80
Tiotropium/Olodaterol 2.5/2.5 mcg/inh ISI 2 inh Qday $315.70
Umeclidinium/vilanterol 62.5/25 mcg/blister DPI 1 inh Qday $315.70
Glycopyrrolate/formoterol 9/4.8 mcg/inh MDI 2 inh bid Not available
Inhaled Corticosteroid/Long-Acting Beta Agonist
Fluticasone Furoate/Salmeterol 100/25 mcg/blister DPI 1 inh Qday $267.00
© American College of Clinical Pharmacy 93

2016 ACCP Annual Meeting
Delivery SystemsType Advantages Disadvantages
Nebulizer • Patient coordination not required• Tidal breathing
• Device cleaning required • Expensive• Contamination possible• Not all medication available in solution
formPressurizedmetered dose inhaler
• Portable and compact• Treatment time is short• No drug preparation required• Dose-dose reproducibility high
• Coordination of breathing and actuation needed
• Necessary hand strength• High pharyngeal deposition
Dry powder inhaler
• Breath-actuated• Less coordination required• Small and portable• Short treatment time• Dose counters
• Requires moderate to high inspiratory flow
• Some units are single dose (capsules)• Can result in high pharyngeal deposition
Soft mist inhalers
• Similar to neb but more convenient
• Lower pharyngeal deposition• 1/3 the actuation rate of MDI
• High cost• Some coordination required• Limited products
Barrons R et al. Patient Intelligence. 2015;7:53-65.
© American College of Clinical Pharmacy 94

2016 ACCP Annual Meeting
Adherence
“Drugs don’t work in patients that don’t take them”
• 60% of COPD pts nonadherent• Nonadherence leads to:
• ↑ exacerbations, hospitalizations and mortality
• Reasons:• # of meds and dosing frequency contribute significantly• Cost
Restrepo RD et al. Int J Chron Obstruct Pulmon Dis. 2008;3(3):371-384.Agh T et al. Respiration. 2011;82,(4):328–34.Agh T. http://www.intechopen.com/books/chronic-obstructive-pulmonarydisease-current-concepts-and-practice/adherence-to-therapy-in-chronic-obstructive-pulmonary-disease. Accessed 8/14/16
C. Everett Koop, M.D.
© American College of Clinical Pharmacy 95

2016 ACCP Annual Meeting
Ideal Therapy for COPD Adherence
Ease of administration
DyspneaExacerbations
Exercise Tolerance
Quality of LifeMortality
HospitalizationsOverall Cost
© American College of Clinical Pharmacy 96

2016 ACCP Annual Meeting
Christopher K. Finch, Pharm.D., BCPS, FCCM, FCCPDirector of Pharmacy
Methodist University HospitalAssociate Professor
University of Tennessee, College of PharmacyMemphis, TN
October 24, 2016
Update in COPD Pharmacotherapy: Is New Better?
© American College of Clinical Pharmacy 97