Embed Size (px)
DESCRIPTION
(8.20.13)
Citation preview

Copyright restrictions may apply
JAMA Pediatrics Journal Club Slides: Flaxseed in Pediatric Hyperlipidemia
Wong H, Chahal N, Manlhiot C, Niedra E, McCrindle BW. Flaxseed in pediatric hyperlipidemia: a placebo-controlled, blinded, randomized clinical trial of dietary flaxseed supplementation for children and adolescents with hypercholesterolemia. JAMA Pediatr. Published online June 3, 2013. doi:10.1001/jamapediatrics.2013.1442.

Copyright restrictions may apply
• Background
– Elevated lipid profiles in youth are risk factors for early development of atherosclerotic lesions and cardiovascular disease.
– Pharmacologic interventions are used when lifestyle approaches fail to decrease low-density lipoprotein cholesterol within acceptable ranges.
– Dietary flaxseed may be a functional food that contains agents hypothesized to have hypolipidemic activity and/or other properties that may benefit cardiovascular health.
• Study Objective
– To determine the safety and efficacy of dietary flaxseed supplementation in the management of hypercholesterolemia in children.
Introduction

Copyright restrictions may apply
• Study Design
– Placebo-controlled, randomized clinical trial.
– Duration of intervention: 4 weeks.
• Setting
– Specialized dyslipidemia clinic at a tertiary pediatric care center.
• Patients
– 32 participants aged 8 to 18 years.
– Low-density lipoprotein cholesterol from 135 mg/dL (3.5 mmol/L) to less than 193 mg/dL (5.0 mmol/L).
Methods

Copyright restrictions may apply
• Patients
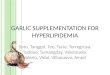
– The intervention group ate 2 muffins and 1 slice of bread daily containing ground flaxseed (30 g flaxseed total).
– The control group ate muffins and bread substituted with whole-wheat flour.
Nutritional Content per Serving of Muffins and Breads Used in the Study
Methods

Copyright restrictions may apply
Methods
• Outcomes– Primary: Attributable change in fasting lipid profile levels of high-density
lipoprotein cholesterol and triglycerides.– Secondary: Attributable change in fasting total cholesterol, low-density
lipoprotein cholesterol, body mass index z score, and total caloric intake.
• Limitations
– Flaxseed may lose nutritional value and thus effectiveness when ground for the consumption of muffins and bread by pediatric patients.
– Increases in body mass index and daily caloric intake were noted in both study groups during the trial.
– Compliance assessments were based on self-report from patient-completed intake logs and not through a direct biological measure.
– Small sample size (n = 32) and short duration of intervention (4 weeks).

Copyright restrictions may apply
Results
Comparison of Baseline Characteristicsa

Copyright restrictions may apply
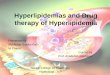
Results
Change in Outcomes

Copyright restrictions may apply
Comment
• Dietary flaxseed supplementation was associated with no attributable benefit regarding lipid levels.
• Dietary flaxseed supplementation, while safe, was associated with adverse changes in the lipid profile of children with hypercholesterolemia:
– Significant decrease noted in high-density lipoprotein cholesterol level.
– Significant increase in triglyceride levels.
• The use of flaxseed supplementation in children with hypercholesterolemia may not be a viable option for lipid management.

Copyright restrictions may apply
Comment
• Nonpharmacologic management of hypercholesterolemia in children is challenging, with few available options.
• Flaxseed has been proposed as a possible alternative therapy for treating dyslipidemia.
• The predominant mechanism by which flaxseed influences lipid profiles remains unknown.
• Flaxseed supplementation remains an unverified strategy for the clinical management of cardiovascular risk factors in youths with hyperlipidemia and may adversely affect the lipid profile.

Copyright restrictions may apply
• If you have questions, please contact the corresponding author:– Brian W. McCrindle, MD, MPH, The Hospital for Sick Children,
555 University Ave, Toronto, ON M5G 1X8, Canada ([email protected]).
Funding/Support
• This study was supported by a research grant from the Labatt Family Innovation Fund.
Conflict of Interest Disclosures
• None reported.
Contact Information