Embed Size (px)
Citation preview

196
as seen previously on intravenous pyelography, but not com-pletely obstructed. A month after the right nephrectomythe left ureter was explored through an anterolateral obliquemuscle-cutting incision. The retroperitoneal mass had notextended so far laterally on this side but the left ureter wasalready embedded in it. It was freed without difficulty,leaving behind a pink shiny trough in which it had lain.The posterior parietal peritoneum was tacked down mediallyto displace the ureter laterally and to prevent its reinvolve-ment, because the peritoneum seemed to form a definitebarrier to the spread of this inflammation.
Aortography.-Since it has been postulated that peri-ureteric fibrosis begins as arteriolitis in the lumbar and othersmall retroperitoneal vessels, aortography was done underdirect vision at the second operation ; but it did not show
any gross abnormality in the lumbar arteries.Follow-up.-Since discharge from hospital after an unevent-
ful recovery this man has remained well and is symptom-free.Discussion
Why the retroperitoneal tissues become involved in amass of young fibrous tissue is unknown. Trauma,previous gastrointestinal disturbances, infection of the
para-aortic lymph-nodes, and arteritis like that seen incertain collagen diseases have been suggested as primarycauses.
All the published cases have been in males aged 35-60.The history is vague but common to all the cases : months ofill health, with loss of weight, appetite, and strength, followedby aching in the abdomen and loins. Sometimes this achingspreads to the thighs and genitalia. Examination does notreveal any physical signs. Some patients are investigated asan orthopxdic problem but may be eventually admittedwith oliguria and anuria. Our patient was urxmic onadmission. Most of the patients have a few red cells andwhite cells in their urine at some stage.The intravenous pyelogram is characteristic, with early
hydronephrosis and medial displacement of the ureters.
Ureteric catheterisation is important diagnostically and
therapeutically but may be impossible because of ureteric
involvement ; the fibrous tissue may have invaded the ureterand narrowed it besides kinking it. In patients with oliguriaor anuria it is remarkable how urine pours down the uretericcatheter. Renal function appears to be satisfactory ; theureteric lumen may be patent, but the ureter cannot pass theurine to the bladder, possibly because of lost peristalsis.The indwelling ureteric catheter, if it can be introduced, allowsdrainage of the distended renal pelvis and tides the patientover the acute obstructive phase.
Treatment is directed solely to prevent progressiveureteric obstruction. No other complication of this largeretroperitoneal mass has been reported. This plaqueof tissue cannot be removed, because the great vesselsand their branches are extensively involved. Surgeryhas been directed to the release of the ureters and the useof the parietal peritoneum as a barrier against reinvolve-ment. One case at Mount Sinai Hospital, New York,was treated by radiotherapy in view of the primitive and" invasive " appearance of the fibroblasts in this mass.The patient recovered well, but the development of
malignant hypertension in cases of seminoma of testistreated by radiotherapy to the para-aortic lymph-nodesmakes one hesitate to use it in a non-malignant condi-tion. Renal damage is often already present and themass is known to undergo spontaneous regression.Chemotherapy has not been found of value. Surgeryseems to offer the best chance of survival. Uretericcatheterisation or nephrostomy is necessary in the veryacute phase when anuria is present. The release of theureters and " protection " by peritoneum can be done instages. It should be possible to avoid nephrectomy in
most cases. We removed the right kidney because theureter was extensively involved and because the
" benign " nature of this mass was not appreciated.
SummaryPeriureteric fibrosis is not so rare as the paucity of
published reports thereof suggests.Its aetiology is unknown.The history is of vague ill health with backache and
abdominal and loin pain. The presenting feature maybe anuria, oliguria, or urxmia. The intravenous pyelo-gram showing medially displaced ureters is verycharacteristic.Treatment consists in restoring renal function by
draining the obstructed kidneys by ureteric catheterisationin the acute phase and by surgical release and peritoneal"
protection " of the ureters as a staged procedure.Chemotherapy does not seem to influence this inflam-
matory mass. Radiotherapy is not advised.We wish to thank Dr. W. A. Bourne for referring this case to us,
and Dr. R. I. K. Elliott for the pathological report.
REFERENCESLancet (1957) ii, 780.Raper, F. P. (1955), Proc. R. Soc. Med. 48, 736.
Preliminary Communication
HYDROXYDIONE IN PSYCHIATRIC INTERVIEWS
THE two main uses of anaesthetic drugs in psychiatricinterviews are exploratory and abreactive. With manydrugs these uses overlap, and to prevent affective releasethe level of anaesthesia has to be deepened, thereby inter-fering with recall and communication. Followingreports 1-4 on the use of steroid anaesthetic agents, witha smooth anxiety-free induction phase and lack of post-anxsthetic depression, we decided to try them in placeof amylobarbitone sodium. Thirty-five patients were
investigated-predominantly psychoneurotic, but includ-ing some with schizophrenia and psychopathic personality.Hydroxydione (’Presuren’) is prepared as a 2-5%
solution in physiological saline solution at 110°F, and israpidly injected intravenously at this temperature. Greatcare must be taken that none escapes into the tissues;the greater the speed of injection the less likelihood ofvenous thrombosis. 5
There is no clinical effect for three minutes after
injection; then the patient relaxes. After five minutes the
patient perseverates somewhat, but if the correct dose isused this is the only evidence of altered consciousness.The effect of the drug lasts for about half an hour fromthis point. The induction phase is invariably smooth,and freedom from anxiety persists. Speech is not slurred.0-5 gr. was found to be the optimal dose to obtain thiseffect for the average man of 10 stones; slightly less wasused for those under this weight. There was no severevenous thrombosis and no ansesthetic complications-e.g., sudden falls in blood-pressure or excessive shallow-ness of respiration. No patient complained of anydepression after the interview that could be attributed tothe steroid.
Except with the catatonic patients, rapport was excellentthroughout the interview and the patients freely recalled1. Taddei, A. Gazz. int. med-chir. 1955, 19, 1521.2. Murphy, F. J., Guadagni, N. P., De Bon, F. J. Amer. Med. Ass. 1955,
158, 1412.3. Taylor, N., Shearer, W. M. Brit. J. Anœsth. 1956, 28, 67.4. Galley, A. H., Rooms, M. Lancet, 1957, i, 990.5. Stedtfeld, G. Anœsthetist, 1957, 6, 140.

197
repressed material with no abreactive release. They wereuncritical in attitude: often many staff were in the room,but this did not cause them to withhold incidents which
they were previously unable to recall even to themselves.One patienty a C. J. voluntary, admitted, while a taperecorder was in action, that he had been doing his best tohoax the staff into believing that he was being cooperative,to avoid remaining in hospital. Several homosexual
patients remembered the early childhood trauma, homo-sexual seductions long repressed. Since no affect wasshown at the interviews, methylamphetamine (up to
60 mg.) was injected before or after the steroid; in thesecases the patient entered a
" perseveratory-ruminative "
state, but no affect was exhibited until after the steroidwas excreted, when abreaction began on the theme whichwas uppermost in consciousness during this phase, withexcellent therapeutic effects.The absence of release in the catatonic patients was
notable, and there was only momentarily clearing of
acrocyanosis. From other work in progress at the momentthis effect seems to be due to a lack of parasympatheticinhibition with hydroxydione, in contrast to thebarbiturates.
In our limited experience, hydroxydione seems to beexcellent where the object of the interview is to uncoverthe psychodynamics of the illness, especially in patientswith early repressed memories; but because of the
qualitative difference of effect upon the autonomic systemit seems inferior to other agents when abreaction is
desired, though this may be overcome by the addition ofmethylamphetamine.We thank Dr. G. J. Harrison, medical superintendent, for per-
mission to undertake this study, and for his and our other colleagues’advice and criticism; and Schering A.G., Berlin, for supplies of’ Presuren ’.
P. M. O’FLANAGAN,L.R.C.P.I., D.P.M.
O. L. MCGUINNESS,M.B. N.U.I.
Winwick Hospital,near Warrington, Lancs
New Inventions
A BLOOD PUMP WHICH MINIMISES HÆMOLYSIS
THE pumps needed to operate such devices’as the artificialheart-lung and kidney raise several problems.They must produce the least possible coagulation (to reduce the
need for heparinisation), and they must be built entirely of materialswhich do not favour coagulation and which are neither toxic norattacked by blood.They must produce the least possible haemolysisņi.e., they must
be tree trom sudden movements leading to
turbulence, and the valves must be efficient, forreflux of blood would lead to the shock of twocolumns meeting.
DESIGN
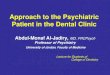
We have developed a pump (fig. 1) builtentirely of methyl methacrylate and silicone.It consists essentially of three chambers:a central one (1, fig. 1), an inlet (6), and anoutlet (7).The central chamber consists of a silicone tube
locked into a methacrylate sleeve. The sleeve isconnected to an air-compressor, which periodi-cally increases the pressure inside the sleeve. Thisincrease compresses the silicone tube, which thusacts as a cardiac ventricle. The increase of
pressure is gentle and uniform, because it isproduced by an increase in the pressure of a gasexerted on a soft flexible wall. The propulsionof the blood is very similar to that in the heart.
This central chamber is tapered at its outletend (2), which is used as a valve seat. The
tapering reduces the calibre gradually and theblood in systole slides smoothly along the walls.This part is fixed to the main chamber by amethacrylate ring (8), which tightens it againstthe wings of the silicone tube.The valve (4) is a silicone tongue-valve. Inside
the tongue is a lead core to give it a certaininertia and make the closing movement moreregular (this lead does not come in contact withthe blood).At the lower end of the central chamber is
another similar valve (5) which lies on the lowerwing with a methacrylate washer to make a moreperfect adjustment than is possible betweensilicone and silicone. The upper end (3) of thelower chamber (6) is tapered in the same wayas (2). The upper (7) and lower chambers aresilicone tubes, of diameter equal to that of thecompression chamber but three times as long.These tubes are fitted over the ends of the
, central chamber, making use of their elasticity,! and at each end is placed a methacrylate con-
nector for joining the pump to the other apparatus.
Fig. 1-The con-struction of thepump. ,
PERFORMANCE
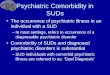
The damping chambers tend to expand during the systoleof the central chamber and to contract during its diastole (fig.2), transforming the discontinuous current produced by theseries of strokes into a continuous current,and preventing the valves from making quickmovements. For instance, the lower valvetends Lo close in systole, but at the sametime the tension in the inlet chamber is
increased, and this tension is greater themore the valve tends to close; thus, suddenclosing is avoided and so is the subsequentdanger of hxmolysis caused by sudden
stoppage of the blood column.The amount of blood pumped depends on
the size of the driving-chamber and the rateof the compressor. For use with the artificial
kidney, we recommend a diameter of 20 mm.for all the silicone tubes, and a length of75 mm. for the compression chamber and of200 mm. for the damping chambers. A pumpof these measurements has a capacity of160 ml. and gives an efficient stroke-volumewith the compressor which we use (pistondiameter 60 mm., stroke 70 mm.) of up to15 ml. The actual stroke-volume dependson whether we direct the whole power ofthe compressor to the driving-chamber or
allow (by means of a special device) a gradual leak of the airdriven by the chamber. 30 strokes per min. is the optimum foruse with artificial kidneys; with this frequency and the describedcompressor the flow is up to 450 ml. a minute.We have pumped 300 ml. of blood continuously, at a speed
of 200 ml. a minute, for twelve hours without any haemolysis,though each erythrocyte has passed about 500 times throughthe pump. The total volume passed through was 144 litres, or30 times the normal blood-volume. With the artificial kidney,rarely is more than 15 times the total blood-volume circulated.
For the bigger flow needed with the artificial heart-lung, werecommend a compression chamber of diameter 30 mm. andlength 100 mm., and an increased compressor rate. This pump,with an adequate compressor, gives an effective output of41 ml. per stroke. With a frequency of 100 strokes a minutewe obtain an output of 4100 ml. In this case the dampingchambers should have a diameter of 30 mm. and a length of200 mm. The pump thus manufactured has a capacity of210 ml.
This pump is manufactured by Messrs. R. Bernadas, 46/A ViaLayetana, Barcelona.
Fig.2-Actionof dampingchambers.
E. ROTELLARM.D. BarcelonaHospital of the Red Cross of Barcelona