Embed Size (px)
Citation preview

10/1/2021
1
PSYCHIATRIC MEDICATION IN PREGNANT AND BREASTFEEDING WOMEN
Madison Holbrook, Pharm.D.
PGY-2 Psychiatric Pharmacy Resident
Laureate Psychiatric Clinic and Hospital
Oklahoma Society of Health System Pharmacists Meeting
October 22, 2021
FINANCIAL DISCLOSURE AND RESOLUTION
Under guidelines established under the Standards for Integrity and Independence in Accredited Continuing Education, disclosure must be made regarding relevant financial relationships with ineligible companies within the last 24 months.
I have no relevant financial relationships with ineligible companies to disclose.

10/1/2021
2
PROFESSIONAL PRACTICE GAP
• There is a lack of significant evidence in the setting of psychiatric medication use in pregnant and breastfeeding women as it is unethical. It is imperative to apply the data we do have to make clinical decisions in favor of both the mother and the fetus or infant at risk.
• It is important to have evidential and reliable resources on hand.
• As pharmacist, it is our responsibility to share and communicate our knowledge and educate patients and colleagues about the risk vs benefit in psychiatric medications use in pregnant or breast feeding women.
LEARNING OBJECTIVES
At the completion of this activity, pharmacists will be able to:
• Identify psychiatric medications appropriate for utilization in pregnant patients
• Identify psychiatric medications appropriate for utilization in breastfeeding patients
• Recognize potential psychiatric medication adverse effects or fetal harm
At the completion of this activity, pharmacy technicians will be able to:
• Identify psychiatric medications appropriate for utilization in pregnant patients
• Identify psychiatric medications appropriate for utilization in breastfeeding patients

10/1/2021
3
PRE-ASSESSMENT QUESTION 1
JN is a pregnant patient on ziprasidone and escitalopram who has struggled with conception for years. Due to this difficulty, she is worried about the impact of medications on her baby. In research studies, which impact on infants has been found to be most associated with in utero antidepressant exposure?
• Spontaneous abortion with 3rd trimester antidepressant use• Reduced gestational time with 2nd trimester antidepressant use • Persistent pulmonary hypertension with any antidepressant use • Postnatal adaption syndrome with 1st trimester antidepressant use
5
PRE-ASSESSMENT QUESTION 2
After discussing the risks of untreated depression with JN, you begin to consider the role of pharmacotherapy in JN’s perinatal depression. Considering what is known about JN, and any known risk factors, which statement describes the most likely impact of antidepressant therapy in JN?
• Conversion to manic episode• Risk of psychosis or infanticide • Possible postpartum hemorrhage • Development of gestational hypertension
6

10/1/2021
4
PRE-ASSESSMENT QUESTION 3
Based on the adverse effects of ziprasidone, what side effect could have added to JN’s struggle in conceiving? Which of the following would be most important to monitor for a patient taking this medication?
• Weight loss • Hyperprolactemia• Akathisia• QTc prolongation
7
ABBREVIATIONS
ABBREVIATION WORD
PTSD Post-traumatic stress disorder
PO Oral
TID Three times daily
BID Twice daily
PRN As needed
SSRI Selective serotonin reuptake inhibitor
SNRI Serotonin norepinephrine reuptake inhibitor
TCA Tricyclic antidepressant
MAOI Monoamine oxidase inhibitor
EPS Extrapyramidal symptoms
OR Odds ratio
AE Adverse effect
EKG Electrocardiogram
FGA First generation antipsychotic
SGA Second generation antipsychotic
SCr Serum creatinine
BUN Blood urea nitrogen
MOA Mechanism of action

10/1/2021
5
THE DEBATE
Exposure to psychiatric medication
Consequences of mother’s poor mental health
• Spontaneous abortion • Birth defects• Abnormal brain development • Behavioral abnormalities • Withdrawal • Unknown
• Low birth weight• Preterm Labor• Preeclampsia • Maternal Suicide • Compliance to fetus/infant care • Use of substances
Risk to infant or fetus from
Controversial evidence for psychiatric medications inducing birth defects
Committee Opinion Number 757. American College of Obstetrician and Gynecologists. Obstet Gynecol. 2018;132:e208-12. Massachusetts General Hospital. Center for Women’s Mental Health.
BACKGROUND
• Facts • 500,000 pregnancies per year involve women with psychiatric illness • Pregnant women who discontinue antidepressants are 5 times more
likely to relapse • Suicide is the leading cause of maternal death • Risk of postpartum psychosis 3-fold higher with perinatal discontinuation
of mood stabilizers • 4.5% rate of infanticide with postpartum depression psychosis
• Pharmacist • 60% of pregnant women take >1 medications • 70% of women who breastfeed and/or pump their milk take medication• 90% of clinically approved medications do not have appropriate drug
labeling information for pregnant and lactating women
Am Fam Physician. 2008 Sep 15;78(6):772-778.MGH Center for Women’s Mental Health.
Cohen L, et al. JAMA. 2006;295(5):499-507.

10/1/2021
6
PATIENT CASE
• Kara is a 29 year old female with a PMH including bipolar disorder, anxiety, PTSD, alcohol use disorder, and type II diabetes.
• Her medications include: • Lithium 300 mg PO TID • Sertraline 50 mg PO daily• Quetiapine 400 mg PO HS • Hydroxyzine 10 mg PO TID prn • Trazodone 50 mg PO HS • Metformin 500 mg PO BID
• Kara has been sober for 2 years and is now 6 weeks pregnant. She presents today asking about her medications in relation to her pregnancy.
ADVERSE EFFECTS
PREGNANCY
BREASTFEEDING
POSTPARTUM THERAPY

10/1/2021
7
ADVERSE EFFECTS
Structural Teratogeneis
Behavioral Teratogensis
Perinatal Syndrome
Postnatal Syndrome
STRUCTURAL TERATOGENESIS
• Physical malformations
• Risk is highest week 2-8 post fertilization
• Occurs in 6% of all pregnancies with 3% induced by drug or environment
• Examples: • Oral cleft • Spinal bifida• Atrial septal defect
Ward R, et al. Am Fam Physician. 2002 .66(4):629-637.

10/1/2021
8
BEHAVIORAL TERATOGENESIS
• Occurrence of behavior or neuropsychiatric symptoms in offspring after in utero exposure to a drug or toxin
• Inherited mental illness vs. drug effects
• Highest risk during the third trimester
• Examples: • Autism • Attention Deficit Hyperactivity Disorder• Feeding issues
Grote N, et al. Arch Gen Psychiatry. 2010;67(10):1012-1024. Ward R, et al. Am Fam Physician. 2002 .66(4):629-637.
PERINATAL SYNDROME
• Drug intoxication or withdrawal
• Examples: • Agitation • Tachycardia • Hypo tonicity • Tremor or restlessness • Respiratory distress or cyanosis • Poor temperature control • Seizures
American College of Obstetricians and Gynecologists: Yonkers K, et al. Obstet Gynecol. 2009;114(3)703-713.Ward R, et al. Am Fam Physician. 2002 .66(4):629-637.

10/1/2021
9
POSTNATAL SYNDROME
• Hormonal changes peak in the third trimester of pregnancy
• After labor and birth of baby, hormones drop dramatically
Ward R, et al. Am Fam Physician. 2002 .66(4):629-637.
ADVERSE EFFECTS
PREGNANCY
BREASTFEEDING
POSTPARTUM THERAPY

10/1/2021
10
PREGNANCY
FIRST TRIMESTER
• Major organ development
SECOND TRIMESTER
• Baby bump • Movement
THIRD TRIMESTER
• Hormonal peak
PREGNANCY
American College of Obstetricians and Gynecologists. Obstet Gynecol. 2018;132:e208-212.
PREGNANCY
• Psychiatric medications are recommended in patients with moderate depression or those with recurrent history of severe depression or psychiatric disorder
• Medication Selection• History • Contraindications • Lowest effective dose • Fewer metabolites • Higher protein binding • Fewer drug interactions
• Alternatives: • Psychotherapy
American College of Obstetricians and Gynecologists. Obstet Gynecol. 2018;132:e208-212.

10/1/2021
11
PHARMACOKINETIC DIFFERENCES IN PREGNANCY
• Pregnancy: • Increased volume of distribution for lipophilic medications (antipsychotics) • Increased hepatic blood flow • Increased renal blood flow and glomerular filtration rate
• CYP enzyme changes • Inhibited during pregnancy
– CYP1A2– CYP2B6– CYP2C19– CYP3A4
• Induced during pregnancy – CYP2A6– CYP1A4– CYP2B7
Deligiannidis K, et al. J Clin Psychopharmacol. 2014;34(2):244-255.
PREGNANCY + DEPRESSION
Medication Adverse Effects Considerations
SSRI Perinatal Syndrome Pulmonary Hypertension (0.3%)Autism Congenital heart defects
Most well-studied class in pregnancy Paroxetine: septal and atrial heart defects Sertraline preferred ACCEPTABLE
SNRI Perinatal Syndrome Venlafaxine increases BPACCEPTABLE
Bupropion Congenital heart defects Non-conclusive data RISK VS BENEFIT
Trazodone Congenital malformations Low risk Little evidenceRISK VS BENEFIT
Mirtazapine Congenital malformations Low risk Little evidenceRISK VS BENEFIT
Tricyclic Preterm birthNeonatal withdrawal
No clear association during pregnancyRISK VS BENEFIT
Monoamine Inhibitors
Structural teratogenisis Evidence of major malformationRequires dietary restrictions Multiple drug interactions NOT RECOMMENDED
Bar-Oz B, et al. Clin Ther. 2007;29:918-926. Wisner KL, et al. Pharmacological treatment of depression during pregnancy. JAMA. 1999;282:1264-9.
CDC Treating for Two: Safer Medication Use in Pregnancy.

10/1/2021
12
ANTIDEPRESSANTS
• Miscarriage • Miscarriage events occur at 10 weeks • Discontinuation of SSRI use 3 months prior to conception is associated
with 24% increase in miscarriage
• Spontaneous abortion • Risk is 7-11% with general population • Risk is 11-15% in patients on SSRIs, SNRIs, or TCAs• Higher with paroxetine and venlafaxine
• Conflicting data around congenital malformations • Recall and surveillance biases • Increased provider vigilance during examinations
• Most SSRIs have mixed results • Both positive and negative association studies • Highly confounded
Yonkers K, et al. Annu Rev Clin Psychol. 2014;10:369-392.Byatt N, et al. Acta Psychiatr Scand. 2013:127:94-114.
Anderson J, et al. Obstet Gynecol.2014;124:655-661.
ANTIDEPRESSANTS AND CARDIAC DEFECTS
• Study with 949,504 pregnant women found NO increase risk for any cardiac malformation when exposed to multiple types of antidepressants
• No significant associations between paroxetine and Right Ventricular Outflow Tract Obstruction (1.07, 95% CI 0.59 -1.93), or between sertraline and Ventral Septal Defects (1.04, 95% CI 0.76-1.41)
Adjusted Risk Ratio Cardiac Malformations
95% CI
SSRIs 1.06 0.93-1.22
TCAs 0.77 0.52-1.14
SNRIs 1.20 0.91-1.57
Other antidepressants 1.22 0.91-1.60
Bupropion 0.92 0.69-1.22
Huybrechts K, et al. N Engl J Med. 2014;370(25):2397-2407.

10/1/2021
13
ANTIDEPRESSANTS AND PRETERM BIRTH
• Antidepressant use typically shortens pregnancy 3-7 days
• 1% preterm deliveries are attributable to consistent use during 2nd trimester
• Risk factors: • Higher dose• Longer treatment periods • Choice of antidepressant • 2nd trimester use
Antidepressant Class Odds Ratio of Preterm Birth
TCA 2.36
SNRI 1.98
SSRI 1.46
Yonkers K, et al. Annu Rev Clin Psychol. 2014;10:369-392.Hayes R, et al. Am I Obstet Gynecol. 2012;207(1):49;e1-9.
ANTIDEPRESSANT DELAYED USE
• Postnatal adaption syndrome • Occurs in up to 30% of those with late pregnancy use of SSRIs • Common in third trimester • More evidence with paroxetine, fluoxetine, and venlafaxine
• Persistent pulmonary hypertension • Mixed data but longer or later exposure may increase risk and severity • Use SSRI after 20th week vs use SSRI before 20 weeks (OR 6.1)
• Neurodevelopment • SSRIs have no impact on global IQ, language, behavioral development• Maternal mental illness in utero is most important factor in development
of Autism Spectrum Disorder (OR 1.49 for depression)
Yonkers K, et al. Annu Rev Clin Psychol. 2014;10:369-392.Byatt N, et al. Acta Psychiatr Scand. 2013:127:94-114.

10/1/2021
14
PREGNANCY + ANXIETY
Medication Adverse Effects Considerations
Benzodiazepines Perinatal Syndrome Floppy infant syndrome Cleft lip Seizures Impaired temperature regulationHypotonicityFeeding difficulties Apnea
2.5-3.0 times more likely:• Require caesarian delivery • Ventilator support for baby
Diazepam: oral cleftAlprazolam, chlordiazepoxide: withdrawal NOT RECOMMENDED
Hydroxyzine Withdrawal Contraindicated NOT RECOMMENDED
Marijuana Low birth weight Same smoke consequences as tobacco on fetusNOT RECOMMENDED
Relcher C, et al. Obstet Med. 2015;8(4):168-171.Briggs GG, et al. Drugs in pregnancy and lactation: a reference guide to fetal and neonatal risk. 5th ed. Baltimore: Williams Wilkins, 1998.
Center for Disease Control and Prevention. Marijuana use in pregnancy.2021.
PREGNANCY + BIPOLAR DISORDER
Medication Adverse Effects Considerations
Lithium 1st Trimester: • Ebstein’s anomaly 3rd Trimester: • Perinatal syndrome• Hypoglycemia• Cardiac arrhythmias• Thyroid disorders• Floppy infant syndrome • Premature delivery • Neonatal lithium toxicity
Teratogenic Suspend 24-48 hours prior to delivery Therapeutic drug monitoring needed RISK VS BENEFIT
Valproic Acid 1st Trimester: • Fetal malformation (4%)Autism Decreased IQ
Teratogenic Contraindicated Clotting factor abnormalities in mother Last line medication in pregnancy NOT RECOMMENDED
Carbamazepine Malformations Malformation dose dependent Therapeutic drug monitoring needed NOT RECOMMENDED for bipolar
Lamotrigine Malformations not observed Therapeutic drug monitoring needed RISK VS BENEFIT
Grover s, et al. Indian J Psychiatry. 2015. 57(2):S308-S323.

10/1/2021
15
LITHIUM
• Lithium clearance changes during pregnancy and postpartum
• Dose Changes: • 2nd trimester: increased 30-50% and administered twice daily • Postpartum: Reduced in the days to weeks following delivery
• Recommendations • Monthly or twice monthly level recommended in pregnancy until week 34 • From week 34, weekly level monitoring recommended until delivery • Twice weekly level monitoring recommended for first 2 weeks postpartum • Levels desired at 0.5-1.2 mmol/L
Westin A, et al. BMJ Open.2017;7(3):e015738.Viguera A, et al. Am J Psychiatry. 2007;164(2):342-345.
PREGNANCY + SCHIZOPHRENIA
Medication Adverse Effect Recommendations
First Generation Antipsychotics:
Haloperidol Limb malformation Increase risk in 1st trimesterMonitoring every 3 months
ACCEPTABLE
Fluphenazine EPS Withdrawal
Increase risk during 3rd trimesterRISK VS BENEFIT
Chlorpromazine Jaundice Withdrawal
Increased risk in 3rd trimester ACCEPTABLE
Second Generation Antipsychotics: NOT RECOMMENDED Adverse Effects: - Increased risk during third trimester of withdrawal and EPS - Increased respiratory depression
Olanzapine Miscarriage Birth defects
Gestational diabetes NOT RECOMMENDED
Quetiapine Withdrawal Most commonACCEPTABLE
Risperidone Agenesis of corpus callosm More risk than others NOT RECOMMENDED
Kulkarni J, et al. Antipsychotic use in pregnancy. Expert Opin Pharmacother. 2015 Jun;16(9):1335-45.

10/1/2021
16
PATIENT CASE
• Kara is a 29 year old female with a PMH including bipolar disorder, anxiety, PTSD, alcohol use disorder, and type II diabetes.
• Her medications include: • Lithium 300 mg PO TID • Sertraline 50 mg PO daily• Quetiapine 400 mg PO HS • Hydroxyzine 10 mg PO TID prn • Trazodone 50 mg PO HS • Metformin 500 mg PO BID
Response:
• Discuss with Kara
• Risk vs Benefit • Lithium • Hydroxyzine • Trazodone • Metformin
• Continue• Sertraline • Quetiapine
Labs
Lithium level 0.9 mmol/L
Poels E, et al. Lithium during pregnancy and after delivery: a review. Int J Bipolar Disord 6, 26 (2018).
BACKGROUND
ADVERSE EFFECTS
PREGNANCY
BREASTFEEDING
ALTERNATIVE THERAPY

10/1/2021
17
PATIENT CASE
• Kara returns for advice, as she is now breastfeeding. She also complains that she has been feeling more depressed than usual. She has not restarted hydroxyzine or trazodone.
33
• Her medications include: • Lithium 300 mg BID • Sertraline 50 mg PO daily • Quetiapine 400 mg PO HS • Metformin 500 mg PO BID
Kara would like to know which medications will her baby be
exposed to and if her medications are still working.
BREASTFEEDING
• Psychiatric medications are indicated only when mental disorder left untreated outweighs risk of infant exposure in breast milk
• Relative infant dose (%) = dose received via breast milk (mg/kg/day) relative to mother’s dose (mg/kg/day), with >10% considered unsafe
• Considerations: • Timing of breastfeeding • Risk vs benefit of exposure• Percentage of exposure • Pumping
• Alternatives: • Formula • Psychotherapy • Change in dose and/or frequency
American College of Obstetricians and Gynecologists. Obstet Gynecol. 2018;132:e208-212.

10/1/2021
18
PHARMACOKINETIC DIFFERENCES POSTPARTUM
• Postpartum: • Rapid decline in sex steroid levels and renal filtration
– Allopregnalone specifically • Risk of adverse effects or toxicity due to dose adjustments
Orsolini L, et al. Hum Psychopharmacol.2015:30(1)4-20.Deligiannidis K, et al. J Clin Psychopharmacol. 2014;34(2):244-255.
Factors Impacting Excretion into Breast Milk
Medication Factors Maternal Factors
Degree of ionization pH gradient of maternal breast milk
Molecular weight CYP2D6 polymorphisms
Time to peak plasma + milk concentrations vs breastfeeding time
Concomitant medications
Blood protein binding Composition of fore and hind milk
Metabolites Cigarette smoking
BREASTFEEDING + DEPRESSION
Medication Class Excreted Considerations
SSRI Excreted Overall infant exposure low or negligibleParoxetine and sertraline: preferred at lowest dose Fluoxetine and citalopram: higher infant serum concentrations ACCEPTABLE
SNRI Excreted Overall infant exposure low or negligibleVenlafaxine: higher infant serum concentrations ACCEPTABLE
Bupropion Excreted Little evidence RISK VS BENEFIT
Trazodone Excreted Little evidence RISK VS BENEFIT
Mirtazapine Excreted Little evidence RISK VS BENEFIT
TCA Excreted Infant exposure low Imipramine or nortriptyline: First lineDoxepin: Avoid due to high infant concentration and sedationRISK VS BENEFIT
MAO inhibitors Uncertain Based on molecular size, most likely excreted RISK VS BENEFIT

10/1/2021
19
BREASTFEEDING + ANXIETY
Medication Excreted Considerations
Benzodiazepines Excreted Infant serum level low ACCEPTABLE Closely monitor baby if utilized • Sleepiness • Low energy • Weight loss • Poor suckling
Hydroxyzine Unknown May decrease prolactin production NOT RECOMMENDED Closely monitor baby if utilized• Drowsiness • Irritability
Cannabis Excreted THC stored in fat and slowly released over timeBaby still exposed even after marijuana cessation Conflicting evidence NOT RECOMMENDED
Colorado Department of Public Health and Environment. Monitoring Health Concerns Related to Marijuana in Colorado: 2014. (2015).
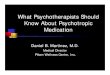
SAFETY SCORE
• Breastfed infant antidepressant safety index • (# infant AE) / (# healthy outcomes + # AEs) x 100 • < 2 = relatively safe during breastfeeding • 2.1-10 = use with great caution • >10 = contraindicated
• Psychotropic Medications:
Uguz F. J Clin Psychopharmcol. 2016;36(3):244-252.
BI-ASI
Sertraline = 0.68
Paroxetine = 0.95
Fluoxetine = 3.5
Citalopram = 5.3
Higher = safer Very low(<3)
Low(3.1-5)
Moderate(5.1-7)
Good (7.1-8.5)
Very good(8.6-10)
Aripiprazole Clozapine Doxepin Zolpidem
Haloperidol Risperidone Paliperidone Ziprasidone Bupropion Duloxetine Trazodone Lithium Diazepam Clonazepam oxazepam
Quetiapine Fluoxetine Escitalopram Venlafaxine Mirtazapine Amitriptyline Nortriptyline Valproic acid Lamotrigine Lorazepam Alprazolam
Olanzapine Citalopram Midazolam
Sertraline Paroxetine

10/1/2021
20
BREASTFEEDING + BIPOLAR DISORDER
Medication Excreted Adverse Effects Considerations
Lithium Excreted Hypotonia Hypothermia CyanosisEKG changes Lethargy
Infant serum level (10-50%) RISK VS BENEFIT
Depakote Excreted Hepatotoxicity Thrombocytopenia Anemia Jaundice
Infant serum levels do not correlate with motherNOT RECOMMENDED
Carbamazepine Excreted Respiratory depression Seizures Nausea/vomiting/diarrhea Decreased feeding Perinatal syndrome
Infant serum level (20-50%) Active metabolite Per guidelines, ACCEPTABLE for bipolar
Lamotrigine Excreted Apnea Drowsiness Poor sucking Thrombocytopenia Rash
Infant serum level (9%) ACCEPTABLE when infant serum level <10%
BREASTFEEDING + SCHIZOPHRENIA
Medication Excreted Adverse Effect Considerations
First Generation Antipsychotics
Haloperidol Excreted Galactorrhea Gynecomastia
RISK VS BENEFITUnless FGA is needed
Fluophenazine Excreted Increase prolactin Galactorrhea
Gynecomastia
NOT RECOMMENDED
Chlorpromazine Excreted Drowsiness Lethargy
NOT RECOMMENDED
Second Generation Antipsychotics - Lurasidone , asenapine, ziprasidone, risperidone (1.5-5% infant serum) - Monitor weekly for 1st month - Consider breastfeeding when concentration is lowest
Aripiprazole Excreted Lactation failure Appetite change
Insomnia
Infant serum level (8.3%) ACCEPTABLE
Clozapine Excreted AgranulocytosisSeizures
NOT RECOMMENDED
Olanzapine Excreted Metabolic side effects CYP1A2 metabolismInfant serum level (0.3-4%)
ACCEPTABLE
Quetiapine Excreted QTc prolongation Infant serum level (0.43%) ACCEPTABLE

10/1/2021
21
UPDATED EVIDENCE
• Lithium: • No longer absolute contraindication • No serious adverse effects observed:
– One infant dehydrated found with toxicity (level = 1.4 mEq/L) – One infant (10%) developed elevated TSH – Three infants (30%) developed elevations in SCr and BUN
• Antipsychotics• Limited data available • 37 reports in n = 206 infants exposed to SGAs
– Most exposure was olanzapine – Only 30 relative infant doses (RID) or milk/plasma ratios were
reported – Results:
• Low RID values for olanzapine, quetiapine, and ziprasidone • Moderate RID values for risperidone, paliperidone, and aripiprazole • All RID estimated < 5%
Poels EMP,et al. Int J Bipolar Disord. 2018;6-26. Uguz F. J Clin Psychopharmcol. 2016;36(3):244-252.
PATIENT EDUCATION
• Limit breast milk exposure with• Lowest effective dose • Use as few drugs as possible • Divided daily doses to avoid high peak serum levels
• Observe for signs and symptoms of toxicity • Behavioral changes • Poor hydration • Sedation • Hypotonia • Poor feeding and slow weight gain • Signs of hepatic impairment • Signs of hematological impairment
Bergink V, et al. Am K Psychiatry.2016;173(12):1179-1188.

10/1/2021
22
BACKGROUND
ADVERSE EFFECTS
PREGNANCY
BREASTFEEDING
POSTPARUM TREATMENT
POSTPARTUM DEPRESSION
• 70-80% of women experience “baby blues”
• Postpartum depression is experienced by 20% of new mothers
• 50% of women begin postpartum depression during pregnancy
• Facts • 10% postpartum cases result in suicide or infanticide • Treatment is 80% effective
• Risks• History of depression or anxiety • Family history of mental illness • Lower socioeconomic status• Diagnosis of Bipolar Disorder• Teen pregnancy • Difficulty becoming pregnant • Preterm baby or hospitalized baby • Twins or triplets
Kanes S, et al. Lancet. 2017;390:480-489.

10/1/2021
23
POSTPARTUM DEPRESSION TREATMENT
Lifestyle
Therapy
Medication
Lifestyle
Therapy
Medications
POSTPARTUM DEPRESSION MEDICATIONS
• Off-label Medication Options: • Sertraline • Fluoxetine
• FDA Approved Medications: • Brexanolone (Zulresso)
– MOA: Positive allosteric modulation of GABA-A receptors – Dose: 4200 mcg/kg IV over 60 minutes– Only available through specialty pharmacy + REMS program – Efficacy trials indicate decrease in HAMD-17 score at 24-84 hours
• Considerations: • Restart medications within first 24 hours after birth • Utilization of non-pharmacotherapy treatments
Meltzer-Brody S, et al. Lancet 2018:392; 1058-70.Kanes S, et al. Lancet. 2017;390:480-489.
Powell JG, et al. Brexanolone (Zulresso). Ann Pharmacother. 2020 Feb;54(2):157-163.

10/1/2021
24
PATIENT CASE
• Kara returns for advice, as she is now breastfeeding. She also complains that she has been feeling more depressed than usual. She has not restarted her previous medications.
• Her current medications include: • Lithium 300 mg PO BID• Sertraline 50 mg PO daily • Quetiapine 400 mg PO daily • Metformin 500 mg PO BID
Kara would like to know which medications will her baby be
exposed to and if her medications are still working.
Response:Counsel Kara on baby blues and discuss risk vs benefit for each medication.
• Exposed to: • Lithium • Sertraline • Quetiapine• Metformin
SUMMARY
48

10/1/2021
25
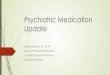
SUMMARY
First Trimester Second Trimester
Third Trimester Breastfeeding Postpartum
SSRI ✔Paroxetine
✔Paroxetine
✔Paroxetine
✔Fluoxetine Paroxetine
✔
SNRI ✔Venlafaxine
✔Venlafaxine
✔Venlafaxine
✔Venlafaxine
✔
TCA X X X ✔Doxepin
MAOI X X X X
Benzodiazepines X X X ✔Antipsychotics
Quetiapine
XHaloperidolQuetiapine
XHaloperidolQuetiapine
XOlanzapineQuetiapineAripiprazole
✔
Mood StabilizersLamotrigine Valproic acid
✔
CONCLUSION AND CLINICAL PEARLS
• Pregnant • Fetus risk to medication exposure vs mother with poor mental health• SSRIs require a second or third trimester dose increase • Close clinical and pharmacokinetic monitoring recommended
• Depression: • AVOID: paroxetine, fluoxetine, venlafaxine, and MAOI • Preferred: sertraline
– Anxiety: • AVOID: benzodiazepines, marijuana, hydroxyzine
– Bipolar Disorder: • AVOID: valproic acid, carbamazepine
– Schizophrenia: • AVOID: Most • Preferred: quetiapine

10/1/2021
26
CONCLUSION AND CLINICAL PEARLS
• Breastfeeding • All psychiatric medications are excreted into the breastmilk • Recommended use if infant serum level <5-10% attainable
– Depression: • AVOID: citalopram, fluoxetine, venlafaxine, and MAOI • Preferred: paroxetine, sertraline
– Anxiety: • AVOID: marijuana, hydroxyzine
– Bipolar Disorder: • AVOID: valproic acid
– Schizophrenia: • AVOID: first generation antipsychotics
POST-ASSESSMENT QUESTION 1
JN is a pregnant patient on ziprasidone and escitalopram who has struggled with conception for years. Due to this difficulty, she is worried about the impact of medications on her baby. In research studies, which impact on infants has been found to be most associated with in utero antidepressant exposure?
• Spontaneous abortion with 3rd trimester antidepressant use• Reduced gestational time with 2nd trimester antidepressant use • Persistent pulmonary hypertension with any antidepressant use • Postnatal adaption syndrome with 1st trimester antidepressant use
52

10/1/2021
27
POST-ASSESSMENT QUESTION 2
After discussing the risks of untreated depression with JN, you begin to consider the role of pharmacotherapy in JN’s perinatal depression. Considering what is known about JN, and any known risk factors, which statement describes the most likely impact of antidepressant therapy in JN?
• Conversion to manic episode• Risk of psychosis or infanticide • Possible postpartum hemorrhage • Development of gestational hypertension
53
POST-ASSESSMENT QUESTION 3
Based on the adverse effects of ziprasidone, what side effect could have added to JN’s struggle in conceiving? Which of the following would be most important to monitor for a patient taking this medication?
• Weight loss • Hyperprolactemia• Akathisia• QTc prolongation
54

10/1/2021
28
ADDITIONAL RESOURCES
• https://www.cdc.gov/pregnancy /meds/treatingforwo/facts.html
• https://womensmentalhealth.org/specialty-clinics/psychiatric -disorders-during-pregnancy/
• http://www.motherrisk.org/
REFERENCES
• Committee Opinion Number 757. American College of Obstetrician and Gynecologists. Obstet Gynecol. 2018;132:e208‐12. • Massachusetts General Hospital. Center for Women’s Mental Health• Am Fam Physician. 2008 Sep 15;78(6):772‐778.• Cohen L, et al. JAMA. 2006;295(5):499‐507• Ward R, et al. Am Fam Physician. 2002 .66(4):629‐637.• Grote N, et al. Arch Gen Psychiatry. 2010;67(10):1012‐1024. • American College of Obstetricians and Gynecologists: Yonkers K, et al. Obstet Gynecol. 2009;114(3)703‐713.• Deligiannidis K, et al. J Clin Psychopharmacol. 2014;34(2):244‐255.• Bar‐Oz B, et al. Clin Ther. 2007;29:918‐926. • Wisner KL, et al. Pharmacological treatment of depression during pregnancy. JAMA. 1999;282:1264‐9.• CDC Treating for Two: Safer Medication Use in Pregnancy. • Yonkers K, et al. Annu Rev Clin Psychol. 2014;10:369‐392.• Anderson J, et al. Obstet Gynecol.2014;124:655‐661.• Huybrechts K, et al. N Engl J Med. 2014;370(25):2397‐2407.• Relcher C, et al. Obstet Med. 2015;8(4):168‐171.• Briggs GG, et al. Drugs in pregnancy and lactation: a reference guide to fetal and neonatal risk. 5th ed. Baltimore: Williams Wilkins, 1998.• Grover s, et al. Indian J Psychiatry. 2015. 57(2):S308‐S323. • Westin A, et al. BMJ Open.2017;7(3):e015738.• Viguera A, et al. Am J Psychiatry. 2007;164(2):342‐345.• Kulkarni J, et al. Antipsychotic use in pregnancy. Expert Opin Pharmacother. 2015 Jun;16(9):1335‐45. • Poels E, et al. Lithium during pregnancy and after delivery: a review. Int J Bipolar Disord 6, 26 (2018).• Orsolini L, et al. Hum Psychopharmacol.2015:30(1)4‐20.• Uguz E. Am J Ther. 2019. • Colorado Department of Public Health and Environment. Monitoring Health Concerns Related to Marijuana in Colorado: 2014. (2015).• Kanes S, et al. Lancet. 2017;390:480‐489.• Meltzer‐Brody S, et al. Lancet 2018:392; 1058‐70.• Powell JG, et al. Brexanolone (Zulresso). Ann Pharmacother. 2020 Feb;54(2):157‐163.

10/1/2021
29
PSYCHIATRIC MEDICATION IN PREGNANT AND BREASTFEEDING WOMEN
Madison Holbrook, Pharm.D.
PGY-2 Psychiatry Pharmacy Resident
Laureate Psychiatric Clinic and Hospital
Oklahoma Society of Health System Pharmacist Meeting
October 22, 2021