Embed Size (px)
Citation preview
Huntington’s
Disease Iain Conlon / D00128197

Decleration
I hereby declare that the project work entitled “Huntington’s Disease” submitted to the Dundalk Institute of
Technology, is a record of an original work done by me, Iain Conlon, under the guidance of Sinead
Loughran, Faculty Member, Faculty of Science, Dundalk Institute of Technology, and this project work has
not performed the basis for the award of any Degree or diploma and similar project if any.
Acknowledgements
I would like to thank my original mentor, Dr. Sinead Loughran, for all the help and support she has given
me throughout the process of writing this literature review. I would also like to thank Ronan Bree for his
informative lectures with regard to researching for, writing and presenting literature reviews throughout the
semester. Finally, I want to thank Dr. Gillian Lambe for taking me as her protégé and in advance for
reviewing and correcting my work.
Contents Introduction ............................................................................................................................................. 3
What is Huntington’s Disease? ........................................................................................................... 3
Symptoms of Huntington’s disease ..................................................................................................... 3
Chorea ............................................................................................................................................. 3
Depression ....................................................................................................................................... 3
Neuropsychiatric symptoms ............................................................................................................ 4
Impaired cognitive ability ............................................................................................................... 4
Diagnosis and Diagnostic procedures ................................................................................................. 4
The brain, medium spiny neurons and GABA ........................................................................................ 4
Pathophysiology ...................................................................................................................................... 4
Overview ............................................................................................................................................. 4
Htt and mHtt ....................................................................................................................................... 5
Age and Huntington’s disease ............................................................................................................. 5
Potential pathophysiological pathways ............................................................................................... 6
Overview ......................................................................................................................................... 6
mHtt protein aggregation ................................................................................................................ 6
Transcription ................................................................................................................................... 7
Apoptosis and Mitochondrial involvement ..................................................................................... 7
Other possible causes ...................................................................................................................... 8
Treatment ................................................................................................................................................ 8
Overview ............................................................................................................................................. 8
Neuroleptics ........................................................................................................................................ 8
Dopamine depleters ............................................................................................................................ 8
Antidepressants ................................................................................................................................... 9
Therapeutic treatment ......................................................................................................................... 9
Latest advances ................................................................................................................................... 9
Conclusion .............................................................................................................................................. 9
Bibliography ......................................................................................... Error! Bookmark not defined.

Huntington’s disease (HD) is an autosomal dominant, neurodegenerative disease. The disease causes chorea,
decrease in cognitive ability, neuropsychiatric symptoms and other symptoms. It can be detected using genetic
tests. It is caused by an abnormality on the Huntingtin gene which causes a polyglutamine (polyQ) of over 35 to
be created on the Huntingtin protein, in affect, creating mutant Huntingtin protein, or mHtt. The length of the
polyQ repeat length seems to affect the age of onset of HD. This mutant huntingtin protein is thought to cause
specific neurodegeneration of striatal medium spiny neurons (MSN). It is not known exactly how the mHtt may
affect the MSNs but there are many theories of possible pathophysiological pathways. mHtt aggregation is
thought to have a major affect on its toxicity to MSNs, whilst the mHtt interactions with apoptotic and
translation proteins may also be the root of the toxicity. mHtt may have an affect on the mitochondria to cause
an apoptotic pathway. As there’s no known cause to the disease, the main treatments to the disease are
symptomatic ie. treating chorea, depression and cognitive impairments. However, studies on prions disease
show that neurodegeneration can be completely stopped with the use of a drug called PERK. This may
translate to provide a basis on how to prevent the HD neurodegeration. In this piece, all aspects of HD are
reviewed with concentration on the possible pathophysiological pathways.
Introduction
What is Huntington’s Disease?
Huntington’s disease (HD) is a hereditary
neurodegenerative disease (Kent, 2004). HD is
autosomal dominant ie. if a father in a family has it but
the mother does not, any child of the two will have a
50% chance of getting the disease. The disease was
first described by George Huntington, in 1872, as
Huntington’s Chorea, due to the observation one of the
main symptoms, chorea, in his patients (Adam &
Jankovic, 2008). Some other symptoms associated
with HD, aside from chorea, are impaired cognitive
ability, depression, dementia and other motor function
impairments (Stanley, 2009).
HD is caused by a defect in the Huntington
gene, located on the short arm of chromosome 4
(Adam & Jankovic, 2008). This defect is an unusually
large amount of polyglutamine, CAG triplet, repeats
(Ross & Tabrizi, 2011). This unusual amount of
polyglutamine repeats always results in the creation of
the mutant Huntingtin protein, mHtt, that somehow has
a toxic effect on the brain, and specifically, medium
spiny neurons (Damiano et al., 2010). It is not known
exactly how, or if, the mutant Huntingtin protein is
neurotoxic but there is much research on the subject of
Huntington’s pathophysiology happening at the
moment, and some ideas will be discussed in this
paper.
HD is not very prevalent when it is compared
to other diseases as it only happens in every 4 – 8
persons in every 100’000. Other neurodegenerative
diseases are a lot more common. Its onset usually
occurs in adults around 35 – 45 years of age (Ross &
Tabrizi, 2011), however the age of onset of symptoms
correlates with the amount polyglutamine repeats
present (Chen, Ferrone & Wetzel, 2002). Death usually
occurs about 15 – 20 years after onset of symptoms
(Ross & Tabrizi, 2011). Death usually happens by the
HD sufferer falling. There is no known cure for HD
but there are many drugs and treatments that can help
the different symptoms of the disease (Adam &
Jankovic, 2008).
Symptoms of Huntington’s disease
There are many different symptoms that are associated
with HD. There are three different types of symptoms
involved with HD; Physical (mainly motor), emotional
and cognitive symptoms (Stanley, 2009). Below are
the main 3 studies symptoms of HD.
Chorea
Chorea is a symptom in which the body makes
uncontrollable “jerky” movements (Stroke, 2010). It
seems to be the most common symptom associated
with HD The disease was originally called
Huntington’s Chorea due to these involuntary
movements looking like a dance (Cha, 2000). Natually,
chorea progressively gets worse as the disease
progress’. These movements are mainly seen in the
trunk, legs, arms and face of HD sufferers. HD causes
death of medium spiny neurons and as they are
GABAergic (GABA secreting) neurons, this results in
a decrease in GABA activity in the body, causes these
movements (Boecker, 2013).
Depression
Depression also seems to be a common emotional
symptom caused by HD. Depression is known to lead
suicidality. There may be a higher rate of suicide in
HD person than in a non HD person (Hubers et al.,
2012). Although, a depressed mood might be due to
HD itself, actual depression might not actually be a
symptom of HD (Fiedorowicz et al., 2011). A history
of depression, or attempted suicide, may make a
person with HD more likely to be suicidal during HD
(Fiedorowicz et al., 2011). Interestingly, a study done
mentioned that 25% of the people in the study with HD
had attempted suicide (Walker, 2007).
This worsened suicidal behaviour may be due to
having to deal with other symptoms associated with
HD.
Neuropsychiatric symptoms
Neuropsychiatric symptoms in HD are very prevalent
(Paulson et al.,2001). The most common of them are
dysphoria, agitation and irritability, whilst apathy and
anxiety are also present in more than 50% of HD
sufferers (see table 1) (Paulson et al., 2001).
Table 1: Study done by Paulsen et al.(2001) regarding
neuropsychiatric symptoms on HD sufferers.
NPI Scale Frequency* Mean SD
Dysphoria 69.2 3.12 3.46
Agitation 67.3 2.88 3.32
Irritability 65.4 2.63 3.11
Apathy 55.8 2.79 4.02
Anxiety 51.9 1.96 3.14
Disinhibition 34.6 1.29 2.77
Euphoria 30.8 1.04 2.27
Delusions 11.5 0.75 2.63
Abberant motor 9.6 0.60 2.18
Hallucinations 1.9 0.23 1.66
N = 52; NPI = Neuropsychiatric inventory; *percent of
patients with an NPI score ≥1;
Most of the symptoms shown above can be treated
specifically.
Impaired cognitive ability
The problems with cognitive ability start to begin
before the onset of motor problems, like chorea
(Milnerwood & Raymond, 2010). These cognitive
symptoms presents a difficulty to the HD sufferer from
understanding people, learning, using memory to
attention keeping. Cognitive ability is usually in steady
decline as the disease progresses and can eventually
lead to a HD sufferer forgetting their family and
friends.
Diagnosis and Diagnostic procedures
There a number of ways to test if a person is positive
for having HD. Brain imaging, such as fMRI and PET
scans, can show volume and appearance differences in
the brains striatum caused by the disease (Reviewed in
Walker, 2007). Family history of the disease is also a
good indicator as to whether a person may have it. The
most effective test that can be done is the genetic test,
which tests for the mutant Huntingtin allele (Reviewed
in Walker, 2007). This test, however, can be cost
effective like many other genetic tests. Other tests that
can be done are tests for chorea and cognitive ability or
impairment.
The brain, medium spiny neurons and
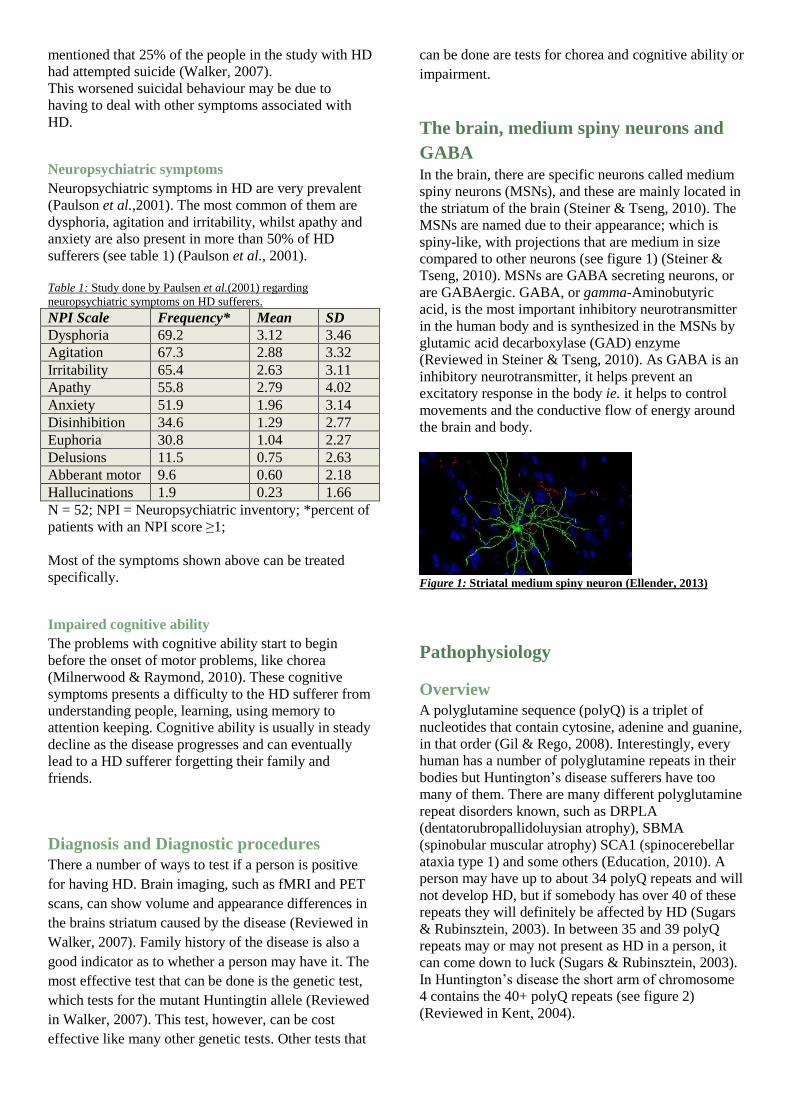
GABA In the brain, there are specific neurons called medium
spiny neurons (MSNs), and these are mainly located in
the striatum of the brain (Steiner & Tseng, 2010). The
MSNs are named due to their appearance; which is
spiny-like, with projections that are medium in size
compared to other neurons (see figure 1) (Steiner &
Tseng, 2010). MSNs are GABA secreting neurons, or
are GABAergic. GABA, or gamma-Aminobutyric
acid, is the most important inhibitory neurotransmitter
in the human body and is synthesized in the MSNs by
glutamic acid decarboxylase (GAD) enzyme
(Reviewed in Steiner & Tseng, 2010). As GABA is an
inhibitory neurotransmitter, it helps prevent an
excitatory response in the body ie. it helps to control
movements and the conductive flow of energy around
the brain and body.
Figure 1: Striatal medium spiny neuron (Ellender, 2013)
Pathophysiology
Overview
A polyglutamine sequence (polyQ) is a triplet of
nucleotides that contain cytosine, adenine and guanine,
in that order (Gil & Rego, 2008). Interestingly, every
human has a number of polyglutamine repeats in their
bodies but Huntington’s disease sufferers have too
many of them. There are many different polyglutamine
repeat disorders known, such as DRPLA
(dentatorubropallidoluysian atrophy), SBMA
(spinobular muscular atrophy) SCA1 (spinocerebellar
ataxia type 1) and some others (Education, 2010). A
person may have up to about 34 polyQ repeats and will
not develop HD, but if somebody has over 40 of these
repeats they will definitely be affected by HD (Sugars
& Rubinsztein, 2003). In between 35 and 39 polyQ
repeats may or may not present as HD in a person, it
can come down to luck (Sugars & Rubinsztein, 2003).
In Huntington’s disease the short arm of chromosome
4 contains the 40+ polyQ repeats (see figure 2)
(Reviewed in Kent, 2004).
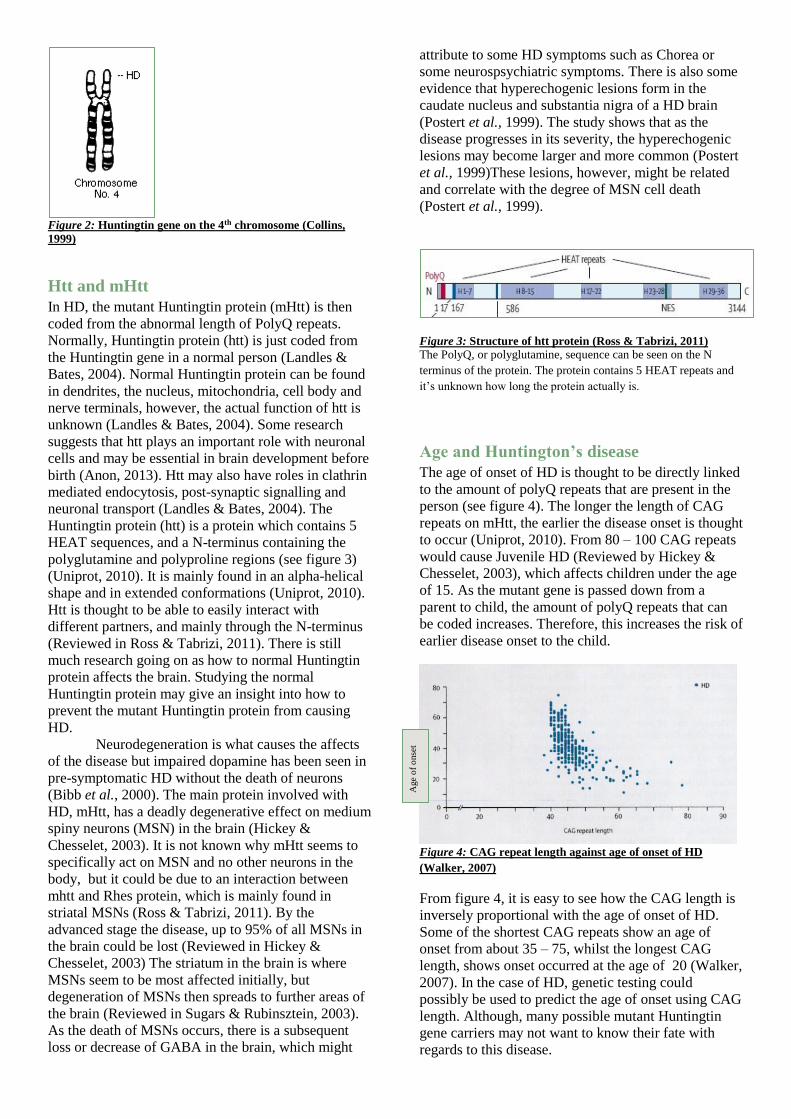
Figure 2: Huntingtin gene on the 4th chromosome (Collins,
1999)
Htt and mHtt
In HD, the mutant Huntingtin protein (mHtt) is then
coded from the abnormal length of PolyQ repeats.
Normally, Huntingtin protein (htt) is just coded from
the Huntingtin gene in a normal person (Landles &
Bates, 2004). Normal Huntingtin protein can be found
in dendrites, the nucleus, mitochondria, cell body and
nerve terminals, however, the actual function of htt is
unknown (Landles & Bates, 2004). Some research
suggests that htt plays an important role with neuronal
cells and may be essential in brain development before
birth (Anon, 2013). Htt may also have roles in clathrin
mediated endocytosis, post-synaptic signalling and
neuronal transport (Landles & Bates, 2004). The
Huntingtin protein (htt) is a protein which contains 5
HEAT sequences, and a N-terminus containing the
polyglutamine and polyproline regions (see figure 3)
(Uniprot, 2010). It is mainly found in an alpha-helical
shape and in extended conformations (Uniprot, 2010).
Htt is thought to be able to easily interact with
different partners, and mainly through the N-terminus
(Reviewed in Ross & Tabrizi, 2011). There is still
much research going on as how to normal Huntingtin
protein affects the brain. Studying the normal
Huntingtin protein may give an insight into how to
prevent the mutant Huntingtin protein from causing
HD.
Neurodegeneration is what causes the affects
of the disease but impaired dopamine has been seen in
pre-symptomatic HD without the death of neurons
(Bibb et al., 2000). The main protein involved with
HD, mHtt, has a deadly degenerative effect on medium
spiny neurons (MSN) in the brain (Hickey &
Chesselet, 2003). It is not known why mHtt seems to
specifically act on MSN and no other neurons in the
body, but it could be due to an interaction between
mhtt and Rhes protein, which is mainly found in
striatal MSNs (Ross & Tabrizi, 2011). By the
advanced stage the disease, up to 95% of all MSNs in
the brain could be lost (Reviewed in Hickey &
Chesselet, 2003) The striatum in the brain is where
MSNs seem to be most affected initially, but
degeneration of MSNs then spreads to further areas of
the brain (Reviewed in Sugars & Rubinsztein, 2003).
As the death of MSNs occurs, there is a subsequent
loss or decrease of GABA in the brain, which might
attribute to some HD symptoms such as Chorea or
some neurospsychiatric symptoms. There is also some
evidence that hyperechogenic lesions form in the
caudate nucleus and substantia nigra of a HD brain
(Postert et al., 1999). The study shows that as the
disease progresses in its severity, the hyperechogenic
lesions may become larger and more common (Postert
et al., 1999)These lesions, however, might be related
and correlate with the degree of MSN cell death
(Postert et al., 1999).
Figure 3: Structure of htt protein (Ross & Tabrizi, 2011)
The PolyQ, or polyglutamine, sequence can be seen on the N
terminus of the protein. The protein contains 5 HEAT repeats and
it’s unknown how long the protein actually is.
Age and Huntington’s disease
The age of onset of HD is thought to be directly linked
to the amount of polyQ repeats that are present in the
person (see figure 4). The longer the length of CAG
repeats on mHtt, the earlier the disease onset is thought
to occur (Uniprot, 2010). From 80 – 100 CAG repeats
would cause Juvenile HD (Reviewed by Hickey &
Chesselet, 2003), which affects children under the age
of 15. As the mutant gene is passed down from a
parent to child, the amount of polyQ repeats that can
be coded increases. Therefore, this increases the risk of
earlier disease onset to the child.
Figure 4: CAG repeat length against age of onset of HD
(Walker, 2007)
From figure 4, it is easy to see how the CAG length is
inversely proportional with the age of onset of HD.
Some of the shortest CAG repeats show an age of
onset from about 35 – 75, whilst the longest CAG
length, shows onset occurred at the age of 20 (Walker,
2007). In the case of HD, genetic testing could
possibly be used to predict the age of onset using CAG
length. Although, many possible mutant Huntingtin
gene carriers may not want to know their fate with
regards to this disease.
Age
of
onse
t
Potential pathophysiological pathways
Overview
There are many theories of ways in which the mutant
Huntingtin protein may have a neurodegenerative
affect on medium spiny neurons of the striatum. Since
the htt gene was found back in 1993 (Huntington’s
Disease Collaborative Research Group, 1993), much
research was done into the possible pathophysiology of
the Huntingtin protein after it is coded. It is possible
that the protein may affect apoptosis, functions of the
mitochondria, transcription and other cellular
processes, but one of the most common ideas in the
theories is that the mHtt clump together to form
aggregates (Chen, Ferrone & Wetzel, 2002; Truant et
al., 2008; Bates, 2003; Bocharova et al., 2009).
There are a few different model systems that
can be used by scientists when they are trying to
determine how mHtt may affect cells (Ross & Tabrizi,
2011). Cell models, which can derived from patients
with Huntington’s disease, are good in-vitro models
due to their ability to act similar to neurons in the body
(Ross & Tabrizi, 2011). Mouse models are one of the
most commonly used models. They offer a decent way
of obtaining changes in behaviour in the test subject,
which obviously can not be done on any in-vitro
models. The phenotypes of the disease can be seen
very quickly after infection (Ross & Tabrizi, 2011).
Yeast models, invertebrate models and other
mammalian models are also used (Bocharova, Chave-
Cox, Sokolov, et al., 2009; Ross & Tabrizi, 2011).
mHtt protein aggregation
In most studies, aggregation of mHtt seems to be a
common theme. Bates (2003) believes that it may be
the centre of the pathophysiological pathway of the
disease and that aggregation is the basis of MSN
degeneration in the disease in some way. Aggregation
of the proteins only seems to occur with Huntingtin
proteins containing at least 36 polyQ repeats (ie.
mutant Huntingtin protein) and any proteins with less
than 36 polyQ repeats do not seem to aggregate, so
they do not form any possibly toxic structures
(Reviewed in Truant et al., 2008). Proof of this was
found when insertion of long polyQ repeats was added
to a gene, aggregates were subsequently formed
(Reviewed in Hickey & Chesselet, 2003). Aggregation
seems to happen because of a hydrophobic interaction
on the N-terminus of the mHtt proteins (Ross &
Tabrizi, 2011). It is hypothesised that these
interactions could be targeted as a way of preventing
aggregation, and therefore possibly preventing the
disease (Ross & Tabrizi, 2011). Aggregation
inhibitors, such as sulfobenzoic acid derivatives, could
aid in prevention of aggregation. However, the actual
creation method of the aggregates is not fully
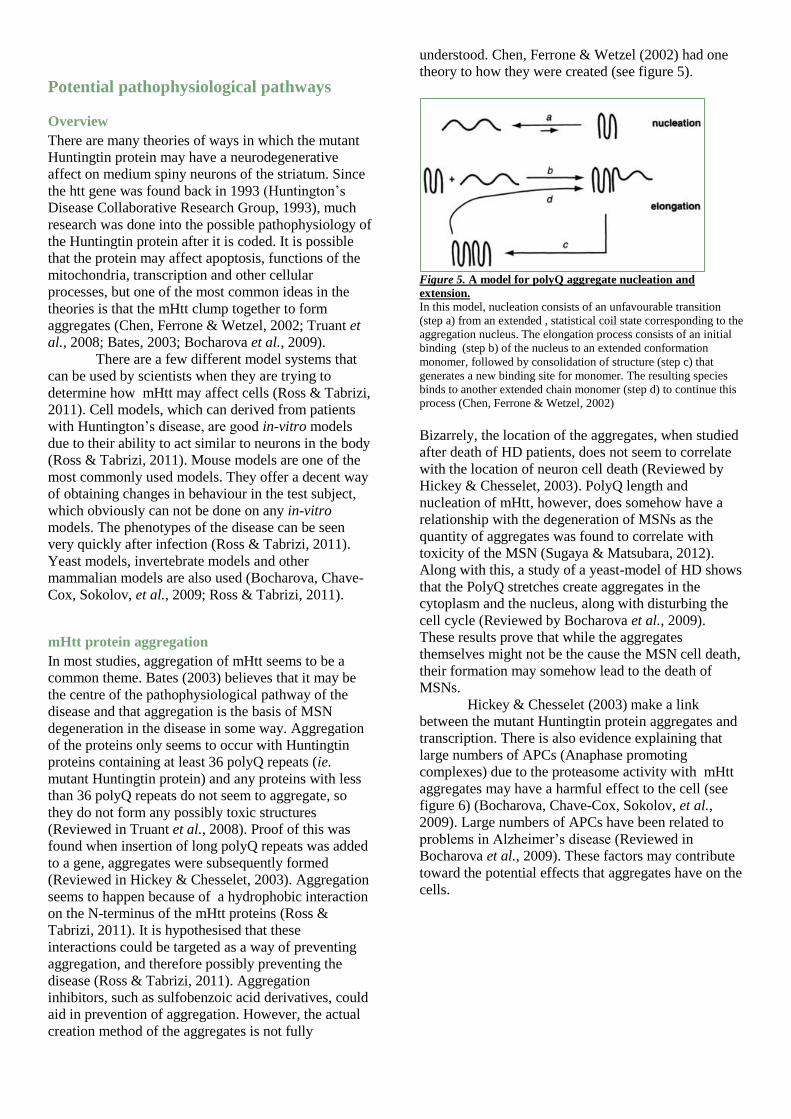
understood. Chen, Ferrone & Wetzel (2002) had one
theory to how they were created (see figure 5).
Figure 5. A model for polyQ aggregate nucleation and
extension.
In this model, nucleation consists of an unfavourable transition
(step a) from an extended , statistical coil state corresponding to the
aggregation nucleus. The elongation process consists of an initial
binding (step b) of the nucleus to an extended conformation
monomer, followed by consolidation of structure (step c) that
generates a new binding site for monomer. The resulting species
binds to another extended chain monomer (step d) to continue this
process (Chen, Ferrone & Wetzel, 2002)
Bizarrely, the location of the aggregates, when studied
after death of HD patients, does not seem to correlate
with the location of neuron cell death (Reviewed by
Hickey & Chesselet, 2003). PolyQ length and
nucleation of mHtt, however, does somehow have a
relationship with the degeneration of MSNs as the
quantity of aggregates was found to correlate with
toxicity of the MSN (Sugaya & Matsubara, 2012).
Along with this, a study of a yeast-model of HD shows
that the PolyQ stretches create aggregates in the
cytoplasm and the nucleus, along with disturbing the
cell cycle (Reviewed by Bocharova et al., 2009).
These results prove that while the aggregates
themselves might not be the cause the MSN cell death,
their formation may somehow lead to the death of
MSNs.
Hickey & Chesselet (2003) make a link
between the mutant Huntingtin protein aggregates and
transcription. There is also evidence explaining that
large numbers of APCs (Anaphase promoting
complexes) due to the proteasome activity with mHtt
aggregates may have a harmful effect to the cell (see
figure 6) (Bocharova, Chave-Cox, Sokolov, et al.,
2009). Large numbers of APCs have been related to
problems in Alzheimer’s disease (Reviewed in
Bocharova et al., 2009). These factors may contribute
toward the potential effects that aggregates have on the
cells.
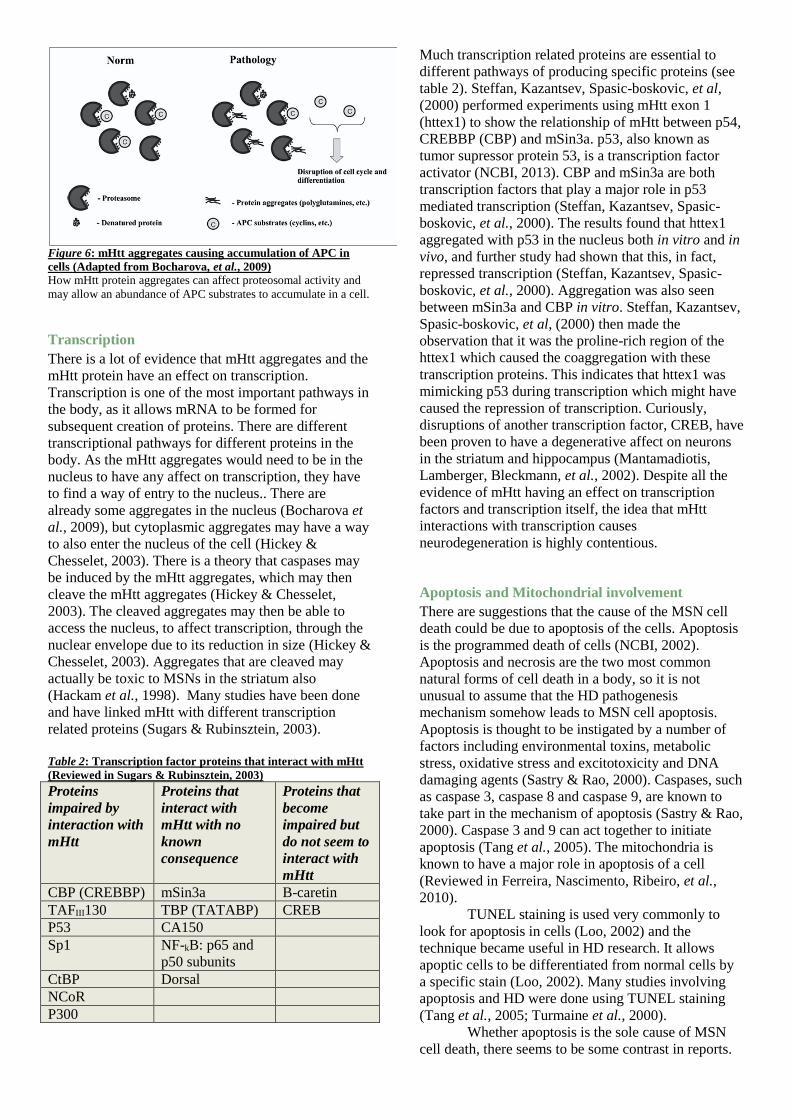
Figure 6: mHtt aggregates causing accumulation of APC in
cells (Adapted from Bocharova, et al., 2009)
How mHtt protein aggregates can affect proteosomal activity and
may allow an abundance of APC substrates to accumulate in a cell.
Transcription
There is a lot of evidence that mHtt aggregates and the
mHtt protein have an effect on transcription.
Transcription is one of the most important pathways in
the body, as it allows mRNA to be formed for
subsequent creation of proteins. There are different
transcriptional pathways for different proteins in the
body. As the mHtt aggregates would need to be in the
nucleus to have any affect on transcription, they have
to find a way of entry to the nucleus.. There are
already some aggregates in the nucleus (Bocharova et
al., 2009), but cytoplasmic aggregates may have a way
to also enter the nucleus of the cell (Hickey &
Chesselet, 2003). There is a theory that caspases may
be induced by the mHtt aggregates, which may then
cleave the mHtt aggregates (Hickey & Chesselet,
2003). The cleaved aggregates may then be able to
access the nucleus, to affect transcription, through the
nuclear envelope due to its reduction in size (Hickey &
Chesselet, 2003). Aggregates that are cleaved may
actually be toxic to MSNs in the striatum also
(Hackam et al., 1998). Many studies have been done
and have linked mHtt with different transcription
related proteins (Sugars & Rubinsztein, 2003).
Table 2: Transcription factor proteins that interact with mHtt
(Reviewed in Sugars & Rubinsztein, 2003)
Proteins
impaired by
interaction with
mHtt
Proteins that
interact with
mHtt with no
known
consequence
Proteins that
become
impaired but
do not seem to
interact with
mHtt
CBP (CREBBP) mSin3a B-caretin
TAFIII130 TBP (TATABP) CREB
P53 CA150
Sp1 NF-kB: p65 and
p50 subunits
CtBP Dorsal
NCoR
P300
Much transcription related proteins are essential to
different pathways of producing specific proteins (see
table 2). Steffan, Kazantsev, Spasic-boskovic, et al,
(2000) performed experiments using mHtt exon 1
(httex1) to show the relationship of mHtt between p54,
CREBBP (CBP) and mSin3a. p53, also known as
tumor supressor protein 53, is a transcription factor
activator (NCBI, 2013). CBP and mSin3a are both
transcription factors that play a major role in p53
mediated transcription (Steffan, Kazantsev, Spasic-
boskovic, et al., 2000). The results found that httex1
aggregated with p53 in the nucleus both in vitro and in
vivo, and further study had shown that this, in fact,
repressed transcription (Steffan, Kazantsev, Spasic-
boskovic, et al., 2000). Aggregation was also seen
between mSin3a and CBP in vitro. Steffan, Kazantsev,
Spasic-boskovic, et al, (2000) then made the
observation that it was the proline-rich region of the
httex1 which caused the coaggregation with these
transcription proteins. This indicates that httex1 was
mimicking p53 during transcription which might have
caused the repression of transcription. Curiously,
disruptions of another transcription factor, CREB, have
been proven to have a degenerative affect on neurons
in the striatum and hippocampus (Mantamadiotis,
Lamberger, Bleckmann, et al., 2002). Despite all the
evidence of mHtt having an effect on transcription
factors and transcription itself, the idea that mHtt
interactions with transcription causes
neurodegeneration is highly contentious.
Apoptosis and Mitochondrial involvement
There are suggestions that the cause of the MSN cell
death could be due to apoptosis of the cells. Apoptosis
is the programmed death of cells (NCBI, 2002).
Apoptosis and necrosis are the two most common
natural forms of cell death in a body, so it is not
unusual to assume that the HD pathogenesis
mechanism somehow leads to MSN cell apoptosis.
Apoptosis is thought to be instigated by a number of
factors including environmental toxins, metabolic
stress, oxidative stress and excitotoxicity and DNA
damaging agents (Sastry & Rao, 2000). Caspases, such
as caspase 3, caspase 8 and caspase 9, are known to
take part in the mechanism of apoptosis (Sastry & Rao,
2000). Caspase 3 and 9 can act together to initiate
apoptosis (Tang et al., 2005). The mitochondria is
known to have a major role in apoptosis of a cell
(Reviewed in Ferreira, Nascimento, Ribeiro, et al.,
2010).
TUNEL staining is used very commonly to
look for apoptosis in cells (Loo, 2002) and the
technique became useful in HD research. It allows
apoptic cells to be differentiated from normal cells by
a specific stain (Loo, 2002). Many studies involving
apoptosis and HD were done using TUNEL staining
(Tang et al., 2005; Turmaine et al., 2000).
Whether apoptosis is the sole cause of MSN
cell death, there seems to be some contrast in reports.

TUNEL positive, or apoptotic cells, can be present in
HD (Tang et al., 2005). In vitro models of HD have
seen apoptotic cell death in these experiments (Tang,
Slow, Lupu, et al., 2005). It is thought that it may be
glutamate induced apoptosis that causes the MSN cell
death (Tang, Slow, Lupu, et al., 2005). Tang, Slow,
Lupu, et al., (2005) suggest that the mHtt has an affect
on Ca2+ signalling and that leads to the apoptic
mechanism. The proposed mechanism of this
happening is that glutamate stimulates NR1 / NR2B
NMDAR and mGluR5 receptors in the MSNs, and
then the activation of these receptors allows the release
of Ca2+ and InsP3 (inositol triphosphate) from InsP3R
(inositol triphosphate receptor). The mHtt exon would
affect the Ca2+ signalling by making InsP3R1 more
sensitive to InsP3, allowing more NR1 / NR2B
NMDAR, which then causes the mitochondria to take
in more Ca2+ that it can actually hold (Fig. 7). When
the amount of Ca2+ goes past its limit in the
mitochondria, cytochrome c is subsequently released
(Fig. 7) (Tang et al., 2005). Cytochrome c can then
activate caspases (Uniprot, 2007), such as caspase 9
and caspase 3, which in turn, activates the mechanism
of apoptosis (Fig. 7)(Tang, Slow, Lupu, et al., 2005).
This hypothesis would be very plausible because it
also explains the reason for selective
neurodegeneration of MSN as NR1 / NR2B NMDAR
and mGluR5 receptors are present mainly in MSN
(Reviewed in Tang et al., 2005). Conflictingly, a
study done by Ferreira et al., (2010) indicates that it is
not cytochrome c that is involved with the
degeneration process, but AIF (apoptosis inducing
factor) and there may be a degenerative process
involving it.
Figure 7: Hypothesised mechanism for to cause apoptosis to
occur in MSNs (Tang et al., 2005)
Contrary to these studies done indicating that apoptosis
causes neurogeneration of MSN, a study was done
using in vivo and in vitro models of HD, which
indicated that apoptosis was not the cause of cell death
in HD (Turmaine et al., 2000). Turmaine et al., (2000)
used TUNEL staining to try and identify apoptotic
cells but no cells were seen as TUNEL positive. As
well as this, no fragmentation of the nucleus and
cytoplasm; or apoptotic bodies were found in the cells
either (Turmaine et al., 2000).
Other possible causes
Mutant Huntingtin protein also seems to have an affect
the way cells replace themselves, have an excitotoxic
affect on neurons, inflammatory affects and metabolic
pathways in the cell (Reviewed by Ross & Tabrizi,
2011). A major change in some of these processes
could have a detrimental affect on neurons, specifically
medium spiny neurons.
Treatment
Overview
Even with all the information that surrounds
Huntington’s disease, there is still no known cure for
the disease. The only way the sufferers of HD can be
treated at the minute is by using symptomatic
treatments (Adam & Jankovic, 2008) and some
possible therapeutic treatments. There are plenty of
clinical trials ongoing at the moment with regard to
finding symptomatic treatments. Quality of life can be
greatly improved with some symptomatic treatments,
so even if it is not a cure, the HD sufferer, as well as
family and friends, would not have to suffer as much.
Neuroleptics
Neuroleptics are drugs which help prevent psychotic
episodes in HD. There are two main types of
neuroleptics; typical neuroleptics and atypical
neuroleptics (Reviewed by Adam & Jankovic, 2008).
Typical neuroleptics work by having a high affinity on
D2 dopamine receptors, whilst atypical neuroleptics
work by having a higher affinity for 5-HT2A receptors.
Typical neuroleptics are known to treat chorea as well
as psychosis (Bonelli & Hofmann, 2007), but have
more side effects than atypical neuroleptics (Gardner,
Baldessarini & Waraich, 2005). Some examples of
typical neuroleptics include fluphenazine, sulpiride,
haloperidol and pimozide (Reviewed by Adam &
Jankovic, 2008). Some atypical neuroleptics drug
examples are clozapine and olanzapine (Reviewed by
Adam & Jankovic, 2008).
Dopamine depleters
Dopamine depleters can be used as a treatment for
chorea and other movement problems associated with
HD. Some examples of dopamine depleters include
reserpine and tetrabenzine (Adam & Jankovic, 2008).
Tetrabenzine is the more commonly used drug due to

its success rate and the fact that it has less side effects
than reserpine (Reviewed in Adam & Jankovic, 2008).
One of the most severe side effects of these drugs is
depression (Tomlinson, 1977)
Antidepressants
Antidepressants help to alleviate symptoms of
depression. In HD, depression can be a serious
symptom, as mentioned before. Anti-depressants such
as tri-cyclic antidepressants, SSRI’s (selective
serotonin reuptake inhibitors) and SNRI’s (serotonin
norepinephrine reuptake inhibitors) can be used to treat
depression (Medicine, 2013). Fluoxetine may have a
positive effect on chorea, but this is highly disputed
(Reviewed in Adam & Jankovic, 2008).
Therapeutic treatment
There have been studies done on whether therapeutic
target treatment is an effective treatment. The use of
anti-aggregation drugs has been shown to delay
neurodegeneration in a Drosophila model of the
disease (Kazantsev et al., 2002). The prevention of the
cleavage of the mHtt aggregates might help to prevent
mHtt having access to cellular transcription factors,
and therefore possibly inhibiting the disease
(Reviewed in Hickey & Chesselet, 2003).
Latest advances
Lately, a study has been done with regard to
neurodegeneration in prions disease (Moreno,
Halliday, Molloy, et al., 2013). The results of this
study shows a complete stoppage in neurodegeneration
in prions disease in mice with the use of drug called
PERK (protein kinase RNA–like endoplasmic
reticulum kinase) (Moreno, Halliday, Molloy, et al.,
2013). This study might only be seen in prions disease
so far but there is no reason not to believe that the drug
may show the same neuro-protective traits in HD. This
is a first step in what could be a cure for HD.
Conclusion Huntington’s disease is clearly a detrimental disease to
the sufferer, and their family and friends. It seems that
the polyQ repeats are the prime cause of the disease
and that ultimately, MSNs in the brains striatum and
beyond die because of the abnormally long polyQ
repeats. As there are many conflicting reports on the
different possible pathophysiological pathways of HD,
it is extremely difficult to know which one is the
correct neurodegenerative pathway, if any actually are.
It is possible that all of these pathways may occur and
may be part of a major central pathway. As there is the
formation of mHtt aggregates in the disease, it is likely
that these have a major part to play, but it could be that
the aggregates are just a harmless bi-product of another
possible pathophysiological reaction. There is still
copious amounts of research being done into solving
the puzzle that is the pathophysiology of HD. There
are many symptomatic treatments and therapeutic
treatments that can help with the disease but not until a
proven, full pathophysiological mechanism is found
for HD, can finding a cure for the disease be a reality.
References
Adam, O.R. & Jankovic, J. (2008) Symptomatic treatment of
Huntington disease. Neurotherapeutics : the journal of the
American Society for Experimental NeuroTherapeutics.
[Online] 5 (2), 181–197. Available from: doi:10.1016/j.nurt.2008.01.008.
Anon (2013) HTT - huntingtin. [Online]. 12 November 2013. US
National Library of Medicine. Available from:
http://ghr.nlm.nih.gov/gene/HTT [Accessed: 13 November 2013].
Bates, G. (2003) Huntingtin aggregation and toxicity in Huntington’s disease. The Lancet. 361 (May), 1642–1644.
Bibb, J. a, Yan, Z., Svenningsson, P., Snyder, G.L., et al. (2000)
Severe deficiencies in dopamine signaling in
presymptomatic Huntington’s disease mice. Proceedings of
the National Academy of Sciences of the United States of
America. [Online] 97 (12), 6809–6814. Available from: doi:10.1073/pnas.120166397 [Accessed: 18 October 2013].
Bocharova, N., Chave-Cox, R., Sokolov, S., Knorre, D., et al.
(2009) Protein aggregation and neurodegeneration: Clues
from a yeast model of Huntington’s disease. Biochemistry
(Moscow). [Online] 74 (2), 231–234. Available from: doi:10.1134/S0006297909020163.
Boecker, H. (2013) Imaging the role of GABA in movement
disorders. Current neurology and neuroscience reports.
[Online] 13 (10), 385. Available from: doi:10.1007/s11910-013-0385-9 [Accessed: 18 October 2013].
Bonelli, R.M. & Hofmann, P. (2007) A systematic review of the
treatment studies in Huntington’s disease since 1990. Expert
opinion on pharmacotherapy. [Online] 8 (2), 141–153.
Available from: doi:10.1517/14656566.8.2.141 [Accessed: 19 November 2013].
Cha, J.-H. (2000) Huntington’s Disease. [Online]. 2000.
Neuropsychopharmacology: The Fifth Generation of
Progress. Available from: http://www.acnp.org/g4/gn401000151/ch.html.
Chen, S., Ferrone, F. a & Wetzel, R. (2002) Huntington’s disease
age-of-onset linked to polyglutamine aggregation nucleation.
Proceedings of the National Academy of Sciences of the
United States of America. [Online] 99 (18), 11884–11889.
Available from: doi:10.1073/pnas.182276099 [Accessed: 18
October 2013].
Collins, D. (1999) Genetics of Huntington’s Disease. [Online].
1999. University of Kansas Medical Center. Available from:
http://www.kumc.edu/hospital/huntingtons/genetics.html
[Accessed: 2 December 2013].
Damiano, M., Galvan, L., Déglon, N. & Brouillet, E. (2010)
Mitochondria in Huntington’s disease. Biochimica et
biophysica acta. [Online] 1802 (1), 52–61. Available from:
doi:10.1016/j.bbadis.2009.07.012 [Accessed: 18 October
2013].
Education, H.O.P. for (2010) Trinucleotide Repeat Disorders.
[Online]. 2010. Stanford. Available from:
http://www.stanford.edu/group/hopes/cgi-
bin/wordpress/2010/06/trinucleotide-repeat-disorders/ [Accessed: 12 November 2013].
Ellender (2013) Medium Spiny Neurons. [Online]. 2013. University
of Oxford. Available from:
http://www.mrc.ox.ac.uk/gallery/images/striatal-medium-spiny-neuron-ellender-et-al.
Ferreira, I.L., Nascimento, M. V, Ribeiro, M., Almeida, S., et al.
(2010) Mitochondrial-dependent apoptosis in Huntington’s
disease human cybrids. Experimental neurology. [Online]
222 (2), 243–255. Available from:
doi:10.1016/j.expneurol.2010.01.002 [Accessed: 18 October 2013].
Fiedorowicz, J.G., Mills, J.A., Ruggle, A., Langbehn, D., et al.
(2011) Suicidal behavior in prodromal Huntington disease.
Neuro-degenerative diseases. [Online] 8 (6), 483–490.
Available from: doi:10.1159/000327754 [Accessed: 29 October 2013].
Gardner, D.M., Baldessarini, R.J. & Waraich, P. (2005) Modern
antipsychotic drugs: a critical overview. CMAJ : Canadian
Medical Association journal = journal de l’Association
medicale canadienne. [Online] 172 (13), 1703–1711.
Available from: doi:10.1503/cmaj.1041064 [Accessed: 19 November 2013].
Gil, J.M. & Rego, A.C. (2008) Mechanisms of neurodegeneration
in Huntington’s disease. The European journal of
neuroscience. [Online] 27 (11), 2803–2820. Available from:
doi:10.1111/j.1460-9568.2008.06310.x [Accessed: 18 October 2013].
Hackam, A.S., Singaraja, R., Wellington, C.L., Metzler, M., et al.
(1998) The influence of huntingtin protein size on nuclear
localization and cellular toxicity. The Journal of cell
biology. [Online] 141 (5), 1097–1105. Available from:
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=
2137174&tool=pmcentrez&rendertype=abstract [Accessed: 17 November 2013].
Hickey, M. a & Chesselet, M.F. (2003) Apoptosis in Huntington’s
disease. Progress in neuro-psychopharmacology &
biological psychiatry. [Online] 27 (2), 255–265. Available
from: doi:10.1016/S0278-5846(03)00021-6 [Accessed: 18 October 2013].
Hubers, A.A.M., Reedeker, N., Giltay, E.J., Roos, R.A.C., et al.
(2012) Suicidality in Huntington’s disease. Journal of
Affective Disorders. [Online] 136 (3), 550–557. Available
from:
http://www.sciencedirect.com/science/article/pii/S016503271100680X [Accessed: 29 October 2013].
Huntington’s Disease Collaborative Research Group (1993) Gene
found for Huntington’s Disease. British Medical Journal. 306 (6882), 878–879.
Kazantsev, A., Walker, H., Slepko, N. & Etc (2002) A bivalent
Huntingtin binding peptide supresses polyglutamine
aggregation and pathogenesis in Drosophila. Nature. 30367 – 76.
Kent, A. (2004) Huntington ’ s disease. Nursing Standard. 18 (32).
Landles, C. & Bates, G.P. (2004) Huntingtin and the molecular
pathogenesis of Huntington’s disease. Fourth in molecular
medicine review series. EMBO reports. [Online] 5 (10),
958–963. Available from: doi:10.1038/sj.embor.7400250 [Accessed: 18 October 2013].
Loo, D. (2002) TUNEL Assay: An Overview of Techniques.
[Online]. 2002. Springer. Available from:
http://www.springerprotocols.com/Abstract/doi/10.1385/1-
59259-179-5:21.
Mantamadiotis, T., Lamberger, T., Bleckmann, S. & Kern, H.
(2002) Disruption of CREB function in the brain leads to neurodegeneration. Nature. 3147 – 54.
Medicine, U.S.N.L. of (2013) Antidepressants. [Online]. p.1.
Available from:
http://www.nlm.nih.gov/medlineplus/antidepressants.html
[Accessed: 19 November 2013].
Milnerwood, A.J. & Raymond, L. a (2010) Early synaptic
pathophysiology in neurodegeneration: insights from
Huntington’s disease. Trends in neurosciences. [Online] 33
(11), 513–523. Available from:
doi:10.1016/j.tins.2010.08.002 [Accessed: 18 October
2013].
Moreno, J.A., Halliday, M., Molloy, C., Radford, H., et al. (2013)
Oral Treatment Targeting the Unfolded Protein Response
Prevents Neurodegeneration and Clinical Disease in Prion-
Infected Mice. Science translational medicine. [Online] 5
(206), 206ra138. Available from:
doi:10.1126/scitranslmed.3006767 [Accessed: 17 October 2013].
NCBI (2002) Programmed Cell Death (Apoptosis). [Online]. p.1.
Available from:
http://www.ncbi.nlm.nih.gov/books/NBK26873/ [Accessed:
18 November 2013].
NCBI (2013) TP53 tumor protein p53 [Homo sapiens (human)] -
Gene - NCBI. [Online]. 2013. NCBI. Available from:
http://www.ncbi.nlm.nih.gov/gene/7157 [Accessed: 17 November 2013].
Postert, J., Lack, B., Kuhn, W., Jergas, M. (1999) Basal ganglia alterations and brain atrophy in Huntington ’ s disease ...
Ross, C. a & Tabrizi, S.J. (2011) Huntington’s disease: from
molecular pathogenesis to clinical treatment. Lancet
neurology. [Online] 10 (1), 83–98. Available from:
doi:10.1016/S1474-4422(10)70245-3 [Accessed: 18 October 2013].
Sastry, P.S. & Rao, K.S. (2000) Apoptosis and the nervous system.
Journal of neurochemistry. [Online] 74 (1), 1–20. Available
from: http://www.ncbi.nlm.nih.gov/pubmed/10617101 [Accessed: 18 November 2013].
Stanley, C. (2009) Huntington ’ s disease. 5 (2), 88–90.
Steffan, J.S., Kazantsev, A., Spasic-boskovic, O., Greenwald, M.,
et al. (2000) The Huntington’s Disease Protein Interacts
with p53 and CREB-Binding Protein and Represses
Transcription. Proceedings of the National Academy of
Sciences of the United States of America,. [Online] 97 (12). Available from: doi:10.1073/pnas.1001.
Steiner, H. & Tseng, K.Y. (2010) Handbook of Basal Ganglia
Structure and Function: A Decade of Progress. 1st edition.
[Online]. Academic Press. Available from:
http://books.google.com/books?id=Fu1SefIyEysC&pgis=1 [Accessed: 13 November 2013].
Stroke, N.I. of N.D. and (2010) Chorea Information Page.
[Online]. 2010. National Institute of Neurological Disorders
and Stroke (NINDS). Available from:
http://www.ninds.nih.gov/disorders/chorea/chorea.htm.
Sugars, K.L. & Rubinsztein, D.C. (2003) Transcriptional
abnormalities in Huntington disease. Trends in genetics : TIG. 19 (5), 233–238.
Sugaya, K. & Matsubara, S. (2012) Quantitative connection
between polyglutamine aggregation kinetics and
neurodegenerative process in patients with Huntington’s
disease. Molecular neurodegeneration. [Online] 7 (1), 20.
Available from: doi:10.1186/1750-1326-7-20 [Accessed: 18 October 2013].
Tang, T.-S., Slow, E., Lupu, V., Stavrovskaya, I.G., et al. (2005)
Disturbed Ca2+ signaling and apoptosis of medium spiny
neurons in Huntington’s disease. Proceedings of the
National Academy of Sciences of the United States of
America. [Online] 102 (7), 2602–2607. Available from: doi:10.1073/pnas.0409402102 [Accessed: 18 October 2013].
Tomlinson, D.R. (1977) The mode of action of tetrabenazine on
peripheral noradrenergic nerves. British journal of
pharmacology. [Online] 61 (3), 339–344. Available from:
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=
1667862&tool=pmcentrez&rendertype=abstract [Accessed: 19 November 2013].
Truant, R., Atwal, R.S., Desmond, C., Munsie, L., et al. (2008)
Huntington’s disease: revisiting the aggregation hypothesis
in polyglutamine neurodegenerative diseases. The FEBS
journal. [Online] 275 (17), 4252–4262. Available from:
doi:10.1111/j.1742-4658.2008.06561.x [Accessed: 18
October 2013].
Turmaine, M., Raza, a, Mahal, a, Mangiarini, L., et al. (2000)
Nonapoptotic neurodegeneration in a transgenic mouse
model of Huntington’s disease. Proceedings of the National
Academy of Sciences of the United States of America.
[Online] 97 (14), 8093–8097. Available from:
doi:10.1073/pnas.110078997.
Uniprot (2007) Cytochrome c. [Online]. 2007. Uniprot. Available from: http://www.uniprot.org/uniprot/P99999.
Uniprot (2010) Huntingtin - Homo sapiens (Human). [Online]. p.1. Available from: http://www.uniprot.org/uniprot/P42858.
Walker, F.O. (2007) Huntington’s Disease. Seminars in neurology.
[Online] 27 (2), 143–150. Available from: doi:10.1055/s-2007-971176.





























