Embed Size (px)
Citation preview

Human herpesvirus type 8 and Epstein±Barr virus-associatedcutaneous lymphoma taking anaplastic large cell morphologyin a man with HIV infection
K.NAKAMURA, H.KATANO,* Y.HOSHINO,² T.NAKAMURA,³ O.HOSONO,§A.MASUNAGA,¶ S.MORI,* A.IWAMOTO² AND K.TAMAKI
Department of Dermatology, University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-0033, Japan
Departments of *Pathology, ²Infectious Diseases, ³Infectious Diseases and Applied Immunology,
§Clinical Immunology and AIDS Research Centre, and ¶Laboratory of Medicine, Institute of Medical Science,University of Tokyo, Tokyo, Japan
Accepted for publication 11 February 1999
Summary Human herpesvirus type 8 (HHV-8, Kaposi's sarcoma-associated herpesvirus)-positive lymphoma
taking anaplastic large cell morphology in the skin is described in a 46-year-old man with AIDS.Multiple erythematous nodules appeared on the trunk and extremities during the treatment of AIDS.
Histological examination of cutaneous nodules showed dense in®ltration of CD30� atypical
lymphoid cells in the deep dermis. Immunoglobulin JH gene rearrangement was detected in theselymphoma cells. Both Epstein±Barr virus-encoded small RNA and HHV-8 mRNA (T1.1/nut-1) were
detected in these lymphoma cells by in situ hybridization. Remarkable retention of the pericardial
¯uid was observed at the same time that cutaneous lesions grew, and lymphoma cells in thepericardial ¯uid showed the same phenotype as the cutaneous lymphoma. Chemotherapy with
cyclophosphamide, doxorubicin, vincristine and prednisone effectively reduced both the cutaneous
nodules and pericardial ¯uid. However, the patient died 4 months after diagnosis because ofcytomegalovirus infection. As far as we know, this is the ®rst report of an HHV-8-positive cutaneous
lymphoma taking anaplastic large cell morphology. This case suggests the association of AIDS-related anaplastic large cell lymphoma with HHV-8.
Key words: anaplastic large cell lymphoma, Epstein±Barr virus, human herpesvirus type 8, human
immunode®ciency virus, Kaposi's sarcoma-associated herpesvirus, primary effusion lymphoma
Non-Hodgkin's lymphoma (NHL) is the most frequent
neoplasm in Japanese AIDS patients.1 The incidence isreported to be 4±10% among Western AIDS patients,
but exceeds 20% among Japanese.1±3 Most AIDS-
related NHLs are diffuse, aggressive B-cell lymphomas,namely, small non-cleaved cell lymphoma (Burkitt's
lymphoma), large cell and large cell immunoblastic
plasmacytoid lymphoma.4±6 Of AIDS-related NHLs,10±15% have been reported using the term AIDS-
related anaplastic large cell lymphoma (ALCL).7,8
ALCL is a clinically heterogeneous population ofNHL.8±11 ALCL is classi®ed as a T/null-cell type lym-
phoma in the revised European±American classi®cation
of lymphoid neoplasms (REAL);10 however, there aresome B-cell lymphomas exhibiting anaplastic large cell
morphology. p80NPM/ALK protein, a fusion protein of
translocation (2;5), is identi®ed in many ALCLs, andcases expressing p80 have been reported to have a good
prognosis.12
Primary effusion lymphoma (PEL) is a distinct clin-icopathological subtype of NHL, which mainly occurs in
HIV-positive homosexual men.13±15 PEL mainly occurs
in the pleural, pericardial and abdominal cavities, with-out in®ltration into solid tissues. Histologically, lym-
phoma cells of PEL show marked pleomorphism,
expressing CD30, epithelial membrane antigen (EMA)and HLA-DR. PEL shows clonal immunoglobulin gene
rearrangements, and is generally involved in B-cell
lymphomas.13,14 In addition to HIV, the presence ofEpstein±Barr virus (EBV) and human herpesvirus type
8 (HHV-8, Kaposi's sarcoma-associated herpesvirus)
has been identi®ed in lymphoma cells of PEL.14,15
British Journal of Dermatology 1999; 141: 141±145.
141q 1999 British Association of Dermatologists
Correspondence: K.Nakamura. E-mail: [email protected]

HHV-8 encodes various genes such as v-cyclinD, vbcl-2,
MIP1, T0.7, T1.1/nut-1 and vIL-6. Among these, v-cyclinD,GPCR, T0.7 and K12 have been reported to have the
ability to transform and affect the growth of cells.
We describe a case of AIDS-related, p80-negative,CD30� cutaneous lymphoma taking anaplastic large
cell morphology. The latter proved to be a case of skin
involvement of PEL, which originated from pericardialeffusion. Both EBV-encoded small RNA (EBER) and
HHV-8 mRNA (T1.1/nut-1) were detected.
Case report
A 46-year-old homosexual man was admitted in October
1996 with recurrent pneumonia, and diagnosed as
having HIV infection and a respiratory infection withPneumocystis carinii. In August 1996, his CD4� cell
count had been 8/mm3 (normal 700±1000). InNovember 1996, the patient noticed a slight fever and
increased general malaise. Echocardiogram revealed
abnormal uptake in the pericardial cavity. Hepato-splenomegaly and pancytopenia were detected. No
obvious lymphadenopathy was observed. In December
1996, a large amount of pericardial ¯uid was noted.Aspiration of the pericardial cavity was performed and
this ¯uid showed in®ltration of atypical lymphoid cells
(Fig. 1). At the same time, multiple erythematousnodules appeared on the chest, abdomen and upper
and lower limbs, and these tumours developed progres-
sively. The most prominent nodule of the abdomen wasa 3´2 ´ 4 cm, relatively well demarcated, elastic-soft,
slightly elevated tumour (Fig. 2a). His haemoglobin
was 3´6 g/dL (normal 14´0±18´0) and white bloodcell count 1´43 ´ 109/L (normal 4´5±11´0 ´ 109),
with 73% polymorphonuclear leucocytes, 4% lympho-
cytes and 21% eosinophils. Anti-EBV antibodies were asfollows: EBV antiviral capsid antigen (VCA) IgG 160,
VCA IgM <10, EBV-encoded nuclear antigen (EBNA)
10.Biopsy of the cutaneous tumour of the abdomen
showed diffuse in®ltration of atypical lymphoid cells
142 K.NAKAMURA et al.
q 1999 British Association of Dermatologists, British Journal of Dermatology, 141, 141±145
Figure 1. Giemsa staining of effusion lymphoma in the pericardial
¯uid. Lymphoma cells consist of large immunoblastic cells with round
or oval-shaped nuclei (original magni®cation ´ 800).
Figure 2. (a) Erythematous nodules are
evident on the chest and abdomen
(arrows). (b) Photomicrograph of a biopsyof a nodule of the trunk. Diffuse in®ltration
of atypical lymphoid cells is observed from
the reticular dermis through the fat tissue
(haematoxylin and eosin (H&E); originalmagni®cation ´ 40). (c) High power view of
the lymphoma. Atypical large lymphoid
cells consisted of large blastic cells with
round, and sometimes cleaved nuclei andabundant cytoplasm. Some mitotic ®gures
were observed (H&E; original magni®cation
´ 400). (d) Immunohistochemical stainingof CD30 (Ki-1) in atypical lymphoid cells of
the cutaneous nodule. Almost all atypical
cells are positive for CD30 (original
magni®cation ´ 400).
extending from the reticular dermis through fat tissue(Fig. 2b). These atypical lymphoid cells consisted of
large blastic cells with abundant cytoplasm, large
round nuclei and prominent nucleoli (Fig. 2c). Themitotic count was 5 per high power ®eld. There were
no atypical lymphoid cells in the epidermis. Immuno-
histochemical staining of large atypical lymphoid cellsin the cutaneous nodules revealed positivity for CD30
(Fig. 2d) and CD45RO, but did not show positivity for
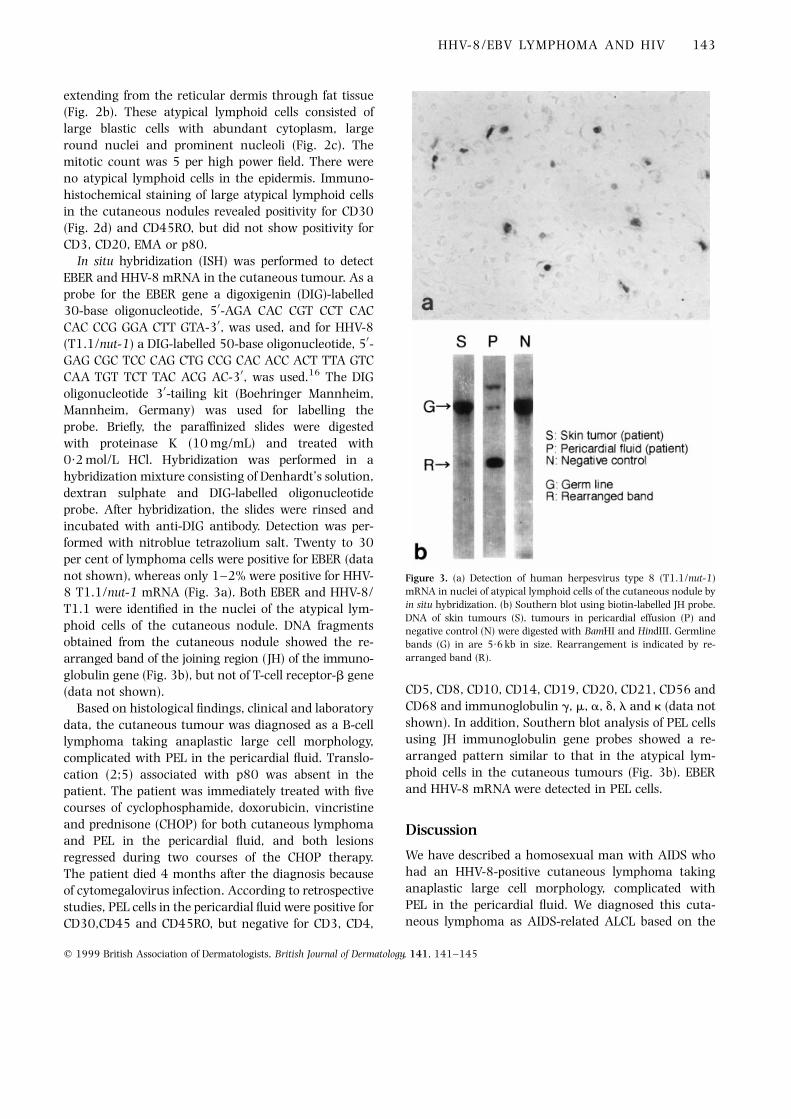
CD3, CD20, EMA or p80.In situ hybridization (ISH) was performed to detect
EBER and HHV-8 mRNA in the cutaneous tumour. As a
probe for the EBER gene a digoxigenin (DIG)-labelled30-base oligonucleotide, 50-AGA CAC CGT CCT CAC
CAC CCG GGA CTT GTA-30, was used, and for HHV-8
(T1.1/nut-1) a DIG-labelled 50-base oligonucleotide, 50-GAG CGC TCC CAG CTG CCG CAC ACC ACT TTA GTC
CAA TGT TCT TAC ACG AC-30, was used.16 The DIG
oligonucleotide 30-tailing kit (Boehringer Mannheim,Mannheim, Germany) was used for labelling the
probe. Brie¯y, the paraf®nized slides were digested
with proteinase K (10 mg/mL) and treated with0´2 mol/L HCl. Hybridization was performed in a
hybridization mixture consisting of Denhardt's solution,
dextran sulphate and DIG-labelled oligonucleotideprobe. After hybridization, the slides were rinsed and
incubated with anti-DIG antibody. Detection was per-formed with nitroblue tetrazolium salt. Twenty to 30
per cent of lymphoma cells were positive for EBER (data
not shown), whereas only 1±2% were positive for HHV-8 T1.1/nut-1 mRNA (Fig. 3a). Both EBER and HHV-8/
T1.1 were identi®ed in the nuclei of the atypical lym-
phoid cells of the cutaneous nodule. DNA fragmentsobtained from the cutaneous nodule showed the re-
arranged band of the joining region (JH) of the immuno-
globulin gene (Fig. 3b), but not of T-cell receptor-b gene(data not shown).
Based on histological ®ndings, clinical and laboratory
data, the cutaneous tumour was diagnosed as a B-celllymphoma taking anaplastic large cell morphology,
complicated with PEL in the pericardial ¯uid. Translo-
cation (2;5) associated with p80 was absent in thepatient. The patient was immediately treated with ®ve
courses of cyclophosphamide, doxorubicin, vincristine
and prednisone (CHOP) for both cutaneous lymphomaand PEL in the pericardial ¯uid, and both lesions
regressed during two courses of the CHOP therapy.
The patient died 4 months after the diagnosis becauseof cytomegalovirus infection. According to retrospective
studies, PEL cells in the pericardial ¯uid were positive for
CD30,CD45 and CD45RO, but negative for CD3, CD4,
CD5, CD8, CD10, CD14, CD19, CD20, CD21, CD56 and
CD68 and immunoglobulin g, m, a, d, l and k (data not
shown). In addition, Southern blot analysis of PEL cellsusing JH immunoglobulin gene probes showed a re-
arranged pattern similar to that in the atypical lym-
phoid cells in the cutaneous tumours (Fig. 3b). EBERand HHV-8 mRNA were detected in PEL cells.
Discussion
We have described a homosexual man with AIDS whohad an HHV-8-positive cutaneous lymphoma taking
anaplastic large cell morphology, complicated with
PEL in the pericardial ¯uid. We diagnosed this cuta-neous lymphoma as AIDS-related ALCL based on the
HHV-8/EBV LYMPHOMA AND HIV 143
q 1999 British Association of Dermatologists, British Journal of Dermatology, 141, 141±145
Figure 3. (a) Detection of human herpesvirus type 8 (T1.1/nut-1)
mRNA in nuclei of atypical lymphoid cells of the cutaneous nodule by
in situ hybridization. (b) Southern blot using biotin-labelled JH probe.
DNA of skin tumours (S), tumours in pericardial effusion (P) andnegative control (N) were digested with BamHI and HindIII. Germline
bands (G) in are 5´6 kb in size. Rearrangement is indicated by re-
arranged band (R).

histopathological features of the lymphoma cells, posi-tivity of CD30 and response to chemotherapy. The
cutaneous lymphoma was a null-cell lymphoma
immunohistologically, but a B-cell lymphoma geneti-cally. The diagnostic criteria for ALCL are still under
debate. While B-cell lymphomas taking anaplastic large
cell morphology were excluded from ALCL under theREAL classi®cation,10 they have been included in ALCL
in other classi®cations such as the updated Kiel classi-
®cation.17 Strictly, our case cannot be included in ALCLunder the REAL classi®cation, but according to the
updated Kiel classi®cation, the diagnosis was AIDS-
related ALCL.ALCL consists of pathogenetically heterogeneous
entities. In about half of ALCLs, the chimeric protein
p80 is expressed. ALCLs with p80 generally occur inyoung patients and tend to be associated with a benign
prognosis, compared with p80-negative ALCLs.12
Beylot-Barry et al. detected p80 in primary cutaneousALCLs, using nested polymerase chain reaction and
ISH.18 Our case did not exhibit p80 in either cutaneous
tumours or the pericardial ¯uid, and was considered tobe an aggressive type of ALCL.
We ®nally diagnosed this cutaneous lymphoma as a
skin involvement of PEL for the following reasons: ®rst,both the cutaneous lymphoma and the pericardial PEL
showed similar immunophenotypes; secondly, EBV andHHV-8 were detected in both lymphomas; thirdly, the
immunoglobulin gene rearrangement pattern of the
cutaneous lymphoma was similar to that of the PEL;fourthly, CHOP chemotherapy reduced both lymphomas
simultaneously and effectively; and lastly, the cutaneous
lymphoma occurred as multiple lesions near the chest.Almost 30 cases of PEL have been reported; however,
the involvement of solid tissues is quite rare. Only a few
cases involving tissues such as lung, submandibulargland and large intestine have been reported.19,20 Our
case was characterized by the simultaneous appearance
of tumours of the skin and pericardial ¯uid. Our case wasdifferent from subcutaneous T-cell lymphoma21 because
the lymphoma cells mainly in®ltrated in the dermis and
did not show panniculitis histologically. In addition, thesecells did not exhibit a T-cell immunophenotype.
HHV-8 is a newly described human herpesvirus that
is a causal factor of Kaposi's sarcoma.22 Recently, DNAsequences of HHV-8 have been discovered in PEL from
HIV-positive patients.23 HHV-8 (T1.1/nut-1) mRNA is
generally transcribed in lytic cells when PEL cells arecultured with phorbol ester in vitro.24 Thus, HHV-8
(T1.1/nut-1) might play an important part in nuclear
processing during lytic growth. Our case had HHV-8
(T1.1/nut-1) mRNA in lymphoma cells of both cuta-neous nodules and pericardial effusion. As far as we
know, this is the ®rst report of the detection of HHV-8
(T1.1/nut-1) mRNA in cutaneous AIDS-related ALCL.Strong expression of HHV-8 (T1.1/nut-1) suggests a
rapid growth of HHV-8 in the lymphoma cells of both
regions.EBERs are transcribed in high copy numbers (107 per
cell) in infected cells, and are used as markers for latent
EBV infection.25 EBERs are detected in a higher propor-tion of EBV-infected cells than are latent membrane
protein-1 and EBNA-2. We detected EBERs in both
skin and pericardial ¯uid by ISH. Most cases of AIDS-related ALCL are associated with EBV infection.26,27 In
addition, PEL often correlates with EBV infection.14,15
There were fewer HHV-8 (T1.1/nut-1) mRNA-positivecells than EBER-positive cells in our case of cutaneous
ALCL, because EBER is expressed in the latent phase,
while HHV-8 T1.1/nut-1 is speci®c for the lytic phase.We did not detect lytic EBV in our case. These data
suggest that the latent EBV, as well as HHV-8, may be
associated with the pathogenesis of AIDS-related ALCL.We suggest that HHV-8 may act in conjunction with
EBV to generate full transformation.
In summary, we report a case of HHV-8-positive,CD30 � lymphoma taking anaplastic large cell mor-
phology, which developed in the skin. Our case differsfrom previous reports in which PEL did not involve solid
tissues. Multiple cutaneous nodules developed along
with the appearance of PEL in our case. Further inves-tigations will elucidate the pathogenetic role of HHV-8
and EBV in AIDS-related ALCL and PEL.
References
1 Katano H, Mori S. Opportunistic lymphoma. Nippon Rinsho±Jpn J
Clin Med 1997; 55: 441±5.
2 Raphael M, Audoujin J, Bryon PA et al. Anatomic and histologicdistribution of 448 cases of AIDS-related non Hodgkin's lym-
phoma. Blood 1993; 82 (Suppl. 1): 386 (Abstr.).
3 Levine AM. Acquired immunode®ciency syndrome-related lym-
phoma. Blood 1992; 80: 8±20.4 Knowles DM, Chamulak GA, Subar M et al. Lymphoid neoplasia
associated with acquired immunode®ciency syndrome (AIDS):
The New York University Med Center Experience with 105
Patients (1981±86). Ann Intern Med 1988; 108: 744±53.5 Raphael MM, Audouin J, French Study Group of Pathology for
HIV-associated Tumors et al. Immunophenotypic and genetic
analysis of acquired immunode®ciency syndrome related non-Hodgkin's lymphomas. Am J Clin Pathol 1994; 101: 773±82.
6 Carbone A, Gaidano G, Glioghini A et al. Clinicopathological
construction. Morphological patterns and molecular pathways
of AIDS-related head and neck and other systemic lymphomas.Ann Otol Rhino Laryngol 1996; 105: 495±9.
7 Tirelli U, Vaccher E, Zagone Vet al. CD30 (Ki-1) -positive anaplastic
144 K.NAKAMURA et al.
q 1999 British Association of Dermatologists, British Journal of Dermatology, 141, 141±145

large-cell lymphomas in 13 patients with and 27 patients without
human immunode®ciency virus infection: the ®rst comparative
clinicopathologic study from a single institution that also includes80 patients with other human immunode®ciency virus-related
systemic lymphomas. J Clin Oncol 1995; 13: 373±80.
8 Nosari A, Cantoni S, Morra E et al. Anaplastic large cell (CD30/Ki-
1�) lymphoma in HIV� patients: clinical and pathological ®nd-ings in a group of ten patients. Br J Haematol 1996; 95: 508±12.
9 Kaudewitz P, Stein H, Dallenbach F et al. Primary and secondary
cutaneous Ki-1� (CD30�) anaplastic large cell lymphomas. Am J
Pathol 1989; 135: 359±67.10 Harris NL, Jaffe ES, Warnke RA et al. A revised European-
American classi®cation of lymphoid neoplasms: a proposal from
the International Lymphoma Study Group. Blood 1994; 84:1361±92.
11 Willemze R, Bejaards RC. Spectrum of primary cutaneous CD30
(Ki-1) -positive lymphoproliferative disorders. J Am Acad Dermatol
1993; 28: 973±80.12 Shiota M, Nakamura S, Ichinohasama R et al. Anaplastic large cell
lymphomas expressing the novel chimeric protein p80 NPM/ALK.
a distinct clinicopathologic entity. Blood 1995; 86: 1954±60.
13 Ansari MQ, Dawson DB, McKenna RW et al. Primary body cavity-based AIDS-related lymphomas. Am J Clin Pathol 1996; 105: 221±
9.
14 Nador RG, Cesarman E, Chadburn A et al. Primary effusionlymphoma: a distinct clinicopathological entity associated with
the Kaposi's sarcoma-associated herpes virus. Blood 1996; 88:
645±56.
15 Cesarman E, Chang Y, Moore PS et al. Kaposi's sarcoma-associatedherpesvirus-like DNA sequences are present in AIDS-related body
cavity-based lymphomas. N Engl J Med 1995; 332: 1186±91.
16 Orenstein JM, Alkan S, Bluvelt A et al. Visualization of human
herpesvirus type 8 in Kaposi's sarcoma by light and transmissionelectron microscopy. AIDS 1997; 11: 35±45.
17 Lennert K, Feller AC. Histopathology of Non-Hodgkin's Lymphoma
(Based on the Updated Kiel Classi®cation). Berlin: Springer-Verlag,
1992.
18 Beylot-Barry M, Lamant L, Vergier B et al. Detection of t(2;5)
(p23;q35) translocation by reverse transcriptase polymerase
chain reaction and in situ hybridization in CD30-positive primarycutaneous lymphoma and lymphomatoid papulosis. Am J Pathol
1996; 149: 483±92.
19 DePond W, Said JW, Tasaka T et al. Kaposi's sarcoma-associated
herpesvirus and human herpesvirus 8 (KSHV/HHV8) -associatedlymphoma of the bowel. Am J Surg Pathol 1997; 21: 719±24.
20 Knowles DM, Inghirami G, Ubriaco A et al. Molecular genetic
analysis of three AIDS-associated neoplasms of uncertain lineage
demonstrates their B-cell derivation and the possible pathogeneticrole of the Epstein±Barr virus. Blood 1989; 73: 792±9.
21 von den Driesch P, Staib G, Simon M Jr et al. Subcutaneous T-cell
lymphoma. J Am Acad Dermatol 1997; 36: 285±9.22 Chang Y, Cesarman E, Ressin MS et al. Identi®cation of
herpesvirus-like DNA sequences in AIDS-associated Kaposi's sar-
coma. Science 1994; 266: 1865±9.
23 Foreman KE, Bacon PE, Hsi ED et al. In situ polymerase chainreaction-based localization studies support role of human herpes-
virus-8 as the cause of two AIDS-related neoplasms: Kaposi's
sarcoma and body cavity lymphoma. J Clin Invest 1997; 99:
2971±8.24 Zhong W, Ganem D. Characterization of ribonucleoprotein com-
plex containing an abundant polyadenylated nuclear RNA
encoded by Kaposi's sarcoma associated herpesvirus (humanherpesvirus 8). J Virol 1997; 71: 1207±12.
25 Howe JG, Steitz JA. Localization of Epstein-Barr virus-encoded
small RNAs by in situ hybridization. Proc Natl Acad Sci USA
1986; 83: 307±15.26 Carbone A, Gloghini A, Zanette I et al. Demonstration of Epstein±
Barr viral genome by in situ hybridization in acquired immune
de®ciency syndrome-related high grade and anaplastic large cell
CD30� lymphomas. Am J Clin Pathol 1993; 99: 289±97.27 Dreno B, Milpied-Homsi B, Moreau P et al. Cutaneous anaplastic T-
cell lymphoma in a patient with human immunode®ciency virus
infection: detection of Epstein±Barr virus DNA. Br J Dermatol
1993; 129: 77±81.
HHV-8/EBV LYMPHOMA AND HIV 145
q 1999 British Association of Dermatologists, British Journal of Dermatology, 141, 141±145





























