Embed Size (px)
Citation preview

1
IMPACT BC:
WHITE PAPER
The Human Dimensions of Change
In British Columbia’s Primary Health Care Culture
December, 2009
Author: Valerie Nicol, Impact BC

2
Executive Summary:
Over the last decade, health care in British Columbia has experienced a substantial amount of change – not the least of which was the 2001 merger of 52 health regions into just 6 Health Authorities. While all systems within the BC health care system were impacted by this vast reorganization, the focus of this white paper is on the BC Primary Health Care system.
In the process of working toward Impact BC’s current aim to increase the capacity for quality improvement work in British Columbia’s Primary Health Care sector, we became aware that conversations with others were frequently focused on human dimensions of change issues regarding current and potential new change initiatives. The issues raised cover a wide spectrum – from the volume and speed at which change is being rolled out - to a perceived lack of role clarity among the various Primary Health Care partners. In many instances, people indicated they did not feel they were managing current changes well and that they were not feeling ready or able to embrace even more change.
Between 2007 and 2009 we saw an increase from an average of 2, to an average of 9, new provincial change initiatives in each health authority (Appendix A, p.22), with several more planned in 2010. This volume of change over a relatively short period of time presents an opportunity to learn more than the measureable outcomes from the various initiatives. It presents an opportunity to learn about how people cope with and respond to frequent and numerous changes. In Appendix A figure 6, we see General Practitioner engagement in change initiatives begin to level off in 2009, while turnover in Health Authority Regional Support teams has increased (figure 2). Through the use of key stakeholder interviews (pp. 8-10) we can start to understand the many ways change is affecting people.
To reach our goal of engaging and sustaining Primary Health Care partners in ongoing transformational change will require a better understanding of the type and scope of human dimensions of change issues. Only when we understand what is really happening can we begin to address and improve upon these issues. The Human Dimensions of Change White Paper examines transformational change issues by providing a scan of the current environment. This White Paper also includes a review of leverage points, key stakeholder interviews from around the province, measurement of indicators related to the human dimensions of change, and recommendations for moving forward with the Human Dimensions of change drivers identified in this report.
British Columbia’s Primary Health Care sector currently has a strong, innovative group of leaders working to make our system highly effective now and sustainable for the future. The Human Dimensions of Change White Paper can provide leaders with insight into issues that may be hindering transformational change efforts, as well as highlighting ways to leverage the knowledge, expertise and good will of our most valuable asset - people.
I. Context and Background:
Why consider the Human Dimensions of Change?
The impetus for considering the impact of the human dimensions of change on transformational change work in BC’s Primary Health Care sector can best be summarized by the following:
“…most change will not happen without the support of people. Focusing only on the changes themselves and not on their effect on people will doom improvement efforts.” (The Improvement Guide, 2nd Edition)

3
and
“Many change projects fail, and the most commonly cited reason is neglect of the human dimensions of change.” (NHS Improvement Leaders’ Guide)
There is currently little understanding of the specifics regarding human dimensions of change issues and how they have manifested in the Primary Care sector of British Columbia. The intent of this White Paper is to understand how the human dimensions of change are impacting transformational change – potentially slowing it - in British Columbia’s Primary Health Care sector and to provide recommendations for improvement.
II. Leverage Points for Improving the Human Dimensions of Change
A. Leadership
The important transformational change work we do in BC’s Primary Health Care sector has us dealing frequently with several human dimensions of change: the change process, interpersonal styles, engagement, leadership, managing conflict, and communication. A better understanding of these dimensions – for us as individuals, and for our work with others - can assist us in improving the success and spread of change initiatives, while also improving the experience of participating in change for all involved.
According to The Improvement Guide, 2nd Edition,
“Knowledge of the human side of change helps us understand how people, as individuals, interact with each other and with a system. It helps us predict how people will react to a specific change and how to gain commitment. It helps us understand the motivations of people and their behavior.”
The NHS Improvement Leaders’ Guide summarizes the most common ways the human dimensions of change are neglected:
1. Lack of insight into why people are unhappy with the change
2. Poor appreciation for the process of change
3. Limited knowledge of the tools and techniques available to help improvement leaders
The truth about the human dimensions of change is that they are complex, challenging, sometimes messy, and if you choose to see it – fascinating – just like people themselves. Margaret Wheatley summarizes it well:
“We have to accept two simple truths: we can’t force anybody to change. And no two people see the world the same way. We can only engage people in the change process from the beginning and see what’s possible. If the issue is meaningful to them, they will become enthusiastic and bright advocates. If we want people’s
“We can’t
force people to
change”

4
intelligence and support, we must welcome them as co-creators. (Leader to Leader, Spring 2001)
Definitions of Change:
• Change: is external and situational: The new site, the new structure, the new team, the new role, the new procedure.
• Transitional Change: is the internal psychological process people go through to come to terms with the new situation.
• Transformational Change: is the combination of both external situational change and internal psychological change and it can only occur when the existing way of doing things no longer works.
The Change Process:
“Change is not the same as transition. Change is situational: The new site, the new structure, the new team, the new role, the new procedure. Transition is the psychological process people go through to come to terms with the new situation. Remember that change is external and transition is internal.”
William Bridges
Bridges describes three stages people can be expected to experience during a transition:
1. The Ending: acknowledge there are things to be let go
2. The Neutral Zone: everything is in flux – the old way is done, but the new way is not yet established
3. The Beginning: the new way feels comfortable and is now the only way
“Most organizations try to start with a beginning, rather than finishing with it. They pay no attention to endings. They do not acknowledge the existence of the neutral zone, and then wonder why people have so much difficulty with change.” (Bridges, 2003)
Common reasons people are hesitant to change include:
• Poor appreciation of the need for change, or considering it less important than other issues
• Poor understanding of proposed solutions, or thinking the solution is inappropriate
• Disagreeing how the change should be implemented
• Embarrassed to admit that things could be improved
• Lack of trust in a person or organization due to past failed change initiatives
• Anticipation of lack of resources
What is
Change?

5
Another method for understanding the change process is to compare “Technical Change” to “Adaptive Change”. Heifetz and Linsky (2002) describe the differences as:
Technical Change – The problem is well defined, a solution is known or can be found and implementation is clear.
Adaptive Change – The problem is complex and requires transforming longstanding habits and deeply held assumptions and values. Feelings of loss and/or sacrifice may occur. The solution requires learning a new way of thinking and creating new relationships.
Most change processes have both technical and adaptive aspects, but it is the adaptive components that may trigger work avoidance as people seek protect themselves from feelings of loss or fear of the unknown.
“People cannot see at the beginning of an adaptive process that the new situation will be any better than the current situation. What they do see clearly is the potential for loss.”
Ron Heifetz
What They Don’t Teach You About Change
In Making Change Last: How to get beyond change fatigue (Ivey Business Journal Jan/Feb 2006) Eric Beaudan describes the implications associated with four learnings leaders may not have had before implementing change:
1. All change runs into resistance. Don’t ever assume, even if it appears so, that resistance to change will be minimal. Be prepared to face open and quiet resistance from unexpected sources.
2. Individuals who support change at the beginning may become neutral, passive or active resistors over time. People change political affiliations once or twice in their lifetime. Expect the same to happen during a demanding change effort.
3. All change involves a shift of the organization’s power structure. Some people will inevitably gain influence, while others will lose some. It’s this unpredictable side-effect that causes most of the passive or open resistance in organizations.
4. No amount of advance thinking, planning and communication guarantees success. That’s because change is by nature unpredictable and unwieldy. The military have a great way to put this: “no plan survives contact with the enemy”.
When change initiatives flounder, people use the phrase “change fatigue” to mean several different things. Typically, it is used to denote an overt unwillingness to continue to participate in a current initiative and/or a resistance to participate in any additional change initiatives. While this describes change fatigue in part, Beaudan describes an additional six symptoms of change fatigue:
1. Outsiders increasingly question the value/objectives of the change effort 2. Change effort leaders/coordinators are stressed out and/or leaving 3. Reluctance to share or comment on data about the effort 4. Budget and resources are diverted to other strategic initiatives 5. (Participant) impatience with duration of change effort 6. Key leaders not attending progress reviews
Whether you believe in the concept of “change fatigue” or not, these symptoms are indicative of a change process that is not likely to arrive at the end stage where the new way
What they
don’t teach
you about
change…

6
of being has been accepted and implemented by the majority. Knowing how to intervene when these symptoms arise is critical to success.
Beaudan maintains that successful change leaders need to do three things:
1. Recognize that the change platform they create is only valid for a brief period. 2. Avoid stalling when the symptoms of change fatigue begin to show. Be aware of their
own emotional state and develop a plan that does not blame themselves or others. 3. Remember that visible leadership is the magic ingredient that keeps change moving
forward. Great change leaders know they need to be seen and heard to provide the inspiration and passion to keep people engaged.
Where transformational change is concerned, the most effective leader is believed to be more humble and less of the heroic all-knowing kind. As it is extremely difficult to determine what the future state of a change process will ultimately be, it is better for a leader to be adaptable and to simply focus on navigating from point to point in the journey. When the desired state is reached, the leader “will know it when they see it”.
Nick Morgan says in Harvard Business School Working Knowledge (Sept. 2001),
“No longer obsessed with the need for larger-than-life leaders and their grand strategies, we can now focus on a quieter, more evolutionary approach to change, one that relies on employee motivation instead of directives from on high.”
In her work on innovation, Margaret Wheatley (Leader to Leader, 2001) writes,
“Innovation has always been a primary challenge of leadership. Today we live in an era of such rapid change and evolution that leaders must work constantly to develop the capacity for continuous change and frequent adaptation.”
In Implementing and sustaining transformational change in health care, McGrath et al (The Medical Journal of Australia 2008, 188) describe leadership by senior executives and clinical leadership among the key elements for success.
“Senior Management needs to set the standards for service delivery and drive the change process. This requires management to engage and challenge staff with ‘stretch goals’ (ambitious goals that stimulate staff beyond their current achievements), set the parameters for acceptable solutions, ensure strategies are implemented within set timeframes and budgets, monitor performance and reward success. Staff members need to see the program is a priority for their chief executive officer.”
“Clinical leadership is critical to success. A very important factor in engaging clinicians is for management to commit in advance to implementing solutions designed by staff. Trust is gained when staff see their solutions being implemented: not implementing solutions identified by staff, we feel, can lead to further cynicism. …management must set the criteria for solution development in advance, and state what resources are available.
Clinicians have a vested interest in simplifying frustrating clinical processes and eliminating waste.”
Speaking directly to the issue raised by the NHS about people having poor appreciation for the process of change, David A. Garvin in the Harvard Management Update, July 2001, states,

7
“Change leaders must explain the particular initiative thoroughly…they must address employee fears: ‘People want to know why you think they can make it through the change. They also want to know how you’re going to help them through it.”
W. Edwards Deming wrote about a “System of Profound Knowledge” which he defined as having four parts: 1. Appreciation for a system, 2. Understanding variation, 3. Building knowledge, 4. Human side of change. He did not propose that improvement leaders need to be experts in all four areas, but rather they should understand the basic theories of each, how they interrelate to one another, and why they are important to improvement. “The Improvement Guide: A practical Approach to Enhancing Organizational Performance” expands on Deming’s ideas by saying,
“Some knowledge of psychology is essential to understand the human side of change. Leaders of improvement plan for the social impact of technical change and make people part of the solution. They look for fundamental (unspoken) assumptions and beliefs behind decisions and actions taken. They appreciate differences in people and the importance of the fundamental attribution error. They understand the value of teams and that cooperation, rather than competition, is necessary if changes are to be successful. Leaders use reward and recognition systems that rely more on intrinsic motivation than extrinsic motivation. Commitment to change is built through sharing of information. (p. 85)
In the Institute for Health Improvement “Executive Review of Improvement Projects: A Primer for CEOs and other Senior Leaders”, it is said that attention is the currency of leadership, and that,
“Leaders who wish to transform their organizations should channel their attention to the key
leverage points for the quality transformation.”
Improvement projects are key leverage points in the long term transformational change process and periodic review by leadership is vital to their success.
“Executive review of projects can be a critical factor in whether the projects will help, or
hurt, the transformation. The first step is for executives to make the decision to channel attention to project reviews, and to budget the time in their own schedules for this activity. The
next step is to learn how to do a good project review…It’s not enough to give projects your time.
You must also know how to use that time well—so that your reviews help, rather than hurt.”
Purpose of Senior Leader Project Review The purpose of reviews of projects by CEOs and other executives should be clear:
1. Learn whether the project is on track, or is likely to fail 2. If the project is not achieving the intended results, to understand why:
a. Lack of organizational will? b. Absence of strong enough ideas for improvement? c. Failure to execute changes?
3. Provide guidance, support, and stimulus to the project team on will, ideas, and execution
4. Decide whether the project should be stopped.
Leaders must champion high aims for improvement, capable project leadership and teamwork, and good organizational support. With these in place, spread throughout the
“Leaders
understand
that we have
bad systems,
not bad
people.”

8
organization and sector are possible. Leaders who build the will for improvement also demonstrate the values and behaviors that drive transformational change.
B. Engagement
Margaret Wheatley describes how she learned the hard way that building participation in transformational change is not optional. She maintains that failing to invite everyone into the creative process results in the eventual appearance of resistors and saboteurs. Wheatley asserts that she did not become insistent on participation to avoid resistance, but rather that she learned she is not smart enough to design anything for an entire system. In order to understand what is meaningful to people or to know how they do their work, Wheatley says we must engage the whole system to harvest the invisible intelligence that exists throughout.
At this point in the evolution of Primary Health Care in BC, it is vital that our leaders engage key stakeholders and publicly show support for transformational change initiatives. In addition, leadership priorities must include efforts to keep people engaged by networking regularly with stakeholders for two reasons. First, to keep people well informed of the status of the initiative, and second, to show that stakeholder needs and issues are being listened to and reflected in decision-making.
III. Key Stakeholder Interviews During the course of this project, 26 interviews were conducted with key stakeholders in BC’s Primary Health Care Sector. The stakeholders interviewed include regional support team staff in health authorities, executives in both PHC partner organizations and health authorities, and General Practice physicians. The interviews were conducted informally either by telephone or in person. This approach was chosen as it enabled the participants to communicate their unique experiences and knowledge in their own words. Some anonymous quotes from the stakeholder interviews are provided to enhance the reporting of the information shared. Confidentiality was established at the beginning of each interview before information was shared and any quotes published from the interviews will remain anonymous to maintain confidentiality. Typically, the interview process began with the interviewer asking interviewees to describe their experiences with transformational change initiatives in BC’s PHC sector. When the interviews were completed, the content from each stakeholder interview was reviewed. Further analysis was conducted whereby information was extracted and categorized according to common themes. In the final analysis, five themes emerged that are common to stakeholders across the BC PHC sector, while nine additional sub-themes pertaining to specific aspects of the BC PHC sector emerged from the interview content.
System-Wide Themes:
1. Volume/Speed of Changes - The number of changes and the speed at which they are being rolled out.
Participation
as a
requirement

9
2. Lack of accomplishment/job satisfaction – often no opportunity to acknowledge or
celebrate completion of work.
3. Lack of role clarity within HAs, and between HAs and PHC partners.
4. Increased expectations for PHC compared to other areas in health care – constant need to prove our worth by saving the health care system.
5. Lack of Integration - Many PHC silos still exist.
Sub-themes:
6. Leadership – need for more frequent visibility, psychological safety to disclose issues, and direct sponsorship of Quality Improvement and Primary Health Care initiatives.
7. Health Authorities – need to address issues leading to employee turnover such as lack
of role clarity, infrequent transparent communication, lack of psychological safety to disclose issues, fear about job security.
8. General Practice Physicians – need for more GP champions and more input regarding collaboration with other service providers.
9. GPSC – need for more collaborative, inclusive approach toward Health Authorities.
10. Staff Turnover: Resignations, Burn-out, Termination – need to address this at all
organizational levels to preserve historical knowledge and reduce costs associated with re-hiring
11. Data – need more emphasis on pre-initiative data collection and data from PSP module users
12. Funding – need to align funding availability with fiscal year framework and to combine
PSP/IHN funding to promote integration
13. Change Fatigue – need for more effective pace and volume of change, and for psychological safety to discuss issues honestly.
14. Competencies – Regional Support Teams need support, access and training to do
Quality Improvement work
Quotes from Key Informants:
“We lose our best people first – the most productive, most engaged people will not stay in an
environment that conflicts with their values.”
“Improving things is not really a priority right now when the majority of us don’t know if we have
jobs.”

10
“Pockets of funding = pockets of activity. There are too many layers to be integrated.”
“It seems to me the leadership is unclear about how to integrate.”
“We have ‘command and control’ leaders running ‘collaborative, integrative’ initiatives.”
“GPs want to be consulted individually on everything and GPs want you to leave them alone.”
“Physicians want some control over who works with them in their practice.”
“The union framework governing health authority staff is incompatible with the culture in a
physician office.”
“Staff will only be accountable if their salaries are paid for by physicians.”
“We need new rules of engagement with patients and with the government to facilitate better
relationships.”
“Earlier use of quality improvement would have got us farther, faster with the available data.”
“PSP work has great value and potential to solve a variety of problems. We need to protect the
enthusiasm and nurture it in those who do the work.”
“There is no organizational history here because of turnover.”
“Sometimes fear is perceived as resistance to change.”
“The relationship aspect is as important as the work itself.”
IV. Recommendations

11
Driver Diagram for Improving the Human Dimensions of Change
Outcome Key Drivers Change Concepts
Figure 7
Improved BC Primary Health
Care Outcomes facilitated by
improvements in the Human
Dimensions of Change.
Visible Leadership
System-Wide
Collaboration
Regular
Communication
Engagement and
Relationship Building
Networking
Provide inspiration and passion
when change falters
Ensure participation is a
requirement. People only
support what they create
Address fears
Report on progress – even if
initiative is lagging
Acknowledge losses associated
with ending of old way
Frequently describe path to the
new way
Seek to understand the
environment and the people you
are asking to change prior to
beginning
Build the will for Q.I. initiatives
Provide resources and remove
barriers to improvement
Periodic review of QI initiatives

12
Driver 1: Implementing Visible Leadership
Great change leaders know that being seen and heard – regularly – is what keeps change
moving forward. If people feel they are being heard by leadership and can see their
concerns reflected in decision-making, they will stay the course of transformational change
and make it the new way of doing things.
When transformational change falters, people expend vast amounts of time and energy
worrying about the situation. Both T. R Clark Associates and Nick Morgan in the Harvard
Management Update recommend that leadership pare down the number of initiatives and
focus on achieving some small, measurable goals. This allows people to focus less on what
seems like a grand unattainable vision and focus more on experiencing some small, yet
motivating successes.
The transformational changes we seek in BC’s Primary Health Care sector are meant to be
collaborative, integrative and sustainable with the aims of improving the health of our
population, improving outcomes for patients, improving the experiences of patients and
providers and reducing the overall costs to the system. The key stakeholder interviews
revealed that people working in this sector believe health authorities still subscribe to the
“command and control” approach to leadership. This causes values conflicts all around for
the people trying to do collaborative, integrative work in health authority environments. From
Margaret Wheatley’s perspective,
“Life always reacts to directives, it never obeys them. It never matters how
clear or visionary or important the message is. It can only elicit reactions, not
straightforward compliance...We can expect reactions that will be as varied as the
individuals who hear it. Therefore, anything we say or write is only an invitation to
others to become involved with us, to think with us. Each reaction reflects a
different perception of what’s important, and if that diversity is explored, the
organization develops a richer, wiser understanding of what’s going on.” (Journal
for Strategic Performance Measurement April/May 1998)
The psychological aspects of the human dimensions of change are becoming the subject of
much discussion and theorising. The NHS has compiled a guide for Improvement Leaders
involved in healthcare initiatives with the aim of educating leaders to be better able to
understand and better manage key issues in the change process and to help leaders to
engage and empower the people they work with.
The NHS advises leaders to adopt an approach to improvement comprised of the following:
1. Set a direction, but be flexible in how you get there.
2. Top down support is needed for bottom up change.
3. Objectives need to be set and celebrated when achieved. Also, recognize that
improvement never actually ends.

13
4. Planning and monitoring improvement is important, while gaining the commitment of
people is VITAL.
Also of prime importance is the ability to take a leadership stance when required. This is not
about asserting positional authority, but rather knowing when to redirect a situation that has
ceased to move forward in a positive direction. In any change process, you may be faced
with a number of potential challenges such as what transpired before you came along,
preconceived notions of your agenda, and in some cases, a general aversion to change. No
matter what the situation, be prepared to take a leadership stance in the change process by
continuously returning the focus of discussions to, “What can we do TODAY?”
It’s easy to get sidetracked by the multitude of issues that crop up in situations of
transformational change. The following are some strategies to keep things moving forward
and focused on the common goal of improving patient and provider outcomes:
• Provide clarity of role and purpose
• Set a boundary for respectful communication between all participants
• Frequently acknowledge the valuable contributions of all parties
• Focus on problems with “systems” rather than people
• Always return the focus of discussion to a common goal of improving patient outcomes
and experiences
Based on the work of Heifetz and Linsky (2002), Jack Silversin makes the following recommendations for addressing adaptive change issues:
• Withhold judgment of those struggling with the issue. Be sure your intention is to be helpful.
• Make it safe to have a candid conversation.
• Ask people to name the issue or describe what they think they are seeing.
• Help people appreciate that if they have adaptive work to do, technical expertise will have limited utility.
Another important idea to consider is the development of improvement capability in Primary
Health Care. Leadership can create the context for this by setting and reinforcing
expectations for everyone with regard to their responsibility for improvement. In “The
Improvement Guide: A practical Approach to Enhancing Organizational Performance”,
specific expectations are outlined for leaders and other individuals at various organization
levels:
“Executives:
Create a system of improvement and integrate it…
Build collaboration by promoting cooperative goals and fostering trust between all stakeholders in the system.
Take a
leadership
stance in
the change
process

14
Invest time and other resources in improvement…and developing people to lead these efforts.
Managers:
Connect the roles of people to the roles of the department and purpose of the organization.
Lead cross-functional improvement teams.
Develop supervisors to lead improvement in their areas.
Front-line supervision:
Remove defects and waste from processes of daily work.
Participate in improvement teams that contribute to the larger aims of the department or Organization.
Help people execute on the requirements of the job with the aim of delighting the internal and external customer.” (p.332-333)
In the IHI White Paper, “Seven Leadership Leverage Points for Organization-Level Improvement in Health Care (Second Edition)”, Reinerstsen et al describe seven key levers for leaders. Leverage Point Three: Channel Leadership Attention to System-Level Improvement: Personal Leadership, Leadership Systems, and Transparency speak to the ways leaders can model successful transformational change by what they attend to:
“Executives are constantly sending signals about what they believe to be important. Some signals are negative (e.g., arriving late to the meeting, not asking questions, taking a phone call during the meeting, and leaving early). Other signals tell the staff that executives really care about achieving the stated quality aim. Examples of positive signals might include the following: • Prioritize Calendars: Leaders can change their personal schedules to make time for data review, meetings with project leaders, and other activities that support the work. • Conduct Project Reviews: Senior executives can send powerful signals by personally performing reviews with project teams—asking about their project aims, connecting the work of the team to the overall organization aims, focusing on results, helping the team to overcome barriers, and providing encouragement. • Tell Stories: Positive organizational “buzz” can be created by the stories that executives tell in their formal and informal communications. If the stories reinforce the cultural changes and practices needed to achieve breakthrough aims (e.g., a story about a manager’s willingness to do multiple rapid tests of change and the great results achieved), they will encourage more rapid adoption of the needed patterns and practices.
Exit interviews present another opportunity for leadership to learn more about their working environment and the human dimensions of change within it. The majority of key stakeholders interviewed for this report said they did not believe exit interviews were many levels as people work through the loss of a colleague, uncertainty, and the subsequent disruption to work flow. However, employee turnover also represents an opportunity to harvest valuable information about the position, the current environment and opportunities for improvement.
Exit
interview
learnings

15
Driver 2: Implementing System-Wide Collaboration
Collaborative, participative processes always seem to take much longer and become more
complex than decision-making with small groups that is then spread to the masses.
However, when you consider how much effort is required to manage unintended side-effects
experienced by people who feel they were left out or ignored, or how much of time is spent
selling a solution you know won’t be embraced by the target population, the idea of
“delivering” changes, rather than involving people in their creation, seems very impractical.
“We have no choice but to invite people into the process of rethinking,
redesigning, restructuring the organization. We ignore people’s need to
participate at our own peril. If they’re involved, they will create a future that
already has them in it. We won’t have to engage in the impossible and
exhausting tasks of ‘selling’ them the solution, getting them ’to enroll’ or figuring
out the incentives that might bribe them into compliant behaviours…People only
support what they create.” (Margaret Wheatley, Journal for Strategic
Performance Measurement April/May 1998)
A critical task for leadership is to increase the number, variety and strength of connections
within a system. By doing so, you support the notion that systems are capable of changing
themselves once they have newer and better information to work with. It also supports the
idea that the system already contains the majority of the expertise it needs. The customer
service revolution exemplifies how this belief system manifested a dramatic improvement in
quality once customers were invited to provide feedback. Without their inclusion, there was
no way to know what or how to change the system. This notion is equally important for
health care and lends great support to the Patients as Partners work in our province.
People are intelligent - they figure out how to make things work even when it seems
impossible. They do this by creating work-around solutions to barriers and ridiculous
policies. They create networks of people to help and support them through periods of
transformational change. By not inviting all of these people to participate in the creation of
change processes, we increase the likelihood that some of them will become resistors and
saboteurs. Because we cannot possibly know everything that is meaningful to people or all
of the ways they manage to do what they do, participation in the creation of change cannot
be optional.
Driver 3: Implementing Regular Communication
Issues around communication are typically at the forefront of any faltering change initiative.
People have numerous ways of communicating and different styles of working. It is
particularly important to be aware of these differences when transformational change is
taking place.
“People only
support what
they create.”

16
The NHS Improvement Leaders Guide to Managing the Human Dimensions of Change
recommends the following ways to improve communication:
• Uncertainty is more painful than bad news, so communicate early and often.
• Seek first to understand, then to be understood.
• Communicate directly with the people that matter – preferably face to face.
• Make the communication process transparent and two-way.
• Be honest and tell the truth.
• The result of a communication is the response you receive, which may be different from
what you intended.
• You are always communicating, even when you think you’re not. A person cannot NOT
communicate and behaviour is the highest form of communication.
Conflict is an unavoidable reality. Unfortunately, many people behave as if it is avoidable,
which leads to many other issues in the long term. A more effective approach is to deal
directly with conflict and that is best done by starting from a place of curiosity. Through the
process of asking and learning what transpired, participants will feel heard and tensions will
subside to the point where resolutions can be discussed. Conflicts tend to be more about
people than issues, and they consist of two elements:
The relationship between the people involved
The issue at the centre of the disagreement
Above all, acknowledge the conflict rather than avoiding it. Listen to understand the
differences in the parties involved (including your own). Ask questions to assist your
understanding of the goal from both perspectives. Seek solutions that incorporate both
goals.
Encouragement and support are essential aspects of communication during transitional
change. As long as ideas are proposed in a collaborative manner, (“What do you think about
trying….”) people will remain engaged and interested in working to move forward.
Challenging people to try new things in subtle ways that inspire creativity and desire to see
tasks through to completion helps push past the inertia of the neutral zone of change.
When progress slows or stops, create solutions to fit needs. After hearing and understanding
what the issues are, apply the knowledge, skills and expertise to create workable solutions.
Fear is a huge detractor in the transitional change process. When people feel afraid for their
jobs or about the uncertain future of an initiative, they want to hear directly from the leaders
how they are going to help them through it. People want to know why the leader thinks they
can make it through the change. Inspiring innovation to push through barriers is a strong
way forward to overcoming fears.

17
William Bridges writes,
“change causes transition, and transition starts with an ending. If things change
within an organization, at least some of the employees and managers are going to
have to let go of something.” (Managing Transitions, 2003)
Most important in this part of the change process is for leadership to acknowledge that
people are dealing with losses. How best to assist people with letting go is summarized from
Bridges’ work on managing transitions and making the most of change:
1. Identify who is losing what.
2. Accept the reality and importance of the subjective losses.
3. Don’t be surprised by overreaction.
4. Acknowledge the losses openly and sympathetically.
5. Expect and accept the signs of grieving.
6. Compensate for the losses. Act, rather than trying to talk people out of their feelings.
7. Define what is over and what isn’t.
8. Mark the endings
9. Treat the past with respect
10. Show how endings protect the continuity of something bigger.
Bridges employs his own advice by stating and restating several times throughout his book,
“Give people information, and do it again and again.” Telling the truth when providing
information is recommended by several sources as being the best way to achieve
consistency in communication.
Driver 4: Implementing Engagement and Relationship Building
“The scientific search for the basic building blocks of life has revealed a startling
fact: there are none. The deeper that physicists peer into the nature of reality, the
only thing they find is relationships...We live in a culture that does not acknowledge
this scientific fact. We believe wholeheartedly in the individual and build
organizations based on this erroneous idea. We create org charts of separate boxes
with lines connecting the boxes that indicate reporting relationships and channels of
communication. But our neatly drawn organizations are as fictitious as building
blocks are to physicists. The only form of organization used on this planet is the
network—webs of interconnected, interdependent relationships.” (Margaret
Wheatley, 2006)
Engagement is about relationship building. Even if you develop the most brilliant
improvement idea ever conceived, little change will occur unless you have created a
relationship where the other person trusts you enough to tell you how they honestly feel
about it.
The context for engagement in primary care improvement is broad. Potentially, engagement
could involve colleagues, physicians, leadership, other health authorities, community
organizations, and PHC partners.

18
Respectful inquiry is essential for successful engagement. By coming from a place of
authentic interest in the person you are engaging, you set the stage for creating the other
elements essential for success. When engaging people, Respectful Inquiry includes an
acknowledgement of the value of their time before you begin asking questions, and by
having a few good questions prepared in advance.
Building trust and rapport is essential for creating and sustaining a relationship of mutual
trust and understanding. Rapport is achieved by listening reflectively and having body
language that indicates your interest in what others are saying.
Rapport is the basis of good communication and is an important form of influence.
Listening to people and letting them know they have been heard is critical to the
engagement and relationship building process. Listening to the context is a very helpful skill
that seeks to understand the whole person in the context of this one situation.
Being aware of your own biases and not reacting is another essential skill, particularly when
others disagree. Leaders who monitor their own feelings of denial, anger, depression etc.
are better able to navigate organizations through transformational change by avoiding the
temptation to blame themselves or others when things falter.
“It’s not what you say, it’s the way that you say it”
Louis Armstrong
• Encourage & Support
• Manage Conflict
• Negotiate
• Focus on Improving Patient & Provider Outcomes
• What Next?
• Encourage & Support
• Create Solutions to Fit Needs
• Negotiate
• Respectful Inquiry
• Attending
• Active Listening
• Trust & Rapport
• Empathy
ASSESS by ASKING
“How can I help you?”
AGREE to a PLAN
“What will work for you?”
ASSIST to IMPLEMENT
“Let’s try one thing.”
ARRANGE to EVALUATE
“How did it go?”
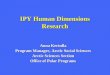
Engagement/Relationship Building Skills
ASK
V.Nicol - 2009 Adapted from “The 5 A’s (Northern Health) and the Brief Model of Therapy
Figure 1

19
Adapted from “The 5 A’s” (A. Domes, Northern Health) and the Brief Therapy model, Figure
6 describes a process for engagement and relationship building as well as a number of skills
corresponding to each stage of the process. The word “ASK” is at the centre of the model
because it is something you need to do throughout the process. Frequently, we start out a
relationship by asking many questions, but over time we stop, because we think we
understand all we need to know about the person and the situation. It is important to ask
questions regularly as is the best way to ensure your knowledge and understanding is
current, and it maintains engagement of people.
Additional key concepts from Figure 6 are:
Seek to understand the perspectives of other people in a respectful manner.
Develop a range of styles to use when working with people. Your way is not the only
way….
Ask open-ended questions, and demonstrate you are listening by using Active Listening
Skills.
Create trust and rapport with people by being present with them (attending skills).
Ask for feedback to learn how you are perceived by others and to determine how to
modify your approach (if necessary) to obtain the results you seek.
Actions speak louder than words. Behaviour tells you important things about a person.
However, people are not their behaviour.
Everybody has a different way of communicating and a different style of working. It is
particularly important to be aware of these differences when transformational change is
taking place. Failure to account for these differences in personal style often leads to people
being labelled “resistant to change”.
Identifying people as ‘laggards’ or ‘resistant to change’ is not helpful as it can lead to conflict.
A more productive approach is to consider that the person simply doesn’t see how this idea
fulfills a need and that they may be an ‘early adopter’ of a different idea.
V. Conclusions
Gaining a better understanding of the human dimensions of change issues in BC’s PHC
sector enabled the identification of key drivers and change concepts to improve upon those
issues. The challenge now lies in embedding the changes for improvement in the way we
work every day, with everybody. The following suggestions are a possible way forward:
Incorporate the four key drivers: Visible Leadership; System-Wide Collaboration;
Regular Communication; and Engagement and Relationship Building into the
improvement charters of new initiatives.
Provide basic information about the human dimensions of change as part of all new
PHC initiatives. This could facilitate the transformational change process by alerting
participants to the potential pitfalls and solutions, before progress becomes stalled.

20
Continue to provide access for PHC participants to Impact B.C.’s Supporting
Improvement and Innovation webinar series, which includes a presentation on the
Human Dimensions of Change. This webinar series is an effective means of
providing both information, and a forum for discussion on this very complex and
important topic.
Throughout all of our work in BC’s Primary Health Care sector, relationships are the critical
element. We need to become better at leveraging the capacities that develop from good
relationships. We need to recognize and celebrate new competencies that develop as a
result of effective relationships.
“We can be human only together.” Archbishop Desmond Tutu
“There are common human yearnings: We want to be together; we want to learn;
we hope to contribute to others; we want our children to be healthy and have better
lives….If we are to evoke kindness, intelligence, accountability and learning in our
organizations, we need to promote healthy relationships… A simple means to
support and develop relationships is to create time to think together.” (Relationships:
The Building Blocks of Life. Margaret Wheatley, 2006)
Thinking together and talking about the human dimensions of change will enable us to
create a path forward that is representative of the needs of the province of BC as a whole,
and that is respectful of the efforts and perspectives of all who work in Primary Health Care.
What can you do today?

21
Appendix A – Measurement
PHC Turnover by HA 2005-2009
Figure 2
There has been substantial turnover in Health Authority PHC staff and executives over the past
four years.
The main concerns arising from turnover are:
1. Cost to the system to re-hire and train new staff
2. Lack of organizational history (loss of knowledge that can be passed on) – particularly
problematic in executive-level positions
3. Disruption to work-flow and service to patients
4. Stress for co-workers when a position is not replaced

22
New BC PHC Initiatives - 2007
Figure 3
BC PHC Initiatives – 2008
Figure 4
BC PHC Initiatives – 2009
Figure 5

23
Summary of BC PHC Initiatives 2007-2009
Health Innovation Fund – (2007-2008 one-time funding) by HAs
NHA: PHC System Improvements for Targeted Populations (Care North) (IHNs)
IHA: Integrated Health Networks
FHA:
o Primary Care Redesign Initiative
o Integrated PHC Network for the Older Adult
o Integrated Health Network for Immigrants: Surrey and Burnaby
VCH: Chronic Disease Management Care Connectivity Pilot
VIHA:
o Seniors At Risk Integrated Health Network
o Chronic Disease Management Co-Morbidity Integrated Health Networks (3)
o Underserved Communities Integrated Health Networks (3)
MOHS and HA (Bi-Laterally Funded Integrated Health Networks (2008-
2010) by HA NHA: PHC System Improvements for Targeted Populations (Care North) (IHNs)
IHA: Integrated Health Networks
FHA:
o Integrated PHC Network for the Older Adult
o Integrated Health Network for Immigrants: Surrey and Burnaby
VCH: Chronic Disease Management Care Connectivity Pilot
VIHA:
o Seniors At Risk Integrated Health Network
o Chronic Disease Management Co-Morbidity Integrated Health Networks (3)
o Underserved Communities Integrated Health Networks (3)
General Practitioners Services Committee Initiatives (All HAs) Complex Care Management
MH Planning
MH Management
Maternity Care
Cardiovascular Risk Assessment
Chronic Disease Management Fees

24
o Diabetes
o CHF
o HRT
o COPD
Community Conferencing Fees
Facility Conferencing Fees
Acute Care Discharge Planning Fees
End of Life Planning
GP Divisions
Multidisciplinary Care Initiative
Attachment to Practice
How’s Your Health Value Test/Prototype
PSP Modules:
o Chronic Disease Management
o Patient Self Management
o Advanced Access
o Group Visits
o Practice Self-Assessment (Short/Long)
o Adult Mental Health
o Youth Mental Health
o Shared care with COPD focus
o End of Life
o Specialist PSP
o Physician Engagement
o Rolling Thunder (post module completion, ongoing QI Support)
o MODULE REDESIGN –
- Practice Management: Access and Efficiency, GMV & PSM
- Clinical Redesign: CDM,
MOHS – New - All HAs
Patients as Partners
Charter 1 – Individual Health Care
Charter 2 – Shaping the PHC System
Charter 3 – Bringing in the Community
Health Literacy Collaborative
New Integrated Health Networks

25
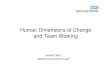
Number of Discrete Participants in BC Practice Support Program Modules (to November 2009) by Health Authority
Figure 6
The BC Practice Support Program has been engaging GP physicians and their MOAs in
modules since 2007. There are a further 5 modules expected to begin in early 2010.
Considerations regarding the PSP initiatives are:
1. GP engagement seems to have levelled off in 2009.
2. GPs who are not participating may not recognize the value of the modules to their patients,
their practices, and themselves.
3. There are no financial disincentives if GPs choose not to participate.

26
References
Banks, Martin. Planning for Transformational Change.
It-director.com/business/change/content.php?cid=11272
Beaudan, Eric. Making change last: How to get beyond change fatigue. Ivey Business Journal,
January/February 2006.
Bridges, William (2003) Managing Transitions : Making the Most of Change. Da Capo Press,
Perseus Books Group, Campbridge MA, USA.
Clark, T.R. and Associates. Communicating Vision in a Change-Battered Organization.
Trclarkglobal.com/pdf/white-paper-communicating-vision.pdf
Domes, Alice, Barg, Marvin. “The 5 A’s”. Northern Health Authority, British Columbia, Canada
Egan, Gerard (1994) The Skilled Helper. Brooks Cole Publishing, Belmont, California USA
Heifetz, Ronald L, Linsky, Marty (2002) Leadership on the Line: Staying Alive Through the
Dangers of Leading. Harvard Business School Publishing, Boston, MA.
Konkin, Mary and Associates. Divisions of Family Practice Needs Assessment Survey, October
2009
Langley, Gerald J., Moen, Ronald D., Nolan, Kevin M., Nolan, Thomas W., Norman, Clifford L.,
Provost, Lloyd P. (2009) The Improvement Guide: A practical Approach to Enhancing
Organizational Performance. Jossey-Bass, San Francisco, California
McGrath, Katherine M., Bennett, Denise M., Ben-Tovim, David I., Boyages, Steven C., Lyons, Nigel J., and O’Connell, Tony J. Implementing and sustaining transformational change in health care: lessons learnt about clinical process redesign. eMedical Journal of Australia 2008; 188 (6 Suppl) S32-S35.
Morgan, Nick. How to Overcome “Change Fatigue”. Harvard Management Update, July 2001.
NHS (July, 2009) Improvement Leaders Guides
www.institute.nhs.uk/improvementleadersguides
Orr, Deborah. The NHS is suffering from reform fatigue. The Independent, December 5, 2007.
Reinertsen JL, Bisognano M, Pugh MD. Seven Leadership Leverage Points for Organization-Level Improvement in Health Care (Second Edition). Cambridge, Massachusetts: Institute for HealthcareImprovement; 2008. Reinertsen, James, Pugh, Michael, Nolan, Tom. Institute for Health Improvement “Executive
Review of Improvement Projects: A Primer for CEOs and other Senior Leaders”
http://www.ihi.org/IHI
Wheatley, Margaret, Kellner-Rogers, Myron. Bringing Life to Organizational Change. Journal
for Strategic Performance Measurement, April/May 1998

27
Wheatley, Margaret. Innovation Means Relying on Everyone’s Creativity. Leader to Leader,
Spring 2001 http://www.margaretwheatley.com/writing.html
Wheatley, Margaret. Relationships: The Basic Building Blocks of Life. 2006
http://www.margaretwheatley.com/writing.html