Embed Size (px)
Citation preview

11
Prevention and Management Prevention and Management
of hypertensive strokeof hypertensive stroke
Dr. LO, ManDr. LO, Man--waiwai
MBChB (CUHK)MBChB (CUHK)
MRCP (UK)MRCP (UK)
MPH (CUHK)MPH (CUHK)
FHKCPFHKCP
FHKAM (Medicine)FHKAM (Medicine)
Specialist in NeurologySpecialist in Neurology
Dept. of MedicineDept. of Medicine
Queen Elizabeth HospitalQueen Elizabeth Hospital
4 Dec 20064 Dec 2006
ContentContent
�� How does HT cause stroke?How does HT cause stroke?
�� What are the clinical and radiological What are the clinical and radiological manifestations for HTmanifestations for HT--related stroke?related stroke?
�� How should we lower BP in acute stroke?How should we lower BP in acute stroke?
�� What is the current concepts in antiWhat is the current concepts in anti--hypertensive therapy for prevention of hypertensive therapy for prevention of first and recurrent stroke?first and recurrent stroke?

22
How does HT cause stroke?How does HT cause stroke?
LipohyalinosisLipohyalinosis
Fibrinoiddegeneration
AtherosclerosisAtherosclerosis

33

44

55
Cortical infarction
MCA territory infarction

66
ACA territory infarction
PCA territory infarction

77
ACA
MCA
PCA
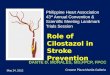
Lacunar Infarct
88
Lacunar Infarct
Binswanger’s disease

99
BinswangerBinswanger’’ss diseasedisease
�� SubcorticalSubcortical arterioscleroticarteriosclerotic
encephalopathyencephalopathy
�� Chronic small vessel diseaseChronic small vessel disease
�� Vascular parkinsonismVascular parkinsonism
�� Lower half parkinsonismLower half parkinsonism
BinswangerBinswanger’’ss diseasedisease
�� ApathyApathy
�� Gait Gait apraxiaapraxia
�� Small step gaitSmall step gait
�� HyperreflexiaHyperreflexia
�� Extensor plantar reflexesExtensor plantar reflexes
�� SubcorticalSubcortical dementia dementia –– cognitive slowingcognitive slowing

1010
Cardioembolicstroke
hypertensive hemorrhage

1111
Basal ganglia haemorrhage
Pontinehaemorrhage

1212
Cerebellar haemorrhage
SubarachnoidSubarachnoid haemorrhagehaemorrhage

1313
SAH
AntiplateletAntiplatelet agentsagents
Aspirin
� small benefit in reducing the death and recurrent stroke rate
� net decrease of 9deaths or occurrences of further stroke per 1000 patients (level Ia)

1414
IV IV thrombolysisthrombolysis
FDA approval 1996FDA approval 1996iv tPA iv tPA <3 hr<3 hr improved outcome at 3 monthsimproved outcome at 3 months
NINDSNINDS
TPATPA--treated group treated group were at least were at least 30%30%more likely to have more likely to have minimal or no minimal or no disability at 3 disability at 3 monthsmonths
Benefit were Benefit were consistent consistent regardless of age, regardless of age, stroke subtype or stroke subtype or prior use of aspirinprior use of aspirin �

1515
6.4% tPA vs. 0.6% in placebo (within 36hrs)
Mortality rate in both treatment group was similar at 3mo & at 1 year
1616
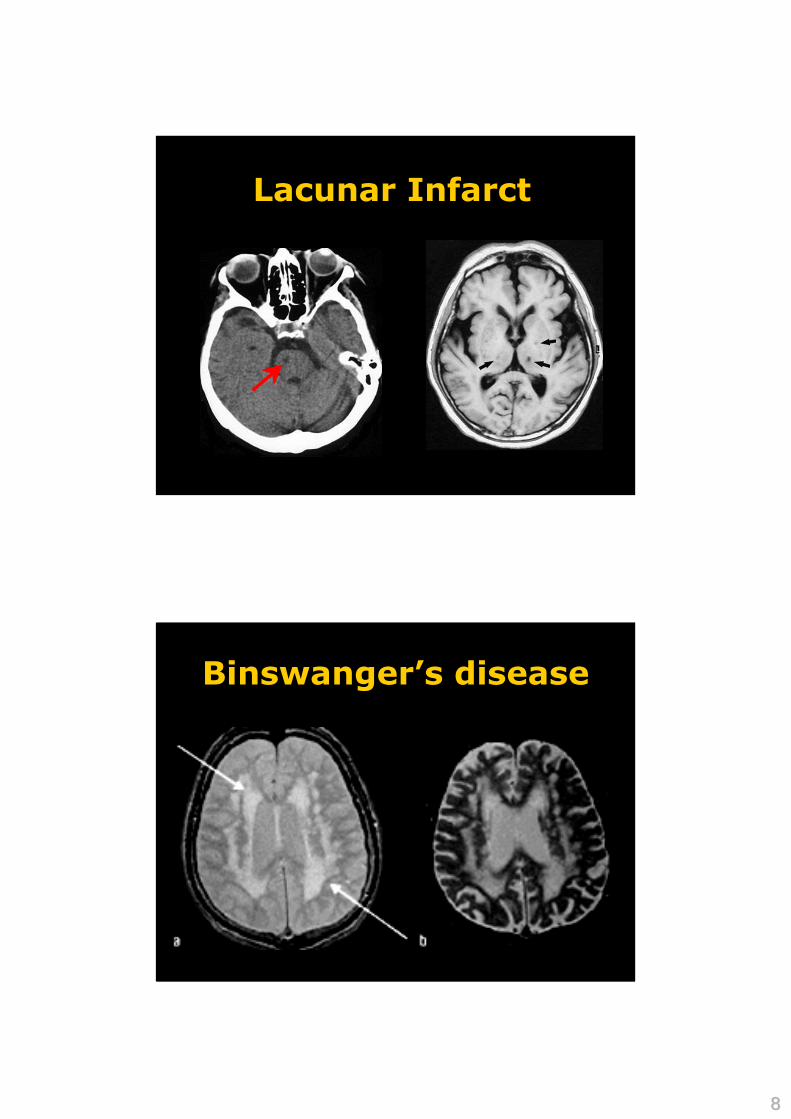
IntraIntra--arterial arterial
thrombolysisthrombolysis
MERCI balloon guide MERCI balloon guide
cathetercatheterFDA August 11, 2004 FDA August 11, 2004
1st medical 1st medical device device specifically specifically
indicated to indicated to --
retrieve blood clots from the retrieve blood clots from the
brain in ischemic stroke for brain in ischemic stroke for --
patients who fail or are patients who fail or are
ineligible for iv tPAineligible for iv tPA

1717
BP lowering BP lowering in acute phasein acute phase
IschaemicIschaemic penumbrapenumbra

1818
IschaemicIschaemic penumbrapenumbra
Cerebral Cerebral autoregulationautoregulation

1919
Cerebral Cerebral autoregulationautoregulation
Normotensive patient
Hypertensive patient
CBF
Mean arterial BP
BP management in acute BP management in acute
ischaemicischaemic strokestroke
�� CBF is pressure dependent in CBF is pressure dependent in ischaemicischaemic
brain regionsbrain regions
�� Further reduction Further reduction
�� irreversibly injure theirreversibly injure the ischaemicischaemic
penumbra penumbra
�� increase stroke volumeincrease stroke volume

2020
BP management in BP management in
acute acute ischaemicischaemic strokestroke
�� Transient HT Transient HT –– common after acute common after acute ischaemicischaemic strokestroke
�� Causes: Causes: �� anxietyanxiety
�� painpain
�� neuroendocrineneuroendocrine factorsfactors
�� stroke locationstroke location
�� compensatory response to brain hypoxia or compensatory response to brain hypoxia or increased ICPincreased ICP
BP management in acute BP management in acute
ischaemicischaemic strokestroke
�� Manage stress responses, pain, nausea and Manage stress responses, pain, nausea and vomiting, bladder distension or other sources of vomiting, bladder distension or other sources of anxietyanxiety
�� Early BP elevations often decline spontaneously Early BP elevations often decline spontaneously during the first minutes to hours during the first minutes to hours
�� May not require pharmacologic RxMay not require pharmacologic Rx

2121
Blood pressure decreaseBlood pressure decrease during the during the acute acute
phasephase of ischemic stroke is associated with of ischemic stroke is associated with
brain injury and poor stroke outcomebrain injury and poor stroke outcome
Castillo J, Castillo J, LeiraLeira R, Garcia MM, Serena J, Blanco M, R, Garcia MM, Serena J, Blanco M, DavalosDavalos A.A.
Stroke. 2004 Feb;35(2):520Stroke. 2004 Feb;35(2):520--6. 6. EpubEpub 2004 Jan 15. 2004 Jan 15.
Power Grade 3/5
Power Grade 1/5
Anti-HT Drugfor BP 180/90

2222
““Stroke in evolutionStroke in evolution””??
NonNon--specificspecific
�� Failure of collateral circulationFailure of collateral circulation
�� Systemic hypotensionSystemic hypotension
�� Cardiac Cardiac arrthymiaarrthymia
�� EmbolizationEmbolization or propagation of thrombusor propagation of thrombus
�� Progressive occlusion of vessel lumenProgressive occlusion of vessel lumen
�� Psychological depressionPsychological depression
�� SepsisSepsis
�� SeizuresSeizures
Any conditions deserve Any conditions deserve
BP lowering?BP lowering?
� AMI
� Aortic dissection
� Hypertensive encephalopathy
� Severe left heart failure
� Post-thrombolysis

2323
Consensus for BP Consensus for BP MxMx(not eligible for (not eligible for thrombolysisthrombolysis))
Sodium Sodium nitroprussidenitroprusside 0.5 0.5 µµm/kg per min IV m/kg per min IV
with continuous BP monitoring with continuous BP monitoring
(target 10%(target 10%––15% reduction)15% reduction)
DBP >140 mm Hg DBP >140 mm Hg
LabetalolLabetalol OR OR nicardipinenicardipine
(target 10%(target 10%––15% reduction) 15% reduction)
SBP >220 mm Hg SBP >220 mm Hg
or or
DBP 121DBP 121––140 mm Hg 140 mm Hg
Observe BPObserve BP
unless end organ involvementunless end organ involvement
SBP <220 mm Hg SBP <220 mm Hg
or or
DBP <120 mm Hg DBP <120 mm Hg
Guidelines for the Early Management of Patients With Ischemic StGuidelines for the Early Management of Patients With Ischemic Stroke roke
Stroke.Stroke. 2003;34:1056 2003;34:1056
Resume previous antiResume previous anti--HT Rx?HT Rx?
Those already taking antiThose already taking anti--HT Rx:HT Rx:
�� Resume drugs to avoid Resume drugs to avoid rebound HTrebound HT
� Maintain::
SBP 180–220 mm Hg
DBP < 120 mm Hg

2424
LabetololLabetolol
�� Selective Selective αα11 antagonist antagonist
�� ßß11 & & ßß22 antagonistantagonist
�� Decrease systemic vascular Decrease systemic vascular
resistance through resistance through αα blockadeblockade
�� BetaBeta--blocking reflex tachycardia blocking reflex tachycardia
induced by vasodilatationinduced by vasodilatation
LabetololLabetolol
Does not affect cerebral blood flowDoes not affect cerebral blood flow
Dosing regimen 10Dosing regimen 10--20mg iv (over 120mg iv (over 1--2 min) 2 min)
every 15every 15--20min 20min
DoubingDoubing of each subsequent dose is of each subsequent dose is
recommendedrecommended

2525
Sublingual Sublingual NifedipineNifedipine
�� Should be avoidedShould be avoided
�� Cause precipitous reduction in BPCause precipitous reduction in BP
AdalatAdalat 5mg S.L. stat5mg S.L. statX
Bring home message:Bring home message:
DonDon’’t lower BP in acute t lower BP in acute ischaemicischaemic stroke if stroke if
SBP <220 mm Hg
or
DBP <120 mm Hg
2626
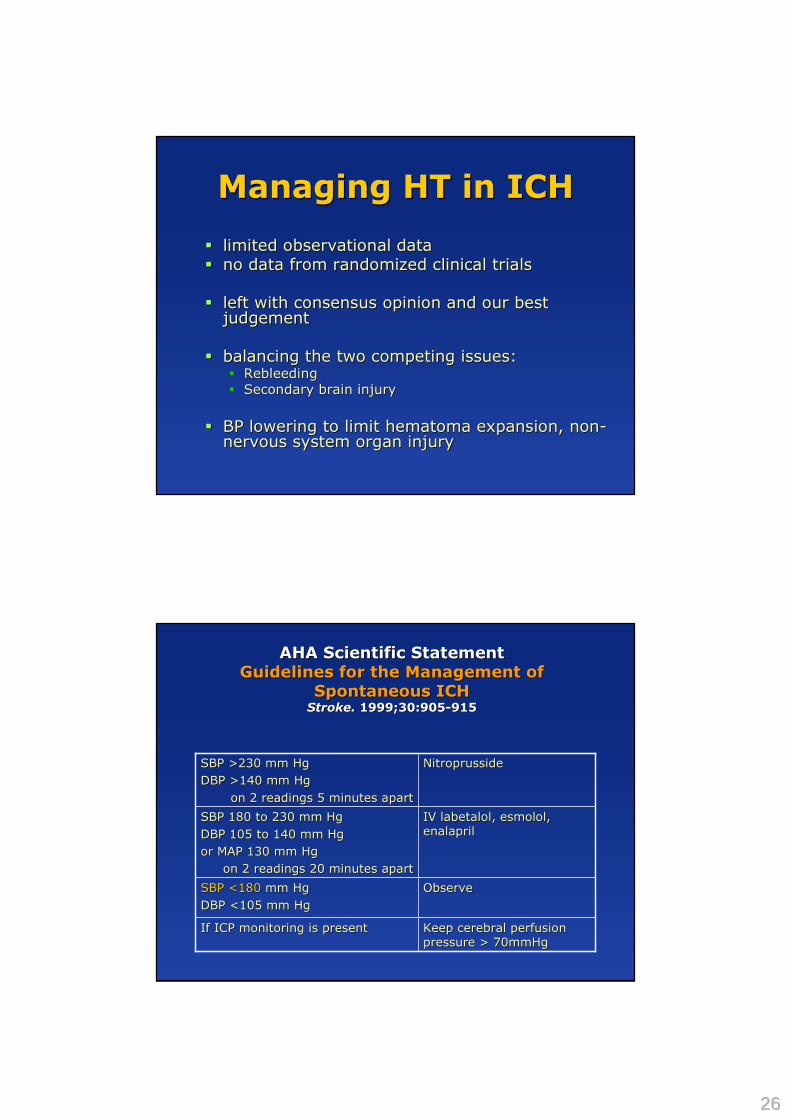
Managing HT in ICHManaging HT in ICH
�� limited observational data limited observational data
�� no data from randomized clinical trialsno data from randomized clinical trials
�� left with consensus opinion and our best left with consensus opinion and our best judgementjudgement
�� balancing the two competing issues: balancing the two competing issues: �� RebleedingRebleeding
�� Secondary brain injurySecondary brain injury
�� BP lowering to limit BP lowering to limit hematomahematoma expansion, nonexpansion, non--nervous system organ injurynervous system organ injury
Keep cerebral perfusion Keep cerebral perfusion
pressure > 70mmHgpressure > 70mmHgIf ICP monitoring is presentIf ICP monitoring is present
Observe Observe SBP <180SBP <180 mm Hgmm Hg
DBP <105 mm HgDBP <105 mm Hg
IV IV labetalollabetalol, , esmololesmolol, ,
enalaprilenalaprilSBP 180 to 230 mm HgSBP 180 to 230 mm Hg
DBP 105 to 140 mm HgDBP 105 to 140 mm Hg
or MAP 130 mm Hg or MAP 130 mm Hg
on 2 readings 20 minutes aparton 2 readings 20 minutes apart
NitroprussideNitroprussideSBP >230 mm HgSBP >230 mm Hg
DBP >140 mm HgDBP >140 mm Hg
on 2 readings 5 minutes aparton 2 readings 5 minutes apart
AHA Scientific StatementAHA Scientific Statement
Guidelines for the Management of Guidelines for the Management of
Spontaneous ICHSpontaneous ICHStroke.Stroke. 1999;30:9051999;30:905--915 915

2727
Primary preventionPrimary prevention

2828
Risk factors for strokeRisk factors for stroke
NonNon--modifiablemodifiable
�� NonNon--white ethnicitywhite ethnicity
�� Male sexMale sex
�� Older ageOlder age
�� Positive family history Positive family history
ModifiableModifiable
�� HTHT
�� SmokingSmoking
�� Excessive alcohol intake Excessive alcohol intake (>60g/d)(>60g/d)
�� ObesityObesity
�� DyslipidaemiaDyslipidaemia
�� DMDM
�� Carotid artery diseaseCarotid artery disease
�� AFAF
�� CHFCHF
Blood Pressure and Stroke: An Overview of Published ReviewsBlood Pressure and Stroke: An Overview of Published ReviewsCarlene M.M. Carlene M.M. LawesLawes, Derrick A. Bennett, , Derrick A. Bennett, ValeryValery L. L. FeiginFeigin, and Anthony Rodgers, and Anthony Rodgers
Stroke 2004 35: 776 Stroke 2004 35: 776 -- 785785

2929
BP level & risk of vascular BP level & risk of vascular
diseasedisease
�� JNC VIIJNC VII
�� Risk begins at 115/75 Risk begins at 115/75 mmHgmmHg
�� No limits below this No limits below this pointpoint
�� No JNo J--curve responsecurve response
Stage 2 HT
Stage 1 HT
Prehypertension
Normal
120120
140140
160160
8080 1001009090
SBPSBP
DBPDBP
Classification of BP by JNC 7Classification of BP by JNC 7

3030
Which drug should we use?Which drug should we use?
Any class effect?Any class effect?
Blood Pressure Lowering Treatment Trialists' Collaboration. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomized trials.
Lancet. 2003;362:1527-1535.
Comparison with placeboComparison with placebo

3131
Blood Pressure Lowering Treatment Trialists' Collaboration. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomized trials.
Lancet. 2003;362:1527-1535.
Direct comparison between Direct comparison between antianti--HT regimenHT regimen
Size does matterSize does matter
Size (intensity)Size (intensity)
of BP of BP ��
Type of Type of
antianti--HT RxHT Rx

3232
Compelling reasons & Compelling reasons &
recommendationsrecommendations
����������������Recurrent Recurrent CVACVA
����������������CRFCRF
����������������������������������������DMDM
��������������������������������High CHD High CHD riskrisk
������������������������PostPost--MIMI
����������������������������������������CHFCHF
AldosteroneAldosteroneAntagonistAntagonist
CCBCCBARBARBACEIACEIBB--blockerblockerDiureticDiuretic

3333
Stage 2 HT
Stage 1 HT
Prehypertension
Normal120120
140140
160160
8080 1001009090
SBPSBP
DBPDBP
Lifestyle modification��������
Compelling indications? treatY
Stage 2 HT
Stage 1 HT
Prehypertension
Normal120120
140140
160160
8080 1001009090
SBPSBP
DBPDBP
Lifestyle modification��������
Treat with Treat with
thiazidethiazideACEI, ARB, BB, CCB,ACEI, ARB, BB, CCB,
or combinationor combination
��������

3434
Stage 2 HT
Stage 1 HT
Prehypertension
Normal120120
140140
160160
8080 1001009090
SBPSBP
DBPDBP
Lifestyle modification��������
2 drugs combinations2 drugs combinations
ThiazideThiazide + ACEI/ARB/BB/CCB+ ACEI/ARB/BB/CCB
Central Central PontinePontine
MyelinolysisMyelinolysis

3535
What are the risk factors for What are the risk factors for
thiazidethiazide induced induced hyponatremiahyponatremia??
�� AgeAge
�� Low body Low body
massmass
�� HypokalemiaHypokalemia
Risk factors for Risk factors for thiazidethiazide--induced induced hyponatraemiahyponatraemia..
K.M. Chow, C.C. K.M. Chow, C.C. SzetoSzeto, T.Y., T.Y.--H. Wong, C.B. Leung P.K.H. Wong, C.B. Leung P.K.--T. Li T. Li
Q J Med 2003; 96: 911Q J Med 2003; 96: 911--917917
Stroke prevention in DiabeticsStroke prevention in Diabetics
�� 40 40 –– 60% adult with type 2 DM have HT60% adult with type 2 DM have HT
�� Any difference in BP management for Any difference in BP management for this special group of patients to prevent this special group of patients to prevent stroke?stroke?

3636
UKPDS UKPDS Event Rates for Select Event Rates for Select Endpoints With Endpoints With
Tight Tight vsvs Less Tight Blood Pressure ControlLess Tight Blood Pressure Control
0
10
20
30
40
50
60
70
80
Any DM-related endpoint
DM-
related deathStroke Microvascular
complications
Events per 1000 patient yrs P=0.005
P=0.02 P=0.01 P=0.009
Less tight (n=390) mean achieved BP 154/87 mmHg
Tight (n=758) mean achieved BP 144/82 mmHg
UKPDS Group. BMJ. 1998;317:703–713.
-33
-25
-21
-16
-12
-50
-40
-30
-20
-10
0
Microalbuminuria at 12 yrs Microvascular complications
Retinopathy Myocardial Infarction
Any DM endpoint
% relative risk reduction
P=0.03
P<0.01
P<0.01
P=0.05
P=0.02
UKPDS Group. Lancet. 1998;352:837-853.
UKPDS Relative Risk Reduction for UKPDS Relative Risk Reduction for Intensive Intensive vsvs Less Intensive Less Intensive Glucose ControlGlucose Control
Over 10 years, HbA1c was 7.0% (6.2-8.2) in the intensive group (n=2,729) compared with 7.9% (6.9-8.8) in the conventional group (n=1,138).

3737
UKPDS Findings:UKPDS Findings:Tight BP Control vs. Intensive Glucose ControlTight BP Control vs. Intensive Glucose Control
�� Tight vs. Less tightTight vs. Less tight BP control BP control reduces risk ofreduces risk of
�� Any diabetesAny diabetes--related endpoint related endpoint 24% 24% P=0.005P=0.005
�� MicrovascularMicrovascular complicationscomplications 37% 37% P=0.009P=0.009
�� Stroke Stroke 44% 44% P=0.01P=0.01
�� Intensive vs. Conventional Intensive vs. Conventional glucose controlglucose control policy policy reduces risk of reduces risk of
�� Any diabetesAny diabetes--related endpoint related endpoint 12% 12% P=0.03P=0.03
�� MicrovascularMicrovascular complications complications 25% 25% P<0.01P<0.01
�� Myocardial infarctionMyocardial infarction 16% 16% P=0.05P=0.05
UKPDS Group. BMJ. 1998;317:703–712.UKPDS Group. Lancet. 1998;352:837-853.
““Is ACEI/ARB better for diabetics ?Is ACEI/ARB better for diabetics ?””
Angiotensinogen
⇑⇑⇑⇑ Angiotensin I
⇑⇑⇑⇑ Angiotensin II
AT1 AT2 ATn
Bradykinin
Inactivepeptides
Non-renin(eg tPA)
Non-ACE(eg chymase) ACE
Renin

3838
ABCD, CAPPP, FACET ABCD, CAPPP, FACET
and UKPDS Metaand UKPDS Meta--AnalysisAnalysis
�� Is ACEI superior to other agents in the prevention of Is ACEI superior to other agents in the prevention of
cardiovascular events in cardiovascular events in hypertensive type 2 hypertensive type 2
diabetics?diabetics?
Pahor M, et al. Diabetes Care. 2000;23:888-892.
atenololcaptoprilcaptopril758758UKPDSUKPDS
amlodipinefosinoprilfosinopril380380FACETFACET
Diuretic or BBcaptoprilcaptopril572572CAPPPCAPPP
nisoldipineenalaprilenalapril470470ABCDABCD
OthersOthersACEIACEISizeSize
Relative Risk Reduction With Relative Risk Reduction With ACEIsACEIsin ABCD, CAPPP and FACETin ABCD, CAPPP and FACET
-24-24-24-24
-43-43-43-43
-63-63-63-63
-51-51-51-51
-70-70-70-70
-60-60-60-60
-50-50-50-50
-40-40-40-40
-30-30-30-30
-20-20-20-20
-10-10-10-10
0000
% relative risk reduction
Pahor M, et al. Diabetes Care. 2000;23:888-892.
AMI CVS Event StrokeAll-cause Mortality
P<0.001
P<0.001
P=0.01
NS

3939
0
5
10
15
20
25Placebo Ramipril
Combined primary endpoint*
Myocardial infarction
Stroke Cardiovascular death
RR=25%P<0.001
RR=22%P=0.01
RR=33%P=0.007
RR=37%P<0.001
Events per patient group (%)
*The occurrence of myocardial infarction, stroke or cardiovascular death
HOPE Study Investigators. Lancet. 2000;355:253-259.
MICROMICRO--HOPEHOPE substudiessubstudies of DM patientsof DM patients
RamiprilRamipril (n = 3,577)(n = 3,577)
LIFE Study LIFE Study Diabetes SubgroupDiabetes Subgroup
((LorsartanLorsartan))
Lindholm LH, et al. Lancet. 2002;359:1004-1010.
0.5 1 1.5Favors atenolol
Adjusted hazard ratio (95% CI)
No. of events
Favors losartan
P value
Composite
CV Death
Stroke
Myocardialinfarction
Total Mortality
242
99
116
91
167
0.031
0.028
NS
NS
0.002
Endpoints
21%

4040
ImplicationsImplications
� Tight control of HT with ACEI or ARB treatment reduces the risk of stroke in persons with DM
� Glycemic control reduces microvascularcomplications, but evidence showing a reduction in stroke risk with tight glycemic control is lacking
ASA/AHA 2006 recommendationASA/AHA 2006 recommendation
Primary stroke prevention for Primary stroke prevention for
DiabeticsDiabetics
�� Tight BP controlTight BP control
�� Keep BP < 130/ 80 Keep BP < 130/ 80
mmHgmmHg
�� Consider ACEI/ Consider ACEI/
ARBARB

4141
Case Case scenerioscenerio
Chan Tai ManChan Tai Man M/52M/52
BP 145/ 85 p70BP 145/ 85 p70 HstixHstix 2hr pp 16.32hr pp 16.3
HypertensionHypertension
StrokeStroke
StrokeStroke
x
x
PrimaryPrimaryPreventionPrevention
SecondarySecondaryPreventionPrevention

4242
ACEI for 2ACEI for 2ndnd stroke prevention? stroke prevention?
�� HOPE HOPE �� RamiprilRamipril vs. Placebo vs. Placebo
�� for 1013 patients with for 1013 patients with HxHx of stroke/TIAof stroke/TIA
�� 24% RR (95% CI, 5 24% RR (95% CI, 5 –– 40) stroke, MI or vascular 40) stroke, MI or vascular death; (n =1013)death; (n =1013)
�� BP lowering 3/2mm Hg (Office BP)BP lowering 3/2mm Hg (Office BP)
�� HOPE HOPE substudysubstudy (Ambulatory BP)(Ambulatory BP)�� 10/4 mmHg reduction over 24hr10/4 mmHg reduction over 24hr�� 17/8 mmHg reduction during nighttime17/8 mmHg reduction during nighttime�� �� BP lowering effect leading to stroke risk reduction?BP lowering effect leading to stroke risk reduction?
Comparative Effects of Ramipril on Ambulatory and Office Blood PressuresPer Svensson; Ulf de Faire; Peter Sleight; Salim Yusuf; Jan Östergren
Hypertension. 2001;38:e28
PROGRESS PROGRESS ((perindoprilperindopril))�� N = 6105N = 6105�� HxHx of stroke or TIAof stroke or TIA�� ACEI, ACEI + ACEI, ACEI + indapamideindapamide
�� Recurrent CVA:Recurrent CVA:�� 43% RRR (95% CI 30 43% RRR (95% CI 30 –– 54); 12/5 mmHg 54); 12/5 mmHg ��
�� Recurrent major CVS events:Recurrent major CVS events:�� 40% RRR (95% CI 29 40% RRR (95% CI 29 –– 49)49)
�� No benefit when ACEI was given aloneNo benefit when ACEI was given alone�� Benefit also shown in Benefit also shown in normotensivenormotensive patientspatients
PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6105 individuals with previous stroke or transient ischaemic attack.
Lancet. 2001;358:1033- 1041.

4343
AHA/ ASA Guideline 2006AHA/ ASA Guideline 2006Secondary Prevention of StrokeSecondary Prevention of Stroke
�� How much?How much?�� Benefit seen in reduction of ~10/5 mmHgBenefit seen in reduction of ~10/5 mmHg�� Normal BP < 120/80 mmHg by JNCNormal BP < 120/80 mmHg by JNC--77
All patients with All patients with ischaemicischaemic strokestroke
or TIAor TIAAntiAnti--HT RxHT Rx

4444
AHA/ ASA Guideline 2006AHA/ ASA Guideline 2006Secondary Prevention of StrokeSecondary Prevention of Stroke
�� Which drug?Which drug?
�� Optimal regimen Optimal regimen ––uncertainuncertain
�� Available data support:Available data support:�� Diuretic Diuretic
�� Diuretic + ACEI Diuretic + ACEI
�� Individualized with Individualized with patient characteristicspatient characteristics
Key messageKey message
�� Benefit for HT Rx is clearBenefit for HT Rx is clear
�� Choice of agent must be individualizedChoice of agent must be individualized
�� Reduction of BP is generally more Reduction of BP is generally more important than specific agentimportant than specific agent
�� ““Size does matter!Size does matter!””