Embed Size (px)
DESCRIPTION
Stroke Prevention –What is New?. Anne E. O’Duffy, MD Assistant Professor of Neurology Stroke Division Vanderbilt University Medical Center February 12, 2007. Vanderbilt Stroke News. JCAHO certified primary stroke center, Nov. 2005 - PowerPoint PPT Presentation
Citation preview

Anne E. O’Duffy, MDAnne E. O’Duffy, MD
Assistant Professor of NeurologyAssistant Professor of Neurology
Stroke DivisionStroke Division
Vanderbilt University Medical CenterVanderbilt University Medical Center
February 12, 2007February 12, 2007
Stroke Prevention –What is Stroke Prevention –What is New?New?

Vanderbilt Stroke NewsVanderbilt Stroke News
• JCAHO certified primary stroke center, JCAHO certified primary stroke center, Nov. 2005Nov. 2005
• 4 members of the Vanderbilt Neurology 4 members of the Vanderbilt Neurology Stroke Division are the only Board Stroke Division are the only Board Certified Vascular Neurologists in the Certified Vascular Neurologists in the state of TNstate of TN

Stroke Morbidity and Mortality
A leading cause of serious, long-term disability
730,000 new or recurrent strokes occur per year in the US
Third leading cause of death in the US, stroke accounted for 167,400 deaths in 1999; second leading cause worldwide
Accounts for > 50% of all hospitalizations for acute neurological disease
American Heart Association, 2002 Heart and Stroke Statistical Update.

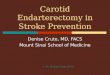
Prognosis of Ischemic StrokeGerman Stroke Data Bank
Follow-up after 90 days
14.70%
57.20%
18.60%
9.40%
Deceased
Slight disabilities (mRS 0-2)Moderate disabilities (mRS 3)
Severe disabilities (mRS 4-5)
Grau AJ, et al. Stroke 2001;32:2559-2566.
n = 5,017

Annual Total(2001) Per Event*
Direct costs(care and treatment)
Indirect costs(lost productivity)
$28.0 billion
$17.4 billion
$45.4 billionTotal
$46,667
$29,000
$75,667
*Based on 730,000 strokes per year
The High Cost of Stroke
American Heart Association, 2001 Heart and Stroke Statistical Update.

Stroke MortalityStroke Mortality

Stroke SubtypesStroke Subtypes

TIA/Stroke Survivor’s Greatest Risk is Stroke, not MI
Recurrence of Events in Antiplatelet Trials in TIA and Ischemic Stroke Patients
2.5%
6.5%
2.5%
13.5%12.5% 12.5%
10.0%
1.5%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
CATSN=1,053
TASSN=3,069
CAPRIE*N=6,431
ESPS 2N=6,602
Per
cent
of p
atie
nts
with
eve
nts
Stroke MI
Albers GW. Neurology 2000;54:1022-1028. *Stroke patient subgroup only (n = 6,431)

Short-term Prognosis after Emergency Department Diagnosis of TIA
Johnston SC, et al. JAMA 2000;284:2901-2906.
10.5%
12.7%
2.6% 2.6%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
Stroke RecurrentTIA
CV event Death
Outcome events Inclusion criteria:
Objective:
Outcome measures:
Total events:
TIA by ED physicians
Short-term risk of strokeafter ED diagnosis
Risk of stroke and otherevents during the 90 daysafter index TIA
25.1%
Within48 hr
Within90 days
5.3%

TIA and Stroke as Predictors of Secondary Stroke
Sacco. Neurology 1997;49(suppl 4):S39-S44.Feinberg, et al. Stroke 1994;25:1320-1335.
4 – 8
12 – 13
24 – 29
30 days
1 year
5 years
3 – 10
5 – 14
25 – 40
Post-Stroke (%)Post-TIA (%)

• 61 year-old man with 61 year-old man with history of HTN, afib, history of HTN, afib, prior stroke 2001, prior stroke 2001, abrupt onset right abrupt onset right hemiparesis 6:50PM hemiparesis 6:50PM while at work, global while at work, global aphasia, INR 1.6aphasia, INR 1.6
• CT outside ER: CT outside ER: hyperdense MCA hyperdense MCA signsign


We (Still) Must We (Still) Must Focus on Focus on
PREVENTION!PREVENTION!

Stroke PreventionStroke Prevention
• Stroke, February, 2006. AHA/ASA/AAN Stroke, February, 2006. AHA/ASA/AAN guidelines on stroke prevention in guidelines on stroke prevention in patients with TIA and strokepatients with TIA and stroke
• Summary with guidelines and levels of Summary with guidelines and levels of evidenceevidence
• Well-referenced, single sourceWell-referenced, single source

Adapted from Goldstein, et al. Circulation 2001;103:163-182.
68% (warfarin)21% (aspirin)
Atrial fibrillation (non-valvular)
20-30% with statins in patients with known coronary heart disease
Hyperlipidemia
44% reduction in hypertensive diabetics with tight blood pressure control
Diabetes
50% within 1 year, baseline after 5 yearsSmoking
30% - 40%Hypertension
Risk reduction with treatmentFactor
Potential Stroke Risk Reduction for IndividualsAHA Guidelines

Stroke Risk and BPStroke Risk and BP
UK-TIA trial BMJ 313 (1996), p. 147

HypertensionHypertension
• Commonest stroke risk factor, 50 million Commonest stroke risk factor, 50 million Americans, undertreatedAmericans, undertreated
• HOPE suggested that ACE-I ramipril HOPE suggested that ACE-I ramipril reduced stroke, MI, vascular death by reduced stroke, MI, vascular death by 22% greater than placebo (32% 22% greater than placebo (32% reduction in stroke)reduction in stroke)
• Yusef,et al NEJM 2000; 342: 145-153Yusef,et al NEJM 2000; 342: 145-153
• LIFE 1LIFE 1° stroke prevention trial in high-° stroke prevention trial in high-risk pts losartin better than atenololrisk pts losartin better than atenolol
• Dahlof et al Lancet 2002; 359: 995-1003Dahlof et al Lancet 2002; 359: 995-1003

HypertensionHypertension
• PROGRESS 2° stroke prevention in 6105 PROGRESS 2° stroke prevention in 6105 patients w/ hx stroke/TIA (irregardless of patients w/ hx stroke/TIA (irregardless of history of HTN) perindopril w/ or w/o history of HTN) perindopril w/ or w/o indapamide vs placebo found 28% indapamide vs placebo found 28% reduction in stroke in ‘active tx’ arm and reduction in stroke in ‘active tx’ arm and 43% reduction w/combination therapy43% reduction w/combination therapy
• Lancet, Vol. 358: September 29,2001Lancet, Vol. 358: September 29,2001

PROGRESS Results:PROGRESS Results:

PROGRESS Results:PROGRESS Results:
BPBP
changechange
Stroke Stroke reduction reduction
(95% CI)(95% CI)
NNT NNT for for
1 yr 1 yr
(mm/Hg)(mm/Hg)
All PatientsAll Patients 9/49/4 28% 28% (17, 38)(17, 38) 115115
Perindopril Perindopril onlyonly
5/35/3 5% 5% (-19, 23)(-19, 23) --
Both agentsBoth agents 12/512/5 43% 43% (30, 54)(30, 54) 7070

HypertensionHypertension
• ALLHAT trial: 33,000 pts w/ HTN and 1 other ALLHAT trial: 33,000 pts w/ HTN and 1 other vascular risk factor tx w/ chlorthalidone, vascular risk factor tx w/ chlorthalidone, lisinopril or amlodipinelisinopril or amlodipine
• No differences in 1No differences in 1° outcome measures of fatal ° outcome measures of fatal or non-fatal MI, chlorthalidone was better than or non-fatal MI, chlorthalidone was better than lisinopril in preventing stroke and combined lisinopril in preventing stroke and combined vascular endpoint of stroke, MI, and PVDvascular endpoint of stroke, MI, and PVD
• Nearly 30% pts were black and thus more Nearly 30% pts were black and thus more likely to do better w/ diureticslikely to do better w/ diuretics
• JAMA, December 18,2002—Vol 288,no 23,2981-97JAMA, December 18,2002—Vol 288,no 23,2981-97

HypertensionHypertension
• Specific BP agent may be less important Specific BP agent may be less important than BP lowering for stroke preventionthan BP lowering for stroke prevention
• The Seventh Report of the Joint National The Seventh Report of the Joint National Committee on Prevention, Detection, Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Evaluation, and Treatment of High Blood Pressure—The JNC 7 ReportPressure—The JNC 7 Report
• JAMA, May 21, 2003—Vol 289, No. 19, 2560-72JAMA, May 21, 2003—Vol 289, No. 19, 2560-72

Lipid LoweringLipid Lowering
• Statins very effective in stroke reduction Statins very effective in stroke reduction in pts w/ CAD:in pts w/ CAD:– 4S, CARE, LIPID trials shown 19-4S, CARE, LIPID trials shown 19- 28% 28%
reduction in stroke outcomes in CAD ptsreduction in stroke outcomes in CAD pts
• SPARCL (Stroke Prevention by SPARCL (Stroke Prevention by Aggressive Reduction in Cholesterol Aggressive Reduction in Cholesterol Levels) 2Levels) 2° stroke prevention, NEJM ° stroke prevention, NEJM 2006; 355:549-5592006; 355:549-559

SPARCL Results, StrokeSPARCL Results, Stroke

SPARCLSPARCL
• 4731 pts. w/cerebrovascular disease, no 4731 pts. w/cerebrovascular disease, no known CAD were randomized to 80 mg known CAD were randomized to 80 mg atorvastatin vs. placeboatorvastatin vs. placebo
• Mean f/up 4.9 yearsMean f/up 4.9 years
• 16% RRR of recurrent stroke16% RRR of recurrent stroke
• Absolute RR 2.2%Absolute RR 2.2%

Women’s Estrogen for Stroke Women’s Estrogen for Stroke Trial (WEST)Trial (WEST)
• Randomized, double-blind, placebo-Randomized, double-blind, placebo-controlled trial of estrogen therapy in 664 controlled trial of estrogen therapy in 664 postmenopausal women who had recently postmenopausal women who had recently had an ischemic stroke or TIA, mean had an ischemic stroke or TIA, mean follow-up of 2.8 yearsfollow-up of 2.8 years
• Results: Estrogen therapy did not reduce Results: Estrogen therapy did not reduce the risk of death alone, or of nonfatal the risk of death alone, or of nonfatal stroke:stroke:

WEST ResultsWEST Results

Women’s Health Initiative Women’s Health Initiative (WHI)(WHI)
• Defining the risks and benefits of strategies that Defining the risks and benefits of strategies that could potentially reduce the incidence of heart could potentially reduce the incidence of heart disease, breast and colorectal cancer, and disease, breast and colorectal cancer, and fractures in postmenopausal womenfractures in postmenopausal women
• 16,608 women, primary outcome was CHD16,608 women, primary outcome was CHD• Study stopped early after mean follow-up of 5.2 Study stopped early after mean follow-up of 5.2
years based on health risks that exceeded years based on health risks that exceeded benefits benefits
JAMA.2002;288:321-333JAMA.2002;288:321-333

WHI Results for StrokeWHI Results for Stroke

WHI ResultsWHI Results
• HR’s for CHD 1.29, breast cancer 1.26, HR’s for CHD 1.29, breast cancer 1.26, stroke 1.41, PE 2.13, colorectal ca 0.63, stroke 1.41, PE 2.13, colorectal ca 0.63, endometrial ca 0.83, hip fractures 0.66, endometrial ca 0.83, hip fractures 0.66, other deaths 0.92other deaths 0.92
• Absolute excess risks per 10,000 person-Absolute excess risks per 10,000 person-yrs: 7 more CHD events, 8 more strokes yrs: 7 more CHD events, 8 more strokes (4800 total strokes/yr est.), 8 more PE’s, 8 (4800 total strokes/yr est.), 8 more PE’s, 8 more invasive breast ca’smore invasive breast ca’s
• Absolute risk reductions: 6 fewer Absolute risk reductions: 6 fewer colorectal ca’s, 5 fewer hip fractures colorectal ca’s, 5 fewer hip fractures

Antithrombotic TherapyAntithrombotic Therapy

Anticoagulation for Primary Stroke Prevention in Patients with Atrial Fibrillation
Hart RG. Ann Intern Med 1999;131:492-501.
100%
80%
60%
40%
20%
0%
AFASAKN=1,007
SPAF IN=1,330
BAATAFN=420
CAFAN=378
SPINAFN=571
Rel
ativ
e R
isk
Red
uctio
n
33%
86%
65%58%
79%
68%
Total patientsN=2,461

Antithrombotic Therapy in Secondary Preventionfor Patients with Atrial Fibrillation
European Atrial Fibrillation Trial (EAFT)
EAFT Study Group. Lancet 1993;342:1255-1262.
n = 439/728Inclusion criteria: TIA or non-severe stroke
66%
15%
80%
60%
40%
20%
0%
Anticoagulation vs. Placebo (INR 3-4.5)
ASA 300 mg vs. Placebo
Relative Risk Reduction

Rate vs. Rhythm?Rate vs. Rhythm?
• AFFIRM:AFFIRM:AAtrial trial FFibrillation ibrillation FFollow-up ollow-up IInvestigation of nvestigation of RRhythm hythm MManagementanagement
• >4000 high-risk patients w/afib>4000 high-risk patients w/afib
• Rhythm control just as likely to suffer Rhythm control just as likely to suffer ischemic stroke over 3.5 yrs. as those who ischemic stroke over 3.5 yrs. as those who receive rate control alonereceive rate control alone
• Warfarin reduced stroke by 68%Warfarin reduced stroke by 68%– Presented at AAN, Honolulu, HI, PI Sherman,DG, Presented at AAN, Honolulu, HI, PI Sherman,DG,


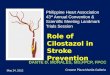
Kaplan-Meier Analyses of the Time to Recurrent Ischemic Stroke or Death According to Treatment Assignment
Days after Randomization
Pro
babi
lity
of E
vent
(%)
30
20
10
0
Aspirin
Warfarin
Mohr JP, et al for WARSS. N Engl J Med 2001;345:1444-1451.
Warfarin-Aspirin Recurrent Stroke Study (WARSS)
n = 2,206
0 90 180 270 360 450 540 630 720
No. At Risk
Warfarin 1,103 1,047 1,013 998 972 956 939 924 885
Aspirin 1,103 1,057 1,032 1,004 984 974 951 932 900


ESPS 2: Effects on Stroke—Survival Curves (“Non-event” Probability)
All patients
1.000
0.950
0.900
0.850
0.800
0.750
Survival probability
0 6 12 18 24
Time (months)
ASA/ER-DPER-DPASAPlacebo
ER-DP = Extended-Release DipyridamoleASA = Acetylsalicylic AcidDiener HC, et al. J Neurol Sci 1996;143:1-13.

ESPRITESPRIT
• Lancet 2006;367:1665-1673Lancet 2006;367:1665-1673
• 2763 pts. w/TIA or minor stroke 2763 pts. w/TIA or minor stroke randomized to low dose aspirin (30-randomized to low dose aspirin (30-325mg) with or w/out dipyridamole325mg) with or w/out dipyridamole
• Mean f/up 3.5 yearsMean f/up 3.5 years
• 20% RRR in vascular death, non-fatal 20% RRR in vascular death, non-fatal stroke or MIstroke or MI
• 1% absolute RR per year1% absolute RR per year

ESPRIT ResultsESPRIT Results

34
ACCP 2004 Guidelines for ACCP 2004 Guidelines for Ischemic Stroke Risk Reduction: Ischemic Stroke Risk Reduction: Antithrombotic TherapyAntithrombotic Therapy
Oral antiplatelet agents (Grade 1A) forOral antiplatelet agents (Grade 1A) fornoncardioembolic stroke:noncardioembolic stroke:
ACCP, American College of Chest PhysiciansAlbers GW et al. Chest. 2004;126:483S.
“Aspirin, 50 to 325 mg qd; the combination of aspirin and extended-release dipyridamole 25 mg/200 mg bid; or clopidogrel 75 mg qd. In these patients, we suggest use of the combination of aspirin and extended-release dipyridamole, 25/200 mg bid, over aspirin (Grade 2A) and clopidogrel over aspirin (Grade 2B).”
“In patients with atrial fibrillation and a recent stroke or TIA, we recommend long-term anticoagulation (target international normalized ratio, 2.5; range, 2.0 to 3.0) [Grade 1A].”
Oral anticoagulants for cardioembolic stroke:Oral anticoagulants for cardioembolic stroke:


MATCHMATCH
• MManagement of anagement of ATATherothrombosis with herothrombosis with CClopidogrel in lopidogrel in HHigh-risk patients with recent igh-risk patients with recent TIA or ischemic stroke TIA or ischemic stroke
• Plavix + aspirin vs Plavix alone in high-risk Plavix + aspirin vs Plavix alone in high-risk stroke/ TIA patients (MI, DM, PVD) stroke/ TIA patients (MI, DM, PVD)
• 7599 pts, 500+ centers, 28 countries7599 pts, 500+ centers, 28 countries• 15.7% of patients taking clopidogrel + ASA 15.7% of patients taking clopidogrel + ASA
had a further ischemic event vs 16.73% of had a further ischemic event vs 16.73% of patients taking clopidogrel + placebo (p=.244)patients taking clopidogrel + placebo (p=.244)

MATCH ResultsMATCH Results

EndpointEndpoint Placebo + Placebo + PlavixPlavix
ASA + ASA + PlavixPlavix
RRRRRR
(95% CI)(95% CI)
P valueP value
PrimaryPrimary 636 636 (16.73%)(16.73%)
596 596 (15.7%)(15.7%)
6.46.4
(-4.6,16.3)(-4.6,16.3)
0.2440.244
MIMI 62 62 (1.63%)(1.63%)
59 59 (1.55%)(1.55%)
Ischemic Ischemic strokestroke
319 319 (8.39%)(8.39%)
299 299 (7.87%)(7.87%)
CV deathCV death 74 74 (1.95%)(1.95%)
69 69 (1.82%)(1.82%)
Rehosp.Rehosp. 181 181 (4.76%)(4.76%)
169 169 (4.45%)(4.45%)

MATCH ResultsMATCH Results
• Life threatening bleeding 2.6 vs 1.3% Life threatening bleeding 2.6 vs 1.3%
P < 0.001P < 0.001
• Raises serious concern about use of Raises serious concern about use of combination anti-platelet agents in stroke combination anti-platelet agents in stroke patients patients

CHARISMACHARISMA
• NEJM 2006;354:1706-1717NEJM 2006;354:1706-1717
• 15,603 pts. with vascular disease (27% 15,603 pts. with vascular disease (27% stroke) randomized to clopidogrel vs. stroke) randomized to clopidogrel vs. placebo plus aspirinplacebo plus aspirin
• Clopidogrel no more effective than Clopidogrel no more effective than placebo in aspirin treated pts.placebo in aspirin treated pts.
• Increased bleeding complications with Increased bleeding complications with combinationcombination

CHARISMA ResultsCHARISMA Results

PRoFESSPRoFESS
• PPrevention revention RRegimen egimen FFor or EEffectively avoiding ffectively avoiding SSecond econd SStrokestrokes
• 2 x 2 factorial design: Aggrenox vs. clopidogrel 2 x 2 factorial design: Aggrenox vs. clopidogrel with or w/out Micardis (telmesartan)with or w/out Micardis (telmesartan)
• N= 18,000N= 18,000• Adults, >55 yrs, ischemic stroke within 90 daysAdults, >55 yrs, ischemic stroke within 90 days• Enrollment period 2 yrs, study duration 4 yrs.Enrollment period 2 yrs, study duration 4 yrs.


SPS3 (Secondary Prevention of SPS3 (Secondary Prevention of Small Subcortical Strokes)Small Subcortical Strokes)
• Multicenter phase III randomized 2x2 Multicenter phase III randomized 2x2 controlled trialcontrolled trial
• 2500 patients2500 patients• 325 mg aspirin vs aspirin + clopidogrel325 mg aspirin vs aspirin + clopidogrel• Targeted BP control: usual (systolic 130-Targeted BP control: usual (systolic 130-
149) vs. aggressive (systolic <130)149) vs. aggressive (systolic <130)• Primary efficacy outcome: recurrent Primary efficacy outcome: recurrent
stroke during mean follow-up 3 yrs.stroke during mean follow-up 3 yrs.• Secondary outcomes: cognitive status, Secondary outcomes: cognitive status,
major vascular events, deathmajor vascular events, death

IRIS (Insulin Resistance IRIS (Insulin Resistance Intervention after Stroke)Intervention after Stroke)
• Patients with recent stroke/TIA who are Patients with recent stroke/TIA who are found to be insulin resistant are treated found to be insulin resistant are treated with pioglitazone vs. placebo for 4 yearswith pioglitazone vs. placebo for 4 years
• Enrolling pts. > 45 years old, no hx. CHFEnrolling pts. > 45 years old, no hx. CHF

““A strategy to reduce cardiovascular A strategy to reduce cardiovascular disease by more than 80%”disease by more than 80%”
• Simultaneously reduce four CV risk factors Simultaneously reduce four CV risk factors (LDL cholesterol, BP, homocysteine, platelet (LDL cholesterol, BP, homocysteine, platelet function)function)
• 10mg atorvastatin or 40mg simvastatin, 3 BP 10mg atorvastatin or 40mg simvastatin, 3 BP meds at half-strength (thiazide, beta-blocker, meds at half-strength (thiazide, beta-blocker, ACE-I), 0.8mg folic acid, 75mg aspirinACE-I), 0.8mg folic acid, 75mg aspirin
• 1/3 people would benefit from “the Polypill”, 1/3 people would benefit from “the Polypill”, gaining average of 11 yrs free from IHD or gaining average of 11 yrs free from IHD or strokestroke
– NJ Wald, MR Law, BMJ Vol 326: 28 June, 2003NJ Wald, MR Law, BMJ Vol 326: 28 June, 2003

ConclusionsConclusions
• While acute stroke interventions capture While acute stroke interventions capture our imagination, the most significant our imagination, the most significant impact on reducing the devastation of impact on reducing the devastation of stroke remains it’s prevention.stroke remains it’s prevention.
• The data is convincing, and yet has not The data is convincing, and yet has not been fully disseminated to physicians and been fully disseminated to physicians and patients.patients.