Embed Size (px)
Citation preview
An evaluation of NHS Health Checks in community pharmacy;
changes in cardiovascular risk factors over one year in patients aged 40-74
SJ Butterworth
SC Willis
P Higginson
Manchester Pharmacy School
The University of Manchester
NHS Health Check
• Cardiovascular risk assessment
• Provided in the English National Health Service
• Population aged 40-74 without recognised cardiovascular disease– Assess cardiovascular risk factors
– Calculate cardiovascular risk (QRisk2-12)
– Convey risk to user in a way they can understand
– Provide supporting lifestyle advice
AIMS
• Evaluate the implementation of NHS Health Checks in a community pharmacy by comparing against national standards and targets
• Investigate the outcomes of intervention by reassessing a sample of patients after a period of around one year.

METHOD

Study design
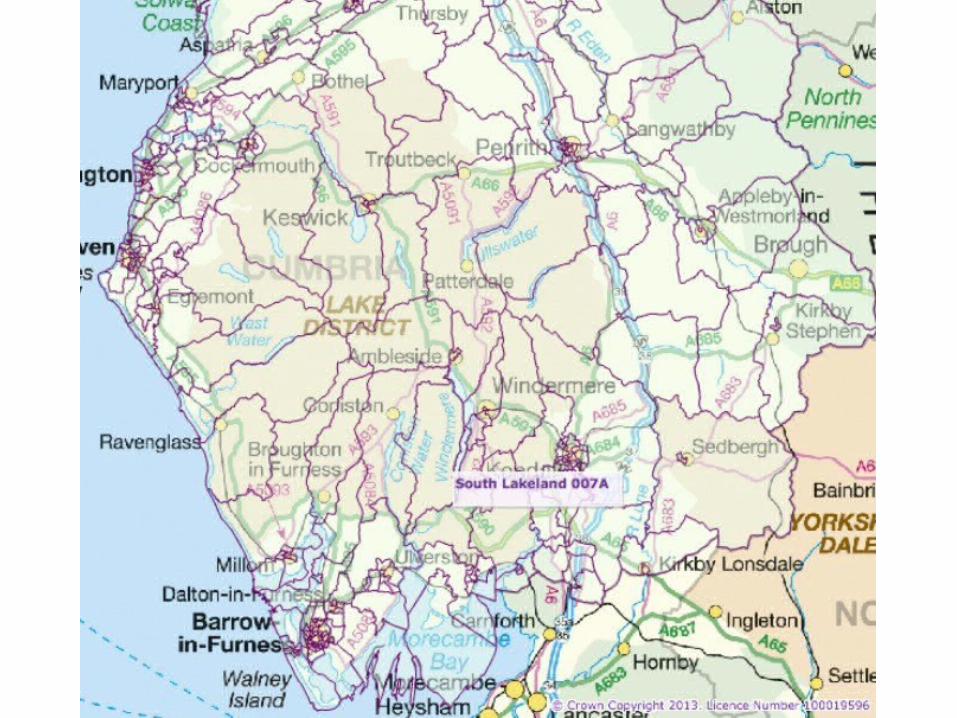
• Single community pharmacy in a rural setting in England
• Initial Health Checks on eligible population (from December 2012-June 2014)
• Follow up after about 1 year on a subset of that population (invited sequentially to return up to a minimum of 50)
RESULTS
Can community pharmacy in non-urban settings effectively contribute to targets for the proportion of Health Checks completed?
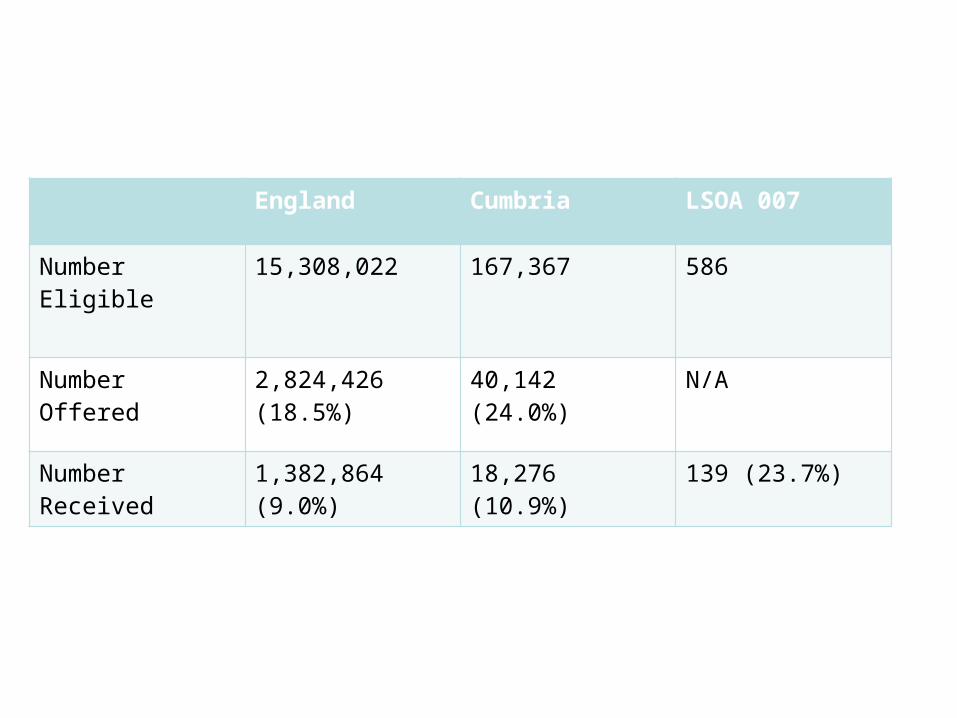
England Cumbria LSOA 007
Number Eligible 15,308,022 167,367 586
Number Offered 2,824,426 (18.5%)
40,142 (24.0%) N/A
Number Received 1,382,864 (9.0%) 18,276 (10.9%) 139 (23.7%)
To what extent do Health Checks completed in community pharmacy meet recognised quality standards?
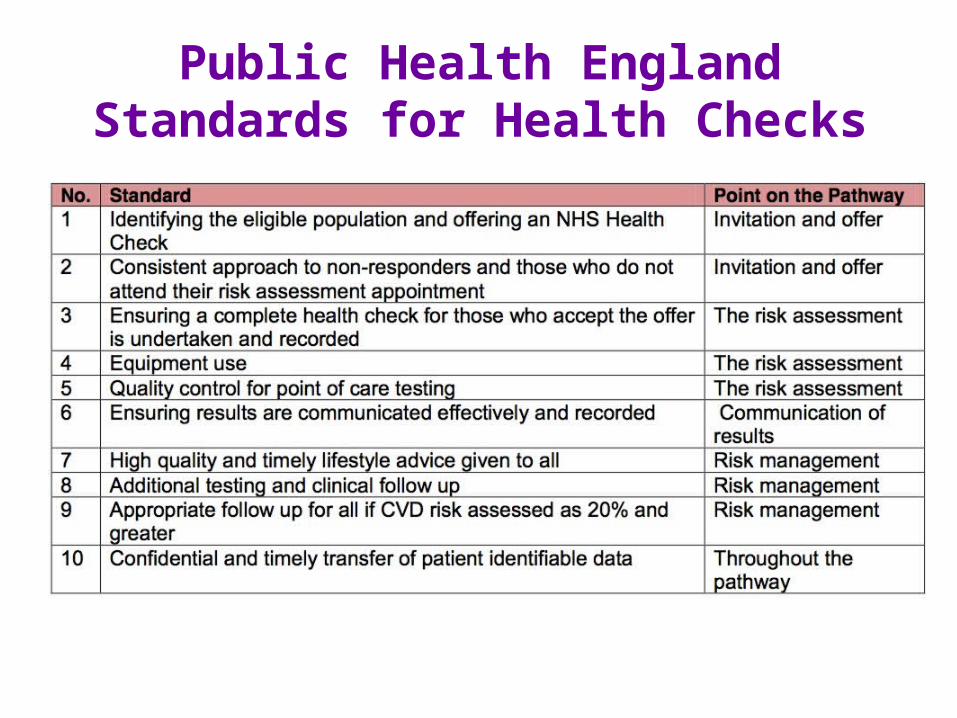
Public Health England Standards for Health Checks
What are the outcomes of health checks completed in community pharmacy either through measurable changes over 12 months or through referral?
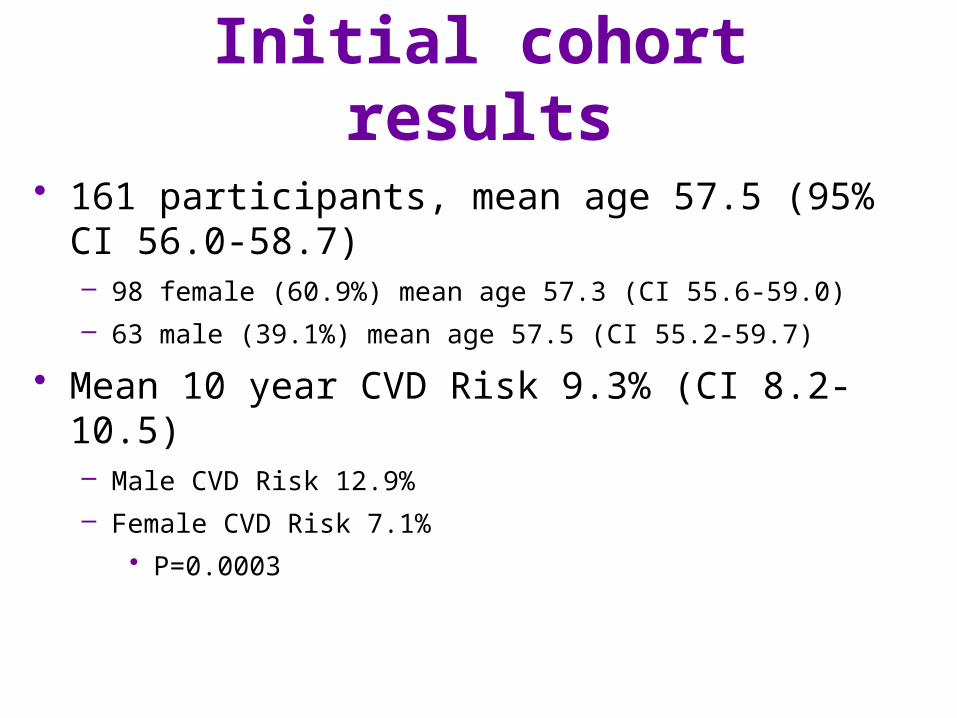
Initial cohort results
• 161 participants, mean age 57.5 (95% CI 56.0-58.7)– 98 female (60.9%) mean age 57.3 (CI 55.6-59.0)
– 63 male (39.1%) mean age 57.5 (CI 55.2-59.7)
• Mean 10 year CVD Risk 9.3% (CI 8.2-10.5)– Male CVD Risk 12.9%
– Female CVD Risk 7.1%
• P=0.0003
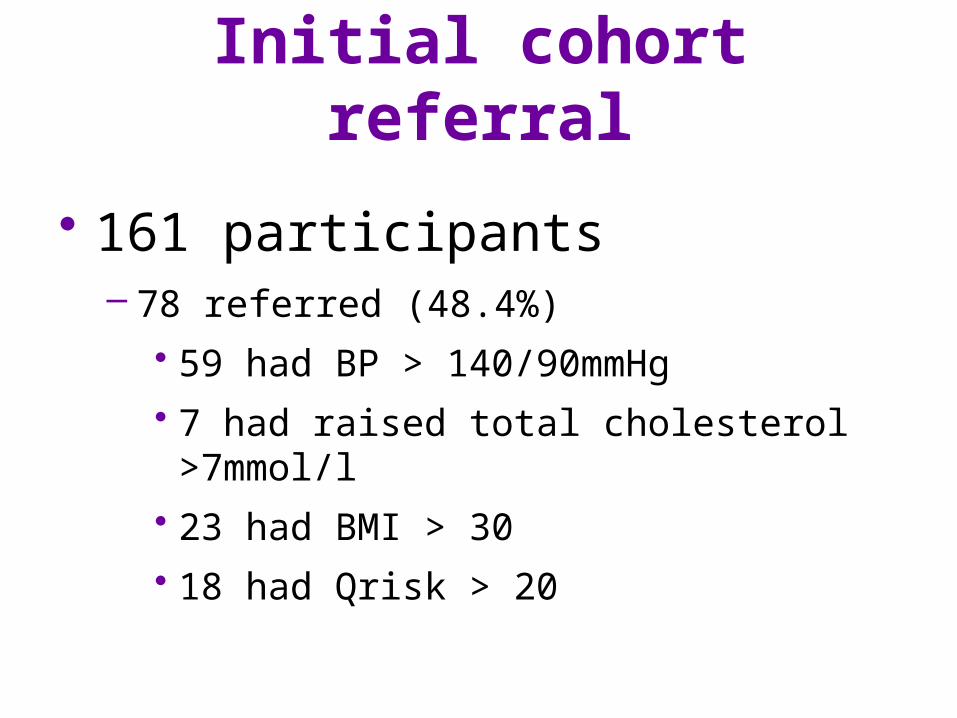
Initial cohort referral
• 161 participants– 78 referred (48.4%)
• 59 had BP > 140/90mmHg
• 7 had raised total cholesterol >7mmol/l
• 23 had BMI > 30
• 18 had Qrisk > 20
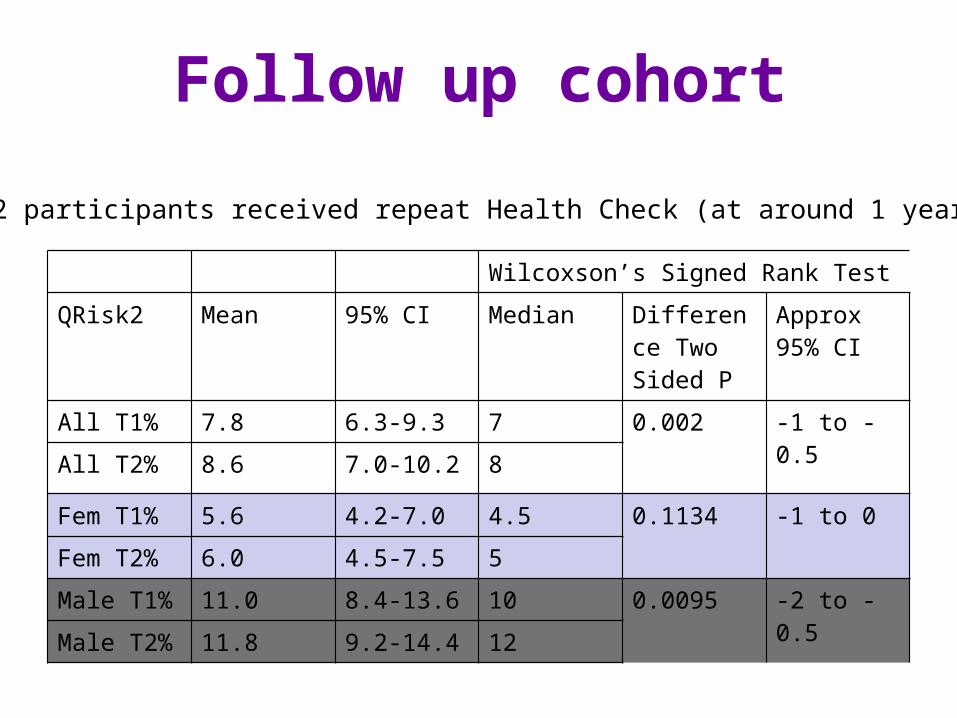
Follow up cohort
Wilcoxson’s Signed Rank Test
QRisk2 Mean 95% CI Median Difference Two Sided P
Approx 95% CI
All T1% 7.8 6.3-9.3 7 0.002 -1 to -0.5
All T2% 8.6 7.0-10.2 8
Fem T1% 5.6 4.2-7.0 4.5 0.1134 -1 to 0
Fem T2% 6.0 4.5-7.5 5
Male T1% 11.0 8.4-13.6 10 0.0095 -2 to -0.5
Male T2% 11.8 9.2-14.4 12
52 participants received repeat Health Check (at around 1 year)
DISCUSSION
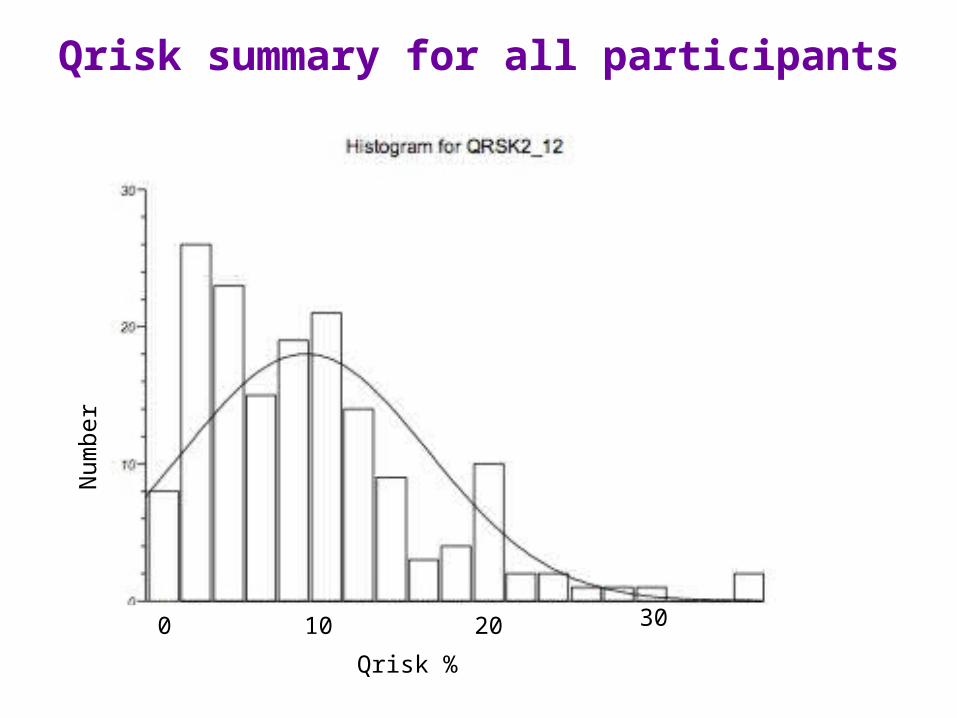
Qrisk summary for all participantsN
umbe
r
Qrisk %
0 10 20 30
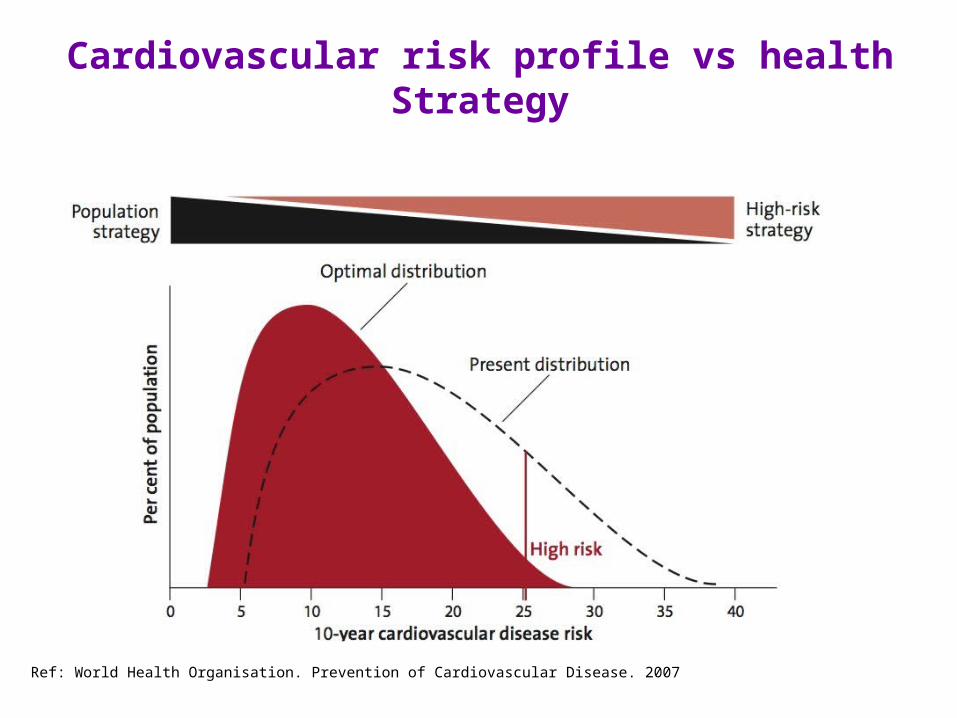
Cardiovascular risk profile vs health Strategy
Ref: World Health Organisation. Prevention of Cardiovascular Disease. 2007
Conclusion
• Community pharmacy is able to identify and refer high cardiovascular risk patients
• Community pharmacy can contribute to targets for delivery of NHS Health Checks
• The extent to which community pharmacy can contribute to longer term outcomes through NHS Health Checks is unknown
Acknowledgement
• Grateful thanks to the Health Education Foundation, whose educational bursary supported this study













![0750650842.Butterworth Heinemann.precast.concrete.structures.mar.2002 Slash Zero]](https://img.pdfslide.us/doc/110x75/5436f7d6219acd0f088b483a/0750650842butterworth-heinemannprecastconcretestructuresmar2002-slash-zero.jpg)