Embed Size (px)
Citation preview
HSCI 678 Intro to US Health Services System
Health Insurance:Major Finance Mechanism
Chapter 6
Dr. Tracey Lynn Koehlmoos
Chapter Overview
• Insurance Concepts
• Evolution of Health Insurance
• Private Health Insurance
• Public Health Insurance
• Pending Policy Reforms
• This chapter will not cover managed care
General Concept
• Insurance protects against infrequent, large loss by establishing contractual relations between the insured and the insurance provider and spreading the risk across a larger population.
General Risk Assessment
• Underwriting Process-actuarial risk• Experience Rating• Cherry Picking/Cream Skimming• Adverse Selection• Redlining
• Insurers goal: premium $ received > benefit $ paid
Specific Health Concepts
• Early days:– Linked to Employment– Hospitalization Only (1:13 among non-elderly)
• Conceptual Shift– Expanded scope of interactions– Non-random, non catastrophic events– Commercial v. social purpose
Risk Assessment
• 35% of insured—no claims
• 5% of insured = majority of claims
• Most insurers require medical screening
• Pre-existing conditions– Excluded– HIPAA (1996)
Direct Risk Adjustment
• Medical Underwriting– Tier rating—by member and industry– Durational rating—Low $ to start, increases
over time
• Redlining– Excludes individuals or groups based on
perceived hazards, life-style or claims history
Indirect Risk Adjustment
• Co-payments
• Limited Benefits Packages (procedures/pharmaceuticals)
• Caps/Ceilings
• Waiting period for effectiveness
• Results in inequitable access across the US
Growth of Commercial Health Insurance
• Provider-Organized Plans—dominant before WWII
• Post-WWII: Growing Non-for Profit Hospitals, more plans based on employment groups
• 1947 Taft-Hartley Act: Health benefits as a condition of employment for which labor was entitled to negotiate
Availability in Small Businesses
• Smaller businesses <100 employees• 50% of US labor firms• Nature of business too high risk• Unaffordable premiums—cannot spread risk• Part-time work force• One claim could increase all premiums• 10 to 40% higher cost to small v. large
business
Retiree Health Insurance
• Larger companies offer this as a benefit
• Hard to capture this group as data
• Jeopardy of benefits due to shake-ups in the mid-1980’s
• Medicare eligible—Medicare 2nd payor
• Employers seek higher cost share
• Medicare Part D; Patient’s Bill of Rights
Self-Funded Health Insurance
• Large group of employees• Eliminates need for insurance company• ERISA exemptions• Pay only what is used• Can negotiate rates• Insurance companies can be hired to bear
excessive financial risk• Third Party Administrator can handle admin.
The Cost of Doing Business
• Health Insurance is a major expense
• Premium growth rates—on the rise, again
• $4,692 per employee & family per year
• $2,088 per employee per year
• 75% of business health expenditures are on health insurance premiums
• 16% Medicare Contributions
• 8% Workman’s Compensation
Cost Containment Measures
Cost Sharing/Co-payments
• Limiting Scope of Benefits
• Caps on Insurance Expenditures
• Controls on Utilization– Prior Authorization– Second opinions– Pre-certification (nursing home stay)
ERISA
• Employee Retirement Income and Security Act of 1974
• Allows large employers to self-insurer
• Response to concerns on pension mismanagement
• Protects health services benefits packages
HIPAA
• Established requirements for carriers at the individual, small and large group markets
• Portability from group to individual plan
• Limits pre-existing condition waiting periods
• Also, state reforms in the early 1990’s
HIPPA
• Health Insurance Portability and Accountability Act of 1996
• Allows employees to “carry” insurance to the next job without a waiting period
• Allows employees in small companies to bring in previous insurance
• Addresses confidentiality issues
Summary of Private Insurance
• Covers 2/3 of US population
• Mostly as employee benefit, large group
• New laws and regulations to protect the benefits of the insured
• Ineligible people—may use individual policies
Public Health Insurance
• Tricare
• Medicare
• Medicaid
• State insurance programs for the uninsurable
• State Child Health Insurance Programs
Tricare
• Military dependents and retirees
• Supplemental to Military Health Service System
• 8.4 million beneficiaries
• Outside of the military system, Tricare functions as an HMO with contracts awarded to regional civilian companies.
Medicare
• Social Security Act of 1965
• Originally only for >65 years of age– Currently: 87% of beneficiaries
• 1972: End Stage Renal Disease (ESRD)
• 1973: Any age, Medicare disability– Currently: 13% of beneficiaries
Do you know your ABCD’s?
• Part A: Hospital Insurance (HI) – SNF, HH, Hospice– Deductible $840 per benefit period– Financed by Fed Trust Fund (payroll
deduction, employer contributions)
• Part B: – Supplemental Medical Insurance (SMI)– Physicians, tests, outpatient services– Monthly premiums 75% & by Fed Trust Fund
More Medicare ABCD’s…
• Part C: Medicare + Choice, 1997– Managed Care with mixed results– Patients were slow to sign up– Providers found it costly
• Part D: Prescription drug plans– New and confusing– Threats to Medicaid/Medicare – Slow patient sign up
Medicaid
• Social Security Act of 1965
• State and Federal Program 50/50
• No or Low co-pay or deductibles
• State offerings varyAll include: Inpatient, outpatient, x-ray, HH,
preventive services for children, family planning
Some: Podiatrist, Dentist, Physical therapy,
case management, eyeglasses
Medicaid Eligibility
• Eligibility varies—almost all “Low Income”
• Pregnant woman
• Infants, children < 6
• Elderly, blind, disabled, poor Medicare
• Special groups who qualify because of the disease (HIV/AIDS, NBCCEDP)
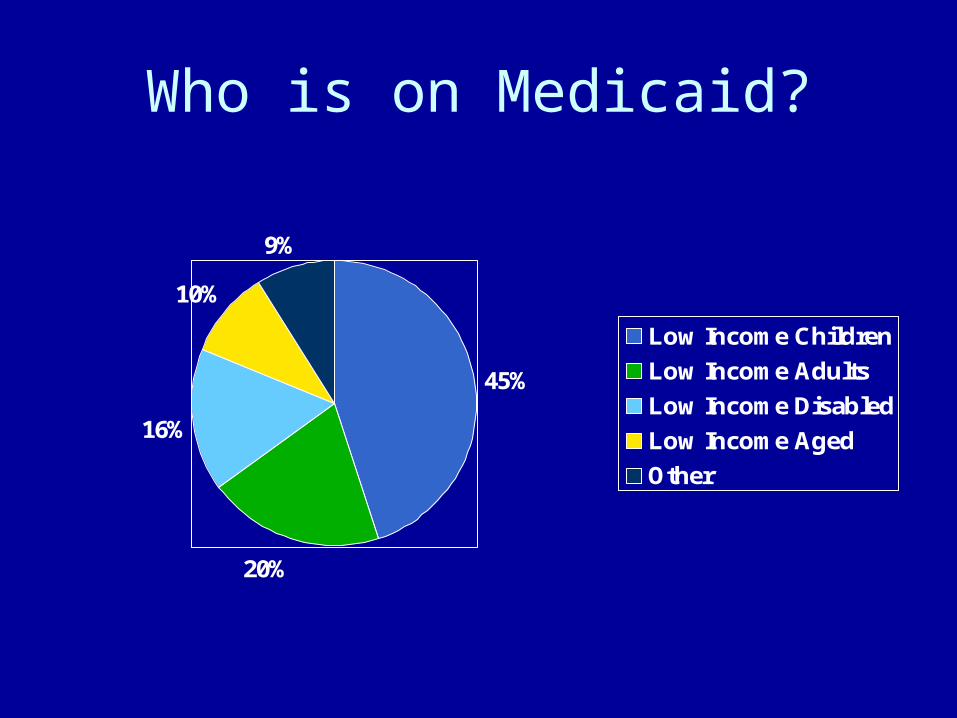
Who is on Medicaid?
45%
20%
16%
10%
9%
Low Income Children
Low Income Adults
Low Income Disabled
Low Income Aged
Other
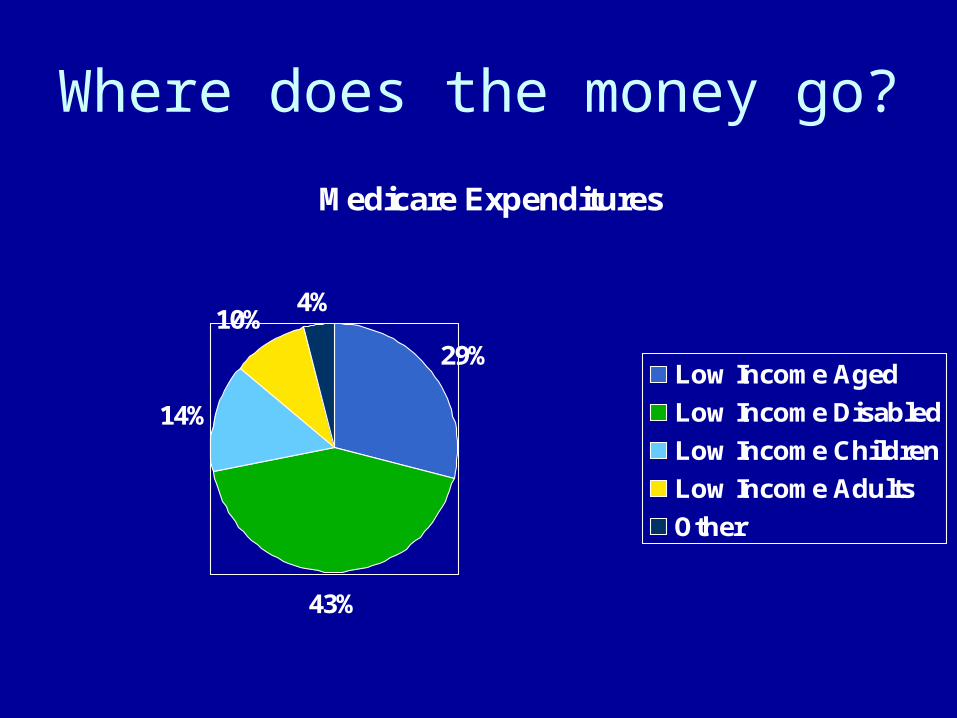
Where does the money go?
Medicare Expenditures
29%
43%
14%
10%4%
Low Income Aged
Low Income Disabled
Low Income Children
Low Income Adults
Other
Other State Run Programs
• Medically Indigent Programs
• State Sponsored Health Insurance Programs for the Uninsurable
• State Children’s Health Insurance Program (SCHIPs)—BBA 1997
Other types of insurance
• Workers’ Compensation Insurance
• Viatical Settlements
• Health Ins Purchasing Cooperatives
Summary
• 70% of US and almost all elderly have health insurance
• Medicaid covers 10% of US population• 20% of US population NO insurance
• Cost of premiums continue to rise• Employer sponsorship remains link• No basic set of benefits in the US