Embed Size (px)
Citation preview

HPI• A 73-year-old woman is brought to your practice by her
husband who is concerned for his wife’s well-being. He explains that for the past few months he has noticed a severe decline in his wife’s short term memory. At first he attributed this to “normal aging”, but has recently noticed that has become less involved in her bridge club and rarely leaves the house. Of most concern, however, is a recent episode in which his wife had been preparing a meal for their son’s visit and had left the gas stove on for several hours unattended.
What other questions would you like to ask?

HPI
• Medical Hx: Tonsilectomy (1948), Hysterectomy (1989)
• Family Hx: Mother suffered from dementia and HTN, Father had HTN and CAD
• Social Hx: Married 55 years, 2 children, works as a substitute teacher
What is your differential diagnosis?

Differential Diagnosis• MCI• Dementia
– Alzheimer’s disease– Vascular dementia– Mixed dementia– Dementia with Lewy bodies (DLB)– Frontotemporal dementia (FTD)
• Depression (“Pseudodementia”)• Hypothyroidism• Normal pressure hydrocephalus (NPH)• Infection
– Neurosyphilis
• Head trauma– Chronic subdural hematoma
• Side effect of medication
• Vitamin deficiency – B12
What is your next step in assessing the patient?

Physical Exam• Vitals:
– BP 115/48 – T 37.3 – RR 22
• Gen: The patient is calm and cooperative• CV, Resp, abdominal exams: all wnl • Psych: negative depression screen• Neuro:
– alert and oriented to person and place, unable to name the day of the week.– Registration 3/3, recall 0/3 at 5 minutes– Unable to recall what the patient ate for breakfast this AM– MMSE: 21/30– Speech is fluent and appropriate in content– CN II-XII grossly intact– Motor: Strength 5/5 proximal and distal bilateral upper and lower extremeties– Sensory: intact to light touch, pinprick, and vibration throughout– MSRs 2+ and equal in upper and lower extremeties– Downgoing plantar response bilaterally– No resting or intention tremor– Tone normal (no rigidity)– Gait is smooth; not wide-based

Laboratory tests
• CBC: normal• WBC: 6,000• TSH: 2.7 uU/mL (normal)• Free T4: normal• B12: 816 pg/mL (normal)• VDRL/RPR: negative
What would you like to do next?

MRIMRI can detect patterns of cerebral atrophy suggestive of various neurodegenerative diseases.
In AD, cortical atrophy is seen as accentuation of the sulci and is localized most commonly to the frontal, temporal, and parietal lobes. Commonly, hippocampal atrophy is seen.
What does this pattern of atrophy suggest?What further testing can we perform?

Neuropsychological Tests• Tests were preformed in order to identify lapses in cognitive
function and abilities. Patient was found to be profoundly affected by short-term memory loss, testing in the 3rd percentile.
• The patient was asked to draw a clock face displaying a time of 2:45. The patient scored a four based on the following scale:

Alzheimer’s Disease• AD is the most common cause of dementia (~50%)
• Alzheimer disease (AD) is a neurodegenerative disorder of uncertain cause and pathogenesis that primarily affects older adults.
• The main clinical manifestations of AD are selective memory impairment and dementia.
• AD symptoms are likely a result of the accumulation of neuritic (senile) plaques as well as neurofibrillary tangles.
How would you like to proceed with this patient?

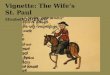
Histological interpretationsLight micrograph of human brain tissue in Alzheimer's disease, showing a senile plaque (pale area in center), a characteristic histological feature of the disease. Alzheimer's disease is a form of progressive dementia; the brain is smaller than normal, with degenerative changes affecting the frontal and temporal lobes.
Senile plaques are extracellular tangled masses of filaments & granules, often centered around an area of amyloid beta. Amyloid beta is derived from the larger protein amyloid precursor protein (APP) located on chromosome 21. Other genes associated with AD are presenilin 1 and 2. The main other feature of Alzheimer's disease is the formation of neurofibrillary tangles, masses of thickened filaments in the cytoplasm of neurons (nerve cells).

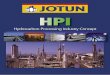
Histological features cont’d
Neurofibrillary tangles are bundles of filaments in the cytoplasm of the neurons that displace the nucleus. They are composed of abnormal tau protein (tauopathy), which normally acts as a microtubule stabilizing protein.In pyramidal neurons, they often have an elongated flame shape, as demonstrated in this slide.

Treatment• While treatments are available that can modulate the course of
the disease and/or ameliorate some symptoms, there is no cure, and the disease inevitably progresses in all patients.
• Most treatments are designed to augment the neurotransmitter acetylcholine.
• Acetylcholinesterase inhibitors (Aricept) are the only drugs that are known to slow the progress of AD-related memory loss.
• NMDA glutamate receptor antagonists (memantine/Namenda) are also commonly used to slow the progression of AD.
• Antidepressants and antipsychotics are frequently employed to treat behavioral disturbances.

Summary
• The patient and her husband were given information on the disease and some symptoms that might manifest as its progression continues.
• Language deficits, loss of mathematical skills and eventual loss of learned motor skills are commonly found in late-stage AD.
• In final stages, patients may become incontinent, mute, or unable to walk.

Neuropsychological Testing Role in Diagnosis
• Helpful in the evaluation of individuals with cognitive impairment and dementia.
• Cognitive testing under standardized conditions using demographically appropriate norms is more sensitive to the presence of impairments, especially impairments of executive function.
• Can establish a baseline in order to follow the patient over time. • Neuropsychological assessment can also help differentiate
between dementia and depression. • Can assess competencies and guide recommendations pertaining
to driving, financial decisions, and need for increasing supervision