Embed Size (px)
Citation preview

How to make changes in the NHS Keith Willett
Prof of Orthopaedic Trauma Surgery University of Oxford prev. National Clinical Director for Trauma Care
Medical Director for Acute Care; NHS England
ATOCP Conference Oxford 2016

Universal health care
Funded by taxation
8.7% of GDP (17.6, 10.9)
UK 3.6k, Can 5.7k, US 9.1k US$

NHS Quality Framework to drive improvement
Bring clarity
to quality
Measure
quality
Publish
quality
Reward
quality
Leadership
for quality
Innovate for
quality
Safeguard
quality
“Compelling evidence that it is possible to change professional
behaviour to improve quality of care, reduce cost ….. for better VALUE”
QUALITY:
clinical effectiveness, patient safety, experience of patients


The NHS is an amoeba . . . . .
Desmond Morris and Keith Willett

First, identify the key interventions in the care pathway that will really
improve care and outcomes ……………
Bring clarity
to quality
Measure
quality
Publish
quality
Reward
quality
Leadership
for quality
Innovate for
quality
Safeguard
quality
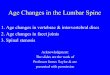
Changing practice for quality improvement in
healthcare at scale
7
Multi-
professional
clinical and
patient advisory
group
Review of
all current
evidence
and
guidelines
Activity data from
registries and Hospital
Episode Statistics
NICE standards
health economics
operational delivery
workforce
Recommendations
Measurable
commissionable
aligned payments
Cost-effective

Secondly, agree the metrics by which care can be
appropriately judged by patients and all clinicians
NHS Hospital Episode Statistics data do not measure quality
Bring clarity
to quality
Measure
quality
Publish
quality
Reward
quality
Leadership
for quality
Innovate for
quality
Safeguard
quality

Hip Fracture - agreed best practice metrics
Time to surgery (<36 hours)
1. Arrival in Emergency Dept (or diagnosis if an inpatient) to start of anaesthesia
Involvement of the multi-professional team: 2. Admitted under the joint care of a Consultant Geriatrician and a Consultant
Orthopaedic Surgeon
3. Admitted using an assessment protocol agreed by geriatrics medicine, orthopaedic surgery and anaesthesiology
4. Assessed by a Geriatrician in the perioperative period
Consultant or senior resident within 72 hours of admission
5. Postoperative Geriatrician-directed: 1. Multiprofessional rehabilitation team
2. Fracture prevention assessments (falls risk and bone health)
6. Dementia Assessment: Mental test score at admission and prior to discharge by nurses

National Clinical Audit / Registry
Bring clarity
to quality
Measure
quality
Publish
quality
Reward
quality
Leadership
for quality
Innovate for
quality
Safeguard
quality

Thirdly incentivise the clinical behaviour and
patient flow changes in the care pathway
money follows the right patient care ……..
Bring clarity
to quality
Measure
quality
Publish
quality
Reward
quality
Leadership
for quality
Innovate for
quality
Safeguard
quality

12
Pay by performance tariff
• Base tariff set below national average cost • Sum of base tariff and BPT higher than national average cost
Base tariff for each HRG
Additional payment for best
practice Reduction in base tariff
for current compliance
Payment
per
patient
Original
base tariff Best
practice
tariff
2-part tariff for best practice initially 9% now 19% of HRG
£1235 of £6500 HRG
HRG
tariff
price

Link to national registry to drive change
LOCAL
HOSPITAL
CLINICAL
TEAM
Commissioner Insurer/Payer
National Hip
Fracture
Registry Unique identifier
Individual patient data
BPT compliance
Additional
payments
pay tariff uplift (~19%) £500k to £1m per year
per hospital in extra
income
(300-500 cases a year)

Improvement in Hip Fracture Care 2010 - 2014 Best Practice Tariff: percentage attained for each criteria; all criteria 24 to 64%
Admitted under joint geriatric/anaesthetic protocol increased from 64 to 97%;
Surgery within 48 hours rising from 65 to 77% in 36 hours, to 87% in 48hrs;
Seen acutely by a Geriatrician up from 48 to 90%; bone health assessment up 72 to 97%
16 quarter-on-quarter improvement
100%

Too difficult to solve for 25 years . . . .
MAJOR TRAUMA
Life threatening
or life-changing serious
physical injury – often
multiple
15
MAJO
R T
RAU
MA
Typified by delay,
inappropriate care,
avoidable death and
disability

Preferred acute patient pathway
16
MAJO
R T
RAU
MA On scene triage 24/7 network coordinator
in Ambulance Service
Medical consultant advice
direct transfer
(<45mins)
indirect transfer
(geography, time-critical
intervention)
MAJOR TRAUMA CENTRE
Consultant led trauma team
Immediate operating theatre
All specialties: neurosciences
Immediate CT scan
Interventional radiology
Specialist critical care
Trauma Unit
trauma team
immediate CT
resus, assess
and ? transfer
enhanced
care team

Preferred rehabilitation pathway Network Director for Rehabilitation
17
MAJO
R T
RAU
MA
Directory
of Rehab
services
PRESCRIPTION
for rehabilitation
physiotherapy, OT, SALT,
social work, mental health
neuropsychology
MAJOR TRAUMA CENTRE
Consultant Clinical Lead
Acute Trauma Rehabilitation Manager
Full multi-disciplinary team
Care & Rehabilitation Coordinator
Trauma Unit
or Local Hospital
Identified Lead for
Trauma Rehab Services
Key worker
Level 1
complex
Level 2
specialist
Level 3 general
independence Vocational / Educational

All networks and MTCs
implemented in April 2012
• Set-up 22 regional trauma
networks (27 MTCs) – pop 53m
• Cover 1.4m to 5.2m population
• Ongoing quality assurance
through TARN trauma registry
• Nationally Commissioned
– NHS England
– Clinical Reference Group
18
MA
JO
R T
RA
UM
A
= established Major Trauma Centre

Best Practice Tariff Criteria
Level 1 ISS > 8 and the following criteria met: the patient is treated in an MTC Complete patient data submitted to TARN registry within 40 days of discharge MDT Rehabilitation prescription is completed for each patient Tranexamic acid administered within 3 hours of injury
Level 2 ISS > 15 Level 1 criteria are met, plus either: Patient received by a trauma team led by a Consultant within 30 (5) minutes of
arrival If the patient is transferred as an ‘urgent’ transfer then the transfer should take place
within 2 calendar days of referral from the trauma unit.

Driving performance improvement
. . . . . . . with a best practice tariff
MAJOR
TRAUMA
CENTRE
Commissioners / payer Trauma Audit
Research
Network (TARN)
Individual patient data
unique identifier
KPI compliance
Additional best practice
tariff per patient
£1500 - £3000
Major Trauma
Centres only
financially viable if
delivered best
practice care …….
MAJO
R T
RAU
MA
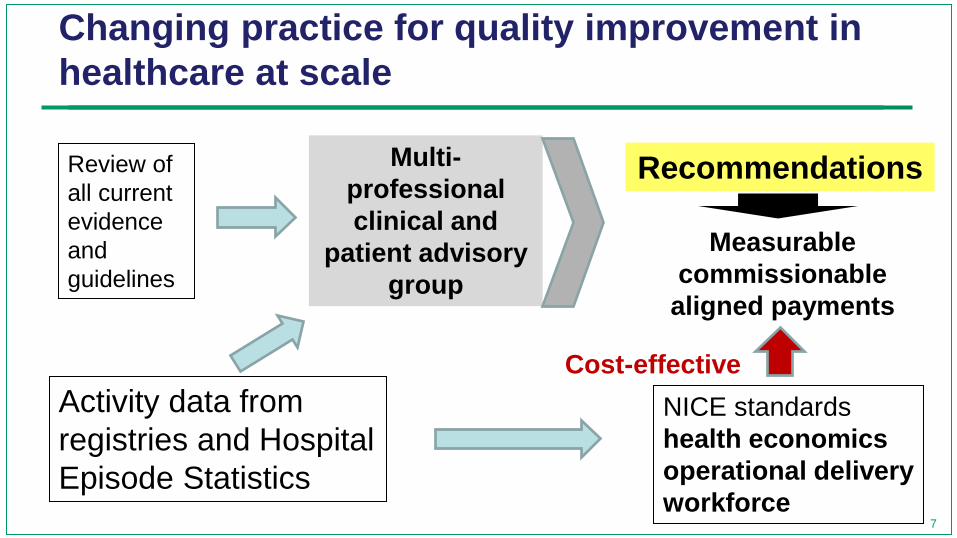
ISS 16-75 Best Practice tariff compliance 2012-13
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 11 12
months
Level 1 criteria only
Level 1 and 2
criteria met
13,000 patients
Consultant led
trauma team
Transfer 2 days

National Dashboard: All Major Trauma Centres
Consultant-led Trauma Team on arrival, patient ISS>15
80%
70%
60%
50%
40%
Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
2011 2011-12 2012-13 Year
2013-14
Q1 Q2
P = 0.001
Q3 Q4
4,000 patients
11,300 patients

National Dashboard: All Major Trauma Centres
Tranexamic acid within 3h injury
80%
70%
60%
50%
40%
Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
2011 2011-12 2012-13 Year
2013-14
Q1 Q2 Q3 Q4
81.5%
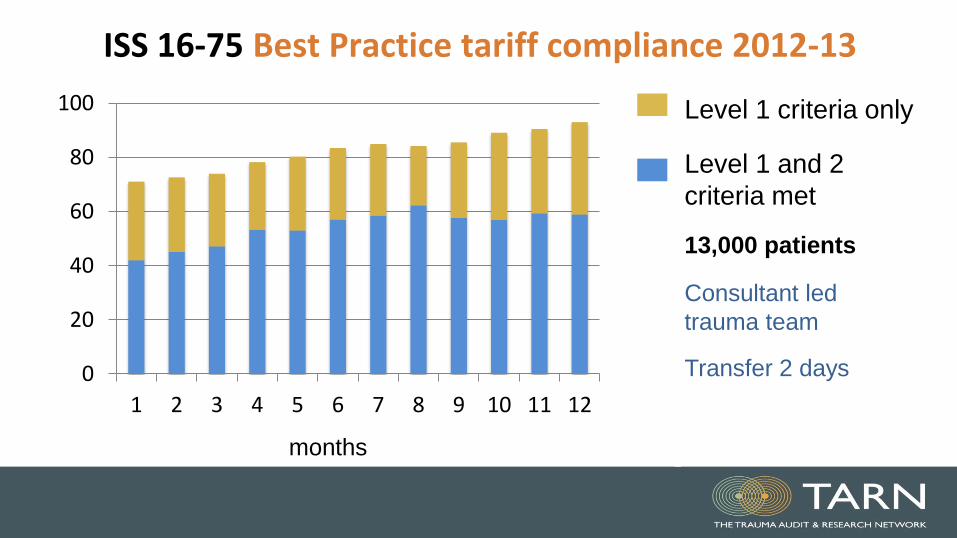
MAJOR TRAUMA NETWORKS INTRODUCED
25-40% increase in
survival

Ws breakdown (Major Trauma Centres and Trauma Units)
After MTC designation (from April 2012)
PROBABILITY of SURVIVAL band
Number in Ps group
EXPECTED number of survivors
ACTUAL number of survivors
Actual number of
deaths
Difference (W) = (Actual vs
Expected / N/100)
Fraction in the TARN
database
Case mix standardised
(adjusted) difference (Ws = total)
>95% 33176 32722 32835 341 0.339 0.673 0.2278
0.90-0.95 10522 9793 9755 767 -0.364 0.159 -0.0579
0.75-0.90 5379 4572 4687 692 2.138 0.085 0.1817
0.50-0.75 2917 1926 1993 924 2.290 0.046 0.1053
0.25-0.50 1542 572 602 940 1.922 0.025 0.0480
0.00-0.25 784 105 138 646 4.144 0.012 0.0497
54,320 Ws = 0.555
equates to ~600 lives saved

-10
-50
510
.5 1 1.5 2 2.5precision (1/seWs)
Ws -2SD
+2SD target
-3SD +3SD
Before Major Trauma Centre DesignationUniversity teaching hospitals before designation as a Major Trauma Centres

-10
-50
510
0 .5 1 1.5 2 2.5precision (1/seWs)
Ws -2SD
+2SD target
-3SD +3SD
After Major Trauma Designation
University teaching hospitals after designation as a Major Trauma Centres
21326 pts, 47% ISS >15

Continuous assurance, reappraisal, comparison
and sharing ……….
public reporting and peer review
Bring clarity
to quality
Measure
quality
Publish
quality
Reward
quality
Leadership
for quality
Innovate for
quality
Safeguard
quality

Rate of Survival


The role of management is to create a culture and reward
system that guides thousands of decisions in the direction of better
quality and service at reduced cost
A Enthoven
Bring clarity
to quality
Measure
quality
Publish
quality
Reward
quality
Leadership
for quality
Innovate for
quality
Safeguard
quality

The role of management is to create a culture and reward
system that guides thousands of decisions in the direction of better
quality and service at reduced cost
K Willett
Bring clarity
to quality
Measure
quality
Publish
quality
Reward
quality
Leadership
for quality
Innovate for
quality
Safeguard
quality
clinicians is to

Clinical risk
Payer risk
Operational risk
Provider risk
Service specifications
Professional standards
Payment systems
Quality assurance

Leadership is the capacity to turn vision into reality
Warren Bennis
LESSON 1
Clinical teams in a universal healthcare system can be trusted to design and commission best practice and best value services and select the measures by which their services should be fairly judged

Leadership is the capacity to turn vision into reality
LESSON 2
Deriving policy through multi-professional and patient consensus has credibility and ensures engagement and ownership in provider clinicians for delivery

Leadership is the capacity to turn vision into reality
LESSON 3
Linking payment for
performance and public
reporting are key, and
ensures government buy-in
We must not be naïve

Leadership is the capacity to turn vision into reality
LESSON 4
We need to move healthcare systems from summative assessment (targets) …… ….. to clinically credible and formative assessment

Healthcare System change in the NHS: If I were doing it again Locally
1. Always question why you are doing it that way?
2. If you have a vision, energy, and passion you will always win through
3. Keep adding to ‘your’ design with others views and ideas
4. What problem is on the managers desk not yours? Can you help it?
Nationally
1. Educate, then use patients and the public more to construct the narrative
2. Work with the next generation of enthusiasts (but beware the fanatics)
3. Take what you could get in the battles you cannot win – it’s iterative
4. Mesh with as many other strategies as possible, but not to be dependent
5. Appreciate the operational delivery and financial complexities early
6. Political will is not essential unless you want to divert or need more funds
7. Be ready for your moment in the sun ……………

Redesigning the whole of Urgent and Emergency Care
39

Bring clarity
to quality
Measure
quality
Publish
quality
Reward
quality
Leadership
for quality
Innovate for
quality
Safeguard
quality

![Consultation on changes to NHS Foundation Trust Annual ... · 3.1 Rationale 3.2 Previous requirement 3.3 for removal ... [IR4]: These requirements ... reports. NHS Foundation Trust](https://img.pdfslide.us/doc/110x75/5ad6da3d7f8b9a32618b97c4/consultation-on-changes-to-nhs-foundation-trust-annual-rationale-32-previous.jpg)